Embed Size (px)
Citation preview

Sanitation and Hygiene Promotion – Programming Guidance 63
SECTION FOUR:PROGRAMMING FOR BETTER IMPLEMENTATION
This section focuses on the challenges of working with communities and households, hygiene pro-motion and selection and marketing of sanitation technologies. The practical implications ofadopting a new approach which focuses on household behaviour change and investment, are sig-nificant and will be briefly reviewed here. It is not the intention of this section to provide detailedguidance on project level implementation but rather to highlight where the realities of workingat the local level with households and communities, can impact on programmatic decisions. Byreviewing what is now known about working effectively at this level the recommendations of Sec-tion Three can be seen in their right context. Chapter 8 discusses the implications of the new approach in terms of how front-line units needto interact with both households and communities. The types of tools and resources they needto do this effectively are briefly discussed. Chapter 9 briefly introduces some approaches toHygiene Promotion – what is currently known about how to make it effective and how to or-ganize it so that it achieves the maximum possible impact are also covered. Chapter 10 talksabout how to select and market technologies. For detailed implementation guidance the readeris directed to other sources; the information presented here is intended as an introduction forthose professionals who do not have experience or knowledge about what has been learnedabout effecting sanitation and hygiene promotion and also to stimulate sector professionals tothink about the wider programming implications of what is known in the field.
The shift away from public construction of latrines to amore complete approach to sanitation and hygiene pro-motion places the household at the centre of decisionmaking. But it also implies a strong role for the commu-nity in planning and management of interventions. Whilemany of the needed changes will happen at the house-hold level, in some contexts some decisions and actionsmay need to be taken collectively by the community.Such shared action may relate to:
● local decision making about the most appropriaterange of sanitation solutions (communities may needto decide whether they are willing and able to man-
age shared facilities or whether they can all afford toinvest in private household facilities);
● local management and oversight of the household ac-tions as they relate to the communal environment(preventing discharge of household excreta in publicplaces for example);
● management of solid wastes, sullage and storm waterdrainage;
● management and financing for operation and mainte-nance of facilities which impact on the shared envi-ronment (this may include operation of shared facili-ties such as drains, but might also include a sharedcommitment to support maintenance and operation
8.1 The different roles for communities and households
Chapter 8 Working with Communities and Households

Sanitation and Hygiene Promotion – Programming Guidance64
of household facilities such as latrines); and● organisation of joint action to lobby service providers
to perform at the margins of the community (for ex-ample, creating pressure for a utility service providerto operate and manage trunk sewers in an urban con-text, or lobbying for public support to regional oper-ation and maintenance service providers).
There are a range of approaches to management ofshared or community facilities including:
● direct community management through elected orappointed committees or other groups;
● delegated management to a trained member or mem-bers of the community;
● delegated management to a professional voluntary,private or public service provider.
Depending on the context (including whether the com-munity exists in a rural or urban environment, and thetype of technologies which are feasible) each communi-ty needs to work out the best way to approach issues ofshared responsibility.
8.2 Building capacity at the community levelWhile there are often clear advantages to collective com-munity action in sanitation and hygiene promotion, it isoften challenging to provide the right sort of support toenable communities to reach their full potential in thesenew roles. As well as the need to build up specific skills(such as planning or book-keeping), communities mayneed support to overcome entrenched biases and inter-
nal conflicts, or they may need support as they begin toengage with other local institutions (such as local gov-ernment bodies, field units of technical agencies, bankers,shop keepers, private suppliers of goods and servicesetc). Capacity building needs at this level will vary enor-mously, but will need to be addressed (planned for, fi-nanced, staffed and implemented), if collective action isto be successful.
8.3 Communicating EffectivelyTo achieve the vision of placing communities and house-holds at the centre of behavour change, service providersand other support agencies have primarily to become ex-pert at communication. Programmers may consider thatthe objective of working with the community is to:
● promote changes in hygiene behaviours;● market and deliver sanitation technologies; and ● build systems of community management.
However, communities and households may have differ-ence perspectives, and see a sanitation and hygiene pro-motion programme as an opportunity to engage with awider social development process. It may often bepreferable to organize work in the community in this
way, so that a range of social objectives can be achievedby the community, with the proper priority placed oneach.
Communication also has to be two-way because each ofthe areas of intervention above involve decisions tochange how things are done within the house and with-in the community. Facilitators of hygiene improvementwill not be able influence these decisions without a thor-ough understanding of the environment and contextswithin which they will be taken. Households and com-munities have much to offer programmers in terms ofproviding the keys which enable changes to take placethrough joint effort.
Sanitation and Hygiene Promotion – Programming Guidance 65
SECTION FOUR: PROGRAMMING FOR BETTER IMPLEMENTATION
Chapter 8: Working with Communities and Households
8.5 The Tools
Having identified the available resources and agreed onthe objectives of community level interventions, gener-ic tools and approaches can be selected and modified foruse in the specific context under consideration. Thetools commonly used in the water supply and sanitationsector include a full range from participatory planningand monitoring through to advertising and the use ofmass media (see Reference Box 13).
8.4 Selecting Community Level Tools
The type of community level interventions required willbe determined by a range of factors. These include:
● the types of behaviour that are to bechanged: for example where unhygienic practicesare deeply entrenched in cultural norms a more in-tensive hygiene promotion programme would beneeded as compared to a situation where personal hy-giene is good but sanitary facilities are lacking – in thiscase more emphasis might be placed on marketingsanitation goods;
● the magnitude of the problem and levels ofawareness: for example where the situation is verypoor and people are already aware of its impact onhealth, there will be more focus on facilitating changedbehaviours, whereas where awareness is low, thefocus will be much more on promoting awareness ofpreviously unknown risks;
● the nature of the communities (rural/ urban)and technologies likely to be used: for examplein scattered rural communities where on-site tech-nologies have been identified as appropriate, theremay be less need for up front mobilization of com-munity “organisation” for their installation than indense urban communities electing to use communallatrines or condominial sewers. Conversely, in thefirst case, more work may be needed to help the com-munity establish a viable long-term system for pit emp-tying and management of wastes, than would beneeded in an urban community using condominialsewers emptying into a working main sewer line;
● the institutional environment: for examplewhere the small scale private sector is likely to be a
key provider of services, marketing and local supportskills may derive from them, and additional communi-ty level interventions may not be required. Impor-tantly, where hygiene promotion is emphasized theremay need to be stronger involvement of health staffand a shift in roles for staff from technical water sup-ply and sanitation agencies;
● the skills available amongst field-workers lo-cally: what skills do field-workers (who may be lo-cated in government departments, NGOs or local or-ganisations) already possess, and what skills do theyhave the potential to learn;
● the nature of existing local organisations: vil-lage development committees, savings groups, wateruser and tapstand committees, handpump/waterpointcaretakers and mechanics, agricultural and forestrygroups, population and health committees alreadyabound, and sometimes their number and demandstax a community’s time and resources. Some of thesegroups could usefully place a priority on hygiene andsanitation. Linking into existing credit groups mayprove a valuable means to channel credit and subsi-dies for sanitation—and ensure equity as well as ac-countability—without creating a separate effort; and
● the availability of funds to support communi-ty level interventions: resources will ultimately de-termine what interventions can be used at what in-tensity for how long. In general local participatory ap-proaches will have higher costs than remote, massmedia type approaches but are likely to be an essen-tial element in achieving real change at the householdlevel.
Participatory Techniquesi
A range of participatory tools/techniques can be used inhygiene improvement programmes. Commonly usedtools include focus group discussions, neighbourhood so-cial mapping; transect walks; and household/school hy-giene self surveys.

Sanitation and Hygiene Promotion – Programming Guidance66
Participatory Rural Appraisal (PRA), is a gener-alized description for a wide range of techniques espe-cially aimed at involving community members in decision-making and self-assessment and in the development ofstakeholder partnerships. PRA evolved through a simpli-fication of conventional techniques for data collectionand analysis. Community action planning, which requiresactive roles by community members, is well served byPRA techniques such as mapping of local problems andresources, wealth ranking, and similar tools. The “PRA”philosophy informs much of the thinking about partici-patory techniques in the sector and has been translatedinto a wide variety of contexts including urban slums.Many of the elements described above have been refinedfor the use of the water supply and sanitation sector andthe three the most commonly used combined ap-proaches are:
● PHAST (Participatory Hygiene and Sanitation Trans-formation) which was developed in Eastern andSouthern Africa in the mid-late 1990s. PHAST toolk-its can be used at the local level to bring about be-havioural changes in hygiene and sanitation.
● SARAR (Self-esteem, Associative strength, Respon-sibility, Action planning, and Resourcefulness) stimu-lates involvement in community-based activities of allkinds, not only by the more prestigious and articulateparticipants (such as community leaders or seriousstaff), but also by the less powerful, including the non-literate community members. SARAR is widely usedin participatory water, hygiene, and sanitation pro-grammes;
● Methodology for Participatory Appraisal(MPA) a selection of participatory techniques whichhave been refined and assembled for the participato-ry appraisal of projects and programmes.
Schools and Education systemsUse of schools, parent-teacher associations and childrenthemselves, are increasingly recognised as powerful toolsin promoting changed behaviours and greater awarenessof hygiene issues. These channels, and specialized toolsto utilize them, can be a key component in a communi-cation programme.
Mass Media and Advertising The use of mass media, and straight forward advertisingcan also play a role in hygiene improvement. These di-dactic interventions emphasize transmittal of messages topromote awareness, market products and transferknowledge. When used well these approaches can playan important role in overall behaviour change but shouldusually be used in tandem with more intensive local mar-keting techniques.
MarketingMarketing in the water supply and sanitation sectors haslong revolved around “social marketing” – where a rangeof tools are used in combination to target specific be-haviours such as hygienic practices or the use of a par-ticular technology. Once it is recognized that the mosteffective interventions in sanitation may be achievedthrough development of a viable sanitation business,marketing may become a major element of a hygiene im-provement programme. New approaches which linkcommercial marketing of goods and services at the locallevel, with national awareness campaigns and hygienepromotion programmes, may be effective in stimulatingthe demand-side of the market. The challenge will ofcourse be to match this demand-side support with suit-able approaches to build up the supply-side business toensure a ready supply of effective and appropriate goodsand services.
8.6 Scaling Up
Scaling up successful experiences of working with com-munities is notoriously difficult. By its very nature thistype of work is resource intensive – it requires a rangeof specialist skills, time and energy to build up real man-agement capacity within most communities in a new andchallenging field such as the management of sanitation.Most practitioners emphasise the need for a slow and
steady approach. This seems to contradict the urgentneed to scale up this type of work and roll it out to anincreasing number of communities. Furthermore, thetask may become progressively harder as the most chal-lenging (remote, poor, socially divided or technological-ly challenging) communities are likely to be left to thelast. Programmers can be proactive in ensuring that suc-

Sanitation and Hygiene Promotion – Programming Guidance 67
SECTION FOUR: PROGRAMMING FOR BETTER IMPLEMENTATION
Chapter 8: Working with Communities and Households
cessful pilot experiences are not translated into ineffec-tive “generic” packages for scaling up by:● emphasizing and planning for the fact that working at
the community level always requires time;● ensuring that capacity building of potential front-line
units and partners is built in to every positive experi-ence so that the number of skilled workers increasesexponentially as time passes;
● working to ensure coherence between efforts in arange of social sectors so that front line units buildingcapacity to organize education for example, can alsocontribute and reinforce community needs in sanita-tion management and vice versa; and
● allocating sufficient funds to this important aspect ofsanitation and hygiene promotion.
For: participatory tools and approachesSee: IRC. (1996). The community-managed sanitation programme in Kerala: Learning from experience. IRC, Danida,SEU Foundation, Kerala.NGO Forum for Drinking Water and Sanitation. (1996) Social mobilisation for sanitation projects. (Annual Report,1995-1996.), Dhaka, Bangladesh.Simpson-Hebert, M., R. Sawyer, and L. Clarke. (1996). The PHAST Initiative. Participatory hygiene and sanitation trans-formation: A new approach to working with communities. WHO, Geneva, Switzerland.Sawyer, R., M. Simpson-Herbert, S. Wood (1998). PHAST Step-by-Step Guide: a participatory approach for the con-trol of diarrhoeal disease. WHO, Geneva, Switzerland.Srinivasan, L. (1992). Tools for community participation. UNDP/PROWWESS. Ferron, S., J. Morgan and M. O’Reilly (2000) Hygiene Promotion: A practical Manual for Relief and Development Intermediate Technology Publications on behalf of CARE International
Reference Box 13: Communications approaches
8.7 Programming InstrumentsSelection of communications approaches to communityand household interventions are best made at the locallevel in the context of projects and local investments.However where the skills and knowledge of those or-ganisations and individuals charged with this interactionare weak, programmers may be able to influence the sit-uation through a number of simple programmatic inter-ventions including:
● Supporting institutional analysis at local level which en-ables realistic strategies for community intervention tobe developed;
● Carrying out an overall assessment into the local-levelconstraints and barriers to hygiene improvement sothat locally-tailored interventions can be designed ap-propriately based on a solid understanding of the de-mand side of the “market”;
● Supporting participatory research into the most ap-propriate field-based tools and approaches;
● Directing funds to training/ research bodies to devel-op and disseminate locally-specific versions of gener-ic tools;
● Providing funds for training of field-level generalists inthe specifics of the hygiene improvement programmeapproach so that they can use their skills effectively;and
● Earmarking funds for national/ programmatic level el-ements of the communications strategy (such as massmedia campaigns etc:
● Developing and disseminating manuals and guidelinesfor the development of local strategies;
● Providing adequate public funds at local level to sup-port participatory planning, local capacity building andongoing support to communities;
● Providing frameworks to support community opera-tion and maintenance and the development of con-federations of communities who wish to access sup-port services for sanitation; and
● Funding training and capacity building for (a) commu-nity development organisations in aspects of hygieneimprovement; and (b) technical service agencies incommunity development approaches.

Sanitation and Hygiene Promotion – Programming Guidance68
8.8 Practical Examples from the Field:What will the community do?
A key challenge for sanitation and hygiene promotionprofessionals is to see how activities and communitymanagement organised around hygiene behaviours andsanitation hardware can and should be linked to existingcommunity and government structures. In Kerala, aDutch-government-supported sanitation programme, re-sulted in significant improvements in hygiene conditionsin a number of villages. Subsequently the approach wasadopted across the state, through pressure exerted byvillage panchayats (local government organisation) on thestate government. The strength of the initial project hadarisen in part because it took explicit notice of existingstructures and provided a clear role for the panchayatwhile also taking explicit action to support target groupsin the community, including women who wished to be-come masons and technicians.
In another Indian project; the Uttar Pradesh Rural Waterand Environmental Sanitation Project (SWAJAL), com-munities in the mountainous parts of Uttar Pradesh, wereempowered to plan and construct their own water sup-ply and sanitation systems. Groups from some villagestraveled to the plains to purchase pipes and other ma-terials, in some cases these journeys were undertaken bywomen-members of the Village Water and SanitationCommittees (VWSC) who had previously never lefttheir villages. Swajal also published a quarterly magazinefor participating villages which served as a news and com-munication tool in a dispersed rural area. While the spe-cific community-empowerment support-mechanisms setup in Swajal were clearly effective, there were someproblems because the institutional link to local govern-ment was not clarified. The government of India subse-quently took a much clearer line while rolling out someof the lessons from Swajal, in specifying the connectionbetween VWSCs and Panchayats.
In situations where water supply and sanitation institu-tions are stronger, it may be more challenging to devel-op local community-level capacity, unless the capacity ofthe utility itself is strengthened in this regard. In El Alto,Bolivia, a major investment of time and resources wentinto supporting the private water company as it devel-oped the condominial model for sanitation in the city.Input from a specialized support organisation, the Waterand Sanitation Program, was needed to build capacity forsocial mobilization, community contracting, participatoryplanning and monitoring, and in general to enable staff towork more effectively with communities.
In Burkina Faso, the Programme Saniya, used a combina-tion of local radio and face-to-face domestic visits, cou-pled with the transmission of messages in a traditional so-cial event called a djandjoba, to communicate well-craft-ed hygiene messages to carefully identified targetaudiences. In Zimbabwe, ZimAHEAD make use of theexisting structure of Environmental Health Technicians ofthe Ministry of Health who establish Community HealthClubs which become the focus for communication andcapacity building. In Mozambique the National SanitationProgramme took a low key approach to sanitation mar-keting, relying on word-of-mouth and the impact of fab-rication centres located in peri-urban localities to gener-ate demand. In central America a partnership with pri-vate soap manufacturers gave governments access tocommercial marketing skills for public health messages.
Key to any successful communication is clearly under-standing of what is to be communicated (what key prac-tices shall we try to change?); who is the target audience;and what are their existing communication habits andpractices. From this type of formative research tailoredcommunication strategies can grow.

Sanitation and Hygiene Promotion – Programming Guidance 69
SECTION FOUR: PROGRAMMING FOR BETTER IMPLEMENTATION
Chapter 8: Working with Communities and Households
Case Study Box 6: How shall we work with communities and households?
The description of the origins of the Clean Kerala Campaign is inVan Wijk-Sijbesma, C. (2003) Scaling Up Com-munity-managed water supply and sanitation projects in India presentation to the IDPAD Water Seminar, IHE,Delft, The Netherlands, May 12-13, 2003The Swajal Pilot Project is described in various publications. A useful starting point is WSP-SA (2001) Com-munity Contracting in Rural Water Supply and Sanitation: The Swajal Project, India Water and Sanitation ProgramThe El Alto experience is well documented on a dedicated website at www.wsp.orgFor an introduction to the programme, and information on the costs and benefits of the approach see Foster,V. (n.d.) Condominial Water and Sewerage Systems – Costs of Implementation of the Model Water and SantitationProgam, Vice Ministry of Basic Services (Government of Bolivia), Swedish International Development Coop-eration Agency. Programme Saniya and ZimAHEAD are described in Sidibe, M. and V. Curtis (2002) Hygiene Promotion in Burk-ina Faso and Zimbabwe: New Approaches to Behaviour Change Field Note No. 7 in the Blue Gold Series, Waterand Sanitation Program – Africa Region, NairobiThe handwashing partnership in Central America is described in detail in Saadé, C., Massee Bateman, DianeB. Bendahmane (2001) The Story of a Successful Public-Private Partnership in Central America: Handwashing for Di-arrheal Disease Prevention USAID, BASICS II, EHP, UNICEF, The World Bank Group
Notes for Chapter 8
i Much of this section draws on Brian Appleton and van Wijk, Christine(2003) Hygiene Promotion – Thematic Overview Paper IRC Interna-tional Water and Sanitation Centre

Sanitation and Hygiene Promotion – Programming Guidance70
9.2 Making Sure Hygiene Promotion Works
Changing hygiene behaviours is a key element and, as wehave seen, may often be the most crucial step in achiev-ing health gains. Hygiene promotion is all about changingbehaviours. Despite this it is often neglected or margin-alized in programmes which state that they aim to im-prove hygiene; many of these programmes place muchgreater emphasis on the construction of hardware (oftenprioritizing water supply over sanitation). Not only doesthis mean that there is insufficient resources available foreffective hygiene promotion, but it also means that thehardware which is installed may be inappropriate be-cause it is not planned within an overall “hygiene im-provement” framework. In some cases these interven-tions may even make it more difficult for communitiesand households to improve hygiene and enjoy real healthbenefits. This may happen for example when designs areinappropriate and facilities cannot be used or where sec-tions of the community are excluded. To be effectivethen, sanitation and hygiene promotion programmesneed to be designed with the hygiene improvementframework in mind – ensuring adequate resources for allthree elements, and perhaps in some cases, focusing on
hygiene promotion ahead of construction of physical in-frastructure which may be a secondary, more long termstrategy.
Furthermore, hygiene promotion should be seen as amajor element in the programme requiring not only ad-equate financial resources, but also the requisite levels ofprofessional expertise and effort. Too often, engineersmay seek to “add on” a hygiene promotion componentto what is essentially a latrine construction programme,without due attention to the complexities of making hy-giene promotion effective. Importantly it is often neg-lected during the planning phase with insufficient atten-tion paid to gathering the types of information which areneeded to design really effective behaviour changestrategies. At the other end of the scale, insufficient timemay be made available for the needed changes in be-haviour to take root. Changes hygienic practices is oftena long term process, and it may not be achieved for ex-ample within the three year planning horizon of a con-ventional water supply project, or indeed the commonterm for a local political administration.
Much has been learned about making hygiene promotioneffective. Many of the key ideas are summarized in a use-ful Fact Sheet published by WELL i. These ideas aresummarized below:
● Build on what exists: A hygiene promotion pro-gramme should be based on a thorough understand-ing of: ● the most important risky practices which should be
targeted; ● who are primary/ secondary and tertiary audiences
for key messages;● who can most effectively motivate behaviour
change;● what may prevent behaviours;● how can audiences be most effectively reached;
and● how can the effectiveness of the programme be
measured.
Formative research is one approach which can be usedto develop the hygiene promotion strategy. Formativeresearch is a pragmatic approach to planning pro-grammes which has attributes that “make it a particular-ly useful component of…..sanitation programmes”. Theapproach is flexible and allows researchers to devise keyquestions which are specific to the community in whichthey are working. Answers can be used to develop a planof action ii.
● Target a small number of risk practices: Thepriorities for hygiene behaviour change are likely to in-clude handwashing with soap (or a local substitute)after contact with excreta, and the safe disposal ofadults’ and childrens’ excreta.
● Target specific audiences: audiences may includemothers, children, older siblings, fathers, opinion lead-ers, or other groups. An important group is those
9.1 Introduction
Chapter 9 Hygiene Promotion

Sanitation and Hygiene Promotion – Programming Guidance 71
SECTION FOUR: PROGRAMMING FOR BETTER IMPLEMENTATION
Chapter 9: Hygiene Promotion
Table 14: Applying the Principles to Hygiene Promotion
Use hygiene promo-tion as a two-wayprocess of communi-cation to: (i) informand influence house-hold behaviours and(ii) gauge effectiveways of harnessingcommunal effort forthe public good
Support approachesto hygiene promotionwhich empower peo-ple rather than thosewhich present elitistor patronizing mes-sages
Support informationgathering so that hy-giene promotion canbe based on a thor-ough understandingof: key behaviours tochange; key audi-ences; key motivators;ways to change be-haviours; how toreach audiences; andhow to measure out-comes
Expand the range ofparticipants in hygienepromotion to ensurethat messages are re-inforced and deliveredin the long term
Invest in capacitybuilding to improveapproaches to hy-giene promotion
Maximising publicand private benefits
Achieving Equity Building on whatexists and is in demand
Making use of prac-tical partnerships
Building capacityas part of theprocess
9.3 Applying the PrinciplesTable 14 shows how the principles of good programming can be applied to decisions about hygiene promotion.
people primarily involved with child care. Audiencesneed to be identified in each particular case.
● Identify the motives for changed behaviour:As mentioned elsewhere, these may have nothing todo with health. People may be persuaded to washtheir hands so that their neighbours will respect them,so that their hands smell nice, or for other reasons.Participatory planning with target groups can be usedto discover local views about disease, and ideas aboutthe benefits of safer hygiene practices. This can formthe basis for a hygiene promotion strategy.
● Hygiene messages need to be positive: peoplelearn best when they laugh, and will listen for a longertime if they are entertained. Programmes which at-
tempt to frighten audiences will probably alienatethem. Furthermore, messages consisting of “dos” and“don’ts” can be frustrating and demoralizing for thepoor particularly where they urge actions which areunrealistic for poor families iii.
As with all elements of the hygiene improvement pro-gramme, monitoring will be needed at the local level toensure that inputs are delivered and that they result inthe expected outcomes. At the programmatic level, itwill be essential to provide oversight that ensures that hy-giene promotion is integral to the overall programme,and that where hygiene promotion activities indicate theneed for additional inputs in terms of hardware these canfollow in a responsive manner (see Reference Box 14).
For: A summary of current thinking on hygiene promotion, and links to other resources and referencesSee: Appleton, Brian and Dr Christine van Wijk (2003) Hygiene Promotion: Thematic Overview Paper IRC Inter-national Water and Sanitation CentreCurtis, V. and B. Kanki (1998) Towards Better Programming: A Manual on Hygiene Promotion Water, Environmentand Sanitation Guidelines Series No. 6 UNICEFGet thes reference on the web at www.irc.nl and www.unicef.orgFor: Summary of seven “key messages” about hygiene which can be easily incorporated into a well-designed ad-vocacy campaign.See: Facts for Life UNICEFGet this reference from: Local UNICEF offices or on the web at http://www.unicef.org/ffl/09/
Reference Box 14: Hygiene promotion

Sanitation and Hygiene Promotion – Programming Guidance72
In most cases the most important programming decisionto be taken will be to allocate adequate resources to hy-giene promotion, along with the needed institutionalanalysis, monitoring and feedback systems. In additionhowever, a recognition of the importance of hygienepromotion, should also be linked to decisions about: al-locating responsibility for overall programme manage-ment and project investments; institutional and organiza-tional arrangements; and coordination mechanisms. Spe-cific additional actions might include:● commissioning baselines studies on current hygiene
practices;
● commissioning formative research to determine keybehaviors to focus on;
● developing behavior change strategies including socialmarketing, social mobilization, and community-leveleducation;
● integrating hygiene promotion efforts in Ministry ofHealth programs;
● determining roles and responsibilities for carrying outhygiene programs;
● ongoing monitoring of program effectiveness; and ● training at all levels for program implementation
9.4 Programming Instruments
The Sanitation and Family Education Project was devel-oped and implemented by CARE Bangladesh, with tech-nical assistance from the International Centre for Diar-rhoeal Disease Research (Bangladesh). The SAFE proj-ect had no hardware component but was designed as asupplementary or follow-on activity after an earlier cy-clone relief project which provided tubewells and la-trines. SAFE worked by targeting a small number of spe-cific behaviours including: drinking pond or open wellwater, improper storage of tubewell water, adding pondwater after cooking, using unhygienic latrines, poor hand-washing practices and low use of latrines by childrenunder the age of five. The project area saw a two-thirdsreduction in diarrhea prevalence when compared withcontrol areas, and a substantial increase in hygienic be-haviours including handwashing and hygienic latrine use.What is interesting about the SAFE experience, was thatit operated in an area which had already been targetedwith hardware and showed significant health benefits.Without the additional push on hygiene promotion, it isunlikely that the investment in latrines and water supplywould have yielded expected benefits.
In comparison, the Environmental Health Project (EHP)was able to implement a full range of ‘HIF’ interventionsin Nicaragua during a two –year project which was setup in the aftermath of Hurricane Mitch. The project pro-vided: hardware, through water supply and environmen-tal projects implemented by local NGOs; hygiene pro-motion, using trained community members and schools
as the two primary mechanisms to deliver messages; andstrengthening of the enabling environment, through ca-pacity building of local water committees and at the na-tional level. Here the benefits were substantial and theadvantages of the coordinated approach did not pre-clude a range of innovative institutional arrangementsand partnerships being established.
In general hygiene promotion is a long-term process,which links an understanding of the current situation witha vision of what behaviours can be changed, and how thiscan happen. In Zimbabwe, ZimAHEAD have pioneeredthe Health Club approach to provide a framework forthis needed long-term change. Community Health Clubsprovide a forum for community-members to learn aboutsimple and effective ways of improving hygiene in thehouse and community, and they also provide the com-munity with a focus for planning and implementing watersupply and sanitation activities. But perhaps more signif-icantly the CHCs also provide support for wider eco-nomic activities, and provide a more interesting and stim-ulating framework within which the Ministry of HealthEnvironmental Health Technicians can see long termstructured change occurring in the communities withwhich they work. The CHC approach has proved to beextremely robust, and even with the recent decline in de-velopment budgets and the loss of funds from externalsupport agencies, the CHCs have been able to sustaintheir activities and keep operating.
9.5 Practical Examples from the Field:How will we promote hygienic behaviours?

Sanitation and Hygiene Promotion – Programming Guidance 73
SECTION FOUR: PROGRAMMING FOR BETTER IMPLEMENTATION
Chapter 9: Hygiene Promotion
Case Study Box 7: How will we promote hygienic behaviours?
The Community Health Clubs and ZimAHEAD are described in Sidibe, M. and V. Curtis (2002) Hygiene Pro-motion in Burkina Faso and Zimbabwe: New Approaches to Behaviour Change Field Note No. 7 in the Blue GoldSeries, Water and Sanitation Program – Africa Region, Nairobi. Further discussion of CHCs, along with in-formation about NORWASP and the EHP project in Nicaragua is available in the case studies in the IRC The-matic Overview Paper (TOP) available on the web at www.irc.netVERC’s experience in Bangladesh is discussed in Kar, K. (2003) Subsidy or self respect? Lessons from Bangladeshid21insights, issue 45 on the web at www.id21.org/insights/insights45
Ensuring a robust structure for hygiene promotion is im-portant, but, as was the case in Bangladesh, this may beoutside or in parallel with a programme of hardware pro-vision. Investments in increasing access to hardware, andpromoting hygienic practices need to be coordinated butcan sometimes be successful when they are carried outby different agencies. In Ghana, the Northern WaterSupply and Sanitation Project (NORWASP) integratedhealth and hygiene into water supply and sanitation forrural communities. A thorough evaluation of baselinedata was carried out before a community-based hygieneeducation programme was developed, and this in turnwas first piloted, and evaluated by the community. Theapproach drew from PHAST and PLA methods, but wastailored to local conditions, and made use of a locally-de-veloped health and hygiene game. Identifying and train-ing a cadre of committed fieldworkers is crucial, and this
is a key strategy in NORWASP. The project was notbound to one particular agency, but sought out the bestinstitutional “homes” for different activities, while pro-viding an overall coordinating framework.
As well as getting the institutional structure right, hygienepromotion needs to apply appropriate approaches. Insome contexts for example, shocking messages maywork well; in Zimbabwe, the CHCs use a slogan whichis often “chanted at health club meetings” in the local lan-guage, which when translated states baldly “don’t shareyour shit”. In Bangladesh, VERC carry out village transectwalks during which households discuss where each fam-ily member defecates, and identify areas in the villagewhich are regularly soiled with faeces. Such approachesmay not work in other situations, and each case must beassessed on its own merits.
i This section draws heavily on Appleton, Brian and Dr Christine vanWijk (2003) Hygiene Promotion: Thematic Overview Paper IRC In-ternational Water and Sanitation Centre drawing particularly on Ap-pendix 2. This excellent reference is recommended as a starting pointfor more detailed programme planning.
ii Sidibe, M. and V. Curtis (2002) Hygiene Promotion in Burkina Faso andZimbabwe: New Approaches to Behaviour Change Field Note No. 7in the Blue Gold Series, Water and Sanitation Program – Africa Region,Nairobi
iii Appleton and van Wijk point out that messages such as “wash handswith soap” or “use more water for washing” may simply make peoplemore frustrated and disempowered in situations where for examplesoap is not commonly used or available or where every drop of waterhas to be carried long distances.
Sanitation and Hygiene Promotion – Programming Guidance74
In many parts of the world conventional ‘sanitation’ pro-grammes have tended to focus on the public provisionof latrines, either through direct construction, or by pro-viding subsidies based either on a needs-assessment, oron the completion of a latrine of “acceptable” standard.In a few regions, where progress in the water supply andsanitation sector has moved faster, sanitation has beenviewed more as a “utility” issue often with a focus on reg-ulating to prevent ‘unauthorised’ construction or, inurban situations, to preserve the exclusive right of theutility to provide.
Once sanitation is seen within the context of hygiene im-provement however, it becomes clear that latrines aloneare not very effective, and their provision needs to becoupled with, and often subordinate to, an increase inawareness about hygienic practices in general and achange in the way hygiene is managed locally. Further-more, even where latrines are clearly urgently needed, di-rect public provision has been shown to be problematicin many cases. The sheer scale of the need swamps mostpublic providers i and this, coupled with suspicions of cor-ruption and inefficiency in many programmes, suggeststhat new approaches need to be tried, in tandem withan improvement in public provision where this appro-priate.
Where it exists, the small scale private sector providessome hope that provision can be scaled up, and mademore effective through local innovation and the ability oflocal providers to be more responsive to household de-mand. Where this small scale business does not exist,programmers may want to devote some of their effortand resources towards stimulating and supporting itsgrowth, to relieve the pressure on public provision. Thepotential for this sanitation “business” is easier to under-stand in rural areas or less congested urban slums, whereon-plot provision makes a straight forward business re-lationship between the household and the supplier pos-sible. In congested urban areas where off-plot provisionis needed, this relationship is less clear, and there will al-most certainly be a responsibility retained by the publicprovider or utility. Nonetheless new institutional andtechnical approaches mean that there may still be a rolefor an intermediary or small scale private provider at thelocal level to facilitate the development and managementof and appropriate local network system. For more in-formation on the basic technology issues of sanitation seeSection 10.2 below.
The key idea here is to move away from the direct pro-vision of a pre-determined technology, to a situationwhere households and communities can choose from arange of appropriate options, supported by a range ofsuppliers who are highly motivated and skilled to providethem.
10.1 Introduction
Chapter 10 Selecting and Marketing Technologies
10.2 Making Sure that Technology WorksBroadly, sanitation technologies fall into four main typesas shown in Table 15. The choice of technology will bestrongly influenced by a range of factors, of which thetwo most important are:
● How much used water (wastewater) must be re-moved from the household?
● Will the disposal of the excreta be on-site or off-site?
Sanitation Technology Choices
(a) Limited water use and on-site disposal (la-trines)Many poor people have limited access to water, and donot enjoy the relative luxury of a household connection.Water consumption is thus limited to around 20 lpcd orless, and little wastewater will be generated. On-site toi-let facilities offer substantial advantages over off-site fa-cilities in terms of convenience, privacy, and management(family-owned latrines are in most cases better main-tained than public ones). Basic pit latrines, pour-flush la-

Sanitation and Hygiene Promotion – Programming Guidance 75
SECTION FOUR: PROGRAMMING FOR BETTER IMPLEMENTATION
Chapter 10: Selecting and Marketing Technologies
trines, or variants of these basic types (e.g. EcologicalSanitation, VIPs, etc.) are usually the most appropriatetypes of technology to consider for on-site disposal ofexcreta with little water.
Latrines protect the environment from faecal contami-nation by isolating excreta in a pit. When the pit is fullafter five to ten years, it must be emptied before it canbe used again. Where space permits, a new pit can bedug, and the contents of the full pit may be left to com-post. After a year or more of composting, the pathogensin the waste will have been neutralized, and the contentsmay be safely handled. These contents may be used asagricultural compost. Ventilated Improved Pit (VIP) la-trines improve on the basic design and limit nuisancefrom flies and odours.
Pour-flush latrines are those in which the excreta areflushed from the defecation area by water, and are par-ticularly appropriate in cultures where water is used foranal cleansing. The water may be used to create a waterseal between the wastes in the pit and the outside, thuseliminating problems with odours, flies and mosquitoes.
Pit latrines are difficult to build in areas of high ground-water table, or in rocky areas. High groundwater tablenot only makes construction difficult, but also raises therisk of groundwater contamination from the contents ofthe latrine These risks can, in most cases, be minimizedif the bottom of the latrine is at least 2 m above thegroundwater table, and the latrine is at least 15 m awayfrom any well used for drinking water. Finally, sludge man-agement (i.e. the transport and disposal of the latrinecontents after emptying) should be carefully consideredwhere space is limited, especially in urban or peri-urbanareas. A variety of ecological (“EcoSan”) toilets existwhich are designed to improve the composting of the la-trine’s sludge, and thus turn the problem of sludge man-agement into an opportunity to generate higher valuecompost.
(b) Limited water use and off-site disposal(bucket latrines, public toilets)Where access to water is limited, and excreta disposalon-site is not feasible (due to either cost or space con-straints), bucket latrine systems or public toilets are oftenused.
In the bucket system (or “conservancy system” as it isknown in South Asia) excreta are deposited in a bucket
or lined basket that is emptied several times a week bya “sweeper” who disposes of the waste elsewhere. Inearlier times, elaborate plans were made for the collec-tion of wastes to “bucket transfer stations” where thebuckets were emptied into larger carts and cleaned priorto their reuse. The larger carts, in turn, were meant totransfer the waste to a sanitary disposal site. In currentpractice, however, the disposal is almost always to a near-by drain (eventually leading to drain blockage) or to a pileof solid waste, exposing rag pickers and children to fae-cal wastes. The system is generally considered an ex-tremely unsanitary arrangement, and is officially illegal inIndia and a number of other countries. Where field sur-veys establish the continued existence of this system,however, sanitation planners need to address two ques-tions before simply banning it:
1. What more sanitary option can realistically be of-fered?
2. During the transition period to the more sanitary op-tion, how can the bucket system be rendered morehygienic?
Public or shared toilets are a second form of off-site dis-posal, and indeed, have been promoted in India byNGOs such as Sulabh International Inc, as an answer tothe defects of the bucket system. Public toilets may in-volve any number of technological options, from com-mon pits to sewer system connections. All public toilets,however, involve a number of difficult institutional ques-tions, which have previously weighed against its wide-spread adoption by sanitation professionals.
Management of public toilets is a daunting challenge, al-though recent experience in South Asia shows that it canbe overcome in some cases. While the responsibility for(and interest in!) cleaning private toilets clearly rests withthe owner, responsibilities are often less clear-cut forpublic or shared toilets. It is often difficult to establish aneffective maintenance regime for a toilet shared amongfive or ten families. Government or community run pub-lic toilets are often in an appalling state (in Europe andNorth America as much as anywhere else) because ofthe lack of interest and incentive for adequate mainte-nance.
Sulabh International has developed a public toilet fran-chising system whereby attendants and managers are re-imbursed from a small fee for use levied on adult malecustomers; women and children can use the toilet for

Sanitation and Hygiene Promotion – Programming Guidance76
free. The fee is sufficient to ensure a reasonable incomefor the manager, who has an interest in maintaining aclean well-run establishment; Sulabh’s monitoring of per-formance means that s/he risks losing the job if per-formance slips. While the franchise arrangement worksin a number of settings (e.g. railway or bus stations) it isunclear that the financial model can work to serve theurban poor, when competing with “free” open defeca-tion.
Household toilets, where feasible, are preferable to pub-lic toilets for 3 main reasons:● convenience to the household, which encour-
ages use● clear accountability for cleanliness, which also
encourages use, as the cleanliness is within the con-trol of the household
● safe disposal of children’s faeces is more likelywith a household toilet. Although a number of publictoilet systems try to encourage use by children, it isless likely than a household toilet to work, especiallyfor the disposal of young children’s faeces.
(c) Substantial water use and on-site disposal(septic tanks, soakaways)As access to water increases, water use will also increase,along with the requirement for its safe disposal. Sullageand grey water are the technical terms for householdwastewater that is not used in toilets; sullage is made upof bathing water, water used for washing and cooking,etc. While it is less contaminated than toilet water, it isincorrect to think of it as “uncontaminated”; water usedfor cleaning the clothing and nappies of infants and veryyoung children, is often heavily contaminated.
Pouring large quantities of sullage into a pit latrine pit islikely to lead to pit overflow, bad smells, and insectbreeding. This is because latrine contents will quickly“plug” the soil, and limit the capacity of the soil to ab-sorb large volumes of sullage. The construction of a sep-arate soakaway for sullage is far more likely to work. Asoakaway is a large pit or trench filled with bouldersand/or gravel through which sullage may infiltrate into alarger surface area of soil. By keeping the sullage sepa-rate from the faecal wastes, the risk of soil plugging is re-duced, and the soakaway can serve for a much longertime.
Septic tank systems (with soakaways or drainfields) arean alternative on-site solution for combined wastewater
disposal. A septic tank is a concrete or masonry box inwhich some settling and treatment of faecal solids takesplace; the wastewater leaving the septic tank is relativelyclear and free of solids (although highly contaminated bi-ologically). Sullage enters the septic tank after the set-tling of the solids, and the combined flow is dischargedto the soil through a soakaway or drainfield. As the sep-tic tank removes the faecal solids from the flow, the in-filtration area of the soakaway is far less likely to becomeplugged.
Septic tanks are most commonly used by those with cis-tern-flush toilets and house connections for water.While traditionally each household has its own septictank, a number of households with individual toilets andplumbing arrangements can connect to a single septictank.
The capacity of both soakaways and septic tank systemsto remove wastewater safely from the plot dependsgreatly upon the infiltration capacity of the soil. Soak-aways and septic tanks work best in sandy soils, and can-not work well in tight clays. As with pit latrines, there isa risk of groundwater contamination, and this is particu-larly great when sullage and excreta are combined.
Sludge builds up in septic tanks as the faecal solids settle,and must be removed periodically. As with latrine sludge,the collection and disposal of septic tank sludge requiresattention. Without good sludge management and en-forcement, the public will be exposed to the effects ofclandestine dumping of sludge into drains and piles ofsolid waste.
(d) Substantial water use and off-site disposal(sewers)Sewers are common where water is readily available butsuitable land and soil for septic tank systems are not.Sewers are pipes that carry wastewater (toilet wastesand sullage) away from the household to a centralizedtreatment and disposal point. Sewers are very conven-ient for the user, requiring a minimum of maintenance.They are often, however, a relatively expensive solution,especially if the wastewater is treated (as it should be)before its ultimate disposal to surface water. Sewers re-quire a reliable water supply, and sufficient wastewaterto ensure reasonable flushing of the solids through thesystem. Large systems, or systems in flat areas, often re-quire pump or lift stations, to raise the sewage and thusreduce the depth and excavation costs of downstream

Sanitation and Hygiene Promotion – Programming Guidance 77
SECTION FOUR: PROGRAMMING FOR BETTER IMPLEMENTATION
Chapter 10: Selecting and Marketing Technologies
pipe. Such pump stations not only require careful oper-ation and maintenance, but also a steady source of cashto cover significant power costs. Sewers should only beconsidered in cities and small towns and are not viable inrural villages.
There have been a variety of innovations in sewerageover the last two decades, particularly in Latin America,which have reduced its cost and operational complexitythrough a range of “condominial” technologies and insti-tutional systems; Mara (see Ref. Box 15) is a good guideto some of the technical issues and debates involved inlow-cost sewerage.
Table 15: Range of Technology Choices
Off-site Conservancy/bucket system Public toilets
Sewers (including non-conventionalvariants)ii
On-site Pit latrine and variants, Pour flush latrines
Septic Tanks Pit latrines plus soakaways
Water supply volume
Disposal point
Limited (< 20 lpcd) Ample (>20 lpcd)
The programmers’ responsibility is to balance what iscurrently possible and desirable at the household or pri-vate level (ie what can be achieved in the short term)with long-term public policy objectives such as realizationof full public health benefits, protection of the environ-ment and maintenance of health and safety.
There is no such thing as an “ideal technology”. In manycountries standard designs and approaches, usually justi-fied on the basis of long-run public policy objectives, havebecome entrenched in widescale national latrine con-struction programmes. They may appear to be the onlyviable solution and technicians may aspire to constructonly facilities of the highest specification possible. How-ever, programmes promoting these “ideal” facilities rarelyachieve high rates of coverage – because demand for thehigh-cost technologies on offer is too low and there areinsufficient funds to provide them universally on the pub-lic budget. One look at the latrines that people build forthemselves however, illustrates that a wider range of so-lutions is possible. In many cases these home-built la-trines may fail to improve the situation at all – but theymay point to a viable first step on what is known as ‘thesanitation ladder’ ie the first intervention which will in-crease awareness of the benefits of sanitation, begin tolessen risks and start a household on the process that willlead to the installation and use of a sanitary latrine. In thelong-run this is likely to result in much greater coverage
and health improvement than would be the case if only“the best” were to be built or allowed to be built.
The balancing act for programmers is to judge what is ac-ceptable and likely to be used by households, promoteit appropriately and assess how best to move householdsas rapidly as possible up the sanitation ladder so that bothprivate and public benefits can be realized. To do thisgovernment may retain a prominent role, beyond simplyenforcing standards, in: promoting innovation; balancinglocal needs with national public policy priorities (for ex-ample intervening in emergency situations, enforcingstandards in public places and schools etc); and steeringhousehold choice by supporting sanitation marketing ef-forts (see below).
Climbing the sanitation ladder in this way may not seemvery glamorous but may in fact be the most effectivemeans of making rapid and visible improvements in thesituation. Furthermore the concept of the sanitation lad-der is particularly important for the poorest households,where local conditions, lack of money and low levels ofawareness may preclude the construction and effectiveuse of latrines. Programmers need to support any in-cremental improvements, and may choose to steer pub-lic resources to the provision of appropriate school san-itation and public facilities so that some access is achievedwhile awareness is built.
10.3 Selecting Technologies – the sanitation ladder

Sanitation and Hygiene Promotion – Programming Guidance78
The interaction between technical constraints and orga-nizational issues is also important. For example if peoplehave no space but have proved that they can take con-certed action in some other development sphere thenthe possibility of constructing and managing shared facil-ities should be considered (shared latrines, communal
bathing facilities, condominial sewers etc). Where peo-ple are willing to give up space in their houses for sani-tation but are unwilling or unable to collaborate withtheir neighbours a different (on-site) solution may bepossible.
For: Details of sanitation technologies and guidelines on choice of technologySee: Pickford, John (1995). Low-cost sanitation. Intermediate Technology Publications: London.Mara, Duncan (1996). Low-cost urban sanitation. John Wiley & Sons: Chichester.Cairncross, Sandy and Richard Feachem (1993). Environmental health engineering in the tropics: an introductory text.(2nd edition) John Wiley & Sons: Chichester.Get these references from: Good technical libraries or the Water Engineering Development Centre(WEDC) at www.lboro.ac.uk
Reference Box 15: Sanitation technologies
It is quite obvious that capacity needs to be built amongsthouseholds, communities and even small scale inde-pendent providers so that they can participate more ef-fectively in the provision of sanitation facilities that doachieve health improvements. What may be less obvious,though, is that there may be a need to build capacityamongst technical staff also, many of whom may be welltrained in ‘conventional’ sanitation engineering. Unfor-tunately such conventional training tends to focus on ex-pensive solutions, often with a heavy emphasis on pipedsewerage (which is inappropriate in rural areas, and maynot work in urban areas with low levels of water supply,
unreliable power and low operating revenues). It mayalso place an emphasis on waste water treatment which(a) is inappropriate where on-site solutions are to beused; and (b) may be irrelevant where the public healthimperative is to get as many households as possible touse a latrine as the first step. These staff may lack ex-pertise in the complex area of ‘making-do’ and finding thebest compromise in a less-than-perfect world. They maylack the skills to identify the best innovations and, worse,they may, in good faith, create barriers to the type of in-cremental improvements which are needed.
10.4 Other Factors – community management
10.5 Building Capacity
Sanitation and Hygiene Promotion – Programming Guidance 79
SECTION FOUR: PROGRAMMING FOR BETTER IMPLEMENTATION
Chapter 10: Selecting and Marketing Technologies
Why do people pay for sanitation?As the emphasis shifts from “policing” and “providing”technologies to “marketing sanitation” and ‘promoting in-novation’ technical roles may shift. Marketing of sanita-tion as if it were a business is a relatively new idea. Fewcountries have forged effective links between privateproviders and public agencies. Nonetheless this is maybe infinitely more important, particularly in countries withvibrant small-scale markets for goods and services, thanthe ability of public-sector engineers to design and buildurban sanitation systems.
Because the public interest in sanitation is linked to itsrole as a primary barrier of disease prevention health isoften thought to be the principle driver of demand.However a World Bank survey iii in the rural Philippinesestablished the following reasons for satisfaction withnew latrines (in order of priority):
1. Lack of smell and flies;2. Cleaner surroundings;3. Privacy;4. Less embarrassment when friends visit; and5. Less gastrointestinal disease.
Some may regret that health education has been insuffi-cient to raise the concern about gastrointestinal diseaseto a higher priority. Others, however, will quickly realizethat all of the other reasons are excellent ways to mar-ket sanitation, and will accordingly review their market-ing and product development strategy to take such prac-tical concerns into account.
What influences household demand?Figure 5 illustrates in a simplified way, the relationshipbetween household demand and service delivery. It em-phasizes that, where household demand is a driver for in-vestment decisions, the role of the public sector (bothon the supply side and in creating an appropriate enablingenvironment) remains crucial and may be more chal-lenging than in traditional “public service delivery” typeapproaches.
In order to stimulate or create demand for a service, it isimportant in any situation to understand what is drivingdemand (or lack of it). Figure 5 suggests four main fac-tors which will influence the depth and breadth of house-hold demand for any particular good or service.
These are:
● Awareness: knowing that the goods/services existand that they have benefits. For example, knowingthat latrines exist and can be used to store excretaand knowing that a latrine can improve the health ofchildren and have a positive impact on household in-come;
● Priority: deciding that the service is sufficiently im-portant to merit needed investment For example, de-ciding to build a latrine rather than construct an addi-tional room in the house or invest in a bicycle. Prior-ity may be influenced by access to other priorityservices or a range of other factors such as status orsocial conventions. Priority may also vary betweenmembers of the households – and it is important totarget demand creation and assessment activities ap-propriately (for example building a latrine requires adecision by the member of the household responsi-ble for major capital investments in the home andthat person should be a key target of a latrine mar-keting campaign);
● Access: having access to a service provider who willmarket and provide the specific service. For examplehaving a local mason who knows what types of la-trines can be built, help decide what is the most ap-propriate and build it; and
● Influence: being able to take effective individual ac-tion, or being in a position to participate in effectivecollective action. For example, having space to buildan on-plot latrine, or being in a location where it ispossible to participate in a condominial seweragescheme.
Any sanitation marketing approach probably needs toaddress these four areas. While there is little empiricalknowledge to date of how this can be done most effec-tively some ideas and suggestions are laid out in Table16 which shows an indicative approach to breaking downthe four barriers listed above.
Sanitation marketing has to become more sophisticated.It has to move from the current approach which is heav-ily skewed towards public sector promotion of fixedideas, to a more innovative approach which explores the
10.6 Sanitation Marketing

Sanitation and Hygiene Promotion – Programming Guidance80
Financing
Efficient delivery of appropriate goods and services
Assessment, aggregation &mediation of demand
Awareness
Policy, regulation and institutional
Resources (from households)
HouseholdDemand for goods and services
Priority Access Influence
Demand side(private)
Supply side(public)
Enabling environment
Figure 5: Household demand in the context of service delivery
potential of the market to provide some of the solutions.Marketing expertise can be linked to technical expertiseto create the right mix of messages and promotional ap-proaches which can start to make purchasing and usinga toilet a high-priority choice for households. The chal-lenge for programmers at the moment is to come upwith such new approaches almost from scratch since
there is so little experience to build on. Ultimately thechallenge is to turn toilets into attractive consumer itemsfor those with some money to spare, while maintaininga focus on the supply-side of the market to ensure thatcheap and appropriate versions are accessible by thepoorest households.
Importantly marketing latrines (along with all otherchanges in household hygienic practices) is a long-termundertaking and cannot be achieved in a short timeframe. Programmers need to establish marketing sys-tems that will have adequate resources to work with
households in the long term to improve their awarenessof sanitation, raise its priority, increase household accessto providers of goods and services, and equip householdsto influence those providers as required.

Sanitation and Hygiene Promotion – Programming Guidance 81
SECTION FOUR: PROGRAMMING FOR BETTER IMPLEMENTATION
Chapter 10: Selecting and Marketing Technologies
Table 16: Illustrative sanitation marketing approaches
On-plot/ rural
Mass media campaigns(based on a hygieneimprovement frame-work) linking hygienebehaviour change andhousehold invest-ments in sanitation toimproved lifestyle,higher earnings andstatus.
Household level par-ticipatory evaluationsand planning to em-phasise the need andpotential of HH sani-tation.
Link to primary healthcare and micro-finance interventions.
Public schemes tosupport mason /plumber training, including business-support to small scaleindependent serviceproviders.
Public marketing ofsmall scale privateservices.
Mass media campaignto emphasise the rela-tive ease of household/ shared sanitation inrural and some urbanareas.
Demand Factor
Settlement/Technology
Awareness Priority Access Influence
Networked/ urban
Household / community level par-ticipatory evaluationsand planning to em-phasise the need andpotential of communi-ty sanitation.
Public schemes to licence and supportsmall scale independ-ent providers (ie pitemptying services).
Public funds to trainsupport agencies pro-viding planning, microfinance and manage-ment support for lowcost networks.
House-to-house communication tomarket appropriate shared-or collective ap-proaches.
Community planningcoordinated with andsupported by the utility.
This chapter has emphasized that there needs to be amajor shift away from the idea of public provision of la-trines towards the idea of building, promoting, and sup-porting a sanitation business. Such a business will havethe following key elements:
● Informed demand from households;● Responsive supply from providers of goods and serv-
ices; and ● Appropriate support from the public sector on both
the demand- and supply- side.
In some countries this “business” already exists, and thereal need is to ensure that it is legalized, appropriatelysupported so that it scales up, and then (and possibly onlythen) regulated to secure long term public policy objec-tives. In other countries the ‘business’ does not yet exist.Even where this “business” is likely to remain well with-in the public sector, much more emphasis is needed onpromoting demand, supporting innovation and enabling
local choice to drive incremental improvements in sani-tation.
In most countries there will be a number of barriers tothis including;
● Inappropriate skills (in public and private sector agen-cies);
● Excess of technical staff in public agencies;● Lack of capacity in the small scale private sector (for
both delivery and marketing);● Lack of knowledge and experience of marketing san-
itation;● Technical norms and standards which preclude inno-
vation and drive up costs; and● Other regulations which hamper innovation including
outdated building codes, planning regulations and en-vironmental controls.
All of these barriers need to be addressed at the pro-grammatic level.
10.7 Key issues and barriers
Sanitation and Hygiene Promotion – Programming Guidance82
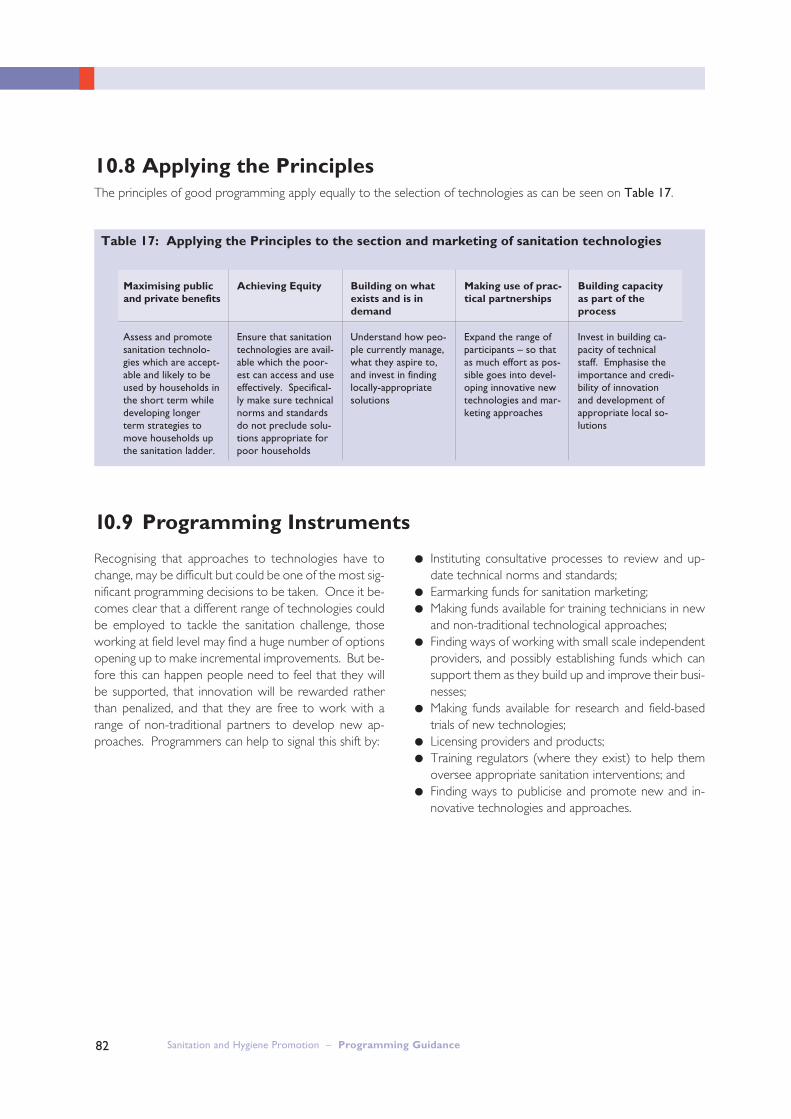
Table 17: Applying the Principles to the section and marketing of sanitation technologies
Assess and promotesanitation technolo-gies which are accept-able and likely to beused by households inthe short term whiledeveloping longerterm strategies tomove households upthe sanitation ladder.
Ensure that sanitationtechnologies are avail-able which the poor-est can access and useeffectively. Specifical-ly make sure technicalnorms and standardsdo not preclude solu-tions appropriate forpoor households
Understand how peo-ple currently manage,what they aspire to,and invest in findinglocally-appropriatesolutions
Expand the range ofparticipants – so thatas much effort as pos-sible goes into devel-oping innovative newtechnologies and mar-keting approaches
Invest in building ca-pacity of technicalstaff. Emphasise theimportance and credi-bility of innovationand development ofappropriate local so-lutions
Maximising publicand private benefits
Achieving Equity Building on whatexists and is in demand
Making use of prac-tical partnerships
Building capacityas part of theprocess
10.8 Applying the PrinciplesThe principles of good programming apply equally to the selection of technologies as can be seen on Table 17.
Recognising that approaches to technologies have tochange, may be difficult but could be one of the most sig-nificant programming decisions to be taken. Once it be-comes clear that a different range of technologies couldbe employed to tackle the sanitation challenge, thoseworking at field level may find a huge number of optionsopening up to make incremental improvements. But be-fore this can happen people need to feel that they willbe supported, that innovation will be rewarded ratherthan penalized, and that they are free to work with arange of non-traditional partners to develop new ap-proaches. Programmers can help to signal this shift by:
● Instituting consultative processes to review and up-date technical norms and standards;
● Earmarking funds for sanitation marketing;● Making funds available for training technicians in new
and non-traditional technological approaches;● Finding ways of working with small scale independent
providers, and possibly establishing funds which cansupport them as they build up and improve their busi-nesses;
● Making funds available for research and field-basedtrials of new technologies;
● Licensing providers and products;● Training regulators (where they exist) to help them
oversee appropriate sanitation interventions; and● Finding ways to publicise and promote new and in-
novative technologies and approaches.
10.9 Programming Instruments

Sanitation and Hygiene Promotion – Programming Guidance 83
SECTION FOUR: PROGRAMMING FOR BETTER IMPLEMENTATION
Chapter 10: Selecting and Marketing Technologies
The adoption of the Blair VIP latrine as a standard tech-nological choice in Zimbabwe in the 1980s had a pro-found impact on the ability of the government’s sanita-tion programme to go to scale. While the approachdoes allow for local innovation, in the choice of materi-als for the superstructure for example, the simplicity ofthe standard design, and the fact that it was developedin Zimbabwe from an analysis of the existing approachesand sanitation conditions, have both been significant fac-tors in its success. Once the design had been proven, anexplicit effort was made to roll out the program by build-ing the capacity of extension workers from the health de-partment, as well as through technical training of engi-neers and promotion of the technology at the nationaland local level. The impact of the Zimbabwean sanita-tion programme is clear; at the peak of the programmein 1987 nearly 50,000 latrines were built.
Despite the success of the Zimbabwean approach, stan-dardizing on a single technology may be problematic. Inmany countries, a range of technologies may be neededto reach all those households who are excluded. Whenthe NGO VERC started to work intensively in Bangla-deshi villages to identify sanitation and hygiene improve-ments, people themselves developed more than 20 vari-ations of low-cost latrines, which were both affordableand appropriate to their situation. By contrast the adop-tion of the TPPF as a standard in India led to high costsand constrained the roll out of the national program, de-spite the fact that the TPPF latrine is technically quite sat-isfactory as a rural technology. The TPPF was adoptedafter detailed research and benefited from the supportof UNICEF and other external support agencies active inwater supply and sanitation. But in this case technicaltraining of engineers, which focused on the TPPF left lit-tle room for local innovation.
The perils of defining “acceptable” sanitation technolo-gies may be avoided if policies and programmes focus onoutcomes rather than inputs. The Government of SouthAfrica defines “access to sanitation” in terms of the adop-tion of hygienic behaviours including safe disposal of exc-reta. This leaves projects and localities with freedom toadopt approaches which are locally appropriate, and forthe impact to be evaluated using simple indicators.
In many Latin American countries, levels of services forsanitation are relatively high and many urban householdsexpect to connect to a networked sewerage system. Inmany congested urban slums, this may be the only op-tion as there is no room for on-site disposal. But sewer-age is expensive. In Brazil an alternative approach to con-ventional sewerage, known as condominial sewerage,was developed over twenty years ago, and is now adopt-ed as standard in many cities and towns. Condominialapproaches are cheaper to build and operate than con-ventional systems, but have not expanded into neigh-bouring Latin American countries as fast as could havebeen expected. In Bolivia, the intervention of an exter-nal support agency (Swedish International DevelopmentCooperation Agency - SIDA) and support from theWater and Sanitation Program (WSP) enabled the gov-ernment and the private operator in La-Paz El-Alto toexperiment with the condominial approach. Externalsupport agencies in such a case can provide access toskills (technical or social development skills) and providefunds for activities which perhaps cannot initially be fund-ed from the governments’ own programme because therules and approaches being piloted fall outside the exist-ing government rules and standards.
In the arena of sanitation marketing, there is much lessexperience than in the area of direct technology devel-opment. Research from Africa shows that many small-scale-independent providers are relatively good at tai-loring their services to the needs of “customers”, but fewcountries have looked at ways to use the skills of the pri-vate sector, and marketing experts in particular, as partof a sanitation marketing effort. More work is needed toexplore this potentially important area of hygiene im-provement.
10.10 Practical Examples from the Field:What Sort of Sanitation do we Want?

Sanitation and Hygiene Promotion – Programming Guidance84
Case Study Box 8: What Sort of Sanitation do we Want?
Information about the adoption of Blair VIP latrines in Zimbabwe is taken from Robinson, A. (2002) VIP La-trines in Zimbabwe: From Local Innovation to Global Sanitation Solution Field Note 4 in the Blue-Gold Series, Waterand Sanitation Program – Africa Region, NairobiThe analysis of the impacts of India’s use of the TPPF latrine is based on Kolsky, P., E Bauman, R Bhatia, J.Chilton, C. van Wijk (2000) Learning from Experience: Evaluation of UNICEF”s Water and Environmental Sanita-tion Programme in India 1966-1998 Swedish International Development Cooperation Agency, StockholmDefinitions of Access are discussed in Evans, B., J. Davis and Cross, P. (2003) Water Supply and Sanitation inAfrica: Defining Access Paper presented at the SADC conference, Reaching the Millennium Development Goals,August 2003South Africa’s systematic reforms are described in Muller, M. (2002) The National Water and Sanitation Pro-gramme in South Africa: Turning the ‘Right to Water’ into Reality Field Note 7 in the Blue-Gold Series, Waterand Sanitation Program – Africa Region, Nairobi and Elledge, M.F., Rosensweig, F. and Warner, D.B. with J.Austin and E.A. Perez (2002) Guidelines for the Assessment of National Sanitation Policies Environmental HealthProject, Arlington VA p.4The El Alto experience is well documented on a dedicated website at www.wsp.org For an introduction tothe programme, and information on the costs and benefits of the approach see Foster, V. (n.d.) CondominialWater and Sewerage Systems – Costs of Implementation of the Model Water and Santitation Progam, Vice Min-istry of Basic Services (Government of Bolivia), Swedish international Development Cooperation Agency. A discussion of the role of small-scale-independent providers is in Collignon, B. and M. Vezina (2000) Inde-pendent Water and Sanitation Providers in African Cities: Full Report of a Ten-Country Study WSP
Notes for Chapter 10
i In urban situations, the cost of providing what is sometimes the only‘allowable’ technology – conventional sewerage – also swamps theprovider (usually the utility) who may respond by doing nothing.
ii This option will have high operating costs if pumping is required. Non-conventional approaches to sewerage (variations on the “small bore”or “shallow” sewer) may reduce operating costs.
iii cited in Cairncross, A.M. Sanitation and Water Supply: PracticalLessons from the Decade. World Bank Water and Sanitation Discus-sion Paper Number 9. World Bank: Washington, D.C.

Water, Sanitation and Hygiene
San
itati
on
an
d H
ygie
ne P
rom
oti
on
– P
rogra
mm
ing G
uid
an
ce
Sanitation andHygiene Promotion
Programming GuidanceISBN 92 4 159303 2
This document was jointly produced by the following organisations:
London School of Hygiene & Tropical Medicine (LSHTM)Keppel Street, London WC1E 7HT, United KingdomTel: +44 20 7636 8636 Fax: +44 20 7436 5389Website: www.lshtm.ac.uk
Pan American Health Organization (PAHO)Pan American Sanitary Bureau,Regional Office of the World Health Organization525 Twenty-third Street, N.W.Washington, D.C. 20037, United States of AmericaTel: +1 202 974 3000 Fax: +1 202 974 3663Website: www.paho.org
United Nations Children Fund (UNICEF)Water, Environment and Sanitation Programme Division3 UN Plaza, New York, NY 10017, United States of AmericaTel: +1 212 824 6307; +1 212 326 7371 Fax: +1 212 824 6480Website: www.unicef.org
U.S.Agency for International Development (USAID)Bureau for Global Health, Infectious Diseases DivisionEnvironmental Health Team, USAID/GH/HIDN/IDRonald Reagan Building,Washington, DC 20523-1000, United States of AmericaTel: +1 202 712 0000 Fax: +1 202 216 3524Websites: www.usaid.gov www.ehproject.org
Water, Engineering and Development Centre (WEDC)Loughborough University, Leicestershire LE11 3TU, United KingdomTel: +44 1509 222885 Fax: +44 1509 211079E-mail: [email protected] Website: www.wedc.ac.uk
Water and Sanitation Program (WSP)1818 H Street, N.W.,Washington, D.C. 20433, United States of AmericaTel: +1 202 473 9785 Fax: +1 202 522 3313, 522 3228E-mail: [email protected] Website: www.wsp.org
Water Supply and Sanitation Collaborative Council (WSSCC)International Environment House, 9 Chemin des Anémones,1219 Châtelaine, Geneva, SwitzerlandTel: +41 22 917 8657 Fax: +41 22 917 8084E-mail: [email protected] Website: www.wsscc.org
World Health Organisation (WHO)Avenue Appia 20, 1211 Geneva 27, SwitzerlandTel: +41 22 791 2111 Fax: +41 22 791 3111Email: [email protected] Website: www.who.int
WHO





























