Embed Size (px)
Citation preview

HEARTBEATA Publication of South Jersey Heart Group
September 2017
Statin-associated muscle symptoms (SAMS) are a
commonly reported problem in patients who use or
start to use statins. This Heartbeat will provide a guide
for clinicians by detailing a structured approach that is
based on published data as well as expert opinion.
Statin Benefits: The cardiovascular (CV) benefits
of statins are backed by a vast database, and statins
have a favorable benefit/risk profile. Treatment with
moderate- and high-intensity statins reduces the
risk of CVD in the setting of high-risk primary and
secondary prevention.1,2 For every 18mg/dl reduction
in low-density lipoprotein-cholesterol (LDL-C), CVD
events are reduced by 21% after one year of treatment
with moderate- or high-intensity statins.3 The reduction
in ASCVD increases with long-term statin use.4
Problem: However, many patients taking statins
report SAMS that prevent the use of guideline-
recommended doses, even though randomized clinical
trials (RCTs) indicate that statins have a side-effect
profile almost indistinguishable from placebo or
comparative drugs, particularly when used in low
dosages.5 But “real world” data obtained from
surveys, registries and insurance claims suggest
that side effects of statins are common, especially
at higher doses.6 Many patients are unwilling to
continue with guideline-recommended statin doses
after experiencing side effects.7
Consequences: Patients who stop statins have a higher risk for recurrent myocardial infarction andstroke.8 This in turn leads to higher healthcare costs.9
The Challenge of SAMS: What makes this amore difficult problem is the overriding “nocebo
effect.” Muscle symptoms are common in the middle-aged population taking statins. The difference between the muscle symptom data from observationalstudies and data from RCTs is due to the nocebo effect. The nocebo effect—opposite of placebo—(Latin for “I do harm”) explains why some patients misattribute symptoms to their exposure to statins. Inthe context of SAMS (without significantly elevatedcreatine phosphokinase [CK] muscle enzyme) or otheradverse events, the nocebo effect is strengthened by exaggerated reports readily available online about thedangers of taking statins and by warnings appropriatelycommunicated by physicians and patient informationleaflets about myopathy/rhabdomyolysis.
Managing Statin Intolerance

In some cases, the patient becomes more conscious of background aches and pains when learning aboutthe adverse effects of statins; in other cases, newmuscle symptoms arise. Because a placebo-controlledrechallenge is not possible in the clinic, the return of symptoms upon rechallenge with the same or a different statin may well also be a nocebo effect.
Plan: Techniques to minimize the nocebo effect inpatients starting statins may help prevent statin intolerance. We should:
• Avoid communications that create negative expectations about statins.
• Emphasize the benefits of statins in reducing CV disease and indicate that serious muscle side effects are very unlikely and are easily detected with a blood test (CK).
• Remind patients that muscle aches and pains are common in middle age and older, and usually are due to other causes.
Management of SAMS
Whatever the etiology, these muscle symptoms are real to the
patient and must be carefully addressed by the physician in
order to keep the patient on a statin.
An excellent expert opinion piece from this month’s
JACC presenting a clinical approach is summarized
in the illustration below.10
How can we diagnose SAMS? Statin discontinuation
and rechallenge is the primary strategy for confirming
the presence of statin intolerance secondary to SAMS.
SAMS Unlikely:1. Symptoms start immediately after initiation
and/or resolve within minutes to hours upon cessation
2. Symptoms that do not improve or disappear within 12 weeks after statin discontinuation (four weeks often enough)
3. Symptom onset that is present after protracted use (>12 weeks) without changes in any other apparent patient status
4. Symptoms that occur with other classes of lipid-lowering agents
Asymmetric, intermittent or non-specific symptoms
to a particular area also make SAMS less likely.
Treatment of SAMSWe need to:
(a) Be convinced of the benefits of statins to convince
the patient to take one
(b) Listen to the patient when he/she reports symptoms,
assess severity of muscle symptoms and individualize
treatment accordingly. If the patient’s symptoms do
not interfere with activities of daily living and/or
post-exercise symptoms generally abate with rest and
occasional acetaminophen, I encourage the patient to
hang in there, and emphasize how important the statin
is to preventing heart attacks and strokes. When a
patient tells me his/her symptoms are unbearable, I’m
concerned about rhabdomyolysis and immediately stop
the statin if the patient hasn’t already done so, and use
the laboratory to further evaluate the patient.
(c) Educate the patient regarding benefits of a statin
(d) Let the patient decide (buy in) among several
recommended approaches:
1. Lower the dose.
2. Change the dose to every other day with high-
dose atorvastatin or rosuvastatin in our highest-
risk patients (both have long half-lives and are as
efficacious as daily dosing in reducing LDL-C,
though efficacy on ASCVD outcomes has not been
established).
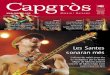
CENTRAL ILLUSTRATION Clinical Approach to Patient With SAMS
After symptom resolution, initiate:Same dose of same statin
(low likelihood that SAMS will reoccur)or
Alternative high-intensity statin
Promote a healthy lifestyle If still high SAMS-CI score, initiate:
Consider non-statin LDL-C lowering therapy
Promote a healthy lifestyle
Clinical assessment: Statin-Associated Muscle Symptom Clinical Index (SAMS-CI)
Patient with suspected statin-associated muscle symptoms (SAMS)
High SAMS-CI scoreLow SAMS-CI score
Before establishing a diagnosis of statin intolerance:Review drug-drug interactions and co-morbidities
Check for hypothyroidism and vitamin D
Statin discontinuation
Readminister SAMS-CI
After symptom resolution, initiate:Lower dose of same statin
orAlternative high-intensity statin
Statin discontinuation
Evaluate for:
HDepression and anxiety
Rosenson, R.S. et al. J Am Coll Cardiol. 2017;70(10):1290–301.

3. Try pitavastatin or pravastatin, which have
less toxic effects because of different pharmokinetic
properties.
4. Discontinue and rechallenge.
All of these have been shown to improve patient adherence to
treatment in medical practice. Our favorite among those most
refractory is rosuvastatin one to three times per week.
Lifestyle Therapeutic lifestyle changes (TLC) should be considered
first-line therapy for lowering LDL-C and reducing CVD
risk. Several non-pharmacological approaches are
effective in lowering LDL-C and CVD risk, including
consumption of a heart-healthy diet, maintaining a
normal weight, avoidance of tobacco products and
regular exercise. TLC is particularly important for
patients with SAMS who cannot tolerate statin therapy.
Beyond statin rechallenge, working with patients to
help them achieve a healthy lifestyle is an essential
component of treating those with SAMS.
Non-Statin TherapiesConsideration should be given to adding non-statin
agents to prevent ASCVD events among patients
unable to tolerate statin therapy or able to tolerate
only low doses or intermittent dosing. Our first choice
is ezetimibe, usually well tolerated and generally
lowering LDL-C by 15% to 25%, as an add-on to
attempt to get your patient to acceptable LDL-C levels.
A PCSK9 inhibitor should be considered to lower LDL-C
in high-risk patients who cannot tolerate any statin.
Bile acid sequestrants, fenofibrates and niacin may
also be considered, but efficacy on ASCVD outcomes
is not convincing.
ConclusionsSAMS are the most common cause for statin
discontinuation or dose reduction. Most of the muscle
symptoms reported in patients taking statins are not
due to a statin-induced myopathy and can be overcome
with an individualized approach to management. We
should avoid statin discontinuation, which results in
increased ASCVD risk, especially in high-risk patients.
Mario L Maiese, DO, FACC, FACOI
Clinical Associate Professor of Medicine, Rowan SOM
Email: [email protected]
Sign up to receiveHeartbeats online: www.sjhg.org
Heartbeat is a South Jersey Heart Group publication.
When a patient presents with SAMS, we should verify
that the patient truly cannot tolerate statin therapy.
These efforts involve evaluation of symptoms after
drug withdrawal and assessment of symptoms upon
re-initiation with an alternative statin or lower doses
of the same or a different statin.
CorrectionLast month’s Heartbeat, “Heart of a Woman,” was based
on a study from JACC called “Knowledge, Attitudes
and Beliefs Regarding CVD.” In the study, the authors
reported that heart disease in women was a top
concern for only 39% of primary care doctors. After
publication, the study authors issued a correction. In
fact, 76% of doctors gave heart disease a concern score
of 4 or 5 on a scale of 1 to 5, with 5 being
“extremely concerned.”

1600 Haddon AvenueCamden, NJ 08103
Our Lady of LourdesMedical Center
NON-PROFIT ORGU.S. POSTAGE
PAIDPERMIT #36BELLMAWR
NJ 08031
References
1 Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol July 2014; 63 (Pt B): 2889–2934.
2 Catapano AL, Graham I, De Backer G, et al. ESC/EAS guidelines for the management of dyslipidaemias: the Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Atherosclerosis October 2016; 253: 281–344.
3 Baigent C, Keech A, Kearney PM, et al. Cholesterol Treatment Trialists' (CTT) Collaborators Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet October 2005; 366: 1267–1278.
4 McConnachie A, Walker A, Robertson M, et al. Long-term impact on healthcare resource utilization of statin treatment, and its cost effectiveness in the primary prevention of cardiovascular disease: a record linkage study. Eur Heart J February 2014; 35: 290–298.
5 Gupta A, Thompson D, Whitehouse A, et al. Adverse events associated with unblinded, but not with blinded, statin therapy in the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid Lowering Arm (ASCOT-LLA): a randomised double-blind placebo-controlled trial and its non-randomized non-blind extension phase. Lancet 2017; 389: 2473–2481.
6 Bruckert E, Hayem G, Dejager S, Yau C, Bégaud B. Mild to moderate muscular symptoms with high-dosage statin therapy in hyperlipidemic patients–the PRIMO study. Cardiovasc Drugs Ther 2005; 19: 403–414.
7 Colantonio LD, Huang L, Monda KL, et al. Adherence to high intensity statins following a myocardial infarction hospitalization among Medicare beneficiaries. JAMA Cardiol, [E-pub ahead of print]. 2017 Apr 19.
8 Colantonio LD, Kent ST, Huang L, et al. Algorithms to identify statin intolerance in Medicare administrative claim data. Cardiovasc Drugs Ther 2016; 30: 525–533.
9 Graham JH, Sanches RJ, Sassen JJ, Mallya UG, Panaccio MP, Evans MA. Clinical and economic consequences of statin intolerance in the United States: results from an integrated health system. J Clin Lipidol 2017; 11:70–79.
10 Rosenson RS, et al. Optimizing cholesterol treatment in patients with muscle complaints. J Am Coll Cardiol September 5 2017; 70: 1290-1301.