Embed Size (px)
Citation preview

Semipermanentand PermanentInjectable Fillers
Derek H. Jones, MDKEYWORDS� Semipermanent and permanent fillers� Hyaluronic acid � Calcium hyaluronic polylactic acid� Polymethyl methacrylate
om
Soft-tissue augmentation dates back more than100 years ago, when autologous fat grafts wereused to restore facial volume defects.1 Paraffinwas used for some time but fell out of favorbecause of a high incidence of foreign-body reac-tions. In the early 1950s, liquid silicone was first in-jected for soft-tissue augmentation. It was usedwidely until 1982, when the US Food and DrugAdministration (FDA) temporarily banned its useover concerns of possible toxicity. Following theban on liquid silicone, injectable bovine collagenbecame available in the United States in the1980s and quickly became the gold standard oftreatment to which many new dermal fillers are stillcompared. Although some may question the dura-tion of effect of collagen, human collagen remainsan agent of comparison in many pivotal trials.
Today, an impressive array of injectable dermalfillers for facial soft-tissue augmentation is avail-able in the United States. These agents, most ofwhich were introduced in the last half decade,represent a variety of semipermanent and perma-nent fillers across several categories. Physicianscan choose between semipermanent fillers, suchas hyaluronic acid derivatives (HA), calciumhydroxylapatite (CaHA), and poly-L-lactic acid(PLA), and longer-lasting, so-called ‘‘permanentfillers,’’ such as polymethyl methacrylate micro-spheres (PMMA), highly purified forms of liquid sili-cone, and hydrogel polymers.
While these fillers are generally safe, effective-ness is related to areas of injection and physicianexpertise. Each has its own specific propertiesand longevity that makes it more suitable for certainuses than for others. Semipermanent fillers must be
Skin Care and Laser Physicians of Beverly Hills, 9201 W. SunE-mail address: [email protected]
Dermatol Clin 27 (2009) 433–444doi:10.1016/j.det.2009.08.0030733-8635/09/$ – see front matter ª 2009 Elsevier Inc. All
c
repeated at regular intervals, although with certainproducts the filler is replaced by the patients’ owncollagen over the course of several treatments.Permanent fillers require minimal touch-ups andhave long-lasting effects of 5 years and longer.
SEMIPERMANENT FILLERSCalcium Hydroxylapatite
CaHA is a normal component of human bone andteeth andhasbeenusedas implantor coatingmate-rial in dentistry and other therapeutic areas for morethan 20 years. The filler iscomposed of CaHA micro-spheres (25–45 microns) suspended in an aqueouscarboxymethylcellulose gel carrier. Radiesse (Bio-Form Medical, San Mateo, California) is the dermalfiller containing CaHA. Skin testing is not required.
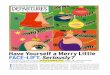
Mechanism of actionThe mechanical filling and volume enhancementoccurs following injection, when the gel carrier andCaHA microspheres displace surrounding softtissue.As thegel isphagocytized, theprocessofneo-collagenesis begins in and around the microspheres,stimulating the gradual growth of the patients’ owncollagen (Fig. 1).2 The spherical CaHA particles aregradually broken down and degraded by way ofnormal metabolic processes and eliminated ascalcium and phosphate ions through the urinarysystem. The proliferation of collagen along with theslow breakdown of the CaHA is understood toaccount for the prolonged effects.3
IndicationsCaHA is indicated for subdermal implantation forthe correction of moderate to severe facial wrinkles
set Boulevard, Suite 602, Los Angeles, CA 90069, USA
rights reserved. derm
.thec
lini
cs.

Fig.1. (A–D) Histology studies demonstrate increased collagen deposition around CaHA microspheres over 4 to 78weeks. Collagen fibers are represented by the darker areas. (From Coleman KM, Voights R, DeVore DP, et al. Neo-collagenesis after injection of calcium hydroxylapatite composition in a canine model. Dermatol Surg2008;34:S53–5; with permission.)
Jones434
and folds, including nasolabial folds (Fig. 2), and forthe correction of HIV-associated facial lipoatrophy(Fig. 3). It is also indicated for vocal cord insuffi-ciency, oral/maxillofacial defects, and radiographictissue marking. Off-label facial uses also includecorrection of marionette lines and oral commis-sures, prejowl sulcus, cheek-volume loss, anddorsal nasal deformities. In its present formulation,CaHA is not appropriate for use in the lips.
Fig. 2. (A, B) Pretreatment and posttreatment photographvolume injected into nasolabial folds was 1.3 mL. (Courte
Efficacy and safetyCaHA was compared with a human-collagenproduct in a United States pivotal trial of 117subjects with moderate to severe nasolabial folds.These subjects were randomized to receive CaHAon one side of the face and an existing humancollagen (HC) product (Cosmoplast, Inamed,Santa Barbara, California) on the other. CaHAprovided significantly longer correction than HC,
s of injection with Radiesse for nasolabial folds. Totalsy of D. Jones, MD, Los Angeles, CA.)

Fig. 3. (A, B) Pretreatment and posttreatment photographs of injection with Radiesse for HIV-associated facial lip-oatrophy. (Courtesy of D. Jones, MD, Los Angeles.)
Semipermanent and Permanent Injectable Fillers 435
and the favorable adverse event profile was similarto HC.4
In this split-face study, the mean change inpretreatment score using theLemperle Rating Scaleover 6 months was 1.23 for CaHA and 0.05 for HC.Dramatic differences between CaHA and HC werealso noted in Global Aesthetic Improvement Scale(GAIS) ratings at 6 months. For CaHA, 94.6% offolds were graded improved, much improved, orvery much improved, compared with 2.7% for HC.Data for up to 3 years has been gathered and isnow in review by investigators. Early analysissuggests some residual effect in some patients forup to 36 months (Brian Pilcher, PhD, San Mateo,CA, personal communication, April 2009).
Adverse events were limited to erythema,edema, and ecchymoses. Edema and bruisingwere more common on the CaHA-treated sidesthan those treated with HC (P<.0001). Edemaand bruising lasted approximately 1 week afterany injection and the average duration forerythema was approximately 2 to 3 weeks, withno significant difference between the two mate-rials. One nongranulomatous nodule wasobserved with CaHA compared with three withHC. All adverse events resolved without sequelae.In addition to the CaHA/HC study, another studyfound longer lasting results and increased satis-faction with CaHA when compared with two hya-luronic acid products.16
In a recent study, Busso and colleagues soughtto determine whether the addition of anestheticagents, such as lidocaine, to prefilled CaHAsyringes might provide sufficient anestheticprophylaxis to reduce the need for conventionalanesthetic pretreatment procedures. The studydemonstrated that the addition of lidocaine toCaHA syringes can be added safely without harm-ful changes in the physical properties of the originalsoft-tissue filler.5 Additional studies are underwayto determine whether the addition of lidocaine
alters patients’ discomfort, durability, and efficacy.It is the author’s opinion that, as described in Bus-so’s manuscript, addition of 0.15 cc 1% lidocainewith epinephrine to the 1.5 cc syringe and mixedby way of a female to female adaptor is revolu-tionary, dramatically lessens patients’ discomfort,and is rapidly becoming the standard of care.
Clinicians have speculated whether CaHA posedany confounding radiographic properties. Car-ruthers and colleagues set out to answer this ques-tion and found that CaHA is not consistently evidenton X ray but is clearly visible on CT. However, CaHAis unlikely to be confused with usual abnormal andnormal radiographic findings. Although usuallyvisible on CT, its appearance is distinct fromsurrounding bony structures, does not obscureunderlying structures, and does not interfere withnormal analysis.6 In summary, while visible on CTand X ray, CaHA does not interfere with usual inter-pretation of the radiographs, and therefore, doesnot pose overt radiographic safety concerns.
TechniqueCaHA should be injected in small amounts ina retrograde fashion into the immediate subcuta-neous plane or epiperiosteal plane, using a linearretrograde tunneling technique. Cross- hatchedlinear threading may also be employed. Overcor-rection should be avoided. The nondominant indexfinger should be used to guide the needle and thethumb and forefinger used to mold the productand to remove any contour irregularities. CaHAshould be injected very slowly in long, linear micro-threads of approximately 0.05 mL per pass.Extreme caution should be taken when injectinginto the subdermal plane around the superior na-solabial fold, where the angular artery andbranches are present (Fig. 4). Occlusion of thisvessel can occur by way of external compressionfrom CaHA or by injection of CaHA directly intothe lumen of the vessel, creating embolic ischemia

Fig. 4. Vascular anatomy of the midface. The angularartery (a branch of the facial artery) anastomoses withthe supratrochlear and dorsal nasal arteries (branchesof the ophthalmic artery), joining the external carotidartery network with the internal carotid arterynetwork. Occlusion or embolic events involving thisnetwork can lead to extensive tissue necrosis. ST, supra-trochlear artery; D, dorsal nasal artery; A, angularartery; SF, superior labial artery; F, facial artery.
Jones436
and tissue necrosis of the nasal alar region alongthe distribution of the angular arteries or itsbranches. Reports of alar vascular necrosis havebeen reported to the author and the superior naso-labial fold should be considered a high-risk areanot only for CaHA but for all injectable fillers.
It is particularly important to use sufficientvolume of CaHA for the treatment of HIV-related lip-oatrophy. While previous studies have demon-strated different efficacy endpoints, such asphotographic documentation of global improve-ment and change in mean skin thickness usingultrasound or skin calipers, treatment often fallsshort of optimal correction in clinical practice. Ina recent study by Carruthers and Carruthers, theauthors defined optimal correction as ‘‘very muchimproved’’ on the GAIS scale, where a touch up isnot required, and sought to determine the volumenecessary to achieve optimal correction. Usinga mean cumulative volume of 13.4 mL of CaHA,subjects in the Carruthers’ study achieved the topGAIS score of ‘‘very much improved’’ in 80% ofsubjects at 3 months and 59% at 6 months,compared with 26% at 3 months and 7% at 6months in a similar study by Silvers that useda mean cumulative volume of 8.4 mL of CaHA.7,8
Poly-L-lactic Acid
PLA is a synthetic polymer that is biodegradableand resorbable. Injectable PLA (Sculptra, DermikLaboratories, Berwyn, Pennsylvania) consists ofmicroparticles of PLA in a sodium carboxymethyl-cellulose gel. The filler must be reconstituted withsterile water before administration. No skin test isrequired. PLA was approved by the FDA in 2004for the treatment of HIV-related facial lipoatrophy,although the product is used off label for limitedage-related lipoatrophy in patients who do nothave HIV.
Mechanism of actionPLA is administered into the subcutaneous plane.There, the suspension of reconstituted PLAprovides mechanical correction and filling. Imme-diate volumizing is mostly from fluid that becomesabsorbed over a few days. Over weeks to months,the PLA microparticles are gradually degraded,while treated areas undergo subtle volume expan-sion as the host tissue responds to the PLA.9 Themicroparticles of PLA become surrounded ina capsuleof connective tissue consistingof connec-tive tissue cells and inflammatory cells, such asmacrophages, lymphocytes, mast cells, and foreignbody giant cells. As time passes, there is a fibrous-tissue response with collagen deposited aroundthe foreign body reaction. This fibrous response isthought to provide sustained correction.
IndicationsPLA is indicated specifically for the correction ofHIV-related facial lipoatrophy. It is also approvedfor correction of nasolabial folds in HIV negativepatients. The filler works best for volume correc-tion, not specific depressions. PLA is also usedoff label in non–HIV-infected patients who havepanfacial stage 1 facial lipoatrophy, a conditionthat is often a consequence of aging in healthy,lean individuals. Monthly injections of one to twovials into the subcutis over many treatments (4–6is usual) often achieve restoration of subcutaneousvolume (Fig. 5). Correction of subcutaneous fat losswill often last for 12 to 24 months. After this time,patients will often seek reinjection. In the author’sexperience, PLA is often not successful in treatingmore advanced cases of HIV facial lipoatrophy.
Efficacy and safetyPLA was first approved in 2004 using a fast-trackprocess, an accelerated review procedure oftenused for HIV drugs. Efficacy and safety data forthe approval was based on data from physician-sponsored Investigational Device Exemptionstudies in the United States and the EuropeanVEGA study. The VEGA study followed 50 subjects

Fig. 5. (A) Pretreatment of age-related, non-HIV facial lipoatrophy compared with 1 month following the finaltreatment with eight vials of Sculptra injected in four treatment sessions over 3 months. (B) One month afterlast injection. (From Jones D, Vleggaar D. Technique for injecting poly-L lactic acid. J Drugs Dermatol2007;6:S13–7; with permission.)
Semipermanent and Permanent Injectable Fillers 437
treated with PLA for 96 weeks.10 Subjects withHIV-associated facial lipoatrophy received foursets of injections: Day 0, followed by every 2weeks for 6 weeks. Subjects were evaluated usingclinical examination, facial ultrasonography, andphotography. At entry, the median facial fat thick-ness was 0 mm. The median total cutaneous thick-ness increased significantly from baseline (up to7.2 mm at weeks 48 and 72). By week 96 themedian total thickness was 6.8 mm. No significantadverse events were observed. In 22 (44%)subjects, palpable but nonvisible subcutaneousnodules were observed, which tended to sponta-neously resolve with time. The study did not useratings of pre-and posttreatment photographsby experienced physicians not performing thetreatment to measure whether optimal correctionwith complete restoration of cheek contourswas achieved. Approval for aesthetic use wasgained in mid 2009 based on the results of arandomized, evaluator-blinded, parallel-group,multicenter study of 233 patients carried out inimmune competent patients. The treatment phaseconsisted of 1 to 4 visits at 3-week intervals duringwhich patients received bilateral injections(average of all injections was 2.3 vials) of Sculp-tra�Aesthetic11 (n 5 116) or collagen (n 5 117)
into the left and right nasolabial fold wrinkles.The follow-up phase consisted of visits at week 3and months 3, 6, 9, and 13 after the last treatment.Of the 116 patients treated with Sculptra�Aes-thetic, 106 patients completed the study andcontinued into the long-term surveillance phase,which extended to 25 months. Ninety-five patientscompleted the surveillance phase. Evaluation wasdone through use of the Wrinkle AssessmentScore (WAS) coding system, (0 5 no wrinkles;5 5 a very deep wrinkle or redundant fold).Improvements from baseline at 25 months provedto be consistent, progressive, and statisticallysignificant at each time point measured (P<0.001)100% of patients improved at week 3; 88.7% atmonth 13; and 86.3% at month 25.
Patients consistently reported high satisfactionwith their Sculptra�Aesthetic treatment resultswith 80% of patients satisfied with results at 25months. In physician-reported adverse eventswith Sculptra�Aesthetic: 8.6% of patients experi-enced papules and nodules up to 13 months fallingto 1–1.9% at 25 months.
An increased risk of papules and nodules in theperiorbital area has been reported in publishedliterature therefore use in the periorbital area isnot recommended. Use of Sculptra�Aesthetic is

Jones438
contraindicated in the lips, in individuals withknown hypersensitivity to any of its components,or in patients with known history of or suscepti-bility to keloid formation or hypertrophic scarring.Sculptra�Aesthetic should not be injected in areaswith active skin infection or inflammation.
In addition to the adverse events in thesestudies, persistent granulomatous reactions havebeen observed (Fig. 6).12
TechniquePLA should be injected into the subdermal plane,not into the dermis, to limit the likelihood of noduleand papule development. Red, palpable, persis-tent dermal nodules may occur with intradermalinjection. Dermal defects are better treated withan HA or collagen filler. A linear retrograde tech-nique, with a cross-hatching approach, shouldbe used with a 25-gauge, 1-in or 2-in needle.Smaller bore needles tend to become easilyclogged. Practitioners should use 1 mL tuberculinsyringes, and shake the solution well before trans-ferring to syringe and immediately before injection.
The 25-gauge needle entry site may be anesthe-tized with small, intradermal injections of 1% lido-caine with epinephrine through a 30-gauge needle,resulting in tolerable injections. Intravascular injec-tion should be avoided; the angular artery runs inthe immediate subdermal plane in the area of thesuperior nasolabial fold. Injection of the parotidduct, which overlies the buccinator muscle in thelateral cheek, should also be avoided.
It is often helpful to outline the treatment areabefore injection. The treated area must not extendabove the inferior orbital rim. To prevent contourirregularity and visible or palpable nodules in theinfraorbital area, the product must be injected
Fig. 6. (A, B) Persistent granulomatous reaction to PLA. (Froinflammatory response induced by injectable poly-L-lactic9; with permission.)
epiperiosteally in small amounts, deep to themuscle layer, using a serial puncture technique.Patients should also be made aware that theimmediate posttreatment appearance will fadewithin 2 to 4 days. This instantaneous effect iscaused by fluid from the filler, which causesedema upon injection. Optimal augmentation willbecome apparent after multiple treatments at 3-to 4-week intervals, as new collagen isregenerated.13
Although the package insert recommendsreconstitution of each vial of PLA with 3 mL ofsterile water, subcutaneous lumps also can beavoided if each vial is reconstituted with 5 mL ofsterile water, or 4 mL of sterile water and 1 mL of1% lidocaine without epinephrine, at least 24hours before injection. The reconstituted vialshould be vigorously shaken immediately beforetransfer into the syringe as settling of the productin the syringe may lead to uneven applicationand contribute to nodule formation.13 UnlikeCaHA, which generally is not massaged bypatients, those who have PLA injections shouldbe instructed to frequently massage the treatedarea in the days to weeks following the procedureto prevent the formation of uneven or lumpy fibro-plasia. Some advocate the ‘‘rule of 5s’’ wherebythe patient massages the area for 5 minutes, 5times daily, for 5 days after the injection.
PLA effect is subtle, and many treatments maybe required to reach optimal correction. Durationis generally 1 to 2 years.
Hyaluronic Acid Derivatives
Hyaluronic acid, an important natural componentof human skin, is a glycosaminoglycan
m Wildemore JK, Jones DH. Persistent granulomatousacid for HIV lipoatrophy. Dermatol Surg 2006;32:1407–

Semipermanent and Permanent Injectable Fillers 439
polysaccharide comprised of residues of themonosaccharides d-glucuronic acid and N-acetyl-d-glucosamine. HA fillers comprise themajor share of the United States market place forinjectable fillers, with Juvederm (Allergan, Irvine,California) and Restylane (Medicis, Scottsdale,Arizona) dominating the market.
Most hyaluronic acid derivatives are superior tobovine collagen 6 months after injection. Forexample, in the pivotal study comparing threeformulations of Juvederm with Zyplast, 81% to90% of nasolabial folds treated with Juvedermmaintained a clinically significant improvementfrom baseline for at least 6 months, comparedwith 36% to 45% with bovine collagen.14 Thepivotal trial for Restylane evaluated 138 subjectswho received Restylane in one nasolabial foldand Zyplast in the contralateral fold. Using theGAIS, investigators rated 62% of folds superiorwith Restylane at 6 months compared withZyplast, and 8% rated Zyplast superior toRestylane.15
Generally, hyaluronic acid-derivative–associ-ated correction has a cosmetic effect for approxi-mately twice as long as bovine collagen (ie,persistence for 4–6 months rather than 2–3months).6 However, recent studies of nonanimalHA derivatives have demonstrated long-lastingeffectiveness of up to 18 months after retreatmentwith either Juvederm or Restylane because of theapparent development of fibroplasia around theinjected product. Therefore, certain hyaluronicacids should be considered semipermanentfillers.16,17
Serious adverse events are rare. In a retrospec-tive analysis of the safety of nonanimal, stabilized
Table1Currently available dermal fillers approved by the US Foo
Temporary fillersBovine collagen Zyplast, Zyderm
Human collagen Cosmoderm, C
Porcine collagen Evolence (Colb
Hyaluronic acid Prevelle Silk (M
Semipermanent fillersCalcium hydroxylapatite Radiesse (BioF
Poly-L-lactic acid Sculptra (Derm
Hyaluronic acid Restylane, PerlIrvine, CA)
Permanent fillersLiquid silicone Silikon-1000 (A
Ophthalmics
Polymethyl methacrylate Artefill (Artes,
HA, major adverse events included hypersensi-tivity reactions, localized granulomatous reac-tions, bacterial infection, and acneiform andcystic lesions.18 One salient advantage of hyalur-onic acid is that adverse reactions or unwantedplacement of product may be quickly and safelyreversed with hyaluronidase.19 Other HA currentlyFDA-approved include Prevelle Silk (Mentor, Irv-ing, Texas), a 5.5 mg/cc HA with pre-incorporatedlidocaine. Compared with Juvederm and Resty-lane, Prevelle Silk is a less concentrated or lighterHA with less lift capacity and a shorter tissue resi-dence time. Also FDA-approved is Elevess (Anika,Woburn, Massachusetts), which is a higherconcentration 28 mg/cc HA (Table 1). Severalother HA are being investigated in clinical trials inthe United States. They include Puragen Plus(Mentor Corporation, Santa Barbara, California),which contains lidocaine integrated directly intothe formula; Belotero Soft and Belotero Basic (An-teis, Geneva, Switzerland), and Teosyal (TeoxaneLaboratories, Geneva, Switzerland).
PERMANENT FILLERSLiquid Silicone
Liquid silicone (LIS) was first used as an injectablefiller in the 1950s. Before collagen injectable fillersbecame available in the early 1980s, LIS was theinjectable filler of choice. There was no standard-ized FDA-approved product and many productsof varying purity were injected often in large bolusform, which led to frequent product migration andforeign-body reactions. Subsequently, in the early1990s, all forms of silicone for cosmetic implanta-tion were banned by the FDA because of possible
d andDrug Administration (May, 2009)
(Allergan, Irvine, CA)
osmoplast (Allergan, Irvine, CA)
ar, Herzliya Israel)
entor, Irving, TX), Elevess (Anika, Woburn, MA)
orm, San Mateo, CA)
ik, Berwyn, PA)
ane (Medicis, Scottsdale, AZ); Juvederm (Allergan,
lcon, Fort Worth, TX); Adatosil-5000 (Escalon, Skillman, NJ)
San Diego, CA)

Jones440
toxicity and systemic reactions related to LIS andsilicone breast implants.
After the FDA resolved safety issues regardingsilicone breast implants and LIS, in the late1990s, two new forms of highly purified liquid sili-cone were approved (Silikon-1000 and Adatosil-5000) for use as an intraocular implant to treatretinal detachment. While this use is the only offi-cial indication for LIS, the FDA Modernization Actof 1997 makes off-label uses legal, provided thatthe physician or drug manufacturer does notadvertise for such use. LIS is now used off labelfor soft-tissue augmentation (see indications dis-cussed later). Silikon-1000 has a lower viscosityand is the most suitable for injectable soft-tissueaugmentation, as it is easier to inject throughsmaller gauge needles.
Current opinion on liquid injectable silicone ispolarized between opponents and advocates.Opponents argue that despite use of proper tech-nique and products, serious adverse events arecommon and unpredictable. Proponents rely ona wealth of anecdotal data to argue that liquidinjectable silicone is safe and effective as long asthree rules are employed: (1) use highly purifiedFDA-approved LIS; (2) employ microdroplet serialpuncture technique (defined as 0.01 cc per injec-tion site injected into the subdermal plane); and(3) use small volumes (0.5 mL for smaller defectsand up to 2 mL for larger areas of atrophy) ateach session with multiple sessions staged atmonthly intervals or longer.
Mechanism of actionAfter LIS is injected, a capsule of new collagendevelops to encircle each microdroplet of silicone.This process continues for about 3 months, duringwhich time the collagen capsule adds volume tothe augmentation of the LIS microdroplet. Thecollagen also holds the droplets in place to preventmigration.9
IndicationsAlthough LIS is used off label for many indications,it is the author’s opinion that LIS should not beroutinely employed for the average cosmeticpatient until longer-term studies with current prod-ucts resolve some of the controversy regardinglonger-term safety and efficacy. However, for theunique and disfiguring defects associated withHIV facial lipoatrophy and serious acne scarring,LIS produces cosmetically superior and moredurable results than currently available less-permanent options (See Efficacy and safety dis-cussed later).
Efficacy and safetyLIS is an excellent choice for HIV-associated faciallipoatrophy. In one trial, highly purified 1000-cStsilicone oil was studied among 77 subjects todetermine the number of treatments, amount ofsilicone, and time required to reach completecorrection. Subjects received 2 mL of Silikon1000 at monthly intervals with the microdroplettechnique until optimal correction was achieved.The researchers elucidated two important find-ings: (1) all three of these parameters were directlyrelated to the initial severity of lipoatrophy, and (2)highly purified 1000-cSt silicon oil is a safe andeffective treatment option for HIV-associated lip-oatrophy (Fig. 7).20 Five-year data is now availableon this cohort and no serious adverse events havebeen found (D. Jones, unpublished data).
Using the microdroplet, multiple-injection tech-nique, Barnett and Barnett have had successwith injections of LIS for acne scars lasting overa 10-, 15-, and 30-year follow-up periods.21
TechniqueClinicians should inject only highly purified FDA-approved LIS, such as Silikon-1000, using the mi-crodroplet serial puncture technique (0.01 mL orless injected through a 27-gauge needle into theimmediate subdermal plane at 2 mm to 4 mmintervals). Intradermal injections should beavoided, as these may create intradermalpapules.22 However, intradermal injections maybe used for atrophic dermal acne scars, using0.001 mL microdroplets.
Very small amounts of LIS should be injected atmonthly intervals, or longer. The immediate goal isundercorrection. Optimal correction occurs slowlyas fibroplasia develops around the microdroplets,creating further tissue augmentation andanchoring each microdroplet into place.
Polymethyl Methacrylate
Injectable PMMA (ArteFill, Artes Medical, SanDiego, California) is a suspension of 20% PMMAsmooth microspheres and 80% bovine collagen.ArteFill is the product of third-generation PMMAmicrosphere technology. Previous generationsinclude Arteplast (used in Germany from 1989 to1994) and Artecoll (used worldwide, except in theUnited States and Japan, from 1994 to 2006). Ar-tefill represents a third-generation product con-taining fewer nanoparticles (less than 20microns), which were thought to be associatedwith granulomatous reactions observed withprevious generations. ArteFill was approved bythe FDA in 2006 for the correction of nasolabialfolds. However, Artes filed for Chapter 7 bank-ruptcy in December 2008, and was acquired by

Fig. 7. (A, B) Pretreatment and posttreatment liquid injectable silicone for HIV-associated facial lipoatrophy.(Courtesy of D. Jones, MD, Los Angeles, CA.)
Semipermanent and Permanent Injectable Fillers 441
Suneva (San Diego, California) which now ownsand distributes ArteFill.
Mechanism of actionAfter PMMA is injected, the collagen vehicle is ab-sorbed within 1 to 3 months. Afterward, newcollagen is deposited by the host to encapsulateand engulf the remaining estimated 6 millionPMMA particles in 1 mL of ArteFill. This processcontributes to tissue augmentation through fibro-plasia. Although collagen is absorbed, the PMMAis permanent and not reabsorbed.9
IndicationsInjectable PMMA is indicated for nasolabial folds.It is also used off label for glabellar frown lines,radial lip lines, and mouth corners.
Injectable PMMA is contraindicated for use inpatients who have a positive result to the requiredArteFill skin test; patients who have severe aller-gies (as indicated by a history of anaphylaxis ormultiple severe allergies); patients who haveknown lidocaine hypersensitivity; patients whohave a history of allergies to bovine collagen prod-ucts; and patients who have known susceptibilityto keloid or hypertrophic scarring. The productshould not be used for lip augmentation.
Efficacy and safetyThe United States pivotal clinical trial for ArteFillwas a controlled, randomized, prospective,
double-masked trial of 251 subjects at eight centersacross the United States. Subjects received eitherArteFill or bovine collagen dermal filler (control). Effi-cacywas ratedbymaskedobserversusingaphoto-graphic Facial Fold Assessment Scale. The studydemonstrated a significant improvement with Arte-Fill compared with the control group at 6 months(P<.001) in nasolabial folds. A subset of subjectswas observed at 12 months and all showed persis-tent wrinkle correction (Fig. 8).23
A subgroup of 69 subjects returned for follow-up4 to 5 years later. Investigator Facial Fold Assess-ment ratings at 4 or 5 years were improved frombaseline by 1.67 points (P<.001). Nearly allsubjects (95.5%) reported that they were at leastsomewhat satisfied and 81.8% reported thatthey were either satisfied or very satisfied.23
Five subjects reported six late, adverse eventsthat occurred from 2 to 5 years after the initialinjection. Of these, four were mild cases of lumpi-ness, and two were severe. The total number oflate, adverse events was 6 of 272 (2.2%) of wrin-kles injected.24
Granulomatous reactions (manifested by in-flamed red nodules) may be treated with intrale-sional cortisone combined with antibiotic therapy.
TechniqueInjectable PMMA is placed into the dermal-subcu-taneous junction using the tunneling or linear

Fig. 8. Results of ArteFill for the treatment of nasolabial folds at pretreatment, 1 year posttreatment, and beyond1 year posttreatment. (A) Pretreatment. (B) 1 year posttreatment. (C) Greater than 1 year posttreatment. (FromCohen SR, Holmes RE. Artecoll: a long-lasting injectable wrinkle filler material: report of a controlled, random-ized, multicenter clinical trial of 251 subjects. Plast Reconstr Surg 2004;114:964–76; with permission.)
Jones442
threading technique with a 26-gauge, 5/8-in nee-dle. Overcorrection is not recommended. It is pref-erable to inject more deeply than superficially, asthe risk of wasted material is less problematicthan superficial injection, which can cause perma-nent skin surface texture or color impairment.
Patients should be evaluated 4 to 6 weeks afterthe injection to assess the need for further treat-ments. Optimal correction usually requires two tothree treatments, and touch-up implantationsshould be at intervals of at least 2 weeks or longerdepending upon the amount of implant used, thesite of placement, and the dynamics of thecorrected sites.
Investigational Permanent Agents
Hydrogel polymersHydrogel polymers are a novel class of fillers,comprised mostly of water with a small amount ofsynthetic polymer. The so-called injectable ‘‘endo-prosthesis’’ agents include Bio-Alcamid (Polyme-kon, Milan, Italy) and Aquamid (Aquamid, Ferrosan,Copenhagen, Denmark), both of which are used inEurope but are not yet FDA approved. Thesenonbiodegradable fillers are composed of 96%water and 4% synthetic polymer (polyalkylimide, inthe case of Bio-Alcamid, and polyacrylamide forAquamid). Both agents are used for large-volumeaugmentation, such as hemifacial lipoatrophy (Rom-berg’s disease) or HIV-associated lipoatrophy.
Mechanism of actionOnce injected, the gel particles become covered bya thin collagen capsule (0.02 mm) which completely
surrounds the particles and isolates them from thehost tissues, creating an injectable prosthesis. Ac-cording to the manufacturer, Bio-Alcamid hasmuch stability, integration among living tissues,and more simple removal, if required, than otherdermal fillers. The results are considered permanent,but removal can be done through aspiration. Full effi-cacy of removal through aspiration remains unclear.
IndicationsWhile both agents are used for replacement offacial volume caused by lipoatrophy, they are alsoused for the treatment of nasolabial folds, lipaugmentation, depressed scars, and enhancementof cheekbones and jawline. They are not indicatedfor the treatment of fine wrinkles.
Efficacy and safetyRecent reports in the literature document thesuccess of Bio-Alcamid for the treatment of HIV-associated facial lipoatrophy.25,26 According tothe manufacturer, risk of infection or allergy isvery low (0.6%) and only 0.2% of patients havehad an immune response to the implant, whichcreated localized swelling that required drainageover a 1- to 6-month period.
Late-appearing streptococcal bacterialabscesses have been reported. A paper by theauthor and colleagues follows five patients whoreceived Bio-Alcamid for HIV-associated lipoatro-phy and developed late-appearing streptococcalbacterial abscesses (Fig. 9).27 In each case, anacute abscess developed several months and upto years after the initial injection of Bio-Alcamid. All

Fig. 9. Bio-Alcamid abscess preincision (A) and (B) postincision and drainage; gram stain of drained materialreveals streptococcal bacteria (C). (Adapted from Jones DH, Carruthers A, Fitzgerald R, et al. Late-appearingabscesses after injections of nonabsorbable hydrogel polymer for HIV-associated facial lipoatrophy. DermatolSurg 2007;33:S193–8; with permission.)
Semipermanent and Permanent Injectable Fillers 443
five cases responded quickly to drainage and antibi-otic therapy, although in two cases the abscessesbecame recurrent. In one case the patient alsodeveloped methicillin-resistant S. aureus andrequired extensive intravenous antibiotic therapy.
Based on the cases, it appears that local oralstreptococcal bacteria may be capable of directlyinvading implant material. It also seems possiblethat the bacteria may reach the implant througha needle puncture during a dental or surgicalprocedure, possibly warranting prophylactic anti-biotic therapy before dental and surgical proce-dures in patients who have received Bio-Alcamid.
Bio-Alcamid and other hydrogel polymers carrythe risk of foreign-body reaction, infection, migra-tion, or granuloma formation.
TechniqueThese agents are injected subcutaneously, usuallyunder local anesthesia, and massaged smooth bythe clinician. A thin layer of collagen graduallyforms around the injected gel over a period of 4
to 8 weeks when the gel becomes completely sur-rounded and isolated from host tissues, in effectmaking it an endogenous prosthesis.
SUMMARY
The use of dermal fillers has advanced significantlyfrom its beginnings with fat grafts in the early 20thcentury to the full array of semipermanent andpermanent fillers now available. Today’s fillersare suitable for many indications and each hasits own advantages and disadvantages.
Many novel dermal fillers that are already avail-able in Europe are now undergoing FDA testing,and some of these will likely be approved for usein the United States within the next few years.They include the aforementioned investigationalHA in the semipermanent class of fillers and hydro-gel polymers among the permanent fillers. Thesefillers will expand the choices available to patientsand physicians and promise to increase longevityand minimize adverse events.

Jones444
ACKNOWLEDGMENTS
The author wishes to acknowledge Mark R. Vogel,MA, and David J. Howell, PhD, RRT for their editorialassistance in the preparation of the manuscript.
REFERENCES
1. KleinA,ElsonM.Thehistoryofsubstances forsoft tissue
augmentation. Dermatol Surg 2000;26:1096–105.
2. ColemanKM,VoightsR,DeVoreDP,etal.Neocollagen-
esis after injection of calcium hydroxylapatite composi-
tion in a canine model. Dermatol Surg 2008;34:S53–5.
3. Berlin AL, Hussain M, Goldberg DJ. Calcium hydrox-
ylapatite filler for facial rejuvenation: a histologic and
immunohistochemical analysis. Dermatol Surg 2008;
34:S64–7.
4. Smith S, Busso M, McClaren M, et al. A randomized,
bilateral, prospective comparison of calcium hydrox-
ylapatite microspheres versus human-based
collagen for the correction of nasolabial folds. Der-
matol Surg 2007;33:S112–21.
5. Busso M, Voigts R. An investigation of changes in
physical properties of injectable calcium hydroxyl-
apatite in a carrier gel when mixed with lidocaine
and with lidocaine/epinephrine. Dermatol Surg
2008;34:S16–23.
6. Carruthers A, Liebeskind M, Carruthers J, et al.
Radiographic and computed tomographic studies
of calcium hydroxylapatite for treatment of HIV-asso-
ciated facial lipoatrophy and correction of nasolabial
folds. Dermatol Surg 2008;34:S78–84.
7. Carruthers A, Carruthers J. Evaluation of injectable
calcium hydroxylapatite for the treatment of facial
lipoatrophy associated with human immunodefi-
ciency virus. Dermatol Surg 2008;34:1486–99.
8. Silvers SL, Eviatar JA, Eschavez MI, et al. Prospec-
tive, open-label, 18-month trial of calcium hydro-
xylapatite (Radiesse) for facial soft-tissue
augmentation in patients with human immunodefi-
ciency virus-associated lipoatrophy: one year dura-
bility. Plast Reconstr Surg 2006;118:34S–45S.
9. Alam M, Gladstone H, Kramer E, et al. ASDS guide-
lines of care: injectable fillers. Dermatol Surg 2008;
34:S115–48.
10. Valantin MA, Aubron-Olivier C, Ghosn J, et al.
Polylactic acid implants (New-Fill) to correct facial
lipoatrophy in HIV-infected patients: results of the
open-label study VEGA. AIDS 2003;17:2471–7.
11. Sculptra�Aesthetic Product Information. Dermik
Laboratories; 2009.
12. Wildemore JK, Jones DH. Persistent granulomatous
inflammatory response induced by injectable poly-
L-lactic acid for HIV lipoatrophy. Dermatol Surg
2006;32:1407–9.
13. Jones D, Vleggaar D. Technique for injecting poly-L-
lactic acid. J Drugs Dermatol 2007;6:S13–7.
14. Baumann LS, Shamban AT, Lupo MP, et al. Compar-
ison of smooth-gel hyaluronic acid dermal fillers with
cross-linked bovine collagen: a multicenter, double-
masked randomized, within-subject study. Dermatol
Surg 2007;33:S128–35.
15. Narins RS, Brandt F, Leyden J, et al. A randomized,
double-blind, multicenter comparison of the efficacy
and tolerability of Restylane versus Zyplast for the
correction of nasolabial folds. Dermatol Surg 2003;
29:588.
16. Narins RS, Davan SH, Brandt FS, et al. Persistence
and improvement of nasolabial fold correction with
nonanimal-stabilized hyaluronic acid 100,000 gel
particles/mL filler on two treatment schedules:
results up to 18 months on two retreatment sched-
ules. Dermatol Surg 2008;34:S2–8.
17. Smith S, Jones D. Efficacy and safety following
repeat treatment for a new family of hyaluronic
acid based fillers. In: Programs and abstracts of
the 64th American Academy of Dermatology Annual
Meeting. San Diego (CA), July 26–30, 2006.
18. Lupton JR, Alster TS. Cutaneous hypersensitivity
reaction to injectable hyaluronic acid gel. Dermatol
Surg 2001;26:135–7.
19. Brody HJ. Use of hyaluronidase in the treatment of
granulomatous hyaluronic acid reactions or
unwanted hyaluronic acid misplacement. Dermatol
Surg 2005;31(8 Pt 1):893–7.
20. Jones D, Carruthers A, Orentreich D, et al. Highly Puri-
fied 1000-cSTsilicon oil for treatment of human immu-
nodeficiency virus-associated facial lipoatrophy: an
open pilot trial. Dermatol Surg 2004;30:1279–86.
21. Barnett JG, Barnett GR. Treatment of acne scars
with liquid silicone injections: 30-year perspective.
Dermatol Surg 2005;31:1542–9.
22. Jones D. HIV facial lipoatrophy: causes and treat-
ment options. Dermatol Surg 2005;31:1519–29.
23. Cohen SR, Holmes RE. Artecoll: a long-lasting inject-
able wrinkle filler material: report of a controlled,
randomized, multicenter clinical trial of 251 subjects.
Plast Reconstr Surg 2004;114:964–76.
24. Cohen SR, Berner CF, Busso M, et al. Artefill: a long-
lasting injectable wrinkle filler material—summary of
the U.S. Food and Drug Administration trials and
a progress report on 4- to 5-year outcomes. Plast
Reconstr Surg 2006;118(35):64S–76S.
25. Protopapa C, Giuseppe S, Caporale D, et al. Bio-
Alcamid in drug-induced lipodystrophy. J Cosmet
Laser Ther 2003;5:226–30.
26. Treacy P, Goldberg D. Use of a biopolymer polyalky-
limide filler for facial lipodystrophy in HIV-positive
patients undergoing treatment with antiretroviral
drugs. J Dermatol Surg 2006;32:804–8.
27. Jones DH, Carruthers A, Fitzgerald R, et al. Late-
appearing abscesses after injections of nonabsorb-
able hydrogel polymer for HIV-associated facial
lipoatrophy. Dermatol Surg 2007;33:S193–8.