Embed Size (px)
Citation preview

Salvage Surgery for RecurrentNasopharyngeal CarcinomaSheng-Po Hao, MD; Ngan-Ming Tsang, MD, DSc; Chen-Nen Chang, MD
Objective: To evaluate the results of salvage surgery forpatients with primary recurrence of nasopharyngeal car-cinoma after radiotherapy.
Design: Cohort study.
Setting: Academic tertiary referral center.
Patients: Eighteen consecutive patients with primary re-currence of nasopharyngeal carcinoma after radiation fail-ure underwent nasopharyngectomy for cure via a facialtranslocation approach from July 1, 1993, to December 31,1999. Follow-up ranged from 3 to 71 months. Five pa-tients with skull base invasion required a combined neu-
rosurgical approach to treatment. Seven patients had ad-ditional postoperative radiotherapy.
Results: The actuarial 3-year survival was 57%, whilethe local control was 78%. Four of 5 patients who hadskull base invasion achieved local control. There was nosurgical mortality, and the morbidity was 22%.
Conclusion: Advances in skull base surgery make pos-sible the effective control of primary recurrence ofnasopharyngeal carcinoma, with acceptable mortality andmorbidity.
Arch Otolaryngol Head Neck Surg. 2002;128:63-67
N ASOPHARYNGEAL carci-noma (NPC) is the mostcommon cancer of thehead and neck in thesoutheastern part of
China, Taiwan, Hong Kong, and Sin-gapore. Nasopharyngeal carcinoma re-fers to malignant tumor arising from theepithelial cells lining the nasopharyngealspace. Other malignant tumors, such asglandular tumors arising from the minorsalivary glands or sarcomas and lympho-mas, are not included in the category ofNPC. Nasopharyngeal carcinoma is re-lated to Epstein-Barr virus,1,2 and, con-trary to epithelial tumors from other partsof the upper aerodigestive tract, the main-stay of NPC treatment is radiotherapy. Thisis because (1) most NPCs are undifferen-tiated or nonkeratinizing carcinomas,which are sensitive to radiotherapy, and(2) the complexity of the nasopharyn-geal anatomy makes radical surgery diffi-cult. However, in recent years, as we havebetter understood the anatomy and spreadof nasopharyngeal tumors, and because ofthe advancements in skull base surgery,the nasopharynx is no longer considereda no-man’s-land. Herein, we report our ex-perience of salvage surgery for recurrent
NPC after radiation failure at the primarysite.
RESULTS
Of the 18 patients, 15 had negative mar-gins, while 3 had microresidual diseases.There was no surgical mortality, and themorbidity was 22% (4/18), including cere-brospinal fluid rhinorrhea in 1 patient, flapnecrosis in 1, osteoradionecrosis (ORN) ofthe translocated facial bone graft in 1, andmild epiphora in 1 (Table 1). The patientwho had postoperative cerebrospinal fluidrhinorrhea died of brain involvement 3months after surgery. The patient with ORNwas treated with 3 successive sequestrec-tomies and hyperbaric oxygen therapy andultimately required a free flap to resolve theproblem. The patient with flap necrosis un-derwent several debridements, and the oro-pharyngeal wound healed with a second-ary intention. However, she died of massivebleeding from carotid artery blowout 15months after surgery.
The 18 patients were followed up for3 to 71 months (Table 1). To date, 3 pa-tients have died of local disease (includ-ing 2 with microresidual disease), 2 havedied of nodal metastases (1 neck and 1 ax-
ORIGINAL ARTICLE
From the Departments ofOtolaryngology (Dr Hao),Radiation Oncology(Dr Tsang), and Neurosurgery(Dr Chang), and Head & NeckOncology (II) (Drs Hao andTsang), Chang Gung MemorialHospital, Chang GungUniversity, Taoyua, Taiwan,Republic of China.
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 128, JAN 2002 WWW.ARCHOTO.COM63
©2002 American Medical Association. All rights reserved. on December 6, 2011 www.archoto.comDownloaded from

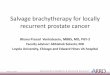
illa), 1 has died of distant metastasis, and 1 has died ofmassive bleeding (Table 1). The actuarial 3-year sur-vival was 57% (Figure 1), while the local control was78% (Figure 2). The survival rates of the patients ac-cording to rT stage are summarized in Table 2.
Five patients who had skull base or intracranialextension needed a combined neurosurgical resection;1 died of local recurrence in the brain and 1 died of ax-illary nodal metastases. Four (80%) of the 5 patients hadlocal control.
Of the 18 patients, 16 had undifferentiated carci-nomas (World Health Organization type 3), and 2 hadkeratinizing squamous cell carcinomas (World Health Or-ganization type 1). In 3 patients, no cancer was found inthe surgical specimens, although preoperative biopsieshad demonstrated recurrent cancer.
COMMENT
The mainstay of NPC treatment is radiotherapy, as mostNPCs are undifferentiated or nonkeratinizing carcino-mas, which are radiosensitive. Nasopharyngeal carci-noma, compared with other epithelial cancers of the up-per aerodigestive tract, has a high incidence of distantmetastasis. However, locoregional failure is still the maincause of death. For example, in our tumor registry, 1002(35%) of 2860 registered patients with NPC died oflocal disease or local recurrence, despite radical radio-therapy.4
Although the incidence of local persistent or recur-rent disease has decreased following introduction ofconcurrent chemoradiotherapy,5 such occurrences leadpatients to a dismal prognosis. Treatment of primary re-currence can be accomplished by additional external beamradiotherapy or by skull base surgery. Reirradiation ofthe primary recurrence of NPC has been reported,6-9 butit was accompanied by significant morbidity caused bycomplications such as severe xerostomia, trismus, deaf-ness, and neurological sequelae.8,9 Other pitfalls includethe complications of ORN following reirradiation.10,11 Thepatient may experience foul odor, severe pain, and mas-sive bleeding. Furthermore, it cannot be assumed thatNPC cells surviving the first course of radiotherapy willrespond to further radiotherapy.
The surgical approach to the nasopharynx has beenthe focus of interest since the development of skull basesurgery. Fisch12 used an infratemporal fossa approach toresect nasopharyngeal tumors. However, in this lateralapproach, mastoidectomy must be accomplished beforeattacking the nasopharynx. Transpalatal approaches havebeen favored by Fee13 and Hsu14 and their colleagues; how-ever, only small mucosal tumors in the central roof ofthe nasopharynx are suitable for this approach. A man-dibular swing approach attacks the tumor from below,but we have found the exposure of the skull base to belimited with this approach, especially when the tumorhas invaded the foramen ovale or touched the pterygoidplate base. Nevertheless, it has been claimed that thismethod offers control of the ascending internal carotidartery and allows resection of the tumor in the parapha-ryngeal space medial to the artery.14 Wei et al,15 from HongKong, used the maxillary swing approach to resect thesedifficult tumors. This approach is ideal for tumors con-fined to the mucosal surface of the nasopharynx or tu-mors with paranasopharyngeal space invasion.15,16 In ourstudy, a facial translocation approach was used exclu-sively,17 and this approach can be combined with neu-
MATERIALS AND METHODS
From July 1, 1993, to December 31, 1999, in the Sec-ond Division of Otolaryngology, Chang Gung Me-morial Hospital, Chang Gung University, Taoyua,Taiwan, Republic of China, we operated on 18 pa-tients in whom local recurrence developed after ra-diotherapy for NPC. There were 13 men and 5 women(age range, 30-62 years). Previously, 17 patients hadundergone a single course of radiotherapy with morethan 6600 rad (66 Gy), while 1 patient had under-gone a second course of radiotherapy for his pri-mary recurrence. Four patients had undergone ra-diotherapy elsewhere. Our preferred method ofpreoperative radiologic diagnosis is magnetic reso-nance imaging scans; however, early in the study,2 patients had computed tomography only.
Preoperatively, the tumors were classified as rT1(8 patients), rT2b (1 patient), rT3 (5 patients), andrT4 (4 patients), according to the American JointCommittee on Cancer staging system.3 The clinicalcharacteristics of the patients are summarized inTable 1. Two patients had previous sinus surgery,including 1 Caldwell-Luc operation and 1 func-tional endoscopic sinus surgery. One patient had per-sistent cervical metastasis after radiotherapy and un-derwent modified radical neck dissection beforenasopharyngectomy. Another patient had recurrentneck disease after completion of nasopharyngec-tomy for his primary recurrence and subsequently un-derwent modified radical neck dissection. The na-sopharyngectomies were carried out via a facialtranslocation approach. Five patients required a com-bined neurosurgical approach (3 subtemporal and 2subfrontal) and appropriate neurosurgical resec-tion. Seven patients who had tumor-positive or closesurgical resection margins underwent a second courseof radiotherapy postoperatively.
All patients had biopsy-proven primary recur-rence. A systemic workup with chest x-ray, abdomi-nal sonography, and technetium Tc 99m bone scanwas carried out before the operation, and if any ofthese examinations had positive findings, the pa-tient entered a second radiotherapy protocol and didnot have surgery. The contraindications for cranialbase surgery for recurrent NPC in our division are(1) extensive intradural invasion, (2) cavernous si-nus involvement, and (3) pharyngobasilar fasciae in-vasion. We do not consider bony destruction of thecranial base unresectable.
The cutoff point for study data was May 31, 2001.Statistical analysis was carried out using commer-cially available software (SPSS version 7.5; SPSS Inc,Chicago, Ill). The actuarial overall survival and lo-cal tumor control were calculated by the Kaplan-Meier method.
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 128, JAN 2002 WWW.ARCHOTO.COM64
©2002 American Medical Association. All rights reserved. on December 6, 2011 www.archoto.comDownloaded from

rosurgical craniotomy for tumors with skull base inva-sion.18
In the facial translocation approach, the facial os-teotomy can be localized based on the location of the tu-mor. If the tumor is confined to the nasopharynx or hasparanasal extension, a nasoorbitomaxillary osteotomy willsuffice, and the infraorbital neurovascular bundle can bepreserved. However, when the tumor has invaded theparapharyngeal space, a larger facial osteotomy, option-ally including part of the zygoma, is created to removethe tumor.
If the tumor has invaded the pterygoid plate base,a combined preauricular infratemporal subtemporalapproach is used.19 This approach offers superior andlateral approaches to the nasopharyngeal and parapha-ryngeal space. After temporal craniotomy, the tempo-
ral lobe is retracted to expose the temporal base. Theforamen ovale can be decompressed, and the trans-verse portion of the petrous internal carotid arterylying behind the foramen ovale is located and pro-tected. The tumor can then be removed from the supe-rior, lateral, and anterior directions. However, it is dif-ficult to differentiate bony invasion by cancer fromORN intraoperatively.20 Confirmation of clear marginsof skull base bone requires histopathological analysis.After the tumor is resected, the temporalis muscle issplit and its anterior half is transposed to fill the defect,covering the exposed subtemporal dura and separatingthe neurocranium from the underlying upper aerodi-gestive tract. Anterior craniofacial resection is carriedout if NPC involves the cribriform plate or the planumsphenoidale.
1.2
0.7
0.8
1.0
1.1
0.9
0.4
0.5
0.6
0.2
0.1
0.3
0 12 24 36 48 60 72 84Time, mo
Surv
ival
Figure 1. Actuarial survival of patients who underwent nasopharyngectomyfor primary recurrence of nasopharyngeal carcinoma.
1.1
0.9
1.0
0.8
0.7
0.6120 24 36 48 60 72 84
Time, mo
Loca
l Con
trol
Figure 2. Actuarial control of disease in the nasopharynx after resection.
Table 1. Clinical Characteristics of Patients With Recurrent Nasopharyngeal Carcinoma at the Primary Site*
Patient No./Sex/Age, y
RetreatmentStage Approach Margins
PathologicFindings Complications
Follow-up, mo/Outcome Status
1/M/38 rT1 FT − UD . . . 14/DLD2/M/42 rT3 FT and ST − UD . . . 21/NER3/M/35 rT2b FT + UD . . . 31/DLD4/M/42 rT4 FT and SF − UD Cerebrospinal fluid
rhinorrhea3/DLD
5/M/46 rT4 FT and ST − UD . . . 18/Died of distantmetastasis
6/M/59 rT3 FT and ST − UD Epiphora 31/NER7/F/30 rT1 FT − UD . . . 69/DN8/M/42 rT3 FT − UD . . . 33/NER9/M/58 rT1 FT − UD . . . 20/NER
10/M/56 rT3 FT − WD Osteoradionecrosis 71/NER11/M/62 rT1 FT − UD . . . 54/NER12/F/32 rT1 FT − UD . . . 49/NER13/F/41 rT1 FT − WD . . . 59/NER14/M/44 rT4 FT and SF + UD . . . 36/DN15/M/41 rT1 FT − UD . . . 18/NER16/M/43 rT1 FT − UD . . . 18/NER17/F/40 rT3 FT + UD Flap necrosis 15/Died of carotid
artery blowout18/F/62 rT4 FT − UD . . . 18/NER
*FT indicates facial translocation; −, negative; +, positive; UD, undifferentiated carcinoma; ellipses, none; DLD, died of local disease; ST, subtemporal; NER, noevidence of recurrence; SF, subfrontal; DN, died of nodal disease; and WD, well-differentiated carcinoma.
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 128, JAN 2002 WWW.ARCHOTO.COM65
©2002 American Medical Association. All rights reserved. on December 6, 2011 www.archoto.comDownloaded from

TUMOR EXTENSION
The nasopharynx lies deep and central in the skull. Itsroof is the undersurface of the sphenoid sinus floor. Theposterior wall is separated from the basiocciput and cli-vus by the pharyngobasilar fasciae. The lateral wall of thenasopharynx consists of the torus tubarius, surroundedby the superior constrictor muscle, and is pierced by thesinus of Morgagni, in which pass the eustachian tube andtensor veli palatini muscle. The nasopharynx commu-nicates freely with the posterior nasal choanae. Naso-pharyngeal carcinoma is notorious for submucosal ex-tension. It commonly resides in the Rosenmuller fossaand may extend laterally through the sinus of Morgagnito invade the parapharyngeal space. Skull base exten-sion by destruction of the pterygoid base is common, andthe tumor may extend superiorly to involve the cavern-ous sinus or go laterally to involve the foramen ovale.The pharyngobasilar fasciae are tough fasciae and can bea strong barrier against tumor. In rare instances, NPC mayinvade these fasciae to involve the clivus.
With understanding of the anatomy of the naso-pharynx and the natural extension of NPC, nasophar-yngectomy can be accomplished by removing most of thenasopharyngeal mucosa, the ipsilateral torus tubarius, andthe medial pterygoid plate and its base by a nasoorbito-maxillary osteotomy. Further lateral extension necessi-tates a combined subtemporal approach. In our study,anterior craniofacial resection via a subfrontal approachwas carried out in patients with anterior cranial base tu-mors. The posterior half of the nasal septum was com-monly removed to gain access to the contralateral Rosen-muller fossa. Currently, the contraindications in ourdivision for salvage surgery for NPC are (1) extensive in-durated invasion, (2) cavernous sinus involvement, and(3) pharyngobasilar fasciae invasion. Preoperatively, mag-netic resonance imaging scans are the imaging methodsof choice to define the local extension of the primary re-currence,21 which is important for surgical planning. Mag-netic resonance imaging scans are also valuable in dif-ferentiating sinus invasion by cancer from obstructingsinusitis. Its excellent soft tissue resolution also revealscavernous sinus or foramen ovale involvement. Based onour experience with the first 2 patients in this series, com-puted tomographic scans are no longer used to define skullbase extensions.
En bloc resection of NPC is not always possible, and,as with other difficult lesions of the skull base, the re-section is often completed piece by piece. However, if thetumor is confined to the nasopharynx, en bloc resectioncan be easily accomplished by fracturing down the sphe-noid sinus floor, cutting the eustachian tube, removing
the medial pterygoid plate, and stripping the tumor offthe posterior pharyngobasilar fasciae. The resulting nudesurface of the nasopharyngeal space is left to reepitheli-alization, which takes about 3 months. During this time,diligent endoscopic cleansing and local hygiene main-tenance are crucial.
COMPLICATIONS
Four patients had postoperative complications, includ-ing 1 cerebrospinal fluid rhinorrhea, 1 flap necrosis, 1ORN of the translocated facial bone, and 1 mild epiphora.In the patient with ORN, a free facial bone graft tech-nique via a facial translocation approach was used. De-spite diligent sequestrectomies and hyperbaric oxygentherapy, the ORN persisted and the patient required afree flap to obliterate the paranasal cavity, thereby re-solving the ORN. Based on our experience with this pa-tient, we now use the vascularized facial bone graft tech-nique exclusively in facial translocation for patients whohave had previous radiotherapy.22
In the immediate postoperative period, patientsmay experience crust formation and accumulation in thehollow paranasal and nasopharyngeal cavities. Regular self-cleansing and irrigation with warm isotonic sodium chlo-ride solution are important to improve the condition.
Fee et al13 described 9 patients with primary recur-rence of NPC; 7 were treated for cure and 2 for palliation.Five of the 7 lived free of disease for 6 to 48 months. Theauthors concluded that surgery produced results as goodas those of reirradiation, if not better. In a follow-up study,Fee and colleagues23 reported that long-term survival (�3years) after surgical resection for recurrent NPC was pos-sible; however, salvage surgery had only slightly better re-sults than reirradiation. Wei et al16 described 26 patientswho underwent maxillary swing approaches to their na-sopharyngeal or paranasopharyngeal tumors, 18 of whichwere recurrent NPC. At 31⁄2 years after salvage surgery, 9were alive without disease, and the actuarial local controlof recurrent NPC was 42%. Hsu et al14 described 24 pa-tients with primary recurrence of NPC, in whom varioussurgical approaches were used based on the location andinvasion of NPC. In their series, 14 patients (58%) sur-vived after surgery during a median 18 months of follow-up. The authors postulated that cranial nerve invasionwas a surgical contraindication but that salvage surgery oth-erwise was a reasonable alternative to reirradiation. Kinget al24 recently described 31 patients with primary recur-rence of NPC, among whom 7 had cervical metastases inaddition to their primary recurrences, requiring nasophar-yngectomy and neck dissection. In their series, 9 patientshad tumor-positive margins, and there was no significantdifference in disease-free survival between them and pa-tients with clear surgical margins. The actuarial 5-year over-all survival was 47%, and the authors concluded that post-operative radiotherapy significantly enhanced survival andtumor control.
In our series, the actuarial 3-year survival of 57%and local control of 78% compared favorably with thoseof the other series. Postoperative radiotherapy was ad-ministered in only 7 patients (39%) who had tumor-positive or close surgical resection margins. Further-
Table 2. Two-Year Survival According to rT Stage
Stage No. of Patients Survival, %
rT1 8 87.5rT2b 1 100.0rT3 5 80.0rT4 4 50.0
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 128, JAN 2002 WWW.ARCHOTO.COM66
©2002 American Medical Association. All rights reserved. on December 6, 2011 www.archoto.comDownloaded from

more, we conclude that intracranial invasion is resectable.Superior dissection around the sphenoid sinus and ptery-goid base and lateral dissection around the foramen ovalethrough a combined anterior facial and superior neuro-surgical approach are crucial to control primary recur-rence of NPC with skull base invasion. In our series, weachieved local control in 4 of 5 patients with skull baseor intracranial involvement. With the concerted effortsof radiologists, radiation oncologists, head and neck sur-geons, and neurosurgeons, nasopharyngectomy can bea safe and oncologically sound approach to treatment ofprimary recurrence of NPC. Further effort should be di-rected to early detection of local recurrence by molecu-lar biology techniques.
Accepted for publication August 24, 2001.Presented at the Fifth International Conference on Head
and Neck Cancer, San Francisco, Calif, July 30, 2000.Corresponding author and reprints: Sheng-Po Hao, MD,
Department of Otolaryngology, Head & Neck Oncology (II),Chang Gung Memorial Hospital, Chang Gung University,5 Fu-Hsing St, Kuei Shan, 333, Taoyua, Taiwan, Republic ofChina (e-mail: [email protected]).
REFERENCES
1. Hausen HZ, Schulte-Holthausen H, Klein G, et al. EBV DNA in biopsies of Burkitttumours and anaplastic carcinomas of the nasopharynx. Nature. 1970;228:1056-1058.
2. Huang DP, Ho HC, Henle W, et al. Presence of EBNA in nasopharyngeal carci-noma and control patient tissues related to EBV serology. Int J Cancer. 1978;22:266-274.
3. Sobin LH, Wittekind C. TNM Classification of Malignant Tumors. 5th ed. NewYork, NY: John Wiley & Sons; 1997.
4. Chen YP, Tsang NM, Tseng CK, et al. Nasopharyngeal cancer registry in sixteenyears. Ther Radiol Oncol. 1996;3:233-237.
5. Cheng SH, Liu TW, Jian JJ, et al. Concomitant chemotherapy and radiotherapyfor locally advanced nasopharyngeal carcinoma. Cancer J Sci Am. 1997;3:100-106.
6. Wang CC. Re-irradiation of recurrent nasopharyngeal carcinoma: treatment tech-niques and results. Int J Radiat Oncol Biol Phys. 1987;13:953-956.
7. Lee AW, Foo W, Law SC, et al. Reirradiation for recurrent nasopharyngeal car-cinoma: factors affecting the therapeutic ratio and ways for improvement. Int JRadiat Oncol Biol Phys. 1997;28:43-52.
8. Teo PM, Kwan WH, Chan AT, et al. How successful is high-dose (�60 Gy) re-irradiation using mainly external beams in salvaging local failures of nasopha-ryngeal carcinoma? Int J Radiat Oncol Biol Phys. 1998;40:897-913.
9. Chua DT, Sham JS, Kwong DL, et al. Locally recurrent nasopharyngeal carci-noma: treatment results for patients with computed tomography assessment.Int J Radiat Oncol Biol Phys. 1998;41:379-386.
10. Lam KSL, Ho JHC, Lee AWM, et al. Symptomatic hypothalamic pituitary dys-function in nasopharyngeal carcinoma patients following radiation therapy: a ret-rospective study. Int J Radiat Oncol Biol Phys. 1987;13:1343-1350.
11. Lee AWM, Ng SH, Ho JHC, et al. Clinical diagnosis of late temporal lobe necro-sis following radiation therapy for nasopharyngeal carcinoma. Cancer. 1988;61:1535-1542.
12. Fisch U. The infratemporal fossa approach for nasopharyngeal tumors. Laryn-goscope. 1983;93:36-44.
13. Fee WE, Gilmer PA, Goffinet DR. Surgical management of recurrent nasopha-ryngeal carcinoma after radiation failure at the primary site. Laryngoscope. 1988;98:1220-1226.
14. Hsu MM, Ko JY, Sheen TS, et al. Salvage surgery for recurrent nasopharyngealcarcinoma. Arch Otolaryngol Head Neck Surg. 1997;123:305-309.
15. Wei WI, Lam KH, Sham JST. New approach to the nasopharynx: the maxillaryswing approach. Head Neck. 1991;13:200-207.
16. Wei WI, Ho CM, Yuen PW, et al. Maxillary swing approach for resection of tu-mors in and around the nasopharynx. Arch Otolaryngol Head Neck Surg. 1995;121:638-642.
17. Janecka IP, Sen CN, Sekhar LN, Arriaga M. Facial translocation: new approachto cranial base. Otolaryngol Head Neck Surg. 1990;103:413-419.
18. Janecka IP, Nuss DW, Sen CN. Facial translocation approach to the cranial base.Acta Neurochir Suppl (Wien). 1991;53:193-198.
19. Sekhar LN, Janecka IP, Jones NF. Subtemporal-infratemporal and basal sub-frontal approach to extensive cranial base tumours. Acta Neurochir (Wien). 1988;92:83-92.
20. Hao SP, Tsang NM, Chang KP. Differentiation of recurrent nasopharyngeal car-cinoma and skull base osteoradionecrosis by Epstein-Barr virus–derived latentmembrane protein-1 gene. Laryngoscope. 2001;111:650-652.
21. Ng SH, Chang JT, Ko SF, et al. MRI in recurrent nasopharyngeal carcinoma. Neu-roradiology. 1999;41:855-862.
22. Hao SP. Facial translocation approach to the skull base: the viability of translo-cated facial bone graft. Otolaryngol Head Neck Surg. 2001;124:292-296.
23. Fee WE, Roberson JB, Goffinet DR. Long-term survival after surgical resectionfor recurrent nasopharyngeal cancer after radiotherapy failure. Arch Otolaryn-gol Head Neck Surg. 1991;117:1233-1236.
24. King WWK, Ku PKM, Mok C, Teo PML. Nasopharyngectomy in the treatmentof recurrent nasopharyngeal carcinoma: a twelve-year experience. Head Neck.2000;22:215-222.
(REPRINTED) ARCH OTOLARYNGOL HEAD NECK SURG/ VOL 128, JAN 2002 WWW.ARCHOTO.COM67
©2002 American Medical Association. All rights reserved. on December 6, 2011 www.archoto.comDownloaded from