Embed Size (px)
Citation preview

Sentinel lymph node biopsy correctly predicts regional lymph node recurrence in trunk malignant melanoma with multiple drainage basins
Saeed Farzanefar1, Mehrshad Abbasi1, Davood Beiki2
1Department of Nuclear Medicine, Valiasr Hospital, Tehran University of Medical Sciences, Tehran, Iran 2Research Center for Nuclear Medicine, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran
(Received 13 September 2016, Revised 15 November 2016, Accepted 16 November 2016)
ABSTRACT
We report a young male with an initial excisional biopsy report of melanoma of the lower back, referred to our hospital for complete excision and sentinel lymph node (SLN) biopsy. Four peritumoral intradermal Tc-99m phytate injection was performed and SLNs were detected in both axillary and right inguinal regions. On the biopsy only the right axillary SLN was metastatic leading to right axillary lymph nodes dissection 6 days later. No other surgical intervention was done for two other lymphatic drainage basins. On follow up the patient noted a right axillary mass with highly suspicious ultrasound findings. Metastatic work up was negative. Second axillary lymph node dissection confirmed conglomerated lymph nodes metastases in this area. Multiple drainage basins in the trunk melanoma are common and many authors have concern about changing in lymphatic drainage pattern after SLN biopsy and surgical manipulation. This case showed correct initial diagnosis of involved lymph nodes in one out of three lymphatic drainage basins, and also correctly predicts regional recurrence in the same location. Key words: Sentinel lymph node; Melanoma; Multiple drainage basin; Recurrence
Iran J Nucl Med 2017;25(1):77-80 Published: January, 2017 http://irjnm.tums.ac.ir
Corresponding author: Dr Saeed Farzanefar, Department of Nuclear Medicine, Valiasr Hospital, Tehran University of Medical Sciences, Tehran, Iran. E-mail: [email protected]
Case R
epo
rt

Sentinel lymph node biopsy in multiple drainage basins Farzanefar et al.
Iran
J N
ucl M
ed 2
017,
Vol
25,
No
1 (S
eria
l No
47)
h
ttp:
//irj
nm.t
ums.
ac.ir
J
anua
ry,
2017
78
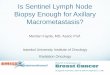
CASE REPORT We present a 27 years old male with a chief complaint of a mole in the lower back region, the lesion showed alteration in the size and color during last 6 month. Excisional biopsy was performed in a day care clinic and patient was referred to us because of malignant melanoma pathology report with maximum tumor depth of 2.5 millimeter. The surgical plan was complete excision of the lesion with sentinel lymph node (SLN) biopsy. Four peritumoral intradermal doses of 0.3 mCi Tc-99m phytate was injected with 10 millimeter distance from previous resection scar and whole body scan was performed 60 minutes later. The lymphoscintigraphy (Figure 1) showed lymphatic drainage to the both axillary and right inguinal regions. Fig 1. Anterior whole body image (lymphoscintigraphy) after 4 peritumoral intradermal injection of 0.3 mCi Tc-99m phytate around previous resection scar. Two SLNs are noted in the right axillary (black arrow), one SLN in the left axillary (arrow) and one SLN in right inguinal regions (arrow head) next to the urinary bladder.
The sentinel lymph nodes were marked on the patient's skin and he was immediately referred to the operating room for SLN biopsy. Only the right axillary SLN was positive on pathologic examination, and right axillary lymph node dissection was performed 6 days later (3 out of 14 dissected node were metastatic), while no additional surgical procedure was done in the left axillary and right inguinal region. Subsequently the patient noted a mass in right axillary region three months later. On physical examination, possible recurrence was suspected, ultrasonic evaluation showed a large hyperemic mass in the right axilla with infiltrating borders. Inguinal regions and left axilla were unremarkable. Bone scan, brain MRI, chest and abdominal CT scan were carried out for metastasis work up. CT showed a 10 centimeter enhancing mass of the right axilla with central necrosis, lungs, liver and other organs appeared normal; brain MRI and bone scan were negative. Tc-99m alpha MSH scan was then performed for the patient after obtaining an informed consent. Briefly, 30, 120 and 240 minutes after IV injection of 25 mCi Tc-99m alpha-MSH, both whole body scan and SPECT images were obtained. The scan showed right axillar mass with central area of significant decreased activity corresponding to necrosis noted on CT images (Figure 2). Mild to moderate tracer uptake noted in the thoracolumbar region (primary tumor resection scar), left axilla and right inguinal region (SLNs biopsy) and interpreted as tracer uptake in healing wound. Surgical resection of the right axillary nodes was done the next day and pathologic report showed multiple conglomerated metastatic lymph nodes. There is no sign of recurrence in the right axilla or any other body site by the publication day of this article.
DISCUSSION Alpha-MSH is a 13 amino acid polypeptide which binds to melanocortin receptor 1 (MCR1). MCR1 is expressed on melanocytes as well as malignant melanoma tumoral cells; the expression makes radiolabeled alpha-MSH scanning feasible in these patients [1-3]. Lymphoscintigraphy is the method of choice for evaluation of the lymphatic drainage pathway in breast cancer and trunk melanoma and SLN biopsy is the standard of care in melanomas greater than 1 mm thick without macroscopic regional lymph node involvement [4]. Blue dye SLN biopsy for trunk melanoma is not recommended because of unpredictable lymphatic drainage and usually multiple drainage routs, therefore radiocolloid injection and lymphoscintigraphy is preferred for these patients [5, 6].

Sentinel lymph node biopsy in multiple drainage basins Farzanefar et al.
Iran
J N
ucl M
ed 2
017,
Vol
25,
No
1 (S
eria
l No
47)
h
ttp:
//irj
nm.t
ums.
ac.ir
J
anua
ry,
2017
79
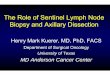
Fig 2. Whole body and SPECT images 4 hour after IV injection of 25 mCi Tc-99m alpha-MSH. The scan showed an area of increased activity in right axilla with central area of significant decreased activity best visualized on SPECT images (arrows), corresponding to necrosis noted on CT images.
Recently SPECT-CT method had been introduced for better SLN detection [7]. Multiple lymphatic basin drainage illustrated by lymphoscintigraphy is a common scenario in the trunk melanoma, but it is not an independent factor for worsening the prognosis [8]. Approaching this problem is a big challenge for both the patient and the surgeon; usually SLN biopsy of all lymphatic drainage routs provides the minimal invasion. A retrospective multicenter study performed by Ribero evaluates the prognostic implication of this method [9] and showed better prognosis in the patients with negative SLN when two or more lymphatic basin were evaluated. Regional lymph node involvement and also number of metastatic lymph nodes have a prognostic implication [10, 11]. Disease free survival and overall survival depended on the tumor loco-regional status. SLN biopsy is a diagnostic and prognostic tool in this clinical setting. This study showed the value of lymphoscintigraphy for evaluating tumor lymphatic drainage; on the other hand, local recurrence after therapeutic lymph node dissection in the same region of positive SLN among one out of three tumor drainage site confirms the prognostic value of SLN biopsy for regional lymph node recurrence, while the remaining two sites with initial negative lymph nodes did not show recurrence on follow up. There is concern about change in lymphatic flow after regional SLN biopsy or lymph node dissection. However, recently Yokota et al. suggest intact lymphatic flow after SLN biopsy, evaluated by near-infrared imaging in 41 patients [12]. In our case, persistent same location relapse also demonstrate similar result following SLN biopsy and lymphatic basin nodal dissection.
CONCLUSION Multiple drainage basins in the trunk melanoma is common, in this clinical setting lymphoscintigraphy is preferred to blue die injection. SLN biopsy of all drainage basins is mandatory; this approach is the optimal therapeutic method for regional tumor management and also provides prognostic information for further patient follow up.
REFERENCES 1. Shamshirian D, Erfani M, Beiki D, Hajiramazanali M,
Fallahi B. A 99mTc-tricine-HYNIC-labeled peptide targeting the melanocortin-1 receptor for melanoma imaging. Iran J Pharm Res. 2016;15(3):349-360.
2. Shamshirian D, Erfani M, Beiki D, Fallahi B, Shafiei M. Development of a 99mTc-labeled lactam bridge-cyclized alpha-MSH derivative peptide as a possible single photon imaging agent for melanoma tumors. Ann Nucl Med. 2015;29:709-720.
3. Lee S, Xie J, Chen X. Peptides and peptide hormones for molecular imaging and disease diagnosis. Chem Rev. 2010 May 12;110(5):3087-111.
4. Mariani G, Erba P, Manca G, Villa G, Gipponi M, Boni G, Buffoni F, Suriano S, Castagnola F, Bartolomei M, Strauss HW. Radioguided sentinel lymph node biopsy in patients with malignant cutaneous melanoma: the nuclear medicine contribution. J Surg Oncol. 2004 Mar;85(3):141-51.
5. Caprio MG, Carbone G, Bracigliano A, Acampa W, Mainolfi C, Molea G, Salvatore M. Sentinel lymph node detection by lymphoscintigraphy in malignant melanoma. Tumori. 2002 May-Jun;88(3):S43-5.
6. Callender GG, Egger ME, Burton AL, Scoggins CR, Ross MI, Stromberg AJ, Hagendoorn L, Martin RC 2nd, McMasters KM. Prognostic implications of anatomic location of primary cutaneous melanoma of 1 mm or thicker. Am J Surg. 2011 Dec;202(6):659-64; discussion 664-5.

Sentinel lymph node biopsy in multiple drainage basins Farzanefar et al.
Iran
J N
ucl M
ed 2
017,
Vol
25,
No
1 (S
eria
l No
47)
h
ttp:
//irj
nm.t
ums.
ac.ir
J
anua
ry,
2017
80
7. Stoffels I, Müller M, Geisel MH, Leyh J, Pöppel T, Schadendorf D, Klode J. Cost-effectiveness of preoperative SPECT/CT combined with lymphoscintigraphy vs. lymphoscintigraphy for sentinel lymph node excision in patients with cutaneous malignant melanoma. Eur J Nucl Med Mol Imaging. 2014 Sep;41(9):1723-31.
8. McHugh JB, Su L, Griffith KA, Schwartz JL, Wong SL, Cimmino V, Chang AE, Johnson TM, Sabel MS. Significance of multiple lymphatic basin drainage in truncal melanoma patients undergoing sentinel lymph node biopsy. Ann Surg Oncol. 2006 Sep;13(9):1216-23.
9. Ribero S, Osella-Abate S, Pasquali S, Rossi CR, Borgognoni L, Piazzalunga D, Solari N, Schiavon M, Brandani P, Ansaloni L, Ponte E, Silan F, Sommariva A, Bellucci F, Macripò G, Quaglino P Prognostic role of multiple lymphatic basin drainage in sentinel lymph node-negative trunk melanoma patients: A multicenter study from the Italian Melanoma Intergroup. Ann Surg Oncol. 2016 May;23(5):1708-15.
10. Kim J, Sun Z, Gulack BC, Adam MA, Mosca PJ, Rice HE, Tracy ET. Sentinel lymph node biopsy is a prognostic measure in pediatric melanoma. J Pediatr Surg. 2016 Jun;51(6):986-90.
11. Sandro P, Andrea M, Nicola M, Simone M, Giuseppe M, Lorenzo B, Nicola S, Dario P, Luigi M, Giuseppe G, Roberto P, Corrado C, Simone R, Ugo M, Mario S, Riccardo RC. Lymph-Node Ratio in Patients with Cutaneous Melanoma: A Multi-Institution Prognostic Study. Ann Surg Oncol. 2015 Jul;22(7):2127-34.
12. Yokota K, Sawada M, Matsumoto T, Hasegawa Y, Kono M, Akiyama M. Lymphatic flow is mostly preserved after sentinel lymph node biopsy in primary cutaneous malignant melanoma. J Dermatol Sci. 2015 May;78(2):101-7.