Embed Size (px)
Citation preview

20 Aging Clin Exp Res, Vol. 18, No. 1
Key words: Elderly, orthostatic hypotension, summer, winter.Correspondence: E. Grossman, MD, Head, Internal Medicine D and Hypertension Unit, The Chaim Sheba Medical Center, Tel Hashomer52621, Israel.E-mail: [email protected] July 19, 2004; accepted in revised form January 4, 2005.
ABSTRACT. Background and aims: Orthostatic hy-potension (OH) is a common finding among older pa-tients. It has been shown that blood pressure (BP) islower in summer than in winter. The aim of this studywas to examine whether OH varies between seasons inthe elderly population. Methods: Five hundred and twoinpatients (241 males, 261 females) of mean age 81.6years were included in the study; 253 were studied insummer and 166 in winter. Orthostatic tests were per-formed 3 times daily, 30 minutes after meals. Ortho-static hypotension was defined as a decrease of atleast 20 mmHg in systolic BP and/or 10 mmHg in di-astolic BP upon assuming an upright posture at leasttwice during the day. Results: OH was documented in107 patients (34.8%). Initial BP did not differ betweenseasons (147.6±24.6/72.6±14.5 mmHg in summer,146.7±23.4/71.5±13.4 mmHg in winter). However,the orthostatic drop in BP in the morning was greaterin summer (–8.4/–2.8 mmHg vs –4.3/+0.2 mmHg inwinter; p<0.05). OH was also more prevalent in sum-mer than in winter (37.9 vs 27.1%; p=0.02). After ad-justment for all confounders, the risk of experiencingOH in summer was 64% higher than in winter [ad-justed odds ratio (OR) 1.64 [95% Confidence Interval(CI) 1.03-2.61]. Conclusions: The prevalence of OH ishigher in summer than winter. Thus, more attentionshould be paid to the diagnosis of OH in summer.(Aging Clin Exp Res 2006; 18: 20-24)©2006, Editrice Kurtis
INTRODUCTIONOrthostatic hypotension (OH) is a relatively common
finding among the elderly, occurring in 5 to 50% of pa-tients (1, 2). Patients with OH have difficulties walking, aremore susceptible to falls, experience more frequent dizzi-ness and syncope, have decreased quality of life, and may
Seasonal changes in orthostatic hypotension amongelderly admitted patientsAvraham Weiss1, Yichayaou Beloosesky1, Joseph Grinblat1, and Ehud Grossman2
1Geriatric Department, Rabin Medical Center, Beilinson Campus, Petah Tiqva, and 2Department of InternalMedicine D and Hypertension Unit, The Chaim Sheba Medical Center, Tel Hashomer, both affiliated to theSackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
have a higher mortality rate (3, 4). Because of age-relat-ed physiological changes in the cardiovascular systemand a blunted response to the recruitment of the sym-pathetic nervous system, older people tend to be more vul-nerable to orthostatic stress than younger ones (5).
We recently studied the prevalence and consistency ofOH in elderly hospitalized patients. In that study, in whichdata collection lasted two years, we found a high rate ofOH (6). It is unknown whether the prevalence of OH isthe same throughout the year. Many studies have shownthat blood pressure (BP) is lower during summer than win-ter (7-14). However, only a few studies have investigatedthe effect of seasons on the prevalence of OH (15-18).The possible effect of weather on OH led us to re-evalu-ate our data according to season.
Therefore, the aim of the present study was to determinethe influence of hot weather on the prevalence of OH.
PATIENTS AND METHODSDuring a 2-year period (1999-2000), 1852 patients
were admitted to our acute 25-bed geriatric ward. Ofthese, 502 patients were selected and enrolled in thisstudy.
Patients were included in the study if they were at least60 years old, able to get out of bed alone or with minorassistance, and stand up for at least 5 minutes. Severelydemented and/or disabled patients, or those who, formedical reasons, could not stand up temporarily or werepermanently bedridden, were excluded from the study.
Blood pressure measurementsBlood pressure (BP) and heart rate were measured with
the Vital Signs Monitor (52 NTP model, Welch Allyn Pro-tocol, Inc., Beaverton, OR, USA), which was checked ev-ery day for accuracy against a mercury sphygmo-manometer. Measurements were taken in the supine
Aging Clinical and Experimental Research

Aging Clin Exp Res 18: 20-24, 2006©2006, Editrice Kurtis
and standing positions 30 minutes after meals 3 times, onthe same day: between 8:00 and 9:00 after breakfast; be-tween 13:00 and 14:00 after lunch; and between 17:00and 18:00 after supper.
Because of technical problems only two sets of mea-surements were obtained in 13 patients, and they were ex-cluded from some of the analyses.
In the supine position, BP was measured in the left armafter at least 5 minutes of complete bed rest. In the up-right position, BP was measured after 2 minutes ofstanding. To ensure accuracy, particular care was taken tokeep the patient’s hand extended. Measurements weretaken twice in each position, 1 minute apart, and the av-erage of the two measurements was recorded.
Orthostatic hypotension was defined as a decreaseof at least 20 mmHg in systolic BP (SBP) and/or 10mmHg in diastolic BP (DBP) upon assuming an uprightposture, at least twice during the day.
Data collectionThe following variables were recorded for each pa-
tient: age, height, weight, body mass index, ethnicity ororigin, reason for admission, diagnoses, and main drugsused. We also noted laboratory results of completeblood cell count and serum levels of glucose, urea, cre-atinine, sodium, potassium, thyrotropin, vitamin B12,and folic acid, and the exact date on which the testswere done.
Meteorologic data were collected from the Israeli Me-teorological Service (IMS), Ministry of Transportation,Beit Dagan, Tel Aviv.
Statistical analysisWe analyzed the prevalence of OH and the magnitude
of orthostatic BP changes each month of the year. Then,for summer, we combined the data for the months withthe highest ambient temperatures (May through Septem-ber) and, for winter, the months with the lowest tem-peratures (December through March). The average out-door temperature in summer was 25.45ºC (average mul-ti-annual outdoor temperature of the corresponding periodin 1964-1979 was 23.46ºC), and the average outdoortemperature in winter was 13.75ºC (average multi-annualoutdoor temperature of the corresponding period in1964-1979 was 13.53ºC).
Results are reported as means±SD. The data of the BPdrop fitted a normal distribution and therefore Student’st-test was used to calculate the differences in the magni-tude of orthostatic BP changes between hot and cold sea-sons. The magnitude of drop was analyzed separately formorning, afternoon and evening. The difference in preva-lence of OH between seasons was tested by chi-squareanalysis. The Mantel-Haenszel test and logistic regressionwere used to assess the effect of sex, treatment, renalfunction, hemoglobin and associated diseases on theseasonal prevalence of OH. Values of p<0.05 were con-sidered significant.
RESULTSPatient characteristicsThe study populations included 502 patients, 241
male and 261 female, of mean age 81.6 years. Duringthe study, 253 patients (125 men, 128 women) were eval-
Seasonability in orthostatic hypotension
Aging Clin Exp Res, Vol. 18, No. 1 21
Table 1 - Patient characteristics.
Characteristics Summer (n=253) Winter (n=166) p-valueMean±SD Mean±SD
Age (yrs) 81.4±6.7 81.8±6.9 0.9Gender (M/F) 125/128 78/88BMI (kg/m2) 25.5±4.6 24.9±4.3 0.2Supine morning SBP (mmHg) 147.6±24.6 146.7±23.4 0.71Supine morning DBP (mmHg) 72.6±14.5 71.5±13.41 0.41Supine morning HR (beats/min) 75.1±13.8 78.5±13.8 0.03
Comorbid diseasesHypertension 166 (66%) 104 (63%) 0.6Ischemic heart disease 140 (56%) 90 (55%) 0.8Stroke 80 (32%) 53 (32%) 0.91Congestive heart failure 82 (32%) 51 (31%) 0.73Diabetes mellitus 67 (26%) 54 (33%) 0.17Chronic lung disease 59 (23%) 35 (31%) 0.61Parkinson’s disease 29 (11%) 23 (14%) 0.45
Medicine useDiuretics 95 (38%) 51 (31%) 0.15ACE inhibitors 87 (34%) 50 (30%) 0.36Calcium antagonists 66 (26%) 51 (31%) 0.3Nitrates 65 (26%) 49 (30%) 0.4β-blockers 47 (19%) 28 (17%) 0.66Sleeping pills 70 (28%) 42 (25%) 0.6

Aging Clin Exp Res 18: 20-24, 2006©2006, Editrice Kurtis
uated in summer and 166 (78 men, 88 women) in winter.The initial supine BP did not differ between seasons(147.6±24.6/72.6±14.5 mmHg in summer and146.7±23.4/71.5±13.4 mmHg in winter), but heartrate was faster during winter than summer (p=0.03).Other baseline characteristics were similar between pa-tients evaluated in summer and winter (Table 1).
Seasonal orthostatic blood pressure and heartrate changesThe orthostatic drop in BP was more pronounced in
summer than in winter, but the difference was significantonly in the morning (Table 2). Postural systolic BP fell by8.4±22.2 mmHg in summer and by 4.3±19.6 mmHg inwinter (p=0.05); diastolic BP fell by 2.8±12.8 mmHg insummer and increased by 0.2±13.9 mmHg in winter(p=0.03).
Postural heart rate increased to the same extent in sum-mer and winter (Table 2).
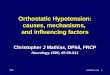
Prevalence of OH during the yearThe rate of OH was higher during the summer months
(Fig. 1). Ninety-six of the 253 patients (37.9%) experi-enced OH during summer, and only 45 of 166 (27.1%)did so in winter (p=0.02). The trend for the higher preva-lence of OH in summer was the same in both sexes(Table 3). The risk of experiencing OH was not affectedby age, sex, diabetes mellitus, extrapyramidal syndromes,chronic renal failure, or use of β-blockers or diuretics[for diuretic users, the odds ratio (OR) was 0.746 (95%confidence interval (CI) 0.46-1.2, p=0.23]. The risk of ex-periencing OH was higher in smokers (OR 2.27; 95% CI1.29-3.99, p=0.005), and patients treated with α-block-ers (OR 2.09; 95% CI 1.08-4.06, p=0.03) and those us-ing antidiabetic agents (OR 2.46; 95% CI 1.25-4.45,p=0.008). It was lower in patients with orthopedic dis-eases (OR 0.57; 95% CI 0.34-0.94, p=0.03), and inthose using anti-arrhythmic agents (OR 0.37; 95% CI0.17-0.80, p=0.01) or steroids (OR 0.08; 95% CI 0.01-0.66, p=0.02). The higher prevalence of OH in summerremained significant after adjustment for diseases, medi-cations and hydration status. The adjusted OR of expe-riencing OH in summer vs winter was 1.64 (95% CI1.03-2.61, p=0.04).
DISCUSSIONOrthostatic hypotension is a common disorder in the
elderly (1, 2). In the present study we showed that, in el-derly hospitalized patients, OH is more common in sum-mer than in winter. On the basis of our previous experi-ence showing that the consistency of OH is low (6), in thepresent study, patients were categorized as having OH on-ly when it was observed at least twice during the day. Totest seasonal variations of OH, we chose for summer the5 months with the highest ambient temperature in Israeland, for winter, the 4 months with the lowest tempera-ture. Even so, the difference in average outdoor tem-perature between the seasons was moderate (12.7ºC).The choice of “hot” and “cold” seasons is usually influ-enced by the actual climate conditions in the research areaand may differ in various studies (19, 20).
Several investigators have suggested that elevated BPlevels in winter may explain the increased cardiovascular
A. Weiss, Y. Beloosesky, J. Grinblat, et al.
22 Aging Clin Exp Res, Vol. 18, No. 1
Table 2 - Orthostatic changes in blood pressure (mmHg) andheart rate (beats/min) during the day in summer and winter.
Summer Winter p-value
MorningChange in SBP –8.4±22.2 –4.3±19.6 0.05Change in DBP –2.8±12.8 +0.2±13.9 0.03Change in HR +9.9±9.8 +9.8±8.6 0.85
AfternoonChange in SBP –8.6±21.6 –6.9±19.4 0.4Change in DBP –4.3±14.2 –2.6±13.4 0.23Change in HR +8.7±9.9 +10.0±10.1 0.23
EveningChange in SBP –3.9±20.6 –0.3±19.6 0.08Change in DBP +0.8±16.0 +0.5±17.9 0.9Change in HR +7.8±10.2 +7.3±10.2 0.61
SBP= systolic blood pressure; DBP= diastolic blood pressure; HR= heart rate.
Table 3 - Prevalence of OH in males and females in summer andwinter.
Summer Winter p-value
Whole group (n) 253 166Patients with OH (%) 96 (37.9) 45 (27.1) 0.02
Males (n) 125 78Patients with OH (%) 52 (41.6) 25 (32.1) 0.17
Females (n) 128 88Patients with OH (%) 44 (34.4) 20 (22.7) 0.07
SummerWinter
Males Females
70
60
50
40
30
20
10
0Dec Jan Feb Mar Apr May June July Aug Sep Oct Nov
% of OH
Month
Fig. 1 - Monthly prevalence of orthostatic hypotension (OH) inmales and females.

Aging Clin Exp Res 18: 20-24, 2006©2006, Editrice Kurtis
morbidity and mortality during this season (21-26). How-ever, we did not observe a difference in baseline supineBP values between seasons, perhaps owing to the mod-erate temperature variation between seasons in Israel. Inaddition, unlike some of the other studies (7, 27-34), weincluded only elderly hospitalized patients who are less ex-posed to outdoor temperatures, and measured supine BP.We observed a faster supine heart rate in winter, whichmay indicate increased sympathetic activity. It cannotbe attributed to medication, because the use of β-blockerswas similar during the seasons. Despite the similar sea-sonal supine BP levels, we observed a greater decrease inorthostatic BP in summer. Moreover, the prevalencewas higher in both sexes in summer than winter. It is note-worthy that the greater drop in summer occurred mainlyin the morning. This difference may reflect volume con-traction due to fluid and salt loss during warm summernights and lack of water replacement through drinking dur-ing sleep. In the daytime, patients were able to replacetheir salt and fluid loss, so that seasonal differences in or-thostatic BP were less pronounced. Not all investigatorsfound a higher rate of OH in summer. Ryynanen et al.(17) reported no excess OH rate in persons 75 years andolder by time of day or month. However, others showedfindings in line with ours (15, 16). Verdon et al. (15) fol-lowed 80 patients of mean age 65±13 years for one yearand noted a greater orthostatic fall in summer than in win-ter, and also more episodes of OH by both the classic def-inition and symptoms (15). Diabetic patients and pa-tients treated with diuretics and vasodilators were partic-ularly vulnerable to OH, whereas those on β-blockerswere less vulnerable to OH in summer (15).
In a more recent study, the same authors studied 219chronically ill, stable, mostly ambulatory patients, and20 normal subjects. They found more orthostatic symp-toms in summer than winter, and a greater decrease in BPin the upright position in summer, especially amongwomen (16). However, they defined OH according to oneobservation (16) but, as OH is not consistent (2, 6, 35,36), this limitation may lead to overdiagnosis. We there-fore performed orthostatic tests three times during thesame day, and categorized patients as having OH onlywhen it occurred at least twice during one day. Thus, ourlarge study, using a rigid definition of OH, confirms theobservation of the higher prevalence of OH in summer.Unlike Verdon et al. (15), we did not observe any effect ofdiuretics or β-blockers on the rate of OH in summer. Nordid Minami et al. observe any effects of medication or dis-ease on seasonal BP variations (24).
Why OH is more prevalent in elderly patients duringsummer is unknown, but several mechanisms may be in-volved in this phenomenon. Hypovolemia due to excesssweating and salt and fluid loss without enough fluid in-take may impair the counteractive mechanism thatmaintains BP upon standing. This mechanism was un-
likely in our patients, since the seasonal difference in therate of OH remained significant after adjustment tohydration parameters such as blood urea andhemoglobin. Alternatively, peripheral vasodilatation inresponse to high ambient temperature may impair theability to cope with orthostatic stress (37). This mecha-nism may be particularly important in elderly patients,who are already more vulnerable to orthostatic stress be-cause of physiologic changes in the cardiovascular sys-tem and a blunted response to the recruitment of thesympathetic system (5, 38).
One limitation of our study is that we included only in-patients and our findings may not therefore represent thegeneral elderly population.
In view of the greater tendency of older persons to OHin summer, clinicians should direct special attention to thediagnosis of OH during hot seasons and educate pa-tients in avoiding this risk.
REFERENCES1. Raiha I, Luutonen S, Piha J, Seppanen A, Toikka T, Sourander
L. Prevalence, predisposing factors, and prognostic importanceof postural hypotension. Arch Intern Med 1995; 155: 930-5.
2. Puisieux F, Boumbar Y, Bulckaen H, Bonnin E, Houssin F, De-vailly P. Intraindividual variability in orthostatic blood pressurechanges among older adults: the influence of meals. J Am Geri-atr Soc 1999; 47: 1332-6.
3. Carlson JE. Assessment of orthostatic blood pressure: measure-ment technique and clinical applications. South Med J 1999; 92:167-73.
4. Luukinen H, Koski K, Laippala P, Kivela SL. Prognosis of dias-tolic and systolic orthostatic hypotension in older persons. ArchIntern Med 1999; 159: 273-80.
5. Lipsitz LA. Orthostatic hypotension in the elderly. N Engl JMed 1989; 321: 952-7.
6. Weiss A, Grossman E, Beloosesky Y, Grinblat J. Orthostatichypotension in acute geriatric ward: is it a consistent finding?Arch Intern Med 2002; 162: 2369-74.
7. Kristal-Boneh E, Harari G, Green MS, Ribak J. Body mass indexis associated with differential seasonal changes in ambulatory bloodpressure levels. Am J Hypertens 1996; 9: 1179-85.
8. Brennan PJ, Greenberg G, Miall WE, Thompson SG. Seasonalvariation in arterial blood pressure. BMJ 1982; 285: 919-23.
9. Hata T, Ogihara T, Maruyama A, et al. The seasonal variation ofblood pressure in patients with essential hypertension. Clin ExpHypertens 1982; 4: 341-54.
10. Nayha S. Adjustment of blood pressure data by season. Scand JPrim Health Care 1985; 3: 99-105.
11. Sharma BK, Sagar S, Sood GK, Varma S, Kalra OP. Seasonalvariations of arterial blood pressure in normotensive and essen-tial hypertensives. Indian Heart J 1990; 42: 66-72.
12. Giaconi S, Palombo C, Genovesi-Ebert A, Marabotti C, VolterraniD, Ghione S. Long-term reproducibility and evaluation of seasonalinfluences on blood pressure monitoring. J Hypertens (Suppl)1988; 6: S64-6.
13. Giaconi S, Ghione S, Palombo C, et al. Seasonal influences onblood pressure in high normal to mild hypertensive range. Hy-pertension 1989; 14: 22-7.
14. Kunes J, Tremblay J, Bellavance F, Hamet P. Influence of envi-
Seasonability in orthostatic hypotension
Aging Clin Exp Res, Vol. 18, No. 1 23

Aging Clin Exp Res 18: 20-24, 2006©2006, Editrice Kurtis
ronmental temperature on the blood pressure of hypertensive pa-tients in Montreal. Am J Hypertens 1991; 4: 422-6.
15. Verdon F, Boudry JF, Chuat M, Studer JP, Truong CB, Jacot E.Seasonal variations in arterial pressure in hypertensive patients.Schweiz Med Wochenschr 1993; 123: 2363-9.
16. Verdon F, Jacot E, Boudry JF, Chuat M, Truong CB, Studer JP.Seasonal variations of blood pressure in normal subjects and pa-tients with chronic disease. Arch Mal Coeur Vaiss 1997; 90:1239-46.
17. Ryynanen OP, Kivela SL, Honkanen R. Times, places, andmechanisms of falls among the elderly. Z Gerontol 1991; 24:154-61.
18. Kallman H. Protecting your elderly patients from winter’s cold.Geriatrics 1985; 40: 69-72, 77, 81.
19. James GD, Yee LS, Pickering TG. Winter-summer differences inthe effects of emotion, posture and place of measurement onblood pressure. Soc Sci Med 1990; 31: 1213-7.
20. Prasad GV, Nash MM, Zaltzman JS. Seasonal variation in out-patient blood pressure in stable renal transplant recipients. Trans-plantation 2001; 72: 1792-4.
21. Tanaka S, Konno A, Hashimoto A, et al. The influence of coldtemperatures on the progression of hypertension: an epidemio-logical study. J Hypertens Suppl 1989; 7: S49-51.
22. Fujiwara T, Kawamura M, Nakajima J, Adachi T, Hiramori K.Seasonal differences in diurnal blood pressure of hypertensive pa-tients living in a stable environmental temperature. J Hypertens1995; 13: 1749-52.
23. Winnicki M, Canali C, Accurso V, Dorigatti F, Giovinazzo P, Pala-tini P. Relation of 24-hour ambulatory blood pressure and short-term blood pressure variability to seasonal changes in environ-mental temperature in stage I hypertensive subjects. Results of theHarvest Trial. Clin Exp Hypertens 1996; 18: 995-1012.
24. Minami J, Kawano Y, Ishimitsu T, Yoshimi H, Takishita S. Sea-sonal variations in office, home and 24 h ambulatory bloodpressure in patients with essential hypertension. J Hypertens1996; 14: 1421-5.
25. Woodhouse PR, Khaw KT, Plummer M. Seasonal variations ofblood pressure and its relationship to ambient temperature in anelderly population. J Hypertens 1993; 11: 1267-74.
26. Cordioli E, Pizzi C, Martinelli M. Winter mortality in Emilia-Ro-magna, Italy. Int J Circumpolar Health 2000; 59: 164-9.
27. Kristal-Boneh E, Harari G, Green MS, Ribak J. Summer-wintervariation in 24 h ambulatory blood pressure. Blood Press Monit1996; 1: 87-94.
28. Kristal-Boneh E, Harari G, Green MS, Ribak J. Seasonal changesin ambulatory blood pressure in employees under different outdoortemperatures. Occup Environ Med 1995; 52: 715-21.
29. Kristal-Boneh E, Harari G, Green MS. Seasonal change in 24-hour blood pressure and heart rate is greater among smokers thannonsmokers. Hypertension 1997; 30: 436-41.
30. Jansen PM, Leineweber MJ, Thien T. The effect of a change inambient temperature on blood pressure in normotensives. JHum Hypertens 2001; 15: 113-7.
31. Kristal-Boneh E, Froom P, Harari G, Silber H, Ribak J. Exerciseblood pressure changes between seasons. Blood Press Monit1997; 2: 223-7.
32. Raven PB, Niki I, Dahms TE, Horvath SM. Compensatory car-diovascular responses during an environmental cold stress, 5degrees C. J Appl Physiol 1970; 29: 417-21.
33. Raven PB, Wilkerson JE, Horvath SM, Bolduan NW. Thermal,metabolic, and cardiovascular responses to various degrees of coldstress. Can J Physiol Pharmacol 1975; 53: 293-8.
34. Tsuchihashi T, Uezono K, Abe I, Matsuoka M, Kawasaki T.Seasonal variation in 24-h blood pressure pattern of young nor-motensive women. Hypertens Res 1995; 18: 209-14.
35. Belmin J, Abderrhamane M, Medjahed S, et al. Variability ofblood pressure response to orthostatism and reproducibility of thediagnosis of orthostatic hypotension in elderly subjects. J Geron-tol 2000; 55: M667-71.
36. Ooi WL, Barrett S, Hossain M, Kelley-Gagnon M, Lipsitz LA. Pat-terns of orthostatic blood pressure change and their clinical cor-relates in a frail, elderly population. JAMA 1997; 277: 1299-304.
37. Wilson TE, Cui J, Zhang R, Witkowski S, Crandall CG. Skincooling maintains cerebral blood flow velocity and orthostatic tol-erance during tilting in heated humans. J Appl Physiol 2002;93: 85-91.
38. Mader SL. Aging and postural hypotension. An update. J AmGeriatr Soc 1989; 37: 129-37.
A. Weiss, Y. Beloosesky, J. Grinblat, et al.
24 Aging Clin Exp Res, Vol. 18, No. 1