Embed Size (px)
Citation preview
Sentinel Node Biopsy Surgical Tech
Asma DahirP.g 496
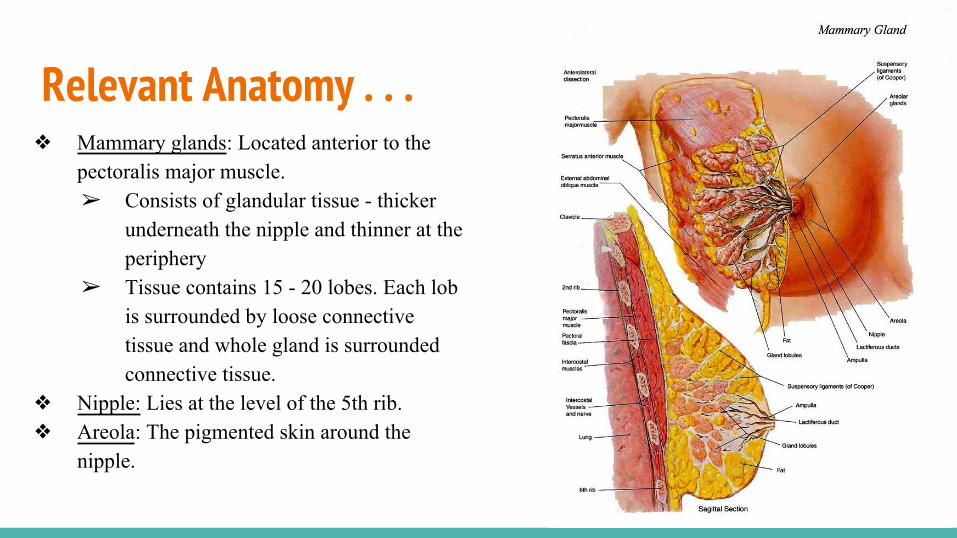
Relevant Anatomy . . .❖ Mammary glands: Located anterior to the
pectoralis major muscle. ➢ Consists of glandular tissue - thicker
underneath the nipple and thinner at the periphery
➢ Tissue contains 15 - 20 lobes. Each lob is surrounded by loose connective tissue and whole gland is surrounded connective tissue.
❖ Nipple: Lies at the level of the 5th rib.❖ Areola: The pigmented skin around the
nipple.
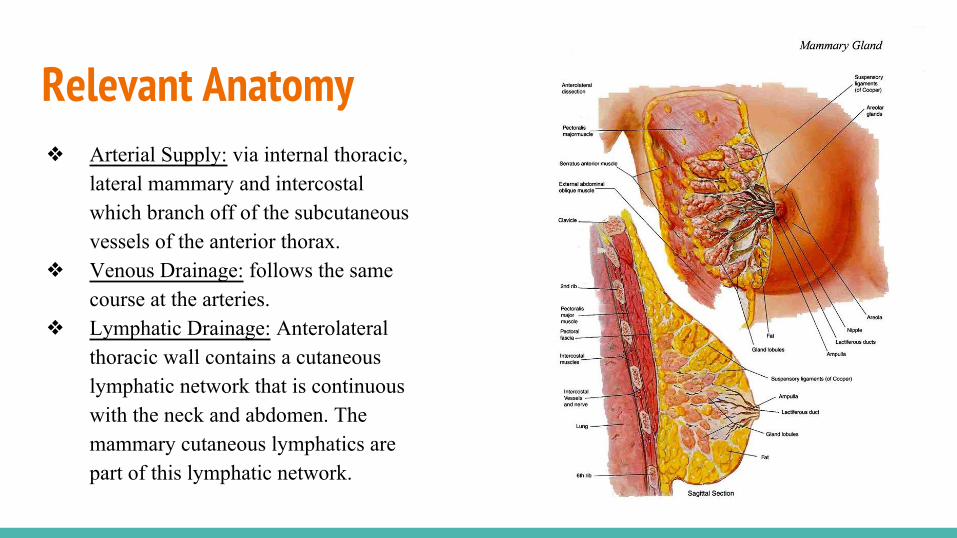
Relevant Anatomy ❖ Arterial Supply: via internal thoracic,
lateral mammary and intercostal which branch off of the subcutaneous vessels of the anterior thorax.
❖ Venous Drainage: follows the same course at the arteries.
❖ Lymphatic Drainage: Anterolateral thoracic wall contains a cutaneous lymphatic network that is continuous with the neck and abdomen. The mammary cutaneous lymphatics are part of this lymphatic network.
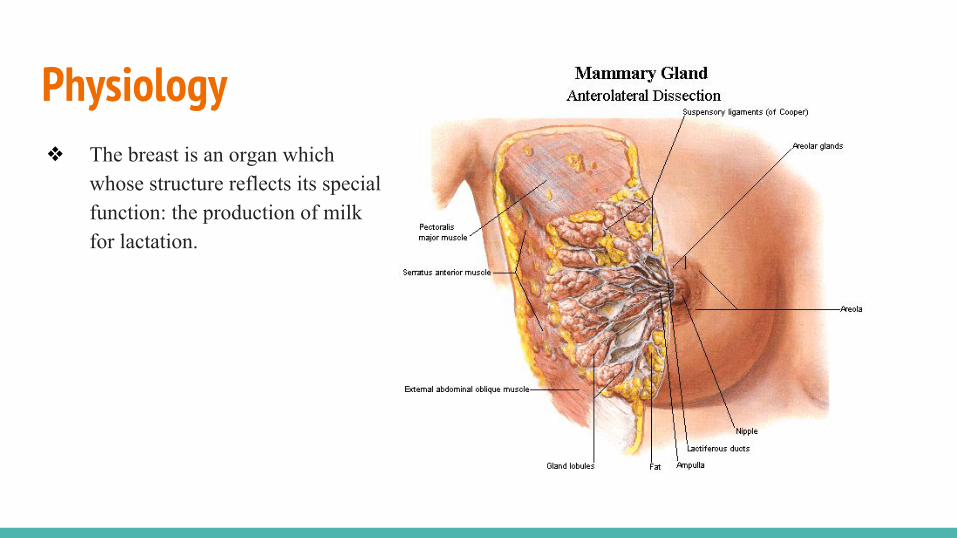
Physiology ❖ The breast is an organ which
whose structure reflects its special function: the production of milk for lactation.

Pathophysiology - TEST QUESTION❖ A sentinel lymph node is defined
as the first lymph node to which cancer cells are most likely to spread from a primary tumor. Sometimes, there can be more than one sentinel lymph node.

Diagnostic Exams❖ Breast examination: palpation of the
breasts ❖ Mammography❖ Breast Biopsy is a diagnostic procedure

Surgical Intervention ❖ A Sentinel Node Biopsy is a procedure in which the sentinel lymph node is identified, removed
and examined to determine whether cancer cells are present.

Supplies❖ Isosulfan blue dye❖ Local Anesthesia ❖ 5- mL syringe❖ 25- gauge needle❖ Blades (2) #15 and (1) #10 if
specimen is likely to be large❖ Electrosurgical pencil and cord❖ Multiple specimen containers with
several pathology request forms ❖ Crash cart immediately available
*(P.T may be allergic reaction to the dye)

Instrument and Equipment Instrument:❖ Minor instrument Set
Equipment:❖ Electric Surgical Unit

Surgical Considerations ❖ Patient may be allergic to isosulfan blue
dye

Anesthesia ❖ Local Anesthesia

Positioning ❖ Patient is supine with the arms on the
affected side extended on a padded armboard, the other arm may be padded and tucked in at the patient’s side using the draw sheet.
❖ Antiembolitic hose may be put on the legs ➢ particularly if a long procedure is
anticipated

Positioning continued ❖ A pillow may be placed:
➢ under the patient's head ➢ Additional small padding placed under the lumbar spine➢ An extra pillow may be placed under the knees to avoid straining back muscles.➢ These are placed to prevent pressure damage to a tissue and for comfort.

Skin prep❖ A gentle circular motion beginning at
the site of the incision and extending from the neckline to lower ribs, including a wide margin beyond the midline and under the arm, down to the table on the affected side.
❖ Scrub is performed with a “gentle touch,” as cancer cells may be dislodged from the specimen into the bloodstream if vigorous scrubbing were done.
Draping ❖ Four folded towels ❖ Laparotomy sheet
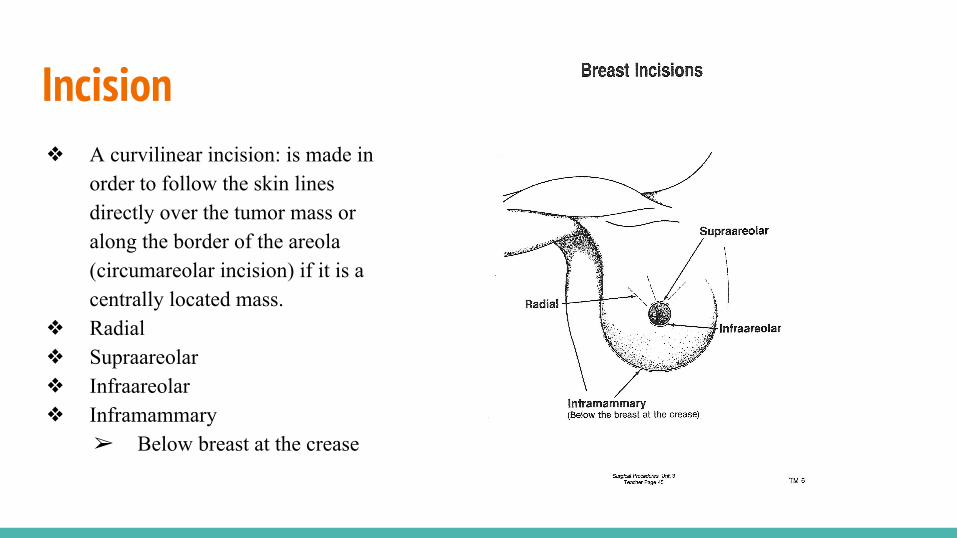
Incision ❖ A curvilinear incision: is made in
order to follow the skin lines directly over the tumor mass or along the border of the areola (circumareolar incision) if it is a centrally located mass.
❖ Radial ❖ Supraareolar❖ Infraareolar ❖ Inframammary
➢ Below breast at the crease
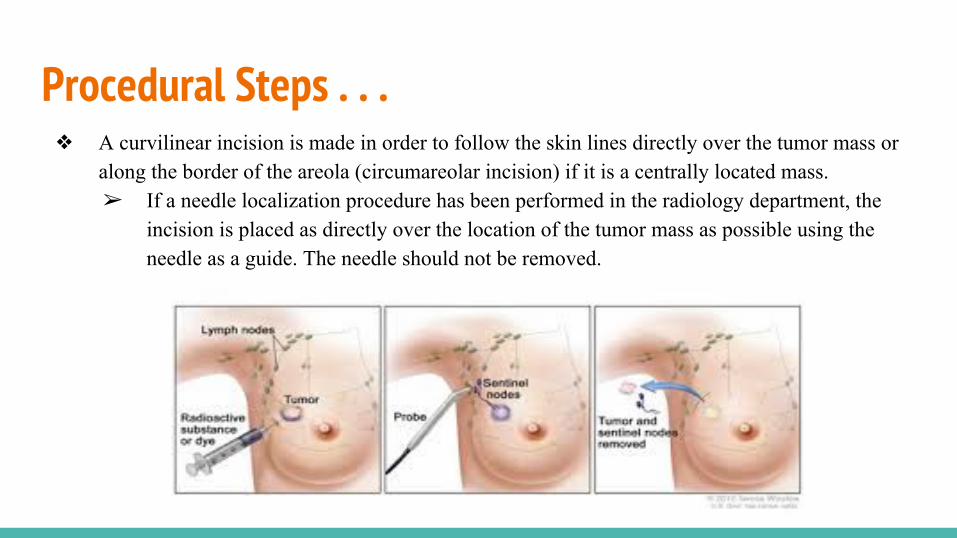
Procedural Steps . . .❖ A curvilinear incision is made in order to follow the skin lines directly over the tumor mass or
along the border of the areola (circumareolar incision) if it is a centrally located mass. ➢ If a needle localization procedure has been performed in the radiology department, the
incision is placed as directly over the location of the tumor mass as possible using the needle as a guide. The needle should not be removed.
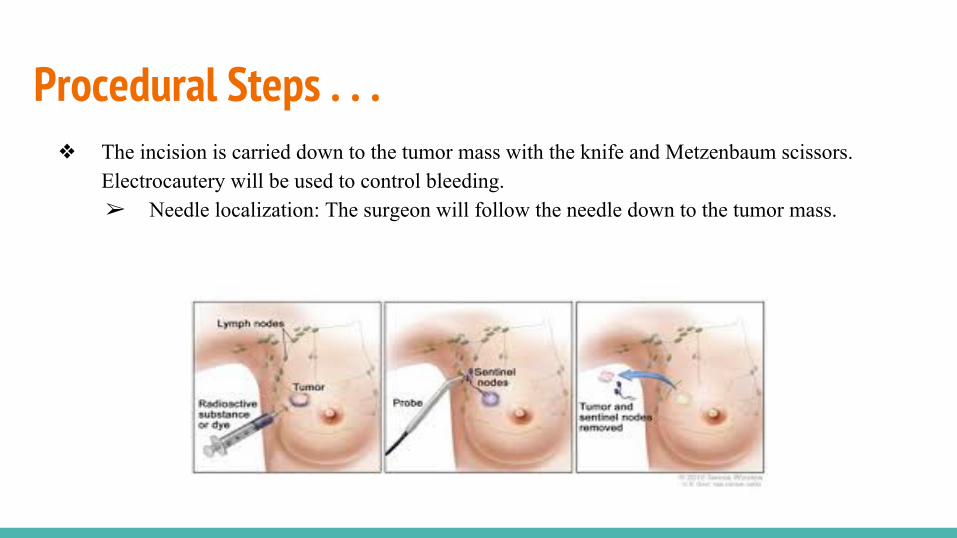
Procedural Steps . . . ❖ The incision is carried down to the tumor mass with the knife and Metzenbaum scissors.
Electrocautery will be used to control bleeding.➢ Needle localization: The surgeon will follow the needle down to the tumor mass.
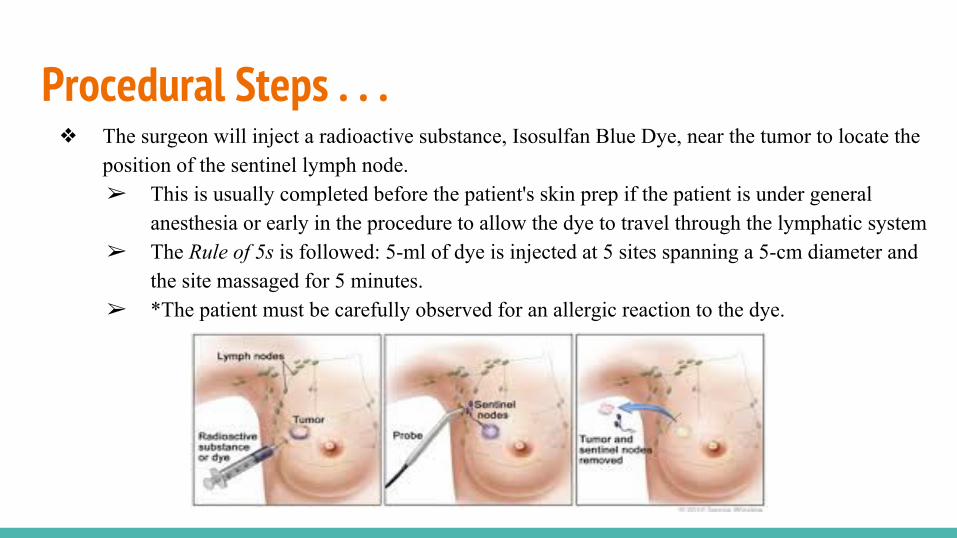
Procedural Steps . . .❖ The surgeon will inject a radioactive substance, Isosulfan Blue Dye, near the tumor to locate the
position of the sentinel lymph node. ➢ This is usually completed before the patient's skin prep if the patient is under general
anesthesia or early in the procedure to allow the dye to travel through the lymphatic system ➢ The Rule of 5s is followed: 5-ml of dye is injected at 5 sites spanning a 5-cm diameter and
the site massaged for 5 minutes.➢ *The patient must be carefully observed for an allergic reaction to the dye.

Procedural Steps . . .❖ The surgeon then uses a device, gamma detector, that detects the radioactivity to find the sentinel
node or looks for lymph nodes that are stained with the blue dye.❖ Once the sentinel lymph node is located, the surgeon makes a small incision (about ½ inch) in
the overlying skin and removes the node.

Procedural Steps ❖ The sentinel node is then checked for the presence of cancer cells by the pathologist. If cancer is
found, the surgeon may remove additional lymph nodes, either during the same biopsy procedure or during a follow-up surgical procedure.➢ The surgeon may want each node placed in a separate specimen container and numbered
each with its own pathology request form.
Specimen Care❖ The sentinel node is then checked for
the presence of cancer cells by the pathologist. If cancer is found, the surgeon may remove additional lymph nodes, either during the same biopsy procedure or during a follow-up surgical procedure.➢ The surgeon may want each
node placed in a separate specimen container and numbered each with its own pathology request form.
Prognosis ❖ Based on extent of surgical that
was performed.
Complications ❖ Complications from sentinel node biopsy
include:➢ Allergic reaction to the dye➢ Sensory nerve damage (rare)➢ Motor nerve damage (rare)➢ Pneumothorax that occurs with
internal mammary node biopsy➢ Dealth

Wound Class / Management ❖ Class 1: Clean
Work Cited❖ Goldman, Maxine A. Pocket guide to the operating room. Philadelphia: F.A. Davis Co, 2008.
Print.❖ "Sentinel Lymph Node Biopsy." National Cancer Institute. N.p., n.d. Web. 24 Feb. 2017.
❖ Frey, Kevin B., and Tracey Ross. Surgical technology for the surgical technologist: a positive care approach. Boston, MA: Cengage Learning, 2016. Print.
❖ "Anatomy and Physiology of the Breast." Anatomy and Physiology of the Breast. N.p., n.d. Web. 01 Mar. 2017.