Embed Size (px)
Citation preview

Selective Intracoronary Thrombolysisin Acute Myocardial Infarctionand Unstable Angina Pectoris
P. RENTROP, M.D., H. BLANKE, M.D., K. R. KARSCH, M.D., H. KAISER, M.D.,
H. KOSTERING, M.D., AND K. LEITZ, M.D.
SUMMARY Streptokinase was infused into the ischemia-related coronary artery at a rate of 1000-2000U/min for 15-95 minutes in 29 patients with acute myocardial infarction(AMI group) and in five patients withunstable angina pectoris (UAP group). Reopening of the completely obstructed vessel or increase of diameterat the site of subtotal lesions occurred in 22 AMI patients within 15-90 minutes of streptokinase infusion. Infour of these patients, antegrade flow to the distal segments of the infarct vessel was seen after intracoronarynitroglycerin or sublingual nifedipine administration, which preceded streptoklinase infusion, and in twopatients, streptokinase infusion was combined with recanalization by means of a guide wire. Chest pain wasalleviated after reperfusion; ejection fraction was 50.5 ± 12% before and 54.6 ± 9% immediately aftersuccessful intracoronary lysis (p < 0.05). Repeat angiography, performed 25 ± 11 days after the acute in-tervention in 19 AMI patients, revealed reocclusion of the infarct vessel in one patient. Aortocoronary bypasssurgery was performed electively in six AMI patients at varying intervals after successful lysis. Upon intra-operative inspection, the bulk of myocardium perfused by the recanalized vessel was found to be viable.
Intracoronary streptokinase infusion did not result in opening the complete obstruction or improvement oflumen at the site of subtotal lesions in seven AMI patients and in all UAP patients. The total dose of128,000 ± 36,000 U of streptokinase resulted in only minor decrease of fibrinogen, from 451 ± 93 mg% to430 ± 91 mg%. Bleeding from the arterial puncture site in two patients, the only complications that could beattributed to the procedure, was due to heparinization.
Intracoronary streptokinase application appears to be a safe and efficient method of achieving reperfusionand alleviating ischemia in the majority of patients with acute myocardial infarction. The method was notbeneficial in treating unstable angina pectoris, and its potential for salvage of myocardium is yet to beassessed.
IN A PREVIOUS STUDY, coronary angiographyperformed in 18 medically treated infarct patients dur-ing the acute and chronic stage revealed spontaneousrecanalization of the infarct vessel in 40% of thecases.' In another study, acutely occluded coronaryarteries could be recanalized mechanically by use ofguide wires and catheters in 10 patients.2 Repeatangiography in the chronic stage of myocardial infarc-tion showed increases in diameter of the recanaliza-tion canal in six of these patients. Most likely, thesefindings indicate endogenous lysis of coronary arterythrombi. As reported in a third study, selective infu-sion of low doses of streptokinase into the infarctvessel resulted in rapid recanalization or increasedluminal diameter in four of five patients with acute in-farction.3
In this report, we present the initial results andfollow-up data of the first 29 patients with acutemyocardial infarction (AMI) and five patients withunstable angina pectoris (UAP) who were treated byintracoronary streptokinase infusion.
From the Medizinische und Thoraxchirurgische Klinik derUniversit5t, Robert-Koch-Strasse 40, D-3400, Gottingen, WestGermany.Address for correspondence: Dr. P. Rentrop, Division of Car-
diology, Mount Sinai Medical Center, One Gustave L. Levy Place,New York, New York 10029.
Received February 1, 1980; revision accepted June 30, 1980.Circulation 63, No. 2, 1981.
307
Materials and Methods
Study Group
The study group consisted of 34 patients in whomacute coronary angiography was performed betweenJune 22, 1979 and March 30, 1980. The final diagnosisof AMI (patients 1-29) and UAP (patients 30-34) wasbased on serial CPK4 and CK-MB5 values. These en-zymes were normal in the UAP patients, but were in-creased to pathologic levels (peak CPK 879 ± 816U/1) in the AMI patients. All patients were admittedto the hospital because they had chest pain at rest thatlasted for more than 20 minutes, was not alleviated bysublingual nitroglycerin (NTG) and was presumed tobe due to myocardial ischemia. The admission ECGshowed changes compatible with acute myocardialischemia in all patients except patient 34. Patient 10was in cardiogenic shock (table 1) and patients 6, 7and 17 were considered to be hemodynamically un-stable. Patients 1, 6, 12, 22, 25 and 33 had a history ofmyocardial infarction.
Intracoronary streptokinase infusion was per-formed in all 34 patients. Acute angiography was notfollowed by intracoronary streptokinase infusion inpne patient not included in the study group, in whomthe ischemia-related coronary artery could not beidentified with certainty during the study period.Acute coronary angiography was not offered to infarctpatients in whom myocardial necrosis seemed to becompleted at the time of hospital admission (i.e., thosewho were already free of pain or had completely lost
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

VOL 63, No 2, FEBRUARY 1981
the R waves in the infarct-related ECG leads). Ad-ditional criteria for rejection were age older than 75years or severe associated diseases that would haveprecluded anticoagulation or subsequent bypass sur-gery.
Informed consent for the procedure was obtainedfrom the patient and from an accompanying relative ifpossible. An i.v. infusion of NTG at a rate of 1.5-6mg/hour was started in all patients in the emergencyroom shortly after admission, except in patient 10,who received i.v. dopamine, 1200 gtg/min, and highdoses of i.v. norepinephrine. Biplane left ventriculog-raphy (patient 10 excepted) and coronary angiog-raphy were performed within 1.5-15.5 hours (mean5.6 ± 4 hours) after the onset of the pain episode forwhich the patient was admitted to the hospital. Left-heart catheterization was performed as previouslydescribed.6 At the beginning of the study a bolus of10,000 U of heparin was administered intraarterially.
Acute Angiography and Intracoronary Interventions
The ischemia-related coronary artery was identifiedon the basis of electrocardiographic and angiographiccriteria: 23 AMI patients had acute ST elevations; twoAMI patients had symmetrical T-wave inversion(patients 20 and 21) and three AMI patients haddownward-sloping ST depression (patients 13, 24 and25). Coronary angiography revealed either a subtotalstenosis or occlusion of a corresponding vessel. Inpatient 13, in whom the ECG showed nonspecific ST-T changes, delayed clearing of contrast medium fromthe segment between the site of circumflex occlusionand the first proximal branch was taken as a sign ofacute obstruction.7 In the UAP group, patient 33 hadST elevation in the inferior leads and severe narrow-ing of the right coronary artery, and patients 30-32had symmetrical T-wave inversion in the left precor-dial chest leads and a high-degree stenosis of the leftanterior descending coronary artery. In patient 34,who had a normal preangiography ECG and three-vessel disease, only the circumflex lesion was subtotal.
Identification of the ischemia-related coronaryartery was followed by premedication for intra-coronary drug therapy: aspirin (1 g i.v.) was injectedto prevent formation of platelet thrombi and cortico-steroids (prednisolone 0.747 mg i.v. in most patients)were applied to avoid allergic reactions to strepto-kinase. The catheter that had been used for coronaryangiography was carefully placed in a stable positionin the ostium of the right or left main coronary artery.Direct contact of the catheter with the site of obstruc-tion or subselective catheterization of the ischemia-related vessel was avoided. A bolus of NTG (0.1-0.45mg) was injected into the coronary artery,7 followedby repeat injections of contrast medium after 30seconds and 3 minutes. Subsequently, patients 21-29received 10 mg of sublingual nifedipine, and the cor-onary artery was opacified 5 minutes later. Strepto-kinase (Deutsche KABI GmbH; 250,000 U dissolvedin 1 1 of normal saline solution) was infused into theischemia-related main vessel at a rate of 2000 U/min
through the coronary catheter. In patient 1, the rate ofstreptokinase infusion was 1000 U/min. In patients1-17, streptokinase infusion was preceded by intra-coronary injection of a bolus of streptokinase(10,000-20,000 U dissolved in 5 ml of normal saline).The soft tip of a 0.032-inch, movable-core guide wirewas passed beyond the obstruction before strep-tokinase infusion in patient 2 and after 78 minutes ofstreptokinase infusion in patient 25. Streptokinase in-fusion was interrupted for repeat injection of contrastmedium every 15 minutes or whenever there was achange of symptoms or ECG. (Leads I, II, III weremonitored continuously throughout the study.)Arterial blood pressure was determined every 5minutes.The streptokinase infusion was terminated after 60
minutes in the majority of patients to avoid majoralterations of coagulation factors. In patients 17-19,23, 25 and 28 the duration of enzyme infusion was ex-tended up to 95 minutes because the angiographicresult did not seem satisfactory after 60 minutes orbecause the patient still complained of chest pain. Inpatients 2-4, 9, 16 and 20, the infusion was terminatedearlier because reperfusion had been achieved andchest pain had subsided. The total dose of strep-tokinase was 128,000 i 36,000 U.
Follow-up Treatment
After completion of the streptokinase infusion, bothcoronary arteries were selectively visualized again andleft ventriculography was repeated in 18 AMIpatients.
In the coronary care unit, i.v. heparin was ad-ministered at a dose of 800-1200 U/hour for 4-7 days,followed by long-term anticoagulation with warfarinin the AMI patients in whom intracoronary lysis hadbeen angiographically successful (with the exceptionof patient 5). Clotting factors were determined beforeand after streptokinase application, and CPK4 andCK-MB5 were determined hourly until they returnedto normal.
Aortocoronary bypass surgery was performed atvarious intervals after the acute study in eight AMIand three UAP patients using standard techniques(table 1). Intraaortic balloon counterpulsation wasbegun in patient 6 immediately after the acute study.In patient 10, the attempt to place a balloon cathetervia the right and left femoral arteries during intra-coronary lysis was unsuccessful due to narrowing ofboth iliac arteries.
Angiography was repeated 15-81 days after theacute study in 22 AMI patients (patients 1, 2, 13 and27 after bypass surgery) and in three UAP patients.8 9At restudy, all patients were being administeredisosorbide dinitrate, fA blockers and warfarin.
Evaluation of Angiographic Data
The severity of coronary artery lesions was deter-mined by the criteria suggested by Gensini.'0 In-tracoronary intervention (streptokinase infusion,
308 CIRCULATION
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

INTRACORONARY THROMBOLYSIS/Rentrop et al.
4_A-4 -4 4% -
0.-
4 -4 m~~~~~~~~~~~~~~~~~~~~~~~ P..I C P-H -4.~
.:D ' ~c + ;S+P-~4 bLJ5 c c
¢ 0i-cc ¢V., mM m;--I .
ort- o t-o"-4 7- -4 P-4 c.~
LC I b lI oX 1
m CD c- C.] 0 0 00c Cocm m cq c1c 0
n ~ ~~~~~II < K
o+ cooc_ ~oo e> < od c C iK e In. ro 1 . c
10
WPb0
~ X-cgU
.
~ 0b U-VS
S ;00
-V 0.0 M
0 90
0-
(0-v4
0
>1
0
-o i
-¢ P4W >g ,
00Cv
0
0(o-
m U;:¢
0
CO10Cch-
Ct
00 ce
cc VE0
+ s s. + + + M t + + +
Vi bA)+ cc pis
¢a
a-40
0
0
0
¢~vl
0
rnaQ3i
0GC
0
c00
v1
0
Q
0V-4oz
00
¢cO d= z c=V);4 C
bi .4b
0
00WV~
0
C)0~
in
1-4
0
Qv-
0 0
c ¢.!
a0
10
o:
CW¢~
r-
C)P-
-In
V V. ;4-4b~
009 c
v0C)0
0
0
c
0
UVc
10100
Uv~
a-40
aVi0c
t-0)C
oi ccn (o i- c C c0 r-ol cm-4 r-4 V-4 -4
c
0
0
00
0
¢~
V=
C.V~
8
+ ts +
a0
a
:"
c)0
0
VI
P:
0
0
-0Z:U2
WP:
0)r-t-
in
0C)0
l-r
10
0
0
0
0
00ccVO
dit) cc - 00-4-4 .. -4 P-4-4
mppW
C)
0
309
cDV.)0
I -..110~
+C|
~s :4
U C-0U
0V.)
0V.)
V.)
0L.
0V.)
V.)
V.)
0V.)
0
I.Q
1.4c3c
o r.
V.0C)
V.)
c
VI)-4
0
12
0
.f
m
--C0
¢..
mV
a.)0V.)
pp
0ta)03 0
p O
P-(
8¢-
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

CIRCULATION VOL 63, No 2, FEBRUARY 1981
,)
-C.WJ7
a.)
100
C~ C~cc 4: ccF.., bL4;.
b£* tb
It
a0)C.)900
-
Cl00
br
00 iiCO
m I
0I °
u.N~NC I1
Cl m LC< lK0 0 0 5 ez 0 uc 0 0c CC] Cl Cl m -l c - T-
r 00 C:0 cO Cl t O O b -
CO0 CCncc in CO e: CO e9 NI
1 2INl -
CO Le cO ccCO tic ~c
_)03 b¢et_ a
+
c
C.r- ~-r
0~ ~O
s_*U-° U
+ +
N 00 n.zCd;. in it ¢be t.¢ e¢
ad
.00)_cZo 0
0
0
0
CZm
U
ct
^ - o, t:. )
N W U c-,
+ + + s
0
0
-)0)
.0,c
Q4
¢r 0U¢4
00
0~ 0 + 0~
~>) +4--.,)
-4 ~ P.' C4-
C3 0 n- -' w
O bp¢ ¢-b
-1-
Z ct ~P
c3
.0 40)4X 4D S
_¢ ¢cm bfl-4ir_
0l)
0)"
a) 0 0
0
<
h OoC
00¢~0U
v~
-
c0N
0Uv~
0
OClC--~~~~~~~~~c
cl,
C(0000CO
0000COm
Cd cB¢ 0
.0 _0
m m
-
cl
-4 cl u: c:o 00 Cl 14CN Cl Cl N Cl Cl c Cl Cl CO CO CO CO m
310
000pp
c;
0.0)
0W
;4
4 ¢~
t ¢ -
¢- X, cq
C.)-00
0W
C.
C.).50sH. 1- oc
¢<0
01C
0 _
O ii
-w vC;
0Q
*5Q 0
* II.0-4-
a)
;0c3d
C --0 0
oc
C;.W ed
0)
c3
;.0)
C.)
U2S-
0
0
.1-
0p
0
0
-)00
10
oj
C.
8r--
p
¢
In
m
0
0~
04-s10)
bI0
ccS
0
.04-
0)
0
40).0
CO0-m
0_)
W Pq cr o
lic
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

INTRACORONARY THROMBOLYSIS/Rentrop et al.
NTG bolus, guide-wire recanalization) or sublingualapplication of nifedipine was considered successful ifantegrade flow beyond an initially total obstructionwas shown or if there was clear-cut increase ofdiameter at the site of subtotal obstruction as deter-mined by angiography. Local wall motion of the leftventricle was qualitatively assessed from biplanecineventriculograms."1' 12 Volumes were determinedusing the area-length method of Dodge et al.'3 Dataare presented as mean ± SD. Differences betweenmean values were assessed by means of the paired ttest.
ResultsAcute Myocardial Infarction Group
Changes in Coronary Artery MorphologyThe initial injection of contrast medium showed
total occlusion of the ischemia-related coronary arteryin 20 patients and subtotal lesions in the remainingnine patients (table 1). All AMI patients had wall mo-tion abnormalities corresponding to the perfusion areaof the ischemia-related vessel.
Intracoronary streptokinase infusion alone or incombination with other measures was successful byangiographic criteria in 22 of 29 infarct patients(AMI, group); the acute interventions did not result inopening the infarct vessel or in an increase of diameterat the site of subtotal lesions in seven infarct patients(AMI2 group).
In five AMI, patients, interventions precedingstreptokinase infusion were successful: Intracoronaryapplication of NTG resulted in angiographicallydemonstrable changes in three patients; in patients 3and 29, the initial total obstructions of the right andleft anterior descending coronary arteries, respec-tively, were subtotal after intracoronary injection ofNTG. There was more rapid and complete distal fill-ing of the subtotally occluded circumflex branch inpatient 4. After sublingual application of nifedipine,the initially total obstruction of the left anterior de-scending coronary artery in patient 21 was subtotal. Inpatient 2 there was delayed antegrade flow to the mid-dle third of the left anterior descending coronaryartery after a guide wire had been passed through theocclusion. In these five patients there was definite ad-ditional improvement in luminal diameter at the siteof previous obstruction during streptokinase infusion.
In four patients with primary subtotal lesions(patients 12, 14, 20 and 24) that did not respond to in-tracoronary NTG or sublingual nifedipine, the degreeof narrowing decreased during intracoronary lysis. In12 patients with initially complete obstruction of theinfarct vessel in whom the interventions precedingstreptokinase application were without effect,antegrade flow was established during intracoronarystreptokinase infusion (patients 5, 7, 8, 10, 11, 13, 15,17-19, 22 and 27) (figs. 1 and 2).The injection of contrast medium that showed
patency was immediately preceded by a sudden onsetof premature ventricular complexes in patients 5, 7,
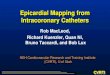
13, 18, 19, 27 and 29; in the remaining patients withcomplete occlusions, no arrhythmias and patencywere noted at the time of routine repeat opacification.Reopening of the infarct vessel was seen after 15-90minutes of intracoronary streptokinase infusion.There seemed to be a loose correlation between lysistime required to achieve reperfusion and duration ofsymptoms before the acute intervention (fig. 3).Subsequent injections of contrast medium showedprogressive increases in luminal diameter at the site ofprevious obstruction, as well as improvement of ante-grade flow (fig. 1). In patient 25, the obstruction of theright coronary artery appeared more convex after 78minutes of streptokinase infusion, but antegrade flowto the distal vessel was seen only after a guide wire hadbeen passed beyond the occlusion. This mechanical in-tervention was followed by streptokinase infusion for15 minutes, and the vessel remained patent.The final contrast injection showed 80-90% lesions
in the 22 AMI, patients in whom intracoronary lysiswas successful and a filling defect, suggestive ofthrombus, in one patient of this group (fig. 2B).Repeat angiography performed before hospital dis-charge 25 ± 11 days after the acute intervention in 19of these patients revealed reocclusion of the infarctvessel in patient 13, no change in 13 patients anddefinite further improvement in luminal diameter atthe site of the initial infarct lesion in patients 15, 17,19, 25 and 27 (fig. 2).The acute intervention was unsuccessful in seven
AMI patients (AMI2 group). Patients 1, 9, 16 and 26had subtotal lesions and patients 6, 23 and 28 hadcomplete obstruction of the infarct vessel. Partialrecanalization occurred during streptokinase infusionin two AMI2 patients with complete obstruction of theinfarct vessel. In patient 23, the filling defect becamemore convex and was partially stained by dye; inpatient 28, a 2.5-cm segment of the occluded right cor-onary artery was recanalized, but the infarct vesselremained obstructed distally in both patients. Repeatangiography performed 3 weeks after the acute in-tervention in the three AMI2 patients with completeocclusion showed patency of the infarct vessel inpatients 6 and 23 and persistent obstruction in patient28. Repeat angiography performed in the chronicstage in two AMI2 patients with subtotal lesions(patients 1 and 16) revealed no change of these lesions.
Changes in Left Ventricular Function
Left ventricular end-diastolic pressure (LVEDP)was determined before initial angiography and im-mediately after streptokinase infusion in 13 AMI,patients. LVEDP decreased from 20.4 ± 8.4 mm Hgto 15.7 ± 7.3 mm Hg (p < 0.005). At repeatangiography during the chronic stage of infarction,LVEDP was 15.9 ± 7.1 mm Hg in these patients.Ejection fraction, determined in 14 AMI, patientsbefore and immediately after the acute interventions,increased from 50.5 ± 12% to 54.6 ± 9% (p < 0.05).In the chronic stage of infarction, ejection fractionwas also significantly higher in these patients
311
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

VOL 63, No 2, FEBRUARY 1981
FIGURE 1. Left coronary artery in patient 7 (right anterior oblique projection). (A) Before lysis; (B) after 19 minutes of in-tracoronary streptokinase infttsion; (C) after 60 minutes of intracoronary lysi,; and (D) in the chronic stage of infirction.
(56.6 ± 12.4%) than before the acute intervention(p < 0.01). In comparison with the value after lysis,ejection fraction in the chronic stage was notsignificantly changed. Statistical analysis of hemo-dynamic changes was not possible in AMI patientsdue to the small number of cases (table 1).
Changes in SymptomsSymptoms could be evaluated only in 19 AMI1
patients. Two patients had received analgesic medica-tion at the beginning of the study and one patient wasin shock.
Four AMI1 patients became asymptomatic before
the intracoronary interventions after initiation of i.v.NTG therapy. One patient was free of pain 5 minutesafter intracoronary application of NTG. Thirteen ofthe remaining 14 patients who still had chest pain atthe beginning of the intracoronary streptokinase infu-sion were asymptomatic when the streptokinase infu-sion was terminated; the remaining patient notedmarked improvement of chest pain immediately afterguide-wire recanalization, although she was not com-pletely asymptomatic at the end of the streptokinaseinfusion. Improvement of symptoms occurred eitherimmediately before or within 10 minutes afterangiographic demonstration of reperfusion in patientsin whom the infarct vessel was completely obstructed.
312 CIRCULATION
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

INTRACORONARY THROMBOLYSIS/Rentrop et al.
FIGURE 2. Right coronary artery in patient 15 (leJianterior oblique projection). (A) Bejore lysis; (B) aJter 60minutes ofintracoronary streptokinase infusion; (C) in thechronic stage of inJdrction.
Lysis time tillreperfusion
[ min]
90 _ 013
80
70
60
50 08018
40 015 017
011
30 - 019
20 07022010 05
10
271 1 1 1 -
2 4 6 8 10 12 14Duration of symptoms (hours]
FiCULRi 3. Relationiship between duration of chest painbefoire acute anigiographv anid intracoronarj lysi.s time re-quired to achieve reperJuision in 12 patients with c,onipleteobstrufction of the inifarct-related vessel.
Chest pain did not improve in two of the threeAMI2 patients with complete occlusion of the infarctvessel. The third patient of this subgroup receivedanalgesic medication. The four AMI2 patients withsubtotal obstruction of the infarct vessel becameasymptomatic before intracoronary intervention afterinitiation of i.v. NTG therapy.
ECG Changes
ST elevation of more than I mV was present in 17AMI1 patients before the acute study. ST elevationwas unchanged in only one of these patients after com-pletion of the streptokinase infusion and was reducedin seven patients. In eight patients, the ST-segmenthad returned to baseline. There were no follow-upECGs in patient 10, who was in cardiogenic shock.Two of the three AMI2 patients with complete
obstruction of the infarct vessel had ST elevation thatwas unchanged after the acute study. The four AMI2patients with subtotal lesions of the infarct vessel hadelevated ST segments before the acute study thatreturned to the baseline after completion of the in-tervention.
Pathologic Q waves were present before the acutestudy in seven AMI1 patients. The ECG obtained afterintracoronary lysis showed new Q waves in one AMI1patient; development of Q waves in subsequent ECGswas noted in two additional AMI1 patients. Patho-
313
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

VOL 63, No 2, FEBRUARY 1981
logic Q waves did not disappear after reperfusion.The admission ECG of one AMI2 patient with com-
plete obstruction of the infarct vessel showed patho-logic Q waves; the remaining two patients of this sub-group developed pathologic Q waves in the coronarycare unit. Immediate or late development of new Qwaves was not observed in the four AMI2 patients withsubtotal lesions of the infarct vessel.Complications and Hospital Course
In patient 10, who died 3 hours after reperfusion,systolic left ventricular pressure could not be raisedabove 60 mm Hg before intracoronary streptokinaseapplication, despite maximal doses of vasopressors.Coronary angiography revealed occlusion of the leftanterior descending and right coronary arteries andabsence of collaterals. Streptokinase infusion into theright coronary artery resulted in patency within 15minutes. Subsequently, left ventricular pressure rosetransiently to 85 mm Hg. An intraaortic ballooncatheter could not be passed beyond the iliac arteriesdue to peripheral atherosclerosis. Ventricular fibrilla-tion occurred repeatedly before and after reperfusion.'The patient died in refractory cardiogenic shock.Autopsy revealed acute anteroseptal and inferior in-farction, acute occlusion of the left anterior descend-ing coronary artery and atheromatous narrowing ofthe right coronary artery with an intimal tear andremnants of an acute thrombus.
Patient 5, who was not placed on full-dose, long-term anticoagulants because of arterial hypertension,suffered an anteroseptal reinfarction 34 days after theacute study and died in cardiogenic shock. Patient 11died suddenly 10 weeks after the acute interventionand 7 days after bypass surgery. Autopsy revealedfresh thrombotic occlusion of a vein graft. All otherpatients were alive and well at the time of submissionof this paper.
In patients 2 and 5, surgical revision of a femoralartery puncture was necessary after the acute studydue to local hemorrhage. Fibrinogen had fallen from480 mg% to 450 mg% in patient 2 and from 600 mg%to 480 mg% in patient 5. After the acute interventionin both patients, thrombin time was more than 5minutes.
Ventricular fibrillation, which occurred in patient 3when a transvenous pacemaker wire was advancedinto the right ventricle during the acute study, could becontrolled by defibrillation.The premature ventricular complexes that im-
mediately preceded angiographic demonstration ofreperfusion in seven patients subsided spontaneouslywithin 10 minutes in six patients. In patient 29, thepremature ventricular complexes were multifocal,refractory to i.v. xylocaine and persisted for 30minutes. Three and one-half hours after reperfusionthis patient had a short bout of ventricular fibrillationthat stopped spontaneously. Patient 2 had ventricularfibrillation 18 hours after the acute study.To date, aortocoronary bypass surgery has been
performed within 1 day to 8 weeks after reperfusion insix AMI1 patients and is scheduled to be performed in
dications for surgery were recurrent ischemic chestpain at rest in two patients and during exercise inseven patients. The first patient (patient 2) wasoperated because of ventricular fibrillation in thepresence of a high-degree lesion of the left anteriordescending coronary artery. Intraoperative inspectionrevealed active contraction of the segments perfusedby the infarct vessel in all six AMI1 patients. Grafts tothe infarct vessel were constructed in five of thesepatients; in patient 14 the distal RCA was not graft-able (table 1). In two AMI2 patients (patients 1 and26), the subtotally obstructed left anterior descendingcoronary artery did not respond to intracoronaryNTG or lysis and had to be revascularized because ofpersistent pain.
Unstable Angina Pectoris Group
The most severe coronary artery lesions in the fivepatients with UAP were subtotal lesions. In-tracoronary injection of NTG and infusion of strep-tokinase did not result in an angiographicallydemonstrable change in luminal diameter at the site ofsubtotal obstruction in any of these patients.
Four UAP patients became asymptomatic beforethe acute study, after therapy with i.v. NTG had beeninitiated. Patient 31, who complained of angina pec-toris during the study and during intracoronary strep-tokinase infusion, became transiently asymptomaticafterwards, when his blood pressure was lowered by ani.v. sodium nitroprusside infusion. Subsequently,patient 33 could be kept stable on oral nitrates and fiblockers. Patient 30 developed delirium tremens andhis symptoms could not be evaluated; follow-up ECGsshowed repeatedly deep symmetrical T-wave inversionwithout enzyme rise. He finally stabilized on medicaltherapy. Patients 31, 32 and 34 could not be weanedfrom parenteral medication (NTG or nitroprusside)without developing severe ischemic pain associatedwith transient ST-T changes. Stabilization wasachieved by aortocoronary bypass surgery in thesepatients.
Clotting Factors
Clotting factors were determined in all AMIpatients (patient 10 excepted) and in all UAP patients(table 2). Systemic fibrinogen and plasminogen valuesdecreased only slightly after intracoronary lysis.Fibrin monomer complexes were elevated before thestudy and normal after completion of lysis. Thrombintime and thromboplastin time, which were determinedbefore administration of streptokinase but after intra-arterial administration of heparin (10,000 U), weremarkedly prolonged immediately before and afterlysis therapy and remained in a therapeutic range 12hours later (table 2).
DiscussionThe Coronary Arteries in Acute Ischemic Syndromes
In all patients who received intracoronary strepto-an additional four AMI1 patients (table 1). The in-
314 CIRCULATION
kinase therapy, identification of the ischem-ia-rel a-ted
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

INTRACORONARY THROMBOLYSIS/Rentrop et al.
TABLE 2. Clotting Factors Before, Immediately After and 12 Hours After Streptokinase Therapy
Thromboplastin Thrombin Fibrin monomerFibrinogen time* time PTT complexes [g%] Plasminogen*(mg%) (Quick %) (sec) (sec) (normal: 0-0.1 mg i.v.) (mg%)
Before therapy 451.67 92.51 49.90 - 16.16 295.54 - 17.51 297.05 4.37 0.521 - 0.272 15.96 - 2.01
Immediatelyafter therapy 413.45 81.57 46.19 - 16.48 296.74 - 13.51 289.50 6.89 0.062 - 0.129 13.47 - 1.85
12 hours aftertherapy 437.83 112.78 75.39 17.23 42.60 20.37 72.13 6.57 14.13 1.94
*n= 22.
coronary artery appeared to be possible based on theacute electrocardiographic and angiographic find-ings. In patient 10, the admission ECG showed signsof an acute inferior and a remote anteroseptal infarc-tion; the autopsy revealed acute necrosis of both theinferior and the anteroseptal wall.
Rapid recanalization of occluded vessels and im-provement of lumen at the site of high-degree lesionsduring intracoronary streptokinase infusion implythat fresh thrombotic material was present at the siteof obstruction in 21 of 29 patients. Also, there wasmost likely thrombotic occlusion in the three AMI2patients in whom antegrade flow was not establishedduring the acute procedure: partial recanalization oc-curred during streptokinase administration in two ofthese patients, and repeat angiography performed inthe chronic stage revealed patency of the infarct vesselin the third patient. Our findings are in agreement withthose of most pathologists, who found fresh coronarythrombosis in the majority of patients with acutemyocardial infarction." Thrombotic occlusion wasusually seen at the site of high-degree atheroscleroticlesions in pathologic studies. In our patients, thenarrowing that persisted after intracoronary lysis andwas still present at repeat angiography in the chronicstage of infarction was most likely due to athero-sclerosis.Improved distal filling or patency of the infarct
vessel after intracoronary application of NTG, whichoccurred in three AMI patients, may be due to an in-crease in caliber of the large conductive vessels,"5 or itmay be evidence of spasm, as suggested by Oliva. Thepossibility of spasm cannot be ruled out in the vesselsthat failed to respond to intracoronary NTG. Inpatient 21, for example, antegrade filling of the ini-tially obstructed infarct vessel occurred after sub-lingual administration of nifedipine. In all fourpatients in whom there was possible evidence of cor-onary artery spasm, the subsequent infusion of strep-tokinase resulted in additional and more marked im-provement of lumen.
Intracoronary infusion of streptokinase did notresult in angiographically demonstrable changes infour AMI patients who had subtotal lesions or in allfive UAP patients who also had subtotal lesions. Mostlikely, narrowing of the ischemia-related coronaryartery was not due to fresh thrombotic material inthese nine patients, and there was no evidence of cor-onary artery spasm.
Alleviation of Acute Myocardial Ischemia
In agreement with animal experiments, rapiddecrease of ST-segment elevation was seen in the ma-jority of patients after reperfusion. Decrease of STelevation has been interpreted as indirect evidence ofsalvage of myocardium by some investigators,'8 and aspossible consequence of accelerated cell necrosis byothers.'7' 1' Rapid alleviation of ischemic pain duringstreptokinase infusion in AMI, patients could be ex-plained by the same two mechanisms. Extension ofcell necrosis seems unlikely, however, because ejectionfraction was increased immediately after strepto-kinase infusion. Intraoperative inspection in sixpatients revealed the bulk of myocardium perfused bythe recanalized vessels to be viable.
Persistence of chest pain throughout the acute studyin the two AMI2 patients who had complete obstruc-tion of the infarct vessel and did not receive opiates in-dicates that myocardial ischemia was not alleviated.In the four AMI2 patients and the five UAP patientswho had subtotal lesions of the infarct vessel, chestpain was alleviated after reduction of preload andafterload by medical therapy. The ischemic episodeswere probably caused by increased myocardial oxygendemand in the presence of high-degree fixed coronaryartery lesions in these subgroups.Technical Aspects of Intracoronary Thrombolysis
The regimen of local lysis used in this study wassuccessful in the 22 AMI, patients as judged byalleviation of symptoms and angiographic changes.Apparently, not all thrombotic material had been dis-solved at the end of the acute intervention in some ofthese patients, as shown by the additional improve-ment of lumen during the chronic stage in five AMI,patients. Our technique was insufficient in three AMI2patients in whom only partial or delayed recanaliza-tion of the infarct vessel was achieved.
In animal experiments, Kanmatsuse et al.1' showedthat the efficiency of intracoronary thrombolysisdepends upon the amount of lytic substance infusedper minute and on the distance between the thrombusand the tip of the infusion catheter. In the presentstudy, the infusion catheter was placed in the ostiumof the right or left coronary artery. Distal placementor subselective catheterization of obstructed brancheswas not attempted for the sake of safety, rapidity andsimplicity of the procedure.The rate of streptokinase infusion was selected on
315
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

VOL 63, No 2, FEBRUARY 1981
the basis of experience with local lysis in peripheralvessels.20 The total dose of streptokinase infusion waslimited to a maximum of 220,000 U to avoid strepto-kinase-induced coagulation disorders, which would in-terfere with possible emergency surgery. In a prelimi-nary study,21 no significant change of fibrinogen orplasminogen was seen after rapid infusion of a totaldose of 50,000-100,000 U of streptokinase. However,there was a significant, albeit moderate, reduction ofboth fibrinogen and plasminogen after 275,000 U ofstreptokinase. In the present study, only minordecrease of systemic fibrinogen and plasminogenlevels was observed. Bleeding from the arterial punc-ture site in two patients was due to heparinization,which resulted in marked prolongation of thrombintime, rather than to fibrinolytic therapy.
Reperfusion might be achieved more efficiently byvarious modifications of the technique, e.g., increaseof streptokinase dosage, subselective infusion viasmall special catheters,'9 more aggressive use ofmechanical devices or different thrombolytic sub-stances. Each of these modifications could increase therisk of the intervention.
In animal experiments, sudden release of mechan-ical coronary artery occlusion frequently results indangerous arrhythmias.22 Moschos et al.23 observedthat serious arrhythmias were less frequent if reperfu-sion was achieved gradually by intracoronary lysis. Inour patients, ventricular flutter or fibrillation did notoccur immediately after reperfusion, although ven-tricular premature complexes that were not presentbefore the acute study developed in seven patients. Inone, patient 29, the premature ventricular complexeswere multifocal and lasted for 30 minutes. It cannot bedetermined if ventricular fibrillation occurring 3 1½2hours later in this patient and 18 hours after the acutestudy in patient 2 were related to reperfusion.
Aortocoronary Bypass SurgeryAfter Intracoronary Thrombolysis
Reperfusion in acute myocardial infarction hasbeen achieved by aortocoronary bypass surgery.24 26Intracoronary interventions performed immediatelyafter diagnostic angiography resulted in more rapidreperfusion in 22 patients of this study. Optimalfollow-up management of these patients has not beendefined. There is a risk of reocclusion at the site of thepersisting high-degree lesion. Reocclusion wasdocumented angiographically in one patient in ourseries. It has been our policy to attempt stabilizationon medical therapy, including anticoagulants, and toperform elective aortocoronary bypass surgery assoon as signs of myocardial ischemia reoccur. Aor-tocoronary bypass surgery was performed within 7days after reperfusion in three patients without peri-operative complications; the operation has been per-formed or scheduled in an additional seven patients ofthis group in the chronic stage of myocardial infarc-tion.The treatment of patients in whom the intra-
coronary interventions were unsuccessful followed
the same guidelines. In three patients with UAP andin two AMI2 patients with subtotal lesions, definitestabilization could not be accomplished by medicaltherapy alone but was achieved by aortocoronarybypass surgery.
References1. Blanke H, Rentrop P, Karsch KR, Kreuzer H: Coronary
angiographic and ventriculographic findings in the acute andchronic stage of myocardial infarction. Circulation 60 (supplII): 11-69, 1979
2. Rentrop P, Blanke H, Wiegand V, Karsch KR: Wieder-ero5ffnung verschlossener Kranzgefade im akuten Infarkt mitHilfe von Kathetern (Transluminale Rekanalisation). DtschMed Wochenschr 104: 1401, 1979
3. Rentrop P, Blanke H, Kdstering K, Karsch KR: Acute myocar-dial infarction: intracoronary application of nitroglycerin andstreptokinase in combination with transluminal recanalization.Clin Cardiol 5: 354, 1979
4. Szasz G, Grube W, Bernt E: Creatine kinase in serum. 1. Deter-mination of optimum reaction conditions. Clin Chem 22: 650,1976
5. Wuirzburg U, Hennrich N, Orth HD, Lang M, Prellwitz W,Neumeier D, Knedel M, Rick W: Quantitative determinationof creatine kinase isoenzyme catalytic concentrations in serumusing immunological methods. J Clin Chem Clin Biochem I5:131, 1977
6. Rentrop P, Blanke H, Karsch KR, Kreuzer H: Koronar-morphologie und links-ventrikulire Pumpfunktion im akutenInfarktstadium und ihre Anderungen im chronischen Stadium.Z Kardiol 68: 335, 1979
7. Oliva PB, Breckinridge JC: Arteriographic evidence of cor-onary spasm in acute myocardial infarction. Circulation 56:366, 1977
8. Sones FM: Cine coronary angiography. Mod Concepts Car-diovasc Dis 31: 735, 1962
9. Judkins MP: Selective coronary arteriography. Part I. A per-cutaneous transfemoral technique. Radiology 89: 815, 1967
10. Gensini GG: Coronary Angiography. Mount Kisco, New York,Futura Publishing Co, 1975
11. AHA Committee Report: A reporting system on patientsevaluated for coronary artery disease. Circulation 51: 5, 1975
12. Herman MV. Heinle RA, Klein MD, Gorlin R: Localized dis-orders in myocardial contraction. N Engl J Med 277: 222, 1967
13. Dodge HT, Sandler H, Baxley WA, Hawley RR: Usefulnessand limitations of radiographic methods for determining leftventricular volume. Am J Cardiol 18: 10, 1966
14. Chandler AB, Chapman I, Erhardt LR, Roberts WC, SchwartzCJ, Sinapius D, Spain DM, Sherry S, Ness PM, Simon TL:Coronary thrombosis in myocardial infarction. Am J Cardiol34: 823, 1974
15. Likoff W, Kasparian H, Lehman JS, Segal BL: Evaluation of"coronary vasodilators" by coronary arteriography. Am J Car-diol 13: 7, 1964
16. Maroko PR, Libby P, Ginks WR, Bloor CM, Shell WE, SobelBE, Ross J Jr: Coronary artery reperfusion. I. Early effects onlocal myocardial function and the extent of myocardialnecrosis. J Clin Invest 51: 2710, 1972
17. Deloche A, Fabiani JN, Camilleri JP, Relland J, Joseph D,Carpentier A, Dubost DH: The effect of coronary artery reper-fusion on the extent of myocardial infarction. Am Heart J 93:358, 1977
18. Capone RJ, Most AS: Myocardial hemorrhage after coronaryreperfusion in pigs. Am J Cardiol 41: 259, 1978
19. Kanmatsuse K, Lando U, Mercier JC, Fishbein MC, SwanHJC, Ganz W: Rapid lysis of coronary thrombi by localapplication of fibrinolysin. Circulation 60 (suppl II): 11-216,1979
20. Kostering H, Barth U, Naidu R: Changes of antistrep-tokinasetiter following long term streptokinase therapy. AktProbl Angiol 37: 110, 1978
21. Ko5stering H, Rentrop P, Ganasinski J, Karsch KR, Blanke H:
316 CIRCULATION
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

CORONARY ARTERY REPERFUSION/Baughman et al.
Lokale Streptokinasebehandlung bei Patienten mit akutemMyokardinfarkt oder instabiler Angina. Blut 40: 56, 1980
22. Sommers HM, Jennings RB: The influence of procaine amideand oxygen on the onset of ventricular fibrillation followingtemporary occlusion of the left circumflex coronary artery. FedProc 23: 444, 1964
23. Moschos CB, Burke WM, Lehan PH, Oldewurtel HA, ReganTJ: Thrombolytic agents and lysis of coronary artery throm-bosis. Cardiovasc Res 4: 228, 1970
24. Berg R Jr, Kendall RW, Duvoisin GE, Ganji JH, Rudy LW,Everhart FJ: Acute myocardial infarction. J Thorac CardiovascSurg 70: 432, 1975
25. Bolooki H, Vargas A: Myocardial revascularization after acutemyocardial infarction. Arch Surg 111: 1216, 1976
26. Phillips SJ, Kongtahworn C, Zeff RH, Benson M, lannone L,Brown T, Gordon DF: Emergency coronary arteryrevascularization: a possible therapy for acute myocardial in-farction. Circulation 60: 241, 1979
Effects of Coronary Artery Reperfusionon Myocardial Infarct Size and
Survival in Conscious DogsKENNETH L. BAUGHMAN, M.D., PETER R. MAROKO, M.D., AND STEPHEN F. VATNER, M.D.
SUMMARY The effects of coronary artery reperfusion at 1 and 3 hours after coronary artery occlusionwere examined on myocardial infarct size and survival in conscious dogs. Left circumflex coronary arteryocclusion was induced by inflating an hydraulic occluder and confirmed thereafter by measuring the absence ofcoronary blood flow. Of the 77 dogs that underwent coronary artery occlusion, 18 died within 1 hour. Of the 59remaining dogs, permanent coronary artery occlusion was carried out in 31 dogs, 12 underwent reperfusionafter 1 hour and 16 underwent reperfusion after 3 hours. Survival at 1 week was enhanced significantly (p <0.01) by reperfusion carried out at either 1 or 3 hours; only 29% of dogs with permanent coronary artery occlu-sion survived, whereas 83% and 75% of dogs survived 1 week with reperfusion at 1 hour and 3 hours, respec-tively. Average infarct size at 1 week was smaller in dogs with reperfusion (NS). The inability to reachstatistical significance was most likely the result of two factors: (1) There was a marked variation in infarctsize in dogs with permanent coronary artery occlusion infarcts averaged 21.3 ± 7.5% and ranged from 0.7-72.6% of the left ventricle. (2) Dogs that died 1-7 days after coronary artery occlusion had significantly (p <0.05) larger infarcts (40 ± 4% of left ventricle) than those that survived 1 week in any of the three groups.Thus, if all dogs had survived 1 week, a beneficial effect on infarct size could have been demonstrated.Nevertheless, coronary artery reperfusion at either 1 or 3 hours after coronary artery occlusion induces a strik-ing beneficial effect on survival, which is of the utmost clinical significance.
CORONARY ARTERY REPERFUSION in theform of coronary artery bypass has become one of themost important therapeutic interventions in medicalpractice. This procedure is most frequently carried outin patients with chronic coronary artery disease, but isalso used in patients with acute myocardial ischemiaand infarction." 2 The physiologic basis for the valueof this intervention is controversial, particularly in theacute phase of myocardial infarction. The results fromexperimental studies in anesthetized animal modelshave conflicted, showing either considerable improve-
From the Department of Medicine, Harvard Medical School andPeter Bent Brigham Hospital, Boston, and the New EnglandRegional Primate Research Center, Southboro, Massachusetts.
Dr. Baughman's current address: Department of Medicine, TheJohns Hopkins Hospital, Baltimore, Maryland.
Dr. Maroko's current address: Deborah Heart and Lung Center,Brown Mills, New Jersey.
Supported in part by USPHS grants HL 17459 and HL 26215.Address for correspondence: Stephen F. Vatner, M.D., New
England Regional Primate Research Center, One Pine Hill Drive,Southboro, Massachusetts 01772.
Received March 13, 1980; revision accepted July 8, 1980.Circulation 63, No. 2, 1981.
ment3 6 or adverse effects.7 9 Little has been done inconscious animal models, although anesthesia exertsprofound effects on cardiovascular control. However,Bresnahan et al.,'0 in a study of conscious dogs, notedthat infarct size was frequently exacerbated by reper-fusion. A recent study from our laboratory in con-scious dogs indicated that coronary artery reperfusiondid not modify the extent of myocardial infarctionsignificantly." In both of these studies, infarct size wasassessed only 1 day after coronary artery occlusionand reperfusion. The nearly uniform presence ofhemorrhagic infarction in dogs sacrificed 24 hoursafter coronary artery reperfusion could have com-plicated the assessment of infarct size. Moreover, thetime period was too brief to permit evaluation of theeffects of coronary reperfusion on survival.The goal of the present investigation was to deter-
mine if coronary artery reperfusion at either 1 or 3hours after coronary artery occlusion exertedbeneficial effects in the conscious animal if the animalswere sacrificed 1 week after occlusion. In this manner,the longer-term salutary effects of the interventioncould be assessed in the absence of acute complicatingfactors, e.g., hemorrhagic infarction, which is known
317
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

P Rentrop, H Blanke, K R Karsch, H Kaiser, H Köstering and K Leitzpectoris.
Selective intracoronary thrombolysis in acute myocardial infarction and unstable angina
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1981 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.63.2.307
1981;63:307-317Circulation.
http://circ.ahajournals.org/content/63/2/307.citationthe World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from