Embed Size (px)
Citation preview

27th Annual SW Conference on Medicine
Westin La Paloma SpaTucson
April 27-29
Edward G. Stiles, DO, FAAODist.Professor of OPP
Kentucky College of Osteopathic Medicine
Sturgill Distinguished ProfessorUniversity of Pikeville
Workshop: OMT principles & care

Sponsors:
• Tucson Osteopathic Medical Foundation
• Cleveland Clinic
Challenges for this workshop: Diversity of participants
• DOs: improve OPP knowledge & OMT skills• MDs: provide / improve OPP knowledge & skills
• NP: make aware of OPP potential• PA: make aware of OPP potential
• DO students: improve skills
Goals:
enable all to gain new OPP understanding and OMT skills

Greenman:
•“ the expert is the one who does the basics the best”•“what makes a DO different is not OMT,
but how they think / problem solve.”•Dispelling some OMT myths
• Something is not “out of place”: it can’t completely open or close.
• Your not “putting something back in place” but restoring physiological motion, doesn’t require a lot of force.
• OMT is not a panacea but can be dramatic when S/D is a major etiological component.
• One indication for OMT ! presence of somatic dysfunction ( S/D ) - not pain, muscle guarding, etc.
• Osteopathic Joint model: vs “out of place” model

Pardigm shifts:
• Amount of force utilized with OMT: Mitchell stool demonstration
• Stiles’ musculo-skeletal / mesokinetic model: Tensegrity• Need to find AGR / sequence: least healthy / functional area
•“Learn principles and get them to work for you”: Kimberly• Spinal mechanics: facet model
• Direct techniques• Demo the facet model for Dx and Rx ( thoracic, cervical & lumbar )
• Using translation to Dx and Rx: the KEY !• HV/LA thumb thrust ( Osteopathic Activator ) – Thoracic
• MET: using a patient specific muscle corrective force• T6-11 FRS dysfunctions MET ( 2 steps )• T12 FRS dysfunctions MET ( 2 steps )
• Indirect techniques ( Laughlin - Still ) thoracic, cervical & lumbar
• Sacral complexity: Left sacral Flexion ( use as example )
• Innominate: “fine-tuning”/ activating only prime mover• Ribs: basic Dx and Rx

Joint Mechanics:an
Osteopathic Perspective
( Normal and abnormal - somatic dysfunction )
What is Somatic dysfunction ?
( S/D )

Normal Joint Mechanics
A E P AEP
Active ROM
Passive ROM
• Elastic & Physiological barriers: provide support & movement• Hypermobility issue: hindered elastic barrier
• Workman’s Compensation: hypomobility significance
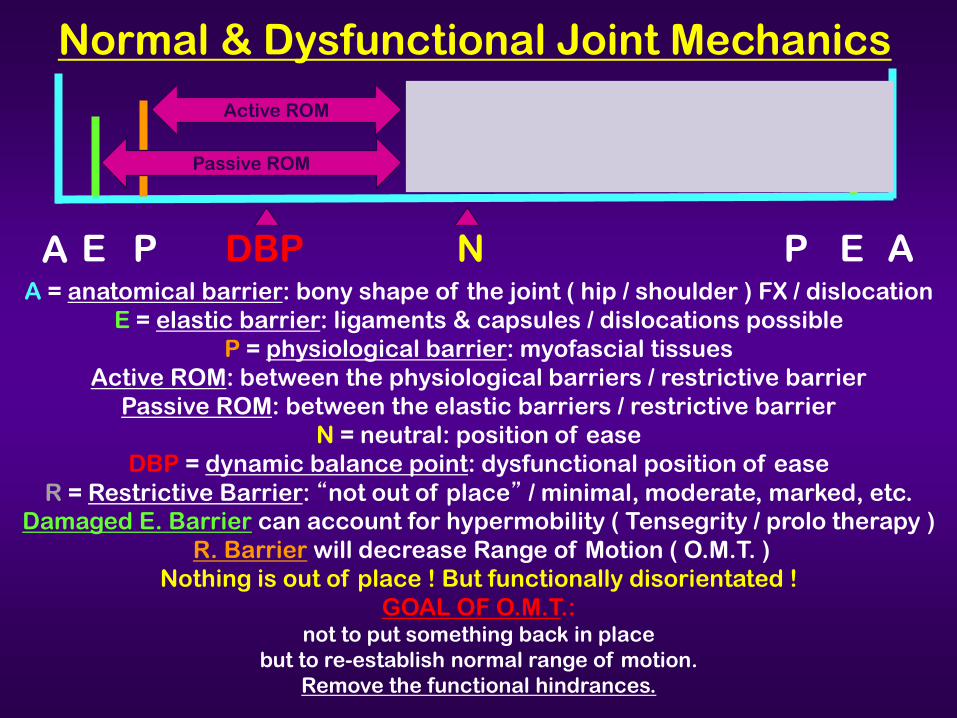
Normal & Dysfunctional Joint Mechanics
A E P AEPA = anatomical barrier: bony shape of the joint ( hip / shoulder ) FX / dislocation
E = elastic barrier: ligaments & capsules / dislocations possibleP = physiological barrier: myofascial tissues
Active ROM: between the physiological barriers / restrictive barrierPassive ROM: between the elastic barriers / restrictive barrier
N = neutral: position of easeDBP = dynamic balance point: dysfunctional position of ease
R = Restrictive Barrier: “not out of place” / minimal, moderate, marked, etc.Damaged E. Barrier can account for hypermobility ( Tensegrity / prolo therapy )
R. Barrier will decrease Range of Motion ( O.M.T. )Nothing is out of place ! But functionally disorientated !
GOAL OF O.M.T.: not to put something back in place
but to re-establish normal range of motion. Remove the functional hindrances.
NDBP
Active ROM
Passive ROM

CONSILIENCE:• E. O. WILSON PhD: HARVARD BIOLOGIST
• A “CALL FOR A UNITY OF ALL KNOWLEDGE”
NATURAL SYSTEMS ARE RESILIENT
UNTIL WE INTRODUCE MECHANISTIC INTERFACES –WITH ALL THE NECESSARY
ADJUSTMENTS AND COMPENSATIONS –AS A MEANS OF SUSTAINING OURSELVES.
THOSE INTERFACES NOT ONLY ISOLATE US FROM NATURE
BUT AT THE SAME TIME CREATE SYSTEMS
THAT AREBRITTLE AND DELICATE
• LOWERED RESISTANCE ?• INCREASED SUSCEPTIBLITY ?
• BECOME LESS NON-LINEAR ! FRAGILE• BECOME “DIS-EASED” HOST
A HARVARD DESCRIPTION OF Somatic Dysfucntion –H IMPACT ?
NOTE: EXCHANGE THE WORDS HOST AND S/D-H

Paradigm Shift:2018
looking at familiar data, come to new understanding &new way of explaining old observations
“Learn the principles and get themto work for you.”
Paul E. Kimberly, DO, FAAO
• Anatomical design• OMT mechanisms

The Musculo-Skeletal System
a21st. Century Perspective

Tensegrity structures are:•Light weight
•Much stronger than experts had predicted•Multi / Omni - directional
•Whole system adapts to stressors•Protects the “weakest link” / the A.G.R.
• defy gravity•Non-metallic materials, organized in a
Tensegrity arrangement, can conduct electricity
• ‘wired’: keep eyes level, evenly distributeweight among all 4 quadrants.•Conduct vibratory information
•Would it not make sense to identify, the A.G.R.
( area of greatest restriction - hindrance )
in thisflexible & adaptive system ?

MESOKINETIC SYSTEMMeso ( mesoderm ): gives rise to
•Connective tissues & fascia•Cartilage
•Bone•Striated and smooth muscle
•Myocardium and pericardium•Blood and lymph vessels
•Kidneys and ureters•Adrenal cortex
•Gonads•Tubes, uterus and upper vagina
•Serous membranes lining the body cavities ( T, A & P )•GI fascial support system
•Spleen
Kinetic:Related to movement of physical objects
NOTE:S/D might impact both musculo-skeletal & visceral structures.
Netter’s Atlas of Human Embryology 16

MESOKINETIC SYSTEMMeso ( mesoderm ): gives rise to
•Connective tissues & fascia•Cartilage
•Bone•Striated and smooth muscle
•Myocardium and pericardium•Blood and lymph vessels
•Kidneys and ureters•Adrenal cortex
•Gonads•Tubes, uterus and upper vagina
•Serous membranes lining the body cavities ( T, A & P )•GI fascial support system
•Spleen
Kinetic:Related to movement of physical objects
NOTE:S/D might impact both mysculo-skeletal & visceral structures.
Netter’s Atlas of Human Embryology 16

Passing on the TraditionAlan Becker, DO, FAAO 2010Journal of AAO – fall edition
•“Dr. Still was keen on being very specific.•He looked at the patient as a Totality.
•He looked for the Elusive Key Lesion – Hindrance ( somatic dysfunction )
that people have quoted for years”.
•That is what He looked for and
when He found it, He fixed it and then left it alone.He said that once done,
the body will do its own work because it is designed to do its own work.
•Our job is to find the Key Restriction – Hindranceto
homeostatic integrity,and once restored to normalcy,
to rest assured that the body will take care of the rest of the work”.

LBP patientA.G.R.
( Key somatic dysfunction )
( Stiles: 100 patients )• T/RC = 60%
• Lumbar = 24%• L.E. = 11%Total: 95%
Note:Sacrum
andinnominates were not the #1 A.G.R. !
may have been treated later in the
treatment sequence
L.B.P.
Other possible A.G.R.s•Cranial: dural tube
•U.E.•L.E.
•Note: ever see a LBP research strategy which considered S/D
in T/RC, UE, LE or cranial ?

In light of this complexity,how do you clinically view your patients ?
Stiles’ Current Perspectivecomplex, dynamic,
inter-connected & inter-woven,multiple, simultaneously functioning systems,
non-linear,autopoietic
functional unit

OPP treatment basic principles: 2 technique components
Positioning of S/D: re Restrictive Barrier• Direct:
• HV/LA: Kimberly,” should be painless and noiseless”( avoid trap of a hypermobile “pop” )
• Muscle Energy• Myofascial
• Indirect:• Strain-Counterstrain ( S/CS )• Balanced Ligamentous Tension ( BLT )• Facilitated Positional Release ( FPR )• Still Techniques ( ST )• Functional / Laughlin ( FRT/L )
Corrective Force:• Clinician introduced force: a thrust / an impulse• Patient introduced force: patient specific muscle effort• Intrinsic forces: self-healing forces of body

Tell me aboutFred L. Mitchell, Sr, DO, FAAO
• Mechanical Engineer• Creative Thinker
• Non-linear Thinker• Tensegrity “thinker”• utilized Cybernetics
• Complex Adaptive Systems Thinker• Phenomenologist
•These attributes enabled Fred to develop:• the unique Mitchell Pelvic Axis Model
• plus a totally new OMT approach utilizing a
patient generated corrective force.• stressed the importance of starting your treatment
at the Key S/D of the total system.
4 Tutorial participants: Greenman, Stiles, Sutton, & Ward are Legends being honored during 2018 Convocation.
Picture = 1,000 words
MSU-COM1972

Leon Chaitow, DO
Comments about various techniques in light of data presentedduring the 4th Fascia Congress: ( Sept. 2015 )
Muscle Energy Techniques• “It is not a Post Isometric Relaxation technique ( PIR ) ! ”
• M.E.T. introduce movement which then decreases the pain.• Leon felt my hypothesis that introduced movement
stimulates the joint mechano-receptors and that
inhibits the nociceptors was an appropriate expanded explanation of his statement.
( Wyke 1980’s research . . . 10+ yrs. after 1st M.E.T. Tutorial ) 48

MUSCLE ENERGY TECHNIQUES( MUSCLE ACTIVATION )
SUMMARY
8 ESSENTIALS: also explains why it doesn't work
• ACCURATE DIAGNOSIS• A.G.R. / SEQUENCING . . . Crucial for FLM,Sr.• SEGMENTAL DIAGNOSIS . . . Specific OMT
• ACCURATE POSITIONING• “FEATHER EDGE” OF RESTRICTIVE BARRIER . . . crucial• DIRECT – BALANCED LIGAMENTOUS TENSION
• UNYIELDING COUNTER-FORCE . . . Crucial( FUNCTIONALLY REVERSES THE ORIGIN AND INSERTION )
• APPROPRIATE MUSCLE EFFORT• DIRECTION: multiple options ( Findley )• AMOUNT: least amount that produces beneficial change• DURATION . . . Cybernetic loop key
• COMPLETE RELAXATION @ Rx SITE BUT DON’T GIVE UP WHAT GAINED
• REPEAT ABOVE STEPS . . . remaining R. barrier, not new ! , # efforts ?• RE-TEST . . . Taking money under false pretenses ?, confirms Dx / Rx
21
A.A.O.M.E.T. - 3 VISIONS
M.E.T. – 3 MASTERSFRED, ED & PHIL SHOW
2005

Functional: Laughlin-Still basics
• establish a S/D diagnosis( works best if start at A.G.R.-H / Key “lesion” )
• start technique at Positional Diagnosis position( take “doodad where it wants to go” )
( “position of ease” )( use translation & have at apex of F/E, SB & R curves )• “fine-tune” dysfunctional joint so maximally relaxed
( “fiddle and diddle” to “fine-tune positioning at D.B.P.” )( Dynamic Balance Point )
Biodynamics language: at “loose-packed” position• add vectored compression
( from side towards which dysfunction will initially rotate )• allow to “unwind”
( initially away from restricted barrier, hits a ‘still point’ & then spontaneously moves into the previously restricted compartment )
• recheck: know made a positive change !2

POSITIONING:FUNCTIONAL TECHNIQUES
• SINCE AN INDIRECT TECHNIQUE• POSITION AT D.B.P.
WHICH IS IN THE ‘POSITIONAL DIAGNOSIS QUADRANT ‘
( NOT AT JOINT NEUTRAL BUT AT JOINT ‘S/D-H’ NEUTRAL )
• EX: DIAGNOSIS L3 FRSL• THE D.B.P.
WILL BE IN THE FRSL QUADRANT
A E P AEP
NDBPFLEXION EXTENSION
R.B.
FUNCTIONAL TECHNIQUES: ALL START AT THE ‘SAME’ POINT / DIFF. NAMES
• IF MONITOR THE DYSFUNCTIONAL FACET & TISSUE CHANGES ( FRT/L-Stiles )[ MECHANORECEPTOR / NOCICEPTOR ROLE WITH PASSIVE ‘UNWINDING’ ]
• IF MONITOR LIGAMENTOUS TENSION ( BLT – WALES, LIPPINCOTT, BECKER & SUTHERLAND )• IF MONITOR A JONES TENDER POINT ( S/CS – JONES )
• IF MONITOR SUPERFICIAL OR DEEP MUSCLES ( FPR – SHIOWITZ )• IF MONITOR 3 SEGMENTS ( FUNCTIONAL METHODS – JOHNSTON )
• IF ACTIVELY BRING THROUGH RESTRICTIVE BARRIER ( STILL – VAN BUSKIRK )( MISINTERPRETED A.T. STILL / SHOULDER VIDEO ? ) 23

“The
scientific method of phenomenology ( Goethean Scientific Method )is used to create a synthesis
between modern orthodox embryology
and a holistic view of the human being.
The human embryo reveals who we are and what we are meant to be.
Practitioners have found that comprehending embryological forces
supports a holistic and biodynamic approach to healthcare because the same forces that formed the body are
continuously at work throughout life,
carrying the blueprint of health into manifestation.”Jaap van der Waal, MD, PhD
The Embryo in UsMay 19-22 2016
A.T. Still: find S/D hindrances, effectively treat the S/D hindrances and enable the “blueprint of health” to emerge / to manifest.Forces we are tapping into by removing S/D hindrances.

Note:I am not saying
AGR / sequencing is the only way
to approach patients !
but
our data suggests
it is an effective clinical strategy
Stiles’ Data: methods• Spinoscope / Gracovetsky
• sEMG evaluation• Ground Reactive Force
• Fractal Analysis• Reactive Fractal Analysis
• golfers• Elite female runners
• Dynamic Athletic Research Institute( DARI ) Jason Hunt, DO - orthopod
Sequenced OMT

Median of 60 gait cycles( tons of data )
• Statistical & fractal significant changes• Immediate changes with sequenced OMT,
not with models, chasing pain or exercise.• Each patient their own research project
Ground Reactive Force data:See similar changes 80% of time with new patients
Not saying AGR / sequencing right way
and other strategies are wrong,just saying we have a lot of data to
support the AGR / sequencing strategy
utilizing several data collection strategies

Spinal Mechanicsan
Osteopathic Perspective

SpinalMechanics
Bottomline
Type I Mechanics:•Bodies in control•Involves multiple vertebra•SB / R occur in
opposite directions•Rotation is toward
produced convexity•Compensate for Type II, pelvic
or rib cage dysfunctions
Type II Mechanics:•Facets in control•Involves 2 vertebra•SB / R occur in the
same direction•R toward produced concavity•Associated with segmental
facilitation
Act likea
pile of
blocks
act like flexible
ruler

Key to establishing an
accurate diagnosis and
quality localizationof your treatment forces
TRANSLATION •Moving a segment along a line
( introduces forces from both above and below )
•Have the segment being diagnosed ! ! !
and
treated ! ! !“floating” at the apex of the curve . . . integrates
( using Law III of Fryette’s Principles to your advantage )
•Minimal dysfunctions can be missed when use just flexion, extension, SBR, SBL or RR, RL
( forces introduced from only above . . . segment not at apex ) 29
XX

Spinal Mechanics: Type II palpate over facets
Flexion
Extension
X
X
ERSL( can’tgo intoFlexionon left )
FRSL( Can’t go into Extensionon right )
Note: both are SBL and RLNeed to use both flexion & extension
to establish an accurate diagnosis

Long mobilizers / restrictors
Short mobilizers / restrictors
DIAGNOSIS:ERSL
Rx – M.E.T.
UnyieldingCounter Force
Treatment procedure:•Position FRSR against “feather edge” of R. Barrier ( D-BLT )
•Do this using translation in 3 planes•Dysfunctional facet pair within normal range of motion
•“fiddle and diddle” to fine tune to dysfunctional facet pair ( left )•Patient makes a gentle isometric SBL and / or RL, or both muscle effort against
a gentle unyielding counter force !•2 effects occur
• Inhibits short restrictors ( Golgi receptor / protective role activated ): inhibited, not stretched !• Long mobilizers restore some of the lost movement ( micro-isotonic response )
• Facet mechano-receptors stimulated and inhibit the pain receptors ( Wyke )•Hold until “cybernetic feedback loop” displays movement, L. facets pair opens
•Have patient relax the treated area•Reposition against the remaining / not new R. Barrier: “take up the slack”
•Repeat 2-3 times• not Post Isometric Relaxation technique

Long mobilizers / restrictors
Short mobilizers / restrictors( “timing gear” problem )
DIAGNOSIS:FRSL
Rx - M.E.T.
UnyieldingCounter Force
Treatment procedure:•Position ERSR against “feather edge” of R. Barrier ( D-BLT )
•Do this using translation in 3 planes•Dysfunctional facet pair within normal range of motion
•“fiddle and diddle” to fine tune to dysfunctional facet pair ( right )•Patient makes a gentle isometric SBL and / or RL, or both muscle effort against
a gentle unyielding counter force !•2 effects occur
• Using the left long mobilizers activates the law of reciprocal innervation, inhibits contralateral short restrictors . . . Doesn’t stretch short restrictors, inhibits them. • Then long mobilizers restore some of the lost movement ( micro-isotonic response )• As closes, stimulates mechano-receptors which then inhibit pain receptors. ( Wyke )
•Hold until “cybernetic feedback loop” displays movement . . . SBR &RR closes R. facet pair•Have patient relax the treated area
•Reposition against the remaining / not new R. Barrier: “take up the slack”•Repeat 2-3 times
• not Post Isometric Relaxation technique
X
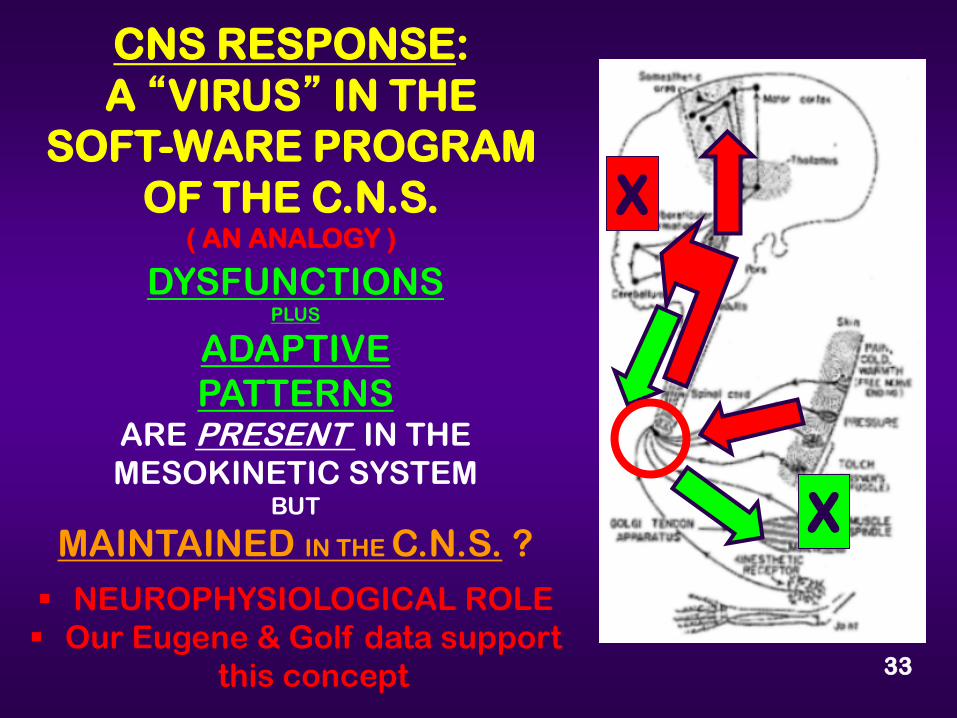
CNS RESPONSE: A “VIRUS” IN THE
SOFT-WARE PROGRAM OF THE C.N.S.
( AN ANALOGY )
DYSFUNCTIONS PLUS
ADAPTIVEPATTERNS
ARE PRESENT IN THE MESOKINETIC SYSTEM
BUT
MAINTAINED IN THE C.N.S. ?
NEUROPHYSIOLOGICAL ROLE Our Eugene & Golf data support
this concept 33
X
X

OKC 1994Bob Foreman, PhD
Ch: Physiology OUMed
AFTER 2008: Engineering Biomechanics of Human Motion
Robert L. Williams, PhD Ohio [email protected]
“virusin
software”analogy
• S/D-H pattern maintained in cerebellum ?
• Cerebellum enables total body adaptations
to occur to:• Keep eyes level
• Evenly distribute weight in all 4 quadrants
• Why finding KEY is important !• Treating Pr. or Sec. S/D ?

T7 ERSL : Functional
Position: instruct patient to•Sit up and push stomach forward
•You then translate T7/8 area to right•These 2 movements “close” the
left facet pair( taking “doodad where wants to go” )
( “fiddle & diddle” to fine tune & add rotation )•Add vectored compression toward
dysfunctional facet pair•Allow to “unwind” in both directions
• maintain compression during whole treatment• ends up at FRSR, may be neutral.
•Recheck: realize self healing potential
6Palpatewhere ?

T7 FRSL Functional
Positioning: instruct patient to•Slump forward / apex of F/E curve
•You then add translation T7/8 to right so at apex of both flexion & SBL curves.
•These 2 movements “open” the right facet pair
( taking “doodad where it wants to go “ )( “fiddle & diddle” to fine tune & add R )
•Add vectored compression toward dysfunctional facet pair
•Allow to “unwind” in both directions•Maintain compression throughout treatment• usually ends up at ERSR, or may be neutral.
7
Palpatewhere ?

LUMBAR DYSFUNCTION: L3 FRSL Functional
POSITION:L3 FRSL
USING TRANSLATION‘FLOAT’ R. FACET PAIR
LOAD OR BEAR WEIGHT
ON
L. I/T
FASCIAL LOAD
TOWARD R. FACET PAIR
37
AS SLOWLY ADD
COMPRESSIONTOWARD
RIGHTFACET PAIR,
THE BODY WILL AUTOMATICALLY
• ROTATE LEFT• HIT A “STILL POINT”
• THEN SPONTANEOUSLY
ROTATESTO RIGHT TOWARD
“RESOLVED”RESTRICTED
BARRIER
ESSENTIALS:• ANT. LUMBAR IS‘LOOKING’ LEFT( SIDE LOAD I.T. )
• RIGHT FACET PR. ISDYSFUNCTIONAL
( SIDE FLOAT )

CervicalRegion
During extension: using fingertip translation, facets should close.If facets don’t close, test both sides for resistance using diagonal translation.
During flexion: using lateral translation, facets should open,test both sides for resistance
Treatment: either • direct ( MET or HV/LA)• indirect: at “position of ease”

FUNCTIONAL TECHNIQUEScervical area
SCREENING EXAMINATION PATIENT IS SEATEDOPERATOR STANDS NEXT TO THE PATIENT
WITH ONE HAND ON THE PATIENT’S HEAD THE OTHER HAND PALPATES ALONG THE
ARTICULAR COLUMN UTILIZING THE DISTAL PAD THE THUMB ( OVER THE FACETS )
• THUMB SLIDES CEPHLAD OVER ARTICULAR COLUMN • AS THE NECK IS ROTATED . . . USE COMPRESSION
• LOOK FOR ‘SPEED-BUMPS’
• PASSIVELY Dx . . . FINDING D.B.P. / POSITION OF EASE 39

FUNCTIONAL TECHNIQUESlower cervical area
40
DIAGNOSIS: FRSR• PATIENT IS SITTING• PASSIVELY POSITION THE
DYSFUNCTIONAL VERTEBRA @ DBP OF FRSR THEN “FIDDLE & DIDDLE” TO “FINE-TUNE”
• ADD GENTLE CAUDAD COMPRESSION TOWARD SEGMENT ( DYSFUNCTIONAL FACET PAIR )
• ALLOW IT TO “UNWIND” TO THE RIGHT, HITS A “STILL POINT” AND THEN SPONTANEOUSLY ROTATES & SIDEBENDS LEFT AND EXTENDS
NOTE: VAN BUSKIRK DOES ACTIVELY & STOOD IN FRONT OF PATIENT
• RETEST . . . TO SEE IF CORRECTED !
FEW MEDICAL RESPONSES OCCUR THIS QUICKLY

Rib Cage Mechanicsan
Osteopathic Perspective

Rib Cage Mechanics Pump-Handle
Bucket-Handle
ClinicalApplication:
“pseudo-angina
WatervilleData
Impact( Medicare codes)
Exhaled Inhaled

MUSCLES: CLINICAL USE( EXPIRED DYSFUNCTIONS )
43
TREATMENTPRINCIPLES:
EXHALEDvs EXPIRED
ALTERNATIVEMETHOD
STABILIZESSCAPULA
X
X
X

MUSCLES: CLINICAL USE( INSPIRED DYSFUNCTIONS )
LOWER RIBS: BUCKET-HANDLEWANT TO USE SIDE-BENDINGTHEN STRETCH OUT FASCIA
UPPER RIBS: PUMP-HANDLEWANT TO USE FLEXION
POSTERIOR M.E.T. EFFORT AT END( GLIDES POSTERIOR END CEPHLAD )
44
Stiles’Pelvic model:an evolving model

PELVIC REGIONAN EVOLVING PERSPECTIVE
1960’s VIEW 1970 MITCHELL
80-90’s2013

TENSEGRITY & FRACTAL GEOMETRY:
• SI/J UNIQUE SIDE TO SIDE• FRACTAL / ROUGH & NON-LINEAR
PROVIDES A PROTECTIVE DESIGN !• WHY DENSE POST. S/I LIGAMENTS ?
( HOLDING TWO SURFACES APART ? )ENABLE COMPLEX SACRAL MOVEMENT ?
• ‘FLOATING COMPRESSION’ PLUS 6 FUNCTIONAL AXES . . . QUANTUM #
( INTERSECTING ITA AND OA’s )NOTE: STA IS ANTERIOR TO ITA . . . ROLE ?
• IF TENSEGRITY IS FUNCTIONINGDO WE NEED FORM / FORCE CLOSURE ?
IS THAT A BACKUP SYSTEM ?
HAS SIGNIFICANCE OF ROUGHNESS BEENMISINTERPRETED ?
( OCCURS DURING 2d & 3d DECADES )MITCHELL-
TENSEGRITY DESIGNENABLE COMPLEX
MOVEMENT PATTERNS AND PREVENT
‘WEAR & TEAR ? 47

“FLOATING COMPRESSION”DESCRIBES A
CLOSED STRUCTURAL SYSTEMCOMPOSED OF A SET OF
THREE OR MORE ELONGATED
COMPRESSION STRUTS WITHIN A
NETWORK OF TENSION TISSUES, THE COMBINED PARTS ARE MUTUALLY SUPPORTIVE
IN SUCH A WAY THAT THE STRUTS DO NOT TOUCH EACH OTHER,
BUT PRESS OUTWARD AGAINST NODAL POINTS IN THE TENSION NETWORK
TO FORM A FIRM, TRIANGULATED, PRESTRESSED
TENSION AND COMPRESSION UNIT
BEFORE AFTER

PALPATING THE SACRAL BASE ( 1970 TUTORIAL )
•Locate the P.S.I.S.•Glide thumbs medial & anterior to sacrum ( sulcus )
•Then glide thumbs superior to sacral base•I.L.A.: palpate sacral hiatus
Palpate inferior lateral to I.L.A. 49

Biomechanical Complexity: anatomical( Mitchell, Sr. always stressed this principle for every anatomical area )
Key: modify technique to patient uniqueness ! ! !( mastery rather than competency )
adduction-abduction
int. / ext. rotationKey to “fine-tuning”

L. SACRAL FLEXION: Rx MET PATIENT IS PRONE Greenman: technique description ( ABD 150 & I/R )
ABD /ADDUCT THE L.. LEG TO “LOOSE-PACK” THE LEFT S/I JOINT ( ALSO INT./EXT. ROTATE LEG )
LOCATE THE MTA OPERATOR DETERMINES THE MOST
EFFICIENT VECTOR DIRECTION WITH THEIR R. HAND ON LEFT ILA
USE RESPIRATORY ASSIST:INSPIRATION
RE-TEST MISTAKES: NOT REALIZING ABOVE
TASKS / ASSUME ALL SI/Js ARE THE SAME . . . SKILLS DEVELOP RAPIDLYWITH THIS APPROACH ! MONITOR
VECTOR
51
TEXT: GREENMAN 2d & 4th EDITIONS• ABD / ADDUCT TO APPROX. 150
• INT. ROTATE THIGH TO “OPEN S/IJ”• BUT . . . .

MTA ( LOCATE WITH A/P TRANSLATION )
LEFT SACRAL FLEXION
( functional )
“FLOAT”LEFT S/IJ( AS SIDEBEND TO RIGHT ) LOAD OR BEAR WEIGHT ON R. I/T
( BY SIDEBENDING TRUNK TO RIGHT ) THE I/T SACRUM ‘LOOKING AT’
FASCIAL LOAD ( SLOWLY ADD COMPRESSION
TOWARD
DYSFUNCTIONAL JOINT )
52
FOOD FOR THOUGHT:• “LOADED” RIGHT I/T, “LOOSE PACKED” LEFT S/IJ & FIND MTA• THIS LOCATES THE DBP FOR THE DYSFUNCTIONAL S/IJ• ADDED COMPRESSION TO “ACTIVATE” TENSEGRITY • IT WILL “UNWIND” AWAY FROM RESTRICTIVE BARRIER• AFTER THE STILL POINT, THE BODY AUTOMATICALLY
• GOES TOWARD THE PREVIOUS RESTRICTED BARRIER• FINDS THE “NEW DBP” & AXIS AUTOMATICALLY ! ! !
• ILLUSTRATE THE RAPID AND DYNAMIC “PLASTICITY” OF THE CNS ? BUOYANCY AND RESILIENCY POTENTIAL !
RL
P/N
I/P
A/D+

RIGHT ANTERIOR INNOMINATE: Rx MET PATIENT IS SUPINE
OPERATOR FLEXES R. HIP UNTIL THE ITA IS LOCATED
THE R. S/I JOINT IS THEN “LOOSE-PACKED” UTILIZING ABD/ ADDUCTION
AND I/R & E/R TO “FLOAT” AGAINST RESTRICTIVE BARRIER . . . Only prime movers activate
PATIENT ATTEMPTS TO EXTEND THE HIP vs YOUR COUNTER-FORCE
MISTAKES: NOT REALIZE ABOVE TASKS….. SYNERGISTS AND ANTAGONISTS ACTIVATED WITH MET EFFORT …. NOT CLEAN M.E.T. RESPONSE
ALTERNATIVES: LATERAL AND PRONE 53

LOCATEITA
RIGHT ANTERIOR INNOMINATE: Functional
“FLOAT”RIGHT S/IJ
( WHERE PALPATE )LOAD OR BEAR
WEIGHTON L. I/T
FASCIAL LOAD
54
RN
LEVEL
LEVEL
ESSENTIALS:• ANT. PELVIS IS ‘LOOKING’ LEFT
( SIDE LOAD )• RIGHT I/SJ IS DYSFUNCTIONAL
( SIDE FLOAT )
S +

L. SACRAL FLEXION
R. SACRAL EXTENSION
L/L SACRAL TORSION
L/R SACRAL TORSION
ANTERIORSACRAL BASE
LEFT LEFT RIGHT RIGHT
SULCUS LEFT DEEP RIGHT NORMAL
LEFT NORMAL RIGHT SHALLOW
RIGHT DEEP LEFT NORMAL
RIGHT NORMALLEFT SHALLOW
SITTING F.B.T. LEFT RIGHT RIGHT LEFT
L5 ROTATION RL RL RR RR
LORDOSIS SL. INCREASED
SL.DECREASED
SL. INCREASED
DECREASED FLAT
POST / INF. I.L.A.
LEFT LEFT LEFT LEFT
AXIS INVOLVED M.T.A. M.T.A. L.O.A. R.O.A.
SPHINX TEST NEGATIVE POSITIVE NEGATIVE POSITIVE
L. LEG LENGTH( MECHANICS )
L. LONG L. LONGR. SHORT
L. SHORTR. LONG
L. SHORT
SACRAL FINDINGS:

Clinical Application:Host + Disease = Illness ( clinical presentation )
• host + DISEASE = Illness • HOST + disease = Illness• HOST + DISEASE = Illness
Additional mechanisms:for explaining OMT outcomes
Cybernetics ( dynamic “feedback loops” )
Gen. Adaptive systems ( 1 system )
Complex systems ( multiple systems )
Fractal Geometry ( distribution issues )
Fractal / Chaos Physiology ( homeo-dynamics )
Autopoiesis ( dynamic S/F changes )
Multi-agent ModelingNetwork of NetworksEmergent Properties
7 Competencies:( P/P “ mirror” strategy )
• Osteopathic integration• Medical Knowledge
• Patient Care• Interpersonal Communications
• Professionalism• Practice-Based Care• System-Based Care
S/D can impact: 1, all, any comboof arms

THE “NEW” CONCEPTS AND LANGUAGE AVAILABLE TO OSTEOPATHY• CYBERNETICS: BILL JOHNSTON AND CHARLES BOWLES – FUNCTIONAL METHODS• AUTOPOESIS: COMPLEX & DYNAMIC STRUCTURE - FUNCTIONAL RELATIONSHIPS
( TERM NOW IN LITERATURE )
• 21 CENTURY MECHANISMS AVAILABLE TO EXPLAIN O.P.P. OUTCOMESBODY IS A COMPLEX FUNCTIONAL UNIT OF INTERCONNECTED SYSTEMS
Complexity & Family Practice:Systems & Complex Thinking
Annals of Family MedicineVol 12 no 1 Jan / Feb 2014

A.C.G.M.E. Educational Model
Experiential Educational Model( utilizing a patho-physiological “mirror” strategy )
• Action / Experience / cc. / symptom / sign
• Reflection / gather data / develop hypothesis
• Abstraction treat / test hypothesis / develop theory( establish a final diagnosis )
• Application / old, new or other
BOTTOM – LINEEducational Phenomenology

OsteopathicManagement
Whatis that
allabout ?
I have abetter
understandingnow !