Embed Size (px)
Citation preview

S Y M P O S I U M : P E D I A T R I C I N T E N S I V E C A R E - I I
Indian J Pediatr 1993; 60 : 367-379
Septic Shock : Pathogenesis and Treatment
Leticia Castillo and Melchor Sanchez*
Pediatric and Neonatal Intensive Care Units, Children's Service, Massachusetts General Hospital Boston, U.S.A. and *Department of Pediatrics, Harvard Medical School
Massachusetts General Hospital Boston, U.S.A.
Abstract, Septic shock is the host's inflammatory response to infection. There are multiple en- dogenous mediators responsible for the pathogenesis of septic shock. Cytokines, nitric oxide and prostaglandins are some of the major mediators. The term sepsis syndrome allows for an earlier diagnosis and treatment. Management of septic shock is focused in maintaining heine- dynamic stability and an adequate oxygen delivery and utilization. Careful attention to each organ-system is of paramount importance to prevent complications and improve outcome. Experimental therapies to modulate the inflammatory response are promising. (Indian J Pedlatr 1993; 60 : 367-379 )
Keyworda : Septic shock; Sepsis syndrome; Critical~, ill.
S eptic shock is a complex syndrome that has become increasingly impor-
tant as a cause of morbidity and mortal- ity in the Intensive Care Unit? Sepsis is the host's inflammatory response to in- fection and it is a continuous progression from a localized infection without sys- temic manifestations such as otitis media or gastroenteritis, to an infection with systemic manifestations such as fever, tachycarrdia, leukocytosis, chills and bacteremia; to an infection with systemic manifestations and hemodynamic insta- bility such as hypotension, poor perfu- sion and cardiorrespiratory arrest. Septic shock is the final stage of the dynamic Process of sepsis. 2
In order to identify a population of Patients at risk for developing sepsis
Reprint requests : Dr. Leticia Castillo, Pediat- tic and Neonatal Intensive Care Unit, Ellison 317, Massachusetts General Hospital, Boston, MA 02114, U.S.A.
early, the term Clinical Sepsis Syndrome was first used by Bone in 1987. 3 Sixty- four percent of 191 patients identified with this criteria subsequently devel- oped shock, and only 45% of the patients had a positive blood culture. Clinical Sepsis Syndrome relies on clinical crite- ria to facilitate diagnosis of sepsis; such as a high suspicion of infection, (confir- mation by blood culture is not required), fever, tachypnea, tachycardia and im- paired organ system function as indi- cated by oliguria, abnormal mentation, hypoxemia or increased plasma lactate. When we apply this concept to the pedi- atric population, a large proportion of our patients, many with uncomplicated viral infections may meet the sepsis syn- drome criteria without necessarily pro- gressing towards septic shock. This deft- nition is significant, however, because it is an effective warning to carefully as- sess, treat and follow patients at risk for

368 THE INDIAN JOURNAL OF PEDIATRICS 1993; Vol. 60. No. 3
TASLE 1. Clinical Sepsis S y n d r o m e in Children
Fever Bounding pulses
Irritability Oliguria
Tachycardia Capillary refill > 3 sec
Flushed, warm skin
developing septic shock. The mortality for those patients who will progress to shock is about 60 to 90%, 4~ despite cur- rent antibiotic therapy and sophisticated techniques of file support. Under these circumstances the early diagnosis and aggressive management of septic pa- tients is of utmost importance in the out- come of septic shock, s Table 1 shows the characteristics of sepsis syndrome in children.
PATHOGENESIS
Traditionally, it has been believed that septic shock occurs as the result of re- leased lipopolysaccharide (LPS) by gram negative bacteria; nonetheless, exotoxin from gram positive bacteria, and fungal and viral products are able to produce the same clinical picture. 67 It is now known that these bacterial, viral and fun- gal products possess no profound toxic- ity of their own, but rather, they elicit the production of highly toxic endogenous mediators by the host. s01~ LPS for in- stance, activates leukocytes, macroph- ages, endothelial cells, and possibly other cells. The activated leukocytes re- lease peptides known as cytokines. These cytokines, particularly tumor ne- crosis factor (TNF)2and interleuikin-1 (IL-1) are responsible for the physiologic changes observed in septic shock. ~u2 TNF and IL-1 elicit the release of nitric
oxide (NO), an oxygen radical product of arginine metabolism synthesized by macrophages, neutrophils, central nerv- ous system (CNS) cells, and endothelial cells. NO is a signal transducer, it has cy- totoxic activity, and is a potent en- dogenous vasodilator responsible for the hypotension observed in septic shock. 13,~4 TNF induces fever, lactic acidosis, hypo- tension and suppresses lipoprotein li- pase resulting in hypertryglyceridemia. If TNF is administered in sublethal doses, it induces fever, anorexia, cachexia, anemia, and leukocytosis. 11,~s IL-1 also has widespread systemic ef- fects. 16.17 At the CNS level it induces leth- argy, release of ACTH, neuropeptides and decreases appetite. IL-1 has pro- found metabolic effects; it increases the synthesis of acute phase reactant pro- teins such as C reactive protein and fi- brinogen, and decreases the synthesis of structural proteins mainly albumin and transferrin; a fragment of IL-1 known as proteinolysis inducing factor is respon- sible for the protein breakdown ob- served in septic patients, also known as septic autocannibalism. IL-1 elicits the release of glucagon, catecholamines, and other counteregulatory hormones result- ing in hyperglycemia? 7 The vascular ef- fects of IL-1 are of great significance in septic shock; it increases leukocyte ad- herence, degranulation, and release of proteases and free radicals. These ele- ments will cause lipid peroxidation of the phospholipid layer in the cellular membrances, resulting in widespread tissue and organ injury, is During this process both pathways of arachidoniC acid metabolism also become activated. The lipooxygenase pathway results in the production of leukotrienes, which

1993; Vol. 60. No. 3
induce enhanced capillary permeability, vasoconstriction, bronchoconstriction, and leukocyte aggregation. Activation of the cyclooxygenase pathway leads to production of prostaglandin (PG) and thromboxane. Some prostaglandins such as PGE and PGI or prostacyclin are syn- thesized primarily by vascular endothe- lium and induce vasodilation and inhibit platelet aggregation. Thromboxane is mainly produced by platelets and results in vosoconstriction and platelet aggrega- tion. 19 The main pathophysiologic events
THE INDIAN JOURNAL OF PEDIATRICS 369
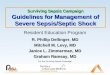
of septic shock are summarized in Figure 1.
There are many other mediators of the inflammatory process of sepsis such as platelet activating factor, fibronectin, complement, proteases, and endogenous opioids (Table 2). It is likely that some others have not been discovered yet. Hence, the pathogenesis of sepsis is multifactorial and once the inflamma- tory cascade is activated, no single "magic bullet" will prevent it from pro- gressing, thus, a wide comprehensive
ACTIVATION �9 Bradykinines �9 Clotting Factors �9 Plasmin �9 Complement
,( Release of Proteases
Vascular Leakage
\ Tissue lniury
INFECTION
LPS, TSST-1, etc. , ---.. MACROPHAGES ENDOTHELIAL CELLS
CYTOKINs Nitric Oxide �9 / \ �9 IL-1 - IL-6
Cytotoxicity Vasodilation
PMN
~ ~ - ~ " ~ " ~ Release of Release Oxygen Radicals
,t Lipid Peroxidatiun
1 ORGAN DYSFUNCTION
Arachidonic Acid Metabolites
Lypooxygenase Cyclooxygenase
Leukotrienes Thromboxane, PGI, PGE
Vasoconstriction Platelet Aggregation
Tissue Injury
/
FThe major pathophysiologic events in sepsis are depicted. Endotoxin or exotoxin activa !Land endothelial cells leaaing to release of endogenous mediators and organ dysfunction
or exotoxin activates factors and cells, mainly macrophages
Fig. 1. Pathophysiologic events of septic shock

370 THE INDIAN JOURNAL OF PEDIATRICS
TASLE 2. Mediators of Septic Shock
Cytokines Tumor necrosis factor Interleukins
Eicosanoids Leukotrienes Thromboxane A2 Prostaglandins
Other Platelet activa~g factor Nitric oxide Complement fragments C3a, CSa Toxic oxygen radicals Proteases Fibrin Thrombin Bradykinism Plasminogen activator inhibitors Beta-endorphins Myocardial depressant factor
approach is necessarily aimed to reduce the morbidity and mortality of septic shock.
CLINICAL MANIFESTATIONS
The clinical manifestations of sepsis are widespread, involving multiple organs and systems.
CNS
At the CNS level, sepsis induces a vari- ety of mental changes, coma, seizures, and focal neurologic alterations. The sep- tic encephalopathy may be caused by toxic and metabolic changes, or diffuse impairment of cerebral perfusion. 2~ A severe peripheral neuropathy character- ized by axonal degeneration of motor and sensory nerves is found in 50% of septic patients. The peripheral neuropa- thy contributes to failure to successfully wean patients from the ventilators. 21
1993; Vol. 60. No. 3
Cardiovascular
Sepsis is manifested by hemodynamic instability. Children, however, have re- markable compensatory mechanisms and hypotension is often a late sign. Di- agnosis of septic shock in children should not be based on hypotension, but rather on early hemodynamic changes such as persistent tachycardia, flushed, warm skin, bounding pulses and wide pulse pressure. This has been known as the "early" hyperdynamic or "warm" phase of septic shock, l~oor capillary re- fill, metabolic acidosis and evidence of organ hypoperfusion such as oliguria or lethargy supervene later. Initially cardiac output is increased several fold and the systemic vascular resistance is low. If hypovolemia is not aggressively cor- rected, the patient will progress towards the late, hypodynamic or "cold" phase of septic shock, characterized by hypo- tension and cold "clammy" skin; in this situation the cardiac output is decreased and the systemic vascular resistance is high.
Hypotension is the result of multifac- torial events affecting pre-load (circulat- ing volume) afterload (systemic vascular resistance), and myocardial contractil- ity. 2~ Some mediators such as nitric oxide, leukotrienes, activated comple- ment, prostacyclin, etc. play a role in the vasodilation of sepsisP Down regulation of cz adrenergic receptors resulting in a decrease capacity for vasoconstriction has also been described with sepsis. In addition, despite the initial increase in cardiac output, there is myocardial de- pression manifested by a decreased left ventricular ejection fraction, u Myocar- dial dysfunction is secondary to dov,~

1993; Vol. 60. No. 3 THE INDIAN JOURNAL OF PEDIATRICS 371
2 a o
0 ~0
0- 39-
- o? 06
o5 oc
o3 ~2 oL
20 30 ~'0
b
lO 20 30 40 Oxygen del;ver~ [mt/mlnlkg)
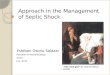
Fig. 2a.Oxygen consumption remains steady, independently of higher or lower oxygen delivery until a critical point; below this point oxygen con- sumption falls. Fi 8 2b. Oxygen ex- traction increases when oxygen deliv- ery falls. (From Schumacker PT, Cain SM. In- tensive Care Med 1987; 13 : 223; with permission).
regulation of I~ receptors. Possibly some ~ mediators such as TNF may be also re- ~
• o , sponsible for the depressed cardiac func-
tion. ~ ~ A controversial hemodynamic event
in septic shock is the development of flow dependent oxygen consumption 0 (VO2).~-~ Oxygen delivery is the product of cardiac output and the arterial oxygen content (DO 2 = CO x CaO2). Cardiac out- Fi 8. 3. put is dependent on preload, afterload, and contractility. Arterial oxygen con- tent is the sum of the oxygen chemically bound by hemoglobin and the oxygen physically dissolved in the plasma; CaO 2 = Hb x 1.34 x SaO~ + PaO 2 x 0.003, where 1.34 is the volume of oxygen (ml) that binds to lg of hemoglobin when it is
fully saturated, 0.003 is the solubility co- efficient of oxygen in human plasma, Hb is hemoglobin concentration and SaO 2 is the percentage o f oxygen saturation. In healthy individuals, the oxygen uptake is independent of oxygen supply. As shown in Figure 2, if DO t is acutely re- duced, oxygen extraction ratio (VO2/ DOt) increases, so the VO 2 can be main- tained. It is only when DO 2 values fall below a critical point (8 ml /kg/min) , that the oxygen extraction capabilities are overwhelmed and VO 2 falls; at this point, lactic acidosis develops. ~
During sepsis, the ability of tissues to extract oxygen is impaired by microvas- cular and cellular abnormalities, and oxygen del ivery is decreased due to myocardial depressant factors a n d / o r abnormal CaO 2 (hypoxemia, anemia, etc.). 26 DO 2 may need to be increased in order to achieve adequate oxygen up-
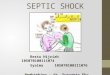
104 | ENDOTOXIN: QO2c= 128 +_ 1 9 ERc=O 54~0 10
s . . . . . . . . . . . . . . . . . . . . . . . . j z
CONTROL: QO2c = 68 -+ I 1 ERe : 078 = 004
i 2~) 4O
SYSTEMtC OXYGEN DELIVERY (mP/min - kg body wt)
Relationship between oxygen delivery and consumption in control animals and after administration of en- dotoxin. In the endotoxin challenged animals the oxgyen requirement is increased, and oxygen extraction is decreased at the critical oxygen deliv- ery. (From Nelson DP, Samsel RW, Wood LDH. J App Physiol. 1988; 64; 2410, with permission)

372 THE INDIAN JOURNAL OF PEDIATRICS
take by the tissues. This is known as an atmormal dependency, of VO~ on DO Z. Figure 3 shows the relationship between VO 2 and DO 2 under physiological condi- tions and after endotoxin administra- tion. ~
Respiratory System
Initially, hyperventilation and respira- tory alkalosis are present during the early stages of septic shock; later, hy- poxemia may develop as a result of pul- monary shunts. Adult respiratory dis- tress syndrome is a dreaded complica- tion of septic shock. Persistent hypoxe- mia, low pressure pulmonary edema, and pulmonary hypertension are impor- tant features of ARDS. ~
Gastrointestinal
There is some degree of liver dysfunc- tion induced by sepsis, Abnormal plasma amino acid patterns character- ized by increased in aromatic amino ac- ids such as phenyhlanine and tyrosine, and decreased branched chain amino ac- ids are seen in later stages of septic shock. 3~ Re-distribution of blood flow may result in gastrointestinal ischemia with translocation of bacteria and/or endotoxin that will set the stage for chronic inflammation and multiorgan failure. 31 Stress ulcers occasionally com- plicate the clinical course of critically ill septic children. Hypoperfusion and oxy- gen radical injury are major factors in the development of stress ulcers, and gastro- intestinal bleeding under these condi- tions. 32
Metabolic
Energy expenditure is greatly increased in septic shock. Oxygen consumption
1993; Vol. 60. No. 3
may be high, normal or low depending on the hemodynamic state. Metabolic acidosis due to excessive production of lactic acid carries a poor prognosis.
Gluconeogenesis is also increased and does not respond to exogenous admini- stration of glucose. There is some degree of insulin resistance and increased prote- olysis that supplies amino acids for glu- coneogenesis, these events frequently lead to glucose intolerance. 33 Hypergly- cemia is an early manifestation of sepsis in infants; hypoglycemia will present in later stages of septic shock, if metabolic support is not provided. Hypertryglyc- eridemia is often present as a result of increased lipolysis.
Septic patients exhibit massive weight loss due to increased protein break- down, which supplies amino acid sub- strate for gluconeogenesis. Nitrogen bal- ance under this circumstances becomes negative. 33
Disseminated Intravascular Coagula- tion (DIC)
DIC is a common manifestation of sepsis and is characterized by coexistent hem- orrhage and microvascular thrombosis. Clinically it presents with persistent gas- trointestinal bleeding, hematuria, bleed- ing at previous puncture sites and mu- cus membrances. If DIC is severe, areas of necrosis may occur. A prolonged prothrombin and partial thromboplastin time (PT, PTr), thrombocytopenia, in- creased fibrin degradation products and microangiopathic hemolytic anemia is frequently found in DIC. u
Renal
Sepsis often manifests with hypoperfu-

1993; Vol. 60. No. 3 THE INDIAN JOURNAL OF PEDIATRICS 373
sion and oliguria, if the hypovolemic state is not promptly corrected, mor- phologic and functional disturbances of the kidneys may occur. Pre-renal disease due to hypovolemia and poor perfusion is the most frequent cause of the renal dysfunction. Activation of mediators and local inflammatory response in the kidneys may lead to tubular necrosis. Drug toxicity such as aminoglycoside antiboifics will contribute to tubulointer- sfifial disease. Decreased urine output to less than 1 m l / k g / h r in children or 30 ml /hr in adolescents should alert the cli- nician. Rising blood urea nitrogen and creafinine, metabolic acidosis, and hy- perkalemia will appear later. Fractional excretion of sodium is less than 1% dur- ing pre-renal states, due to an appropri- ate sodium retention. In the presence of tubular damage, the kidneys fail to re- tain sodium and high urinary sodium excretion results in a fractional excretion greater than 1%. 35
TREATMENT
In view of the multiple pathophysiologic events in septic shock, its treatment must be focused in every organ-system and therefore a broad approach isnecessary. In any critically ill patient, basic prin- ciples of resuscitation (airway, breath- ing, and circulation) are vital in the ini- tial management of these patients. If the patient is diagnosed early and success- fully fluid resuscitated, endotracheal in- tubation and mechanical ventilation may not be necessary. In contrast, if the pa- tient appears to have an increased work of breathing, regardless of normal arte- rial blood gases; or presents with hemo- dynamic instability such as persistent
tachycardia, poor capillary refill, mottled skin or hypotension, endotracheal intu- bation is necessary. 'l-he use of mechani- cal ventilation, sedation and muscle re- laxation will avoid "wasting" cardiac output and oxygen delivery to respira- tory muscles and preventing respiratory arrest. ~s
Endotracheal intubafion, if elective, should always be performed under con- trolled conditions, the patient should re- ceive pre-oxygenation, sedation, and, if necessary, muscle relaxation. Some seda- fives such as morphine or its derivatives may aggravate hypotension. Careful consideration to the side effects of any drugs used, should always be given. Benzodiazepines such as diazepam .2 mg/kg, or midazolam .1 mg/kg, or syn- thetic narcotics such as fentanyl 1-3 mcg/kg W will provide adequate seda- tion with a lesser risk of hemodynamic instability.
Once the patient is intubated and muscle relaxed, optimal ventilation should be achieved, by using the neces- sary tidal volume to appropriately ex- pand the chest. High Positive End Expi- ratory Pressure (PEEP) may be necessary to achieve an adequate arterial oxygena- tion, as assessed by the patient's color, PaO 2, or by pulse oximeter SaO 2. Con- comitant to management of airway and ventilation, support of the circulation is mandatory. Immediate venous access via peripheral or central lines should be gained for fluid resuscitation. If venous access becomes difficult due to hypoten- sion, intraosseous access should be initi- ated. In addition to airway, breathing, and circulation, antibiotic treatment is of paramount importance in the treatment of septic shock. Blood cultures should be

374 THE INDIAN JOURNAL OF PEDIATRICS 1993; Vol. 60. No. 3
promptly obtained and antibiotic cover- age started according to the clinical situ- ation. After the ABC's of resuscitation have been established, individual organ- systems should be considered.
CNS
Critically ill patients should be ade- quately sedated. Anxiety or pain leads to catecholamine release and increased metabolic rate under conditions of al- ready precarious oxygen delivery. Con- tinuous intravenous infusion of seda- fives achieve better sedation than spor- dic IV boluses. Morphine .05 mg/kg/hr , fentanyl 3-5 mcg/kg/hr or midazolam 0.1 mg/kg /hr can be used. Sedatives should be titrated to achieve the desired effect. Some patients may require larger amounts or even combinations of two drugs, particularly those patients with longer clinical course in whom tolerance has developed. ~7 If the patient remains muscle relaxed, the neurologic exam with exception of pupillary reflexes, will be lost. At our institution, we use pheno- barbital to achieve a prophylactic anti- convulsivant effect, particularly on those patients with severe hypoxemic-ischemic events, or meningitis that may predis- pose to seizure activity. In the critically ill muscle relaxed patient, seizure activ- ity may manifest only as episodes of hypertension, tachycardia or desatura- tion. A therapeutic level of phenobarbital of about 20-40 mg/dL should be main- tained under these circumstances.
Cardiovascular
Cardiovascular support will depend on the clinical stage of septic shock that the patient presents with. Early and aggres-
sive fluid resuscitation is paramount for survival achieving increased cardiac out- put, DO 2 and VO 2, An initial bolus of crystalloid solution (lactated Ringer's or normal saline) at 20 m l / k g should be administered as an intravenous push or as a bolus over 20-30 minutes, depend- ing on the clinical status of the patient. Continuous reassessment of the patient's perfusion status (capillary refill time, pulses, heart rate, mentation, blood pres- sure) is mandatory. If there is no im- provement, IV fluid boluses should be repeated up to about 60 ml/kg in the first hour. This amount is only a guide- line and should suffice to restore the cir- culating volume in most patients. Some other patients, however, mainly those with meningococcemia will require larger amounts of fluid resuscitation. Garcillo and coworkers, 5 recently re- ported that a more aggressive fluid re- suscitation approach in the first hours of management is associated with an im- provement in survival and does not in- crease the risk of cardiogenic pulmonary edema or Adult Respiratory Distress Syndrome. If after adequate fluid resus- citation the patient remains hypotensive, invasive monitoring with a pulmonary artery catheter is required. Assessment of central venous pressure, cardiac out- put, pulmonary wedge pressure, sys- temic and pulmonary vascular resis- tances. DOz, VO 2 and oxygen extraction is imFoctant to guide fnrther manage- ment. If pulmonary artery catheteriza- tion is unavailable, determination of CVP, urine output, perfusion, metabolic acidosis and response to therapeutic ma- neuvers will provide the physician with clues about the pathophysiologic state of the patient. Sophisticated monitoring,

1993; VoL 60. No. 3 THE INDIAN JOURNAL OF PEDIATRICS 375
however, will never replace dedicatiorL to the patient and good clinical judge- ment.
When maintenance of an adequate perfusion cannot be achieved with fluid administration, the use of inotropic and / or vasopressor agents should be consid- ered. 3s'4~ Dopamine at starting doses of 5 mcg /kg /min and titrated to response, is a useful agent for hemod3nlamic sup- port. If doses greater than 20 mcg /kg / rain are reached without a satisfactory response, re-assessment of the hemody- namic state is necessary. Addition of an cx adrenergic agent such as epinephrine or norepinephrine, or a second intropic agent such as dobutamine, or further fluid boluses may be necessary. Restor- ing and sustaining hemodynamic stabil- ity is a primary goal in the management of septic shock. Hematocrit should be maintained about 40 in order to improve DO 2 in these patients. Hemodynamic stability should be achieved for at least 24 hours before weaning inotropic sup- port is considered.
Respiratory
The goal of respirator,/, management is to maximize DO 2. If hypoxemia secondary to ARDS develops, higher PEEP may be required. It is important to keep in mind that high PEEP will decrease cardiac out- put by : (i) reducing preload due to higher intrathoracic pressure, (ii) in- creasing right ventricular afterload due to increase in pulmonary vascular resis- tance, and (iii) decreasing left ventricular end diastolic volume (LVEDV) due to ventricular interdependence. If right ventricle becomes enlarged, it will dis-
place the ventricular septum and de- crease the LVEDV. Therefore, further fluid resuscitation or increasing inotropic support may be necessary when using high PEEP. 36-4~
Supplemental oxygen should be weaned as soon as possible. Tolerance for relatively lower PaO 2 (50-60 torr), hypercapnea (50-60 torr) and some respi- ratory acidosis (PH 7.28-7.30) will allow for survivors with lesser morbidity. 42
Gastrointestinal
Early enteral feedings are of major im- portance in preventing multiorgan fail- ure. The enteral route can provide larger amount of calories, avoids gut atrophy and may prevent bacterial transloca- tion. 31 Bronchoaspiration may be a risk, even fore those patients with cuffed en- dotrachealtubes. Use of nasojejunal feed- ings should prevent this complication. Continuous diluted feeding in small vol- ume should be started as soon ss pos- sible, often within 24-36 hours of the ini- tial septic episode.Although muscle re- laxation is not a contraindication for en- ternal feedings, narcotic sedatives may decrease intestinal motility, a change in sedative drugs may be necessary. Gastric PH should be monitored; of PH<4.5, ant- acid medications, H 2 blockers agents or sucralfate should be used.
Renal and Metabolic
Preservation of renal function in the management of the shock states is im- portant. This is done by maintaining an adequate intravascular volume with the administration of fluids and the use of

376 THE INDIAN JOURNAL OF PEDIATRICS 1993; VoL 60. ~ 3
dopamine at low doses (3 mcg/kg/min) to maintain renal blood flow. A Foley catheter should be placed to obtain an accurate estimation of renal function. In the presence of persistent oliguria, it is mmtdatory to rule out decreased cardiac output or hypovolemia before diuretics are used. Despite multiple fluid boluses, septic patients are often hypovolemic due to capillary leak syndrome, so that the infused fluids escape to the intersti- tial space with resultant oliguria. If fluid challenge does not resolve oliguria and there is hemodynamic evidence of ade- quate volume, diuretics such as furosem- ide euld/or mannitol are indicated. 3s
Fluids and Electrolytes
Once the acute episode of sepsis is con- trolled, these patients should be given two thirds to full maintenance fluids. In view of their requirement for blood products, multiple medications and fluid boluses, it is likely that over 24 hours the patients will have an excessively positive fluid balance. The objective of fluid ther- apy is to achieve an envolemic state while avoiding fluid overload. Electro- lyte abnormalities should be promptly corrected. Hypocalcemia often develops in patients with metabolic acidosis cor- rected with sodium bicarbonate. Hypo- phosphatemia and hypomagnesemia is often encountered. The latter particu- larly occurs in patients that have re- ceived aminoglycoside therapy. Hyper- glycemia and glucose intolerance is often seen early in the course of the disease, usually resolved by lowering the amount of glucose provided. ~ The use of insulin in septic hyperglycemic patients is con- troversial; although it will decrease the
blood glucose, insulin does not increase glucose oxidation and utilization in the septic patient. ~ Metabolic acidosis is a sign of poor perfusion and impaired DO r Under these conditions; fluid chal- lenge and improving cardiac output may prove beneficial. If metabolic acidosis persists despite adequate cardiac output and DO 2, sodium bicarbonate may be used. Parenteral nutrition should be ini- tiated whenever internal nutrition is not possible.
Disseminated Intravascular Coagula- tion (DIC)
Rapid recognition and treatment of the primary underlying disease continues to be the most important aspect of success- ful management of DIC, Replacement therapy with fresh frozen plasma (fac- tors II, V, VII, VIII, IX, X, XI, XII, an- tithrombin III, etc.), cryoprecipitate (Fac- tors VIII, yon Willibrand factor, fi- bronectin, fibrinogen), red blood cells, and platelets is necessary. 34 Heparin is not used to treat DIC unless there is evi- dence of thrombosis, and severe is- chemia that may lead to necrosis of the affected area. This is often seen in pa- tients with severe meningococcemia. In- hibitors of fibrinolysis such as e- aminocaproic acid may foster the ap- pearance of thrombosis and are not row tinely used.
Experimental Contmvemial Therapy
During the past years, there has been an explosion of potential therapies for sep- tic shock. When corticosteroids are give~ to animals before a challenge injection of a lethal endotoxin dose, septic shock

1993; Vol. 60. No. 3 THE INDIAN JOURNAL OF PEDIATRICS 377
does not develop. 44 Nevertheless, in human studies, high dose corticosteroid therapy failed to improve survival and increased morbidity and mortality from injection. 3 Corticosteroids are used oIfly in those septic patients with established or suspected adrenal insufficiency.
Nonsteroidal ant i - inf lammatory (NSAID) drugs have proved to be useful in different animal models of septic shock and lung injury. Preliminary stud- ies in human sepsis indicate possible benefits. An NIH sponsored multicenter trial is in progress to determine the effi- cacy of NSAID in the treatment of pa- tients with septic shock. Currently these drugs are still considered experimental. *s
Controlled studies using naloxone, an endrophin inhibitor, have failed to prove a beneficial effect and the therapeutic value is controversial. 46'.7
Pharmacological inhibition of nitric oxide synthesis has restored blood pres- sure in patients with septic shock.** Nev- ertheless, in view of the complex phar- macodynamic effects of drugs that in- hibit NO synthesis, this potential therapy will need to be carefully evaluated be- fore it can be widely applied to the clini- ca] setting. 49
Therapeutic use of human (HA-1A) monoclonal anti-lipid A ant ibody or murine-derived Ig M monoclonal anti- body has shown beneficial effects in se- lected populations of septic patients. The cost of this therapy is excessive and pa- tient selection is still controversia]? ~
Monoclonal ant ibodies to TNF (x proved to be efficacious in experimental animals, s2 Preliminary results in human studies are encouraging, s3 Receptor an- tagonists to IL 1 (ILt-a),S* or to PAF, ss are also potential beneficial therapies. Other
inhibitors of infammafion, such as com- plement C 1 and C s inhibitors, neutrophil and protease inhibitors (pentoxifylline, adenosine, etc.) antioxidants and oxygen radical scavengers may play a role in the management of complex pathophysiol- ogic events of sepsis, la Further studies are necessary to confirm their benefit, and determine proper clinical use.
The t reatment of septic shock no longer is limited to support ive care and anffbiotic adminis t ra t ion. Better understanding of the concepts of oxygen delivery and uptake from the tissues, and of the mechanisms of tissue and cellular injury has opened new opportunities to an earlier diagnosis and better treatment of this disease.
R~Ru~cEs
_I. Jacobs PR, SoweU M, Moss Met al. Sep- tic shock in children : Bacterial etiologies and temporal relationships. Pediatr Infec D/s J 1990; 9 : 196-200.
2. Shoemaker W. Hemodynamic and oxy- ben transport patterns in septic.shock : Physiologic mechanism and therapeutic implications. In : Sibbald W, Sprung CH, ed. Praspective an Sepsis and Septic Shade. Fullerton : Society of Critical Care Medicine, 1986 : p 203-234.
3. Bone R, Fisher C, Clemmer T. A con- trolled clincial trial of high-dose methyl prednisolone in the treatment of severe sepsis and septic shock. N Engl J Med 1987; 317 : 653-658.
4. Parker M, Parrillo J. Septic shock-hemo- dynamics and pathgogenesis. JAMA 1983; 250 : 3324-3327.
5. Garcillo J, Davis A, Zaritsky A. Role of early fluid resuscitation in pediatric sep- tic shock. JAMA 1991; 266 : 1242-1245.
6. Dal Nogare A. Septic shock. Am J Med 5c/1991; 302: 50-65.
7. Thijs L, Schneider A, Groeneveld A. The

378 THE INDIAN JOURNAL OF PEDIATRICS
haemodynamics of septic shock. Inten Care Med 1990; 16 : $182-$186.
8. Michalek S, Moore R, McGhee J e t al. The primary role of lymphoreticular cells in the mediation of host response to bacterial endotoxin. J Infect Dis 1980; 141 : 55-63.
9. Glauser M, Zanetti G, Baugmartner J et al. Septic shock : pathogenesis. Lancet 1991; 338 : 732-736.
10. Dunn D. Role of endotoxin and host cy- tokines iv. septic shock. Chest 1991; 100 : 1645-1685.
11. Beutler B, Cerami A. Cachectin : more than a tumor necrosis factor. N Engl J Med 1987; 316 : 379-385.
12. Fong Y, Lowry S, Cerami A. Cachec~'l/ TNF. A macrophage protein that in- duces cachexia and shock. J P.E.N. 1988; 12 : 725-775.
13. Moncada, S, Palmer R, Higge E. Nitric oxide physiology, pathophysiology and pharmacology. Pharmacol Rev 1991; 43 : 109-142.
14. Joulou-Shaeffer G, Gray G, Fleming I e t al. Loss of vascular responsiveness in- duced by endotoxin involves the L- arginine pathway. Am ] Physiol 1990; 259 : H1038-H1043.
15. Rock C, Lowry S. Tumor necrosis -ct J $urg Research 1991; 51 : 434-445.
16. Dinarello C, Mier J. Current concepts : Lymphokines. N Engl l Med 1987; 317- 940-945.
17. Dinarello C. Biology of interleukin. FASEB J 1988; 2 : 108-115.
18. Zimmerman J, Ringer T. Inflammatory host responses in sepsis. Crit Care Clin 1992; 8 : 163-189.
19. Zimmerman J, Dietrich K. Current per- spectives on septic shock. Ped CIin North Am 1987; 34 : 131-163.
20. Jackson A, Bolton C, Young G e t al. The encephalopathy of sepsis. Neurology 1983; 14 : 141-146.
21. Bolton C, Broun. J, Sibbalb W. The elec- trophysiologic investigation of respira-
1993; Vol. 60. No. 3
tory paralysis in critically ill patients. Neurology 1983; 33 : 2-18.
22. Crone R. Acute circulatory failure in children. Ped Clin North Am 1980; 27 : 525-538.
23. Bone R. Sepsis syndrome: New insights into its pathogenesis and treatment. In- tensive Crit Care Dig 1991; 10 : 49-56.
24. Suffredini A, Fromm R, Parker Me t al. The cardiovascular response of normal humans to the administration of endotoxin. N Engl J Med 1989; 321-280- 287.
25. Schumacker P, Cain S. The concept of a critical oxygen delivery. Intensive Care Medicine 1987; 13 : 223-229.
26. Tuschschmidt J, Fried J, Astiz M et al. Elevation of cardiac outpat and oxygen delivery improves outcome in septic shock. Chest 1992; 102 : 216-220.
27. Wysocki M, Besbes M, Roupiee et al. Modification of oxygen extraction ratio by change in oxygen transport in septic shock. Chest 1992; 102-221-226.
28. Nlson DP, Semsel RN, Wood LD et al. Pathological supply dependence of sys- temic and intestinal O 2 uptake during endo~oxemia. J Appl Phy$iol 1988; 64 : 2410.
29. Demling R. Current concepts on the adult respiratory distress syndrome. Circ Shock 1990; 30 : 297-309.
30. Sprung C, Cerra F, Freund H et al. Amino acid alterations and encephalo- pathy in sepsis syndrome. Crit Care Med 1991; 19 : 753-757.
31. Fiddian-Green R, Baker S. Nosocomial pneumonia in the critically ill : Product of aspiration or translocation. Crit Care Med 1991; 19 : 763-769.
32. Konturek S, Brzozowski T, Majka J et al. Role of nitric oxide and prostaglandins in sucralfate-induced gestroprotection. EurJPharm 1992; 211 : 277-279.
33. Carra F. Metabolic manifestations of multiple systmns organ failure. Crit Care Clin 1989; 5 : 119-131.

1993; Vol. 60. No. 3 THE INDIAN JOURNAL OF PEDIATRICS 379
34. Watson K, Vercelotte G. Issues in he- mostasis : Surgery and critical care. In : Cerra F, ed. Perspectives in Critical Care. 1989; 2 : 115-139.
35. Neild G. Manifestations of Lcellular in- jury : tubuloglomerular dysfunction in multiple organ failure. Bihari D, Cerra T, eds. Fullerton : Society of Critical Care Medicine. California 1989 : pp 263- 276.
36. Lee R, Balb R, Bone R. Ventilatory sup- port in the management of septic patients. Crit Care Clin 1989; S : 157-175.
37. Brill J. Control of pain. Crit Care Clin 1992; 8 : 203-218.
38. Natanson C, Hoffraan W. Septic shock and other forms of distributive shock. In : Parillo J, ed. Current Therapy in Critical Care Medicine. 2nd edn. Philadelphia : Marceli Decker Inc. 1991 : pp 62-70.
39. Schreuder W, Schneider A, Groenveld et al. Effect of dopamine vs norephineph- fine on hemodynamics in septic shock. Chest 1989; 95 : 1282-1288.
40. Chernow B, Kasinski M, Salem M. Cath- echolamines in critical illness. In : Lumb P, Shoemaker W, eds; Fullerton : Critical Care State of the Art Society of Crit Care Med. 1990 : pp. 75-113.
41. Pinky M. The hemodynamic effects of artificial ventilation. In : Snyder D: Pinsky M, eds. Oxygen Transport in the Critically Ill. Chicago : Year Book Medi- cal Publishers Inc. 1987 : pp 319=332.
42. Hickling K, Henderson S, Jackson R. Low mortality associated with low pres- sure limited ventilation with permissive hypercapnia in severe adult respiratory distress syndrome. Inten Care Med 1990; 16 : 372-377.
43. Burke JF, Wolfe RR, Mullany Ch Je t al. Glucose requirements following burn injury. Ann Surg 1979; 190 : 274-285.
44. Hinshaw L, Belier-Todd B, Archer L. Currrent management of the septic shock patient : Experimental basis for treatment. Cir Shock 1982; 9 : 543-553.
45. Petrak R, Balk R, Bone R. Prost- aglandins, cyclooxygenase inhibitors, and thromboxane synthesis inhibitors in the pathogenesis of multiple organ failure. Crit Care Clin 1989; 5 : 303-314.
46. Rock P, Silverman I-I, Plump D et al. Ef- ficacy and safety of naloxone in septic shock. Crit Care Med 1985; 13 : 28-33.
47. Napolitano L, Chemow B. Endorphins in circulatory shock. Crit Care Med 1988; 16 : 566-567.
48. Petros A, Bennett D, Vallance P. Effect of nitric oxide synthase inhibitory on hypotension in patients with septic shock. Lancet 1991; 338 : 1557-1559.
49. Hotchkiss R, Karl I, Parker Jet al. Inhibi- tion of NO synthesis in septic shock. Lancet 1992; 339 : 434-435.
50. Ziegler E, Fisher C, Sprung C et al. Treatment of gram negative bacteremia and septic shock with HA-IA human monoclonal antibody against endotoxin. A randomized, double blind, placebo control trial. N Engl J Med 1991; 324 : 429-436.
51. Warren H, Danner R, Munford R. An- tiendotoxin monoclonal antibodies. N Engl JMed 1~92; 326 : 1153-1157.
52. Walsh C, Sugerman H, Mullen P et al. Monoclonal antibody to tumor necrosis factor a attenuates cardiopulmonary dysfunction in porcine gram negative sepsis. Arch $urg 1992; 127 : 138-145.
53. Vincent J, Baker J, Marceaux G e t al. Administratoin of anti-TNF antibody improves left ventricular function in septic shock patients. Chest 1992; 101 : 810-815.
54. Ohlsson K, Bjork P, Bergenfeldt M e t al. Interleukin-1 receptor antagonist re- duces mortality from endotoxin shock. Nature 1990; 348 : 550-552.
55. Yue T, Farhat M, Rabinovici R. Protec- tive eff~t of BN 50739, a new platelet- activating factor antagonist, in en- dotoxin-treated rabbits, j Pharmacol Exp Ther 1990; 254 : 976-981.








![Septic Shock [EDocFind.com]](https://img.pdfslide.net/doc/110x75/55cf8fb1550346703b9edc7d/septic-shock-edocfindcom.jpg)