Embed Size (px)
Citation preview

Sensoristrain: an exploration of nursing interventions in the context of the Neuman systems theory Pauline Black, Pat Deeny and Hugh McKenna
Pauline Black PGDip Adv Nurs BSc(Hons), RGN, Staff Nurse, Intensive Care Unit, Belfast City Hospital, LIsburn Road, Belfast BT9 lAB, UK
Pat Deeny BSc, RNT, RGN, Lecturer in Critical Care, Department of Nursing, University of Ulster at Colerame, Cromore Road, Coleraine, Co. Londonderry, UK
Hugh McKenna DPhfl, BSc, DipN (Lon), RGN, Coordinator of Nursing Research, Department of Nursing, University of Ulster at Jordanstown, Shore Road, Newtonabbey, Co. Anmm, UK
(Requests for offprints to PB) Manuscript accepted I I July 1997
Defining what nurses do and why has been the endeavour of many researchers, both academic and clinical. Nursing interventions are a fundamental component of nursing practice and a focus on accountability means that nurses must be able to justify their actions. The sensoristrain experience of intensive care patients is widely acknowledged in nursing literature, though without the use of the word 'sensoristrain'. The aim in this paper is to place patients, their experience and the role of nurses within the practical framework of a suitable nursing theory which will elucidate and guide everyday practice in preventing and alleviating the causes (stressors), symptoms (reactions) and emotional aftermath. Nursing interventions appropriate for the three modalities of intervention elucidated by the Neuman systems theory have been outlined, paralleled by a discussion of how these could relate to the three dimensions of nursing care: comfort care; knowing the patient; and the therapeutic presence of the nurse. Nurses must use each opportunity to advance practice through emphasizing the value of nursing in today's cost- conscious health care climate. In order to do this, and to ensure nurses' continued presence at the bedside, clear articulation of the contribution of
nursing interventions to improved patient outcomes is essential.
I N T R O D U C T I O N
A fundamental component o f nursing practice in critical care is the nursing action or nursing intervention. Definition of what is a nursing intervention is difficult in most settings, but such difficulties are more apparent in an inten- sive care setting. The emphasis placed on phys- iological monitoring and the maintenance of homeostasis may contribute to this. Discriminating interventions that can strictly be defined as 'nursing' from the interventions of other health care professionals is sometimes dif- ficult. In the psychosocial domain, such diffi- culties are not as obvious. While such issues may seem pedantic in a setting where the team approach is always encouraged, in an age when accountability for action is crucial, the focus on nursing interventions seems imperative. Nurses must justify their interventions.
Kim (1983) suggested that nursing interven- nons are problematic due to their 'fuzziness'. The causes of such fuzziness are not only the overlap with the interventions of other health care professionals but the percmved similarity of nursing interventions to the actions o f ordi- nary people. She went on to argue that it is not so much the intervention per se that should be the focus but when, how and why the inter- vention should be carried out. Proponents o f evidence-based practice may have moved on from Kim's analysis but the need for reasoned nursing interventions remains the same. Such a rationale not only requires nurses to provide empirical evidence when it is available but also to put each intervention into the context of a nursing model. The model provides the neces- sary clarification of beliefs, values and goals that makes the intervention meaningful.
What makes nursing different is the unique value and belief system that is at the heart of nursing practice, combined with professional knowledge bases and clinical skill. Making explicit what nurses do and why has been the endeavour of nursing theorists. In the clinical area, however, arranging nursing interventions to fit the requirements of a specific model or theory o f nursing can often become a manda- tory exercise rather than a reflection of the focus o f patient care. This may have the poten- tial to exacerbate any theory-practice gap, sustaining the belief that theoretical under- pinnings may be cumbersome m action.
Moving to another perspective, nurses should be enabled to look at specific interven- tions that form the basis of their practice in
Intensive and Critical Care Nursing (I 997) 13 249-258 © 1997 Harcourt Brace & Company Ltd

250 Intensive and Critical Care Nursing
terms of origin, focus and intended effect. Examining the beliefs and values held by nurses during their practice could highlight the achievements of the interventions. It may be that at this stage, the search for a suitable theo- retical framework would be successful and would serve to validate the interventions as uniquely nursing in orientation. In this way, an invaluable contribution could be made to developing a strong rationale for the nurses' role in providing skilled, individualized and evidence-based patient care.
_ ~ II . . . . .
SENSORISTRAIN REVISITED
This paper is concentrated on the nursing interventions associated with the manage- ment o f the sensory response to intensive care, a response conceptualized as sensoris- train in a previous paper (Black et al 1997). While this area has received a lot of attention in the intensive care literature, there is a marked shortage o f papers dedicated to nurs- ing interventions. The sensory stress response to the critical care environment has been explored exhaustively, both in research stud- ies and in discussion articles throughout the nursing literature. Most papers focus on the impact o f the unique physical environment o f intensive care units (ICUs) in terms of noise, light and technology (Kornfeld 1969, McGonigal 1986, Ashworth 1990, Dunn et al 1995, Locsin 1995, Wakers 1995). The expe- rience o f being ventilated and unable to com- municate verbally has been explored, with emphasis on the impact this has on nurse-patient interaction (Bergbom-Engberg et al 1988a, Jablonski 1994, Hagland 1995, Baker & Melby 1996). Other authors decribe the symptoms of sensory stress as displayed by observable patient behaviours (Dyer 1995a, Laitinen 1996), while some offer possible interventions that may be used to reduce the stress experienced by such patients (Bergbom-Engberg et al 1988b, Stanton 1991, Dyer 1995b).
THEORY FOR PRACTICE .... i,!,,llrl
The literature has enabled nurses to understand and recognize patients' experiences ofsensoris- train and to appreciate the impact that this has on physical and psychological recovery and subsequent well-being. In order to advance the dimension of practice in this area, a sound framework for identifying and evaluating effec- tive interventions must be developed. This framework should link the individuality of each
patient, the stressful stimuli and the role o f the nurse in order to identify appropriately the focus and effect of the interventions. This paper will contribute to the development of such a structure by drawing on the relevance of the Neuman system theory (Neuman 1989). Relevant concepts will be outlined, highlight- ing the Inks with current practice. Using the structure of the theory, interventions will be grouped into three hierarchical modalities, and the implications for developing practice dis- cussed.
The theoretical framework proposed is the Neuman system theory, which has been widely utilized as a framework for research into critical care nursing (Gries & Fernsler 1988, Fulbrook 1991, Kido 1991). The focus of critical care - the maintenance and reconstitution of unstable physiological systems - lends itself to the appli- cation of a systems theory which could be rec- ognized as congruent with practice. The most relevant theoretical assumptions for the pur- pose of this paper have been adapted from an analysis of Neuman's theory by Fawcett (1993), and include the belief that:
• Each individual is a unique system in constant interaction with his or her environment, be it internal (physical and personal), or external (people and surroundings). Cushioning this system are various fines ofdefence and resistance which act to protect the system.
• The internal and external environments contain stimuli that individuals may perceive as stressors. Each stressor has the potential to damage lines ofdefence and resistance and thus threaten the stasis of the system.
• This disruption causes a reaction from the system that can be measured or observed and which serves as an alarm indicating violation. Interventions can then be initiated to reconstitute the system and reinforce the affected fines o f resistance.
Neuman uses Selye's (1976) definition o f stress to underpin the theory. Accordingly, stress is the response o f the body to demands made on it in terms of adapting the self and coping with the stress, or attempting to over- come the effects o f the pressure being exerted and maintain some degree o f homeostasis. Individual differences in perception and response patterns, so relevant in sensory stress, are taken into account by the presence o f internal and external conditioning factors, and this reinforces nursing values about the uniqueness o f the human experience o f ill- ness. This theoretical orientatzon can be clearly linked to the physiology of sensory processing, particularly the role o f cortical

Sensoristrain in ICU patients 251
PRIMARY PREVENTION
- /
[
I
I
%% % %,
STRESSORS
i -t -t t t l
%
I I I e ~ l l I I I I I | 11 I I I I t I I I ', ,, ,, , , / / % %% ~ . . . _ . . . = ~ , /
% % ~ - - - - ,,¢.
TERTIARY PREVENTION & RECONSTITUTION Z y
REACTIONS
% % /' I
I I I I I / , I
! I
/ 1 / al
S
SECONDARY INTERVENTION
Nursing Intervention
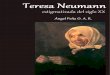
Fig. I Framework for Interventions based on and adapted from Neuman's Systems Theory (Marriner-Romey, [ 994).
association in perception, and would thus appear to reflect the sensoristrain experience accurately.
Each individual is conceptualized as an open system, interacting and adjusting freely with his or her environment, but buffered by lines of defence and resistance that have developed over time (Marriner-Tomey 1994). By this means, the individual maintains equilibrium when confronted by a stressor. In critical ill- ness, the physiological lines ofdefence are vio- lated by intubation, intravascular cannulation, surgery, sepsis and the systemic response to critical illness, i.e. inflammation, disturbance of
homeostasis, stress-induced endocnne changes and autoimmune reactions (Carson 1993). Similarly, the psychosocial and cultural lines of resistance surrounding the self and the integrity of personhood are threatened by stress-induc- ing factors inherent in the sensory environ- ment. Smith (1989) and Price (1990) describe how becoming a patient can alter the way in which the physical body is experienced (pro- prioception) and thus the sense of self is pro- roundly affected. Inability to move, communi- cate and reinforce self-image may contribute to misperception of the sensory environment in an ICU.

252 Intensive and Critical Care Nursing
Table I Stressors identified in selected literature. These are classified as being either intra-, inter- o r extrapersonal in origin, according to the framework of Neuman's theory ( I 989)
. . . . . . . . . . . . . . . . . . . . . . .
Author Study type
Smith (I 989)
Bergbom-Engberg et al (1988a,b)
Gries & Fernsler (1988)
Heath (1989)
Reigel (I 989)
Kido (1991)
Stanton ( 1991 )
Tucker (1993)
Jablonski (1994)
Dyer (I 995a)
Farren et al (1995)
Bergbom-Engberg et al ( 1988a, b)
Gries & Fernsler (1988)
Stanton (1989)
Jablonski (1994)
Farran et al (1995)
Smith (1989)
Gries & Fernsler (1988)
Heath (1989)
Jablonski (1994)
Farran et al (1995)
Personal account
Retrospective Interview-based n = 304
Retrospective Interview-based n = 1 7
Anecdotal discussion
Discussion
Case study
Discussion
Discussion
Retrospective Interview-based n = 1 2
Discussion
Discussion
Retrospective Interview-based n = 304
Retrospective Interview-based n = 1 7
Discussion
Retrospective Interview-based n = 1 7
Discussion
Personal account
Retrospective Interview-based n = 1 7
Anecdotal discussion
Retrospective Interview-based n = 1 2
Discussion
Intrapersonal stressors Proprioception d~sturbances Inability to rationalize care
Fear: of unknown; of dying; of equipment failure Not knowing what was real or unreal Panic Pain
Disturbing dreams
Inability to distinguish passage of time
Perceived lack of control
Disturbed sleep patterns
Impaired day/night rhythms
Toxins, sepsis, medications, hypoxia
Poor vision, taste and tactile ability Numbness D~stortion of time and memory Powerlessness
Monopolization of sight, hearing, touch and smell
Hopelessness Physical deterioration Poorly controlled symptom management
Interpersonal stressors Lack of trust in staff Communication difficulties Inadequate information
Lack of explanations prior to carrying out procedures
Social ~solation
Being treated as a mere object
Devaluation of personhood
Extrapersonal stressors Extremes of environmental temperature
Immobility Physiotherapy and suctioning
Lack of natural light Noise generated by health care staff
Equipment alarms
Poorly controlled symptom management
STRESSORS
According to the Neuman theory (1989), stres- sors are stimuli with the potential for causing disequilibrium and the stress experience within a person. These potentially stressful stimuli may be intrapersonal (within the self), interpersonal (between self and other persons) or extraper- sonal (in the external environment). Literature providing insight into the type o f stressors
experienced by patients in an ICU has been mostly retrospective in nature, research prob- ing the remembered experiences o f patients or anecdotal evidence of stressful events. When discussing these stressors, it must be borne in mind that the depth of the data relies on the accuracy of patient recall, and that positive experiences are often relegated in memory, replaced by more vivid recall of negative events. Table 1 summarizes a selection of these articles and the stressors identified therein.

Sensoristrain in ICU patients 253
Table 2 Reactions identified in selected literature
Author Reactions identified
McGonigal (I 986)
Easton & McKenzie (1988)
Vander et al (I 990)
Inaba-Roland & Maricle (1992)
Daffurn et al (I 994)
Jablonski (I 994)
Farran et al (1995)
Granberg et al (I 996)
Exhaustion Paranoia Delusions Disturbance of perception
Fluctuating consciousness Lack of coherence Aggression Disorientation in t,me, place and person
Hypertension Tachycardia Hyperventilation Palmar sweating Clammy skin and peripheries
Delirium Agitation Anxiety Depression Hostility Memory impairment Emotional lability
Post-discharge: depressmon; irritability; loneliness
Distortion of higher thought processes Non-compliance Hallucinations Disturbing dreams
Hopelessness
Fear Panic
The stimuli in ICUs impose excessive demands on individuals to maintain sensory balance: normally recognizable stimuli are dis- torted and lack meaning. Intense internal effort is made to interpret sense in all the input, and the void is filled with meanings derived from past experiences, memory and imagination, resulting in sensoristrain (Black et al 1997). Laitlnen (1996) proposed that such persons lose touch with reality, replacing it with their own interpretation, to which they respond with anxiety and confusion. The strain produced by this effort to understand and control the stimuli results in the behaviours and reactions that nurses must assess and alleviate so that the integrity o f the individual system is preserved or restored.
L . . . . . . . . . . .
R E A C T I O N S
The amount of system instability precipitated by exposure to the perceived stressors may be called the reaction to the stimuli (Fawcett 1993). The type o f reaction and subsequent behaviour must be as unique as the individual's perception. This may limit the practical value of descriptions of possible behaviours found in the literature, as many behaviours will be discovered in practice
that have not been documented, but which can- not be dismissed as non-indicative o f a stress response. Nevertheless, a knowledge of e~sting reactions uncovered by research is a useful tool for identifying and assessing the extent of per- ceptual disruption (Table 2).
Armed with an awareness o f the vulnerabil- ity of each individual and a knowledge of potential stressors and reactions, the nurse is equipped to recognize that all patients in inten- sive care are at risk of experiencing sensoris- train. This preliminary nursing diagnosis is the first of a three-step nursing process inherent in the Neuman theory. Once the diagnosis has been reached, Neuman (1989) has described the goal o f nursing:
to assist the client in creating and shaping reality in a desired direction . . . the mainte- nance of optimal system wellness . . . through purposeful interventions [which will] mitigate or reduce stress factors and adverse conditions which affect client func- tioning. (p 17)
m_
I N T E R V E N T I O N S
The desired direction and outcome of nursing interventions must be made explicit before implementation can be evaluated as effective. The inherent barriers to communication between a nurse and a patient in intensive care make it difficult to determine the 'desired direction' from the patient's perspective. Minimizing the sources and effects o f sensory stressors in an empathic manner may be one route around this widely recognized problem.
Many interventions for the reliefofsensoris- train have been proposed in the literature. Focused on the reduction and the removal o f stressors from the environment and the reori- entation of the person, many are valuable actions requiring nursing skill. However, Henneman (1989) suggests that many inter- ventions are used in practice because they are traditional or are considered inherently good for patient well-being. The effectiveness of the interventions may not have been subjected to research study or validation. Unclear outcomes do not provide a defensible case for the inclu- sion of the interventions in practice and reflect poorly on the profession as a whole. Using modalities to provide a framework for inter- ventions will facilitate empirical demonstration o f interventions that prove to be appropriate and effective.
In Table 3, interventions have been classi- fied according to Neuman's modalities: pri- mary prevention; secondary intervention; and tertiary prevention. Each intervention has been

254 Intensive and Critical Care Nursing
Table 3 Interventions identified in selected literature
Focus Author
Communication Gries & Fernsler (1988) Dyer (I 995b) Baker & Melby (1996)
Perception Green (I 992) Bassett (1993)
Sleep/rest Finlay (I 99 I) Dunn et al (1995)
Pain
Family
Inaba-Roland & Maricle (1992)
Heath (I 989) Stanton ( 199 I) Waiters (I 995)
Powerlessness Dyer (I 995b) Depersonalization
Confusion Laitinen (I 996)
Hopelessness Farran et al (1995) Cutcliffe (I 996)
Reassurance Stockdale (1989) Fareed (I 996) Cutler & Garner (1995)
Audit Dyer (1995b)
Primary preventions Use reassuring words Nursing introductions when assuming care Explore miming, sign language or writing Extend communication beyond explanations about tasks:
orientation, day, time, weather, current events Use tracheostomy speaking tubes were appropriate,
alphabet boards and picture charts Ensure each named nurse cares for his/her particular patient Use appropriate language which the patient will understand
Ensure unnecessary equipment is out of patient's sight Use -I-V, radio, clocks, calendars Read get well cards Sit up in bed, use spectacles if worn Attach lines securely with plenty of slack to allow movement
Reduce light and noise at night Organize care in 90-minute intervals to allow for completion
of sleep cycles Use massage on back, outside of limbs and scalp Ensure at least 30 minutes of undisturbed rest during the
daytime
Assume that all patients suffer pain unless proved otherwise Assess for signs of pain, i.e. grimacing Administer prescribed boluses of analgesia prior to changing
posit~on in bed Use relaxation, massage, changes of position and hot or cold
packs as non-pharmaceutical aids
Ask for photographs of the patient and family to use to reorientate and provide another image of the patient
Encourage family members to interact with the patient Meet family needs to be with and see the patient
Secondary interventions Inform medical staff and exclude possible physical reasons for any changes in patient behaviour and ensure maintenance af a safe environment Ensure continuity of care by named nurse Repeated introductions and explanations due to poor recall Obtain permission prior to interventions and offer choice
where possible in the care given
Provide a physical presence: use touch Ensure the nurse is known to the patient by name Provide ongoing and appropriate reorientation
Give detailed information and explanations Demonstrate commitment to the patient as a worthwhile
cause: provide consistent help Plan achievable goals to reinforce progress
Ter t iary preventions Continue to use appropriate means of communication Use explanations to present the environment in an
unthreatening manner Allow time to just be with the patient, talking and sharing
their experiences Assert realistic optimism and hope for the future as the
patient continues to recover Demonstrate empathy, genuineness and acceptance of the
person Use improvements in the patient's condition to begin to
prepare him/her psychologically for transfer to the ward
Examine the environment of the ICU and, at a local level, the bedspace itself for the presence of potential sensory s t regsors
Ensure continual scrutiny of practice through sharing experiences and up-to-date information and research with peers
Follow-up patients on transfer to gain feedback of their experience of their care
Put findings into practice

Sensoristrain in ICU patients 255
found in: (1) anecdotal accounts of helpful nursing care; (2) articles discussing interven- tions that are considered to relieve sensory stress; or (3) research studies into specific inter- ventions used in intensive care. The intention has not been to present a definitive categoriza- tion of interventions but to illustrate possibili- ties for research.
Primary preventions and comfort care
Primary preventions are initiated when an individual is admitted to an ICU. Although this person is exposed to a multiplicity o f stressors, reactions may not yet have been observed. Prevention is the goal o f these interventions, in an attempt to reduce the pos- slbility o f the individual encountering a stres- sor and to strengthen the flexible line o f defence, to increase resistance to stressors when encountered.
Open lines o f communication and interac- tion are obviously and ideally the starting point for nursing care in ICU. The power o f an interactive nurse-patient relationship has been well researched (Ashworth 1980, Mallett 1990, 1Kundell 1991, Bergbom-Engberg & Haljamae 1993, Leathart 1993, Hagland 1995). The main issue relating to communica- tion in the I C U appears to be the continued implementation o f the research findings m practice and the ability o f nurses to overcome the unique barriers to interaction in the form of unconscious, unresponsive and intubated but conscious patients. However, not all interaction must be verbal in order for patients to realize that they personally are the central focus o f a caring scenario.
In an attempt to reach an understanding of patient experiences, Kolcaba (1995) suggests that nurses use the concept of comfort care. This has been defined as:
the satisfaction of basic human needs for relief, ease or transcendence that arise from stressful health care situations. (p 288)
Researching the comforting role o f critical care nurses, Walters (1994) found that nurses interviewed described comforting with refer- ence to the following foci:
• Providing support to the patient, from washing their hair to monitoring cardiac output
• Relieving pain • Relieving anxiety through successfully
reading their patients' emotional states and helping them to resolve problems
• Communicating with both conscious and unconscious patients, using opportunities
for interaction, pausing for response or reply • Using touch to establish a presence with
patients and acquire a closeness over the time spent caring for them
• Comforting when death is imminent: priontizing care to ensure dignity and peace
• Comforting family and friends, listening to their concerns and facilitating the maintenance of family unity
• Supporting other nursing staffby sharing experiences and skills in communicating with patients.
It may only be coincidental that many of the primary prevennons listed in Table 3 cor- relate with the comforting role identified by Waiters (1994). It is obvious that comfort care could underpin all nursing practice at this level in the relationship as the patient's physical and psychological comfort becomes the motiva- tion for nursing interventions. 1Kesulting out- comes include the meeting of the patient's needs, the development of patient trust in the nurse, and the nurse's individualized know- ledge o f the patient. It may often mean that care will be creative and innovative in order to enhance comfort and build a solid founda- tion for the nurse-patient relationship (Scott 1995). As well as developing practice, this relationship is particularly important when reactions to sensoristrain develop, and the nurse may be the only remaining constant in the patient's reality.
Secondary interventions: knowing the patient
Secondary interventions are selected when a reaction to a stressor has occurred. These inter- vennons are focused on dealing with immedi- ate symptoms and encouraging individuals to use internal and external resources to strengthen the lines of resistance. In order to &agnose, nurses will have collected data during interactions and will have noted the develop- ment of confusion, depression or other possible signals that all is not well. At this stage, patient would be increasingly aware of the surrounding environment as a result of being weaned from sedation and mechanical ventilation. Inter- ventions would thus be aimed at reorienting and encouraging expression of the patient's experiences through means of communication established during primary interventions. Many of the patients' concerns are self-focused and relate to physical needs or worries embedded in their thoughts. The resolution o f these con- terns is of utmost importance to these patients. Lusardi & Schwartz-Barcott (1996) caution that although these concerns are sensible to the patients, their expressed thoughts are often

256 Intensive and Critical Care Nursing
considered delusional by staff. Often zt is the patient who has withdrawn from reality in response to sensoristrain who presents a chal- lenge to nurses. Hopelessness and powerlessness rapidly demotivate the patient and exhaust stores of motivation. Patients have identified nurses as a specific source o f hope when they had acknowledged that their own internal resources were not strong enough to sustain them (Cutcliffe 1996). Nurse presence and intervention must convey the belief that the patient has a future (within realistic limits). Patients are perceptive, feeling individuals who are sensitive to the way in which they are treated, and the manner in which each nurse approaches and interacts may make or break the therapeutic relationship.
Taking time to obtain permission before commencing tasks and offering a choice of options in the care to be given may have a posi- tive effect on feelings of depersonalization, although a few attempts may need to be made before a patient readily offers a personal opinion after being subjected to the enforced regimes of treament so pervasive in the ICU. The rationale is a simple one: to help patients to become active participants rather than passive recipients of care. Offering several options from which to choose may reinforce self-concept and aware- ness due to the cognitive process involved in reaching a decision such as ' D o / w a n t to get up to sit n o w or later in the afternoon?'.
Skill in identifying suitable and appropriate interventions develops from the unique know- ledge of the patient gained by the nurse, a con- cept analysed by Jenny & Logan (1992) and Tanner et al (1993). Knowing the patient is the result of time spent caring for the individual in a meaningful way: trying to grasp the meaning of a situation for the patient. 1Kadwin (1996) has suggested that it is a further dimension of nursing practice which permits individualized care pivoted around the mutual understanding of the situation and characteristics of the patient and the nurse. As personal practice has demon- strated, using caring as an opportunity to get to know patients pays dividends in understanding what is needed in their care.
Ter t i a ry prevention and nursing presence
Tertiary prevention occurs when some degree of stability has returned following successful secondary intervention, and relates to the mobilization o f an individual's resources to prevent additional reactions to the stress experi- enced. The aim is to reconstitute and strengthen each patient's system, enabling them to balance sensory input during the rest of their stay in the ICU and on transfer to the ward.
Judging from the literature, this appears to be the least developed area o f research. Stockdale (1989) has suggested that it is the quality o f the interpersonal encounter between the nurse and patient that is the most significant factor in determining outcomes. Due to the nature o f critical illness, each patient who leaves the unit has survived a brush with death. The intense emotions that must be associated with this experience and subsequent outcomes do not appear to have been studied in depth. Clearly it is not sufficient for nurses to help medicine to 'patch' physiological systems if the patients leave the environment o f care psychologically abused and scarred. By demonstrating empathy, genuineness and accepting as legitimate the concerns o f patients, nurses may help in recon- ciling patients' experiences o f the sensory envi- ronment and their fears for the future as they return to the ward.
THE ROLE OF NURSING
Putting interventions into practice through all intervention modalities necessitates one com- mon factor: the presence o f the nurse with the patient. Increasing interest has appeared in the concept o f nursing presence. Minick (1995) studied patient care narratives from critical care nurses and discovered that caring, as manifested by an involved stance from the nurse, can heighten nurse perceptions and improve assess- ment and recognition o f problems. Practising nursing presence requires a prerequisite know- ledge o f the patient but also adds a therapeutic dimension. Being present has been conceptual- ized by Osterman & Schwartz-Barcott (1996) as a continuum ranging from being physically there and task-focused to involving the patient (other-focused), and ultimately involving the patient physically, psychosocially and spiritually in a relationship that transforms and illuminates the unity of the nurse and patient towards a common goal. Essentially, being present for the patient in this way involves a gift o f self con- veyed through open and giving behaviours.
Henneman (1989) tested the hypothesis that direct nursing contact (hand-holding and ver- bal interaction) with patients being weaned from mechanical ventilation would reduce the stress response when compared with patients who received no direct nursing contact. The hypothesis was not supported, neither group exhibiting a statistically significant stress response. Both groups, however, received psy- chological preparation, and a nurse was in con- stant attendance. A conclusion that could legit- imately be drawn is that the nurse, by being present, psychologically preparing each patient

Sensoristrain in ICU patients 257
and control l ing the envi ronment , effectively
diminished the stress response for all patients in
the study. Here is an intr iguing allusion to the
relationship be tween the nurse's presence and a
posit ive effect on reducing stress and improv ing
patient ou tcomes as suggested by Broo ten &
Nay lo r (1995).
T h e use o f audit to assess the I C U envi ron-
men t has been encouraged by Dyer (1995b)
w h o devised a checklist for use as a means o f
ensuring that nursing interventions remain
poten t and patient-orientated. This could raise
staff awareness o f the need to consider and
develop their practice in a bid to min imize
patient exposure to unnecessary stressors. M a n y
o f the most effective nursing interventions do
not involve structural alterations or the pur-
chase o f quieter equipment , but personal atten-
tion. H o w e v e r , a l though thoughtful care may
no t have a high financial cost, the personal and
emot ional cost o f caring wi th c o m m i t m e n t
must not be underest imated (1Lushton 1992).
T h e essential investment o f t ime and self in care
requires a strong team spirit and interpersonal
support among peers to ensure that personal
internal resources, so often depleted and
ignored, are replenished to enable nurses to
cont inue to care effectively.
- . . = . . . . . . .
CONCLUSION
In conclusion, an at tempt has been made to
demons t ra te the re levance o f the N e u m a n
systems theory as a f ramework for further
examinat ion o f sensoristrain in I C U patients.
Nurs ing interventions appropriate for the three
modalit les have been delineated, paralleled by a
discussion o f h o w these could relate to three
dimensions o f nursing care: comfor t care;
k n o w i n g the patient; and the therapeutic pres-
ence o f the nurse. Nurses must use each oppor -
tunity to advance practice th rough emphasizing
the value o f nursing in today's cost-conscious
health care climate. In order to do this, and to
ensure the cont inued presence o f nurses at the
bedside, clear articulation o f the cont r ibut ion
o f nursing interventions to improved patient
ou tcomes is required.
Advanced nursing is about not only p rov id-
ing expert physical care but also filling the need
for humanist ic care wi th the core o f nursing
practice; that is, care based on the be l ie f that the
nursing that people receive should include
more than that wh ich concerns the physical
be ing o f the person. Deve lop ing a body o f
knowledge for practice that is different f rom
the knowledge base o f medically orientated
care is the challenge faced by nurse researchers,
w h o must demonstrate the efficacy o f nursing
theories in facilitating advanced research-based
knowledge and practice (Phillips ]995).
Internalizing nursing theories that are con-
gruent wi th individual nurses' values may c o m -
prise the foundat ion for practice w h e n fully
integrated into the nurse's way o f caring. It is in
this way, suggests Smith (1995), that theory
becomes dynamic and practice-transforming,
individualized to different practice settings as
wel l as to patients.
REFERENCES
Ashworth P 1980 Care to communicate - an investigation into problems of communication between patmnts and nurses m intensive therapy units. Royal College of Nursmg, London
Ashworth P 1990 High technology and humanity for intensive care. Intensive Care Nursing 6 (3): 150-160
Baker C, Melby V 1996 An invesnganon into the amtudes and practices of intensive care nurses towards verbal commumcanon with unconsczous patients. Journal of Chnical Nursing 5:185-I92
Bassett C C 1993 Commumcation math the critically 111. Care of the Critically 111 9 (5) 216-219
Bergbom-Engberg I, Haljamae H 1993 The communication process math ventilator patients in the ICU as perceived by the nursing staff. Intensive and Critical Care Nursing 9:40-47
Bergbom-Engberg I, Hallenberg B, Wickstrom I, Haljamae H 1988a A retrospective study of patients' recall of respiratory treatment (1): study design and basic findings. Intensive Care Nursing 4 (2): 56-61
Bergbom-Engberg I, Hallenberg B, Wlckstrom I, Haljamae H 1988b A retrospective study ofpatmnts' recall of respiratory treatment (2): nursing care factors and feehngs of security/insecurity. Intens]ve Care Nursing 4 (2): 95-101
Black P, McKenna H, Deeny P 1997 A concept analysis of the sensoristrain experienced by intensive care patients. Intensive and Critical Care Nursing 13 (4)" 209-215
Brooten D, Naylor M D 1995 Nurses' effect on changing patient outcomes. IMAGE: Journal of Nursing Scholarsl'np 27 (2): 95-99
Carson S 1993 Complicatmns ofcntlcal care In: HallJ B, Schrmdt G A, Wood L D H (eds) Principles of critical care. McGraw Hill, New York
Cutchffe J 1996 Cntlcally 111 patients' perspectives of hope BntlshJournal of Nursing 5 (11): 674-690
Cutler L, Garner M 1995 Reducing relocatmn stress after &scharge from the intensive therapy unit. Intensive and Critical Care Nursing 11 (6): 333-335
Daffurn K, Bishop G F, Hillmann K M, Bauman A 1994 Problems following discharge after intensive care. Intensive and Critical Care Nursing 10 (4). 244-251
Dunn C, Sleep J, Collett D 1995 Sensmg an improvement: an experimental study to evaluate the use ofaromatherapy, massage and periods of rest in an intensive care unit. Journal of Advanced Nursmg 21:34--40
Dyer I 1995a Preventing the ITU syndrome or how not to torture an ITU patient! Part 1. Intensive and Critical Care Nursing 11 (3): 130-139
Dyer I 1995b Preventing the ITU syndrome or how not to torture an ITU patient! Part 2. Intensive and Cntical Care Nursing 11 (4): 223-232
Easton C, Mackenzie F 1988 Sensory-perceptual alterations: dehrium in the intensive care umt. Heart and Lung 17 (3). 229-235

258 Intensive and Critical Care Nursing
Fareed A 1996 The experience of reassurance: paUents' perspectives. Journal of Advanced Nursing 23: 272-279
Farran C J, Herth K A, PopovichJ M 1995 Hope and hopelessness: critical clinical constrncts.Sage, London
FawcettJ 1993 Analysis and evaluation of conceptual models of nursing, 3rd edn. F A Davis, Philadelphia
Finlay G 1991 Sleep and intensive care. Intensive Care Nursing 7 (1): 61-68
Fulbrook P 1% 1991 The application of the Neuman systems model to intensive care. Intensive Care Nursing 7:28-39
Granberg A, Bergbom-Engberg I, Lundberg D 1996 Intensive care syndrome: a literature review. Intensive and Chnical Care Nursing 12 (3) 173-182
Green A 1992 How nurses can ensure that the sounds patients hear have a positive rather than a negative effect on recovery and quality of life. Intensive and Cntical Care Nursing 8 (4): 245-248
Gnes M, FernslerJ 1988 Patient perceptions of the mechanical ventilation experience. Focus on Critical Care 15:52-59
Hagland M 1% 1995 Nurse-patient communication in intensive care: a low prionty? Intensive and Critical Care Nursing 11 (2) 111-i15
HeathJ V 1989 What the patients say. Intensive Care Nursing 5 (3). 101-108
Henneman E A 1989 Effect of nursing contact on the stress response ofpauents being weaned from mechanical ventdation. Heart and Lung 18 (5): 483-489
Inaba-1%oland K E, Mancle 1% A 1992 Assessing delirium in the acute care setting. Heart and Lung 21:48-55
Jablonski 1% S 1994 The experience of being mechanically ventilated. Qualitative Health 1%esearch 4 (2): 186-207
Jenny J, LoganJ 1992 Knowing the patient: one aspect of chmcal knowledge. IMAGE: JournalofNursmg Scholarship 24 (4): 254-258
Kido L M 1991 Sleep deprivation and intensive care unit psychosis. Emphasis: Nursing 4 (1): 23-33
KAm H S 1983 The nature of theoretical thinking in nursing. Appleton-Century-Crofts, Norwalk
Kolcaba K Y 1995 The art of comfort care. IMAGE: Journal of Nursing Scholarship 27 (4): 287-289
Kornfeld D S 1969 Psychiamc view of the intensive care unit. British Medical Journal January: 108-110
Laatlnen H 1996 Patients' experience of confusion in the intensive care unit following cardiac surgery. Intensive and Critical Care Nursing 12 (2): 79-83
Leathart AJ 1994 Communication and soclalisatlon (1): an exploratory study and explanation for nurse-patient communication in an ITU. Intensive and Critical Care Nursing 10 (2): 95-104
Locsin 1% C 1995 Machine technologies and caring in nursing. IMAGE: Journal of Nursing Scholarship 27 (3): 201-203
Lusardi P T, Schwartz-Barcott D 1996 Makang sense of it: a neuro-mteractionai model of meaning emergence in critically 111 ventilated patients. Journal of Advanced Nursing 23:896-903
McGomgal K S 1986 The importance of sleep and the sensory environment to critically ill patients. Intensive Care Nursing 2 (2): 73-83
Marnner-Tomey A 1994 Nursing theonsts and their work, 3rd edn. Mosby, St Louis
Mallett J 1990 Communication between nurses and post- anaesthetic patients. Intensive Care Nursing 6 (1): 45-53
Mlmck P 1995 The power of human caring: early recognition of patient problems. Scholarly Inquiry for Nursing Practice 9 (4): 303-321
Neuman B 1989 The Neuman systems model, 2end edn. Appleton & Lange, Norwalk
Osterman P, Schwartz-Barcott D 1996 Presence: four ways of being there. Nursing Forum 31 (2): 23-30
Phillips J k 1995 Nursing theory-based research for advanced nursing practice. Nursing Science Quarterly 8 (1): 4-5
Pnce B 1990 Body image: nursing concepts and care. Prentice Hall, New York
Radwm L E 1996 Knowing the patient: a review of research on an emerging concept. Journal of Advanced Nursing 23:1142-1146
Raegel B 1989 Stressors ofcntlcally ill patients.In' Riegel B, Ehrenreich D (eds) Psychological aspects of critical care nursing. Aspen, Maryland
1%undeU S 1991 A study of nurse-patient interaction in a high dependency unit. Intensive Care Nursing 7 (3): 171-178
Rushton C H 1992 Care-giver suffering in critical care nursing. Heart and Lung 21 (3): 303-306
Scott A P 1995 Care, attention and imaginative identification in nursing practice. Journal of Advanced Nursing 21:1196-1200
Selye H 1976 The stress ofhfe. McGraw Hill, New York Smith M C 1995 The core of advanced practice nursing.
Nursing Science Quarterly 8 (1): 2-3 Smath S A 1989 Extended body image in the ventilated
patient. Intensive Care Nursing 5 (1): 31-38 Stanton DJ 1991 The psychological impact ofmtensive
therapy the role of nurses. Intensive Care Nursing 7 (4): 230-235
Stockdale L L 1989 Person-centered counselling: apphcation in an intensive care setting. Heart and Lung i8:139-145
Tanner C A, Benner P. Chelsea C, Gordon D 1% 1993 The phenomenology of knowing the patient. IMAGE: Journal of Nursing Scholarship 25 (4): 273-280
Tucker L A 1993 Post-pump dehrium. Intensive and Critical Care Nursing 9 (4): 269-274
Vander A J, Sherman J H, Luciano D S 1990 Human physiology, 5th edn McGraw-Hill, New York
Waiters AJ 1994 The comforting role in critical care nursing practice: a phenomenological interpretation. International Journal of Nursmg Studies 31 (6): 607-616
Waiters AJ 1995 A hermeneutic study of the experiences of relatives of critically 11I patients. Journal of Advanced Nursmg 22:998-1005