Embed Size (px)
Citation preview
Thorax 1987;42:401-408
For debate
Pulmonary sequestration and related congenitalbronchopulmonary-vascular malformations:nomenclature and classification based on anatomicaland embryological considerationsBS CLEMENTS, JO WARNERFrom the Brompton Hospital, London
No satisfactory classification for congenital anoma-lies of the bronchopulmonary airway and related vas-culature has yet been described. An attempt was madeto overcome this problem by expanding the conceptof "sequestration" (originally intended as a singleentity) to include a range of bronchovascular anoma-lies. This has failed to gain universal acceptance andled us to develop an alternative nomenclature andclassification based on simple anatomical description.This paper discusses the background to the newapproach while a companion paper applies it to ourown cases reviewed during five years.
History and background
Defining a congenital anatomical lesion of the lungaffecting a single structure (for example, bronchus) isrelatively simple (for example, bronchial stenosis,bronchogenic cyst). When this lesion includes abnor-malities of other major components of lung tissue-namely, arterial supply, venous drainage, and lungparenchyma-differentiation becomes more complex.In 1946 Pryce coined the term sequestration todescribe a "disconnected ("dislocated," "ectopic")bronchopulmonary mass or cyst with an anomaloussystemic artery supply."' Four of his original sevencases differed considerably from his own definition,which led him to describe three variants ofsequestration-namely: abnormal artery to normallyconnected lung; abnormal artery to both sequesteredmass and adjacent normal lung; and abnormal artery
Address for reprint requests: Dr JO Warner, Department of Pae-diatrics, Brompton Hospital, London SW3 6HP.
Accepted 11 February 1987
confined to the sequestered mass.2 Later the termsintralobar and extralobar were added but they pro-vide no definitive information on the morphologywithin these lesions. Despite this, many authoritieshave adhered to Pryce's terminology and con-sequently encountered problems in defining the vari-ants of sequestration. Many synonyms for thevarious atypical forms have been proposed, con-tributing further to the confusion concerning nomen-clature.3 7 Realisation that these entities mayrepresent variants of a single primary complex ofbronchovascular anomalies46 89 led to the concept ofa "sequestration spectrum," a term introduced bySade in 1974.10 This extended term included variouscombinations of abnormal bronchial connection,arterial supply and venous drainage, so bringing inthe scimitar syndrome and its variations." In 1984Thilenius again reviewed the sequestration spectrumconcept.12 He emphasised the wide range of anoma-lies found by quoting examples of every combinationof abnormal bronchial connection, arterial supply,and venous drainage appearing in published reports.He agreed with Sade, and others,'3 that sequesteredareas of lung with normal vasculature should beincluded in the spectrum. Nevertheless, reports of"atypical" sequestrations continued to inundate pub-lished reports,14 15 indicating that this concept hadfailed to gain general acceptance. To complicatematters further, associated abnormalities of venousdrainage and lung parenchyma were rather neglectedin most earlier reports. Recently the importance ofdefining the venous drainage in these lesions has beenemphasised,'2 16 and our experience further empha-sises this aspect (see p409). Associated abnormalitiesof lung parenchyma, both within the lesions and inthe surrounding lung, have not been widely appre-ciated, although their existence was noted in Pryce's
401
on 25 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.42.6.401 on 1 June 1987. D
ownloaded from
Clements, Warner
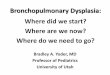
Anomalous venous drainage
Fig 1 Bronchopulmonary malinosculation: an abnormalityofthe bronchopulmonary airway (hatched area) may affect alocalised area (bronchogenic cyst), segment ("sequestration"with normal pulmonary artery supply, cystic adenomatoidmalformation), lobe, or lung (agenesis or hypoplasia). Theremay be associated normal or anomalous venous drainage.
original articles.1 2 We also expand on this feature inour clinical review.From these descriptions it is apparent that there are
essentially four components of these lesions-namely,the tracheobronchial airway, arterial supply, venous
drainage, and lung parenchyma. We should thereforebe able to construct a definition and classificationbased on these components that will cover all possibleanatomical combinations. In this paper we propose a
new nomenclature and classification with supportingevidence from histological and embryological obser-vation. The companion paper (p409) illustrates theclinical advantages of this simple anatomicalapproach.
NOMENCLATURE AND CLASSIFICATIONThere are several major objections to the use of"sequestration" as a collective term for all
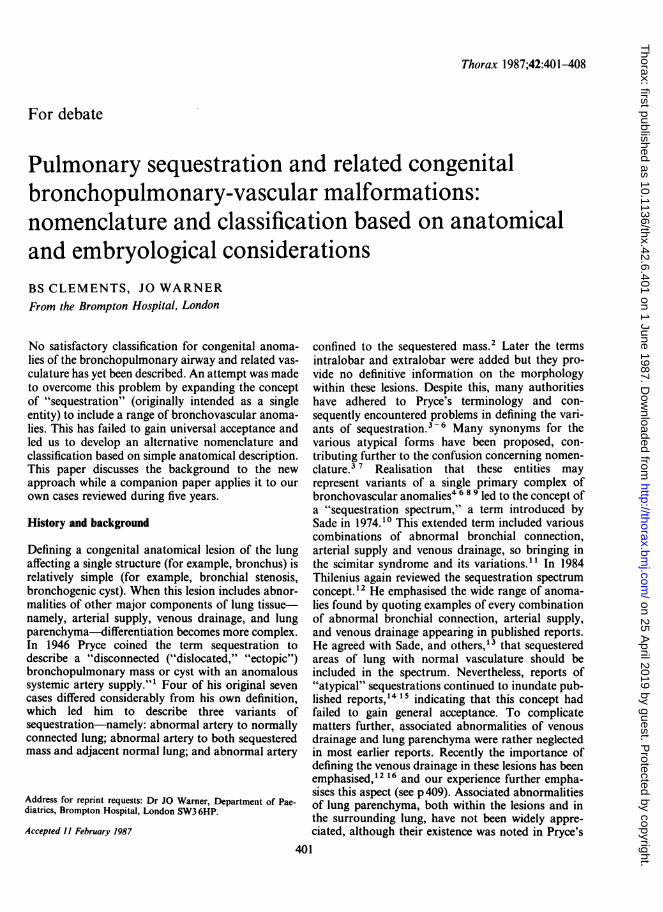
Normal venous drainage Anomalous venous drainage
Fig 2 Arterial pulmonary malinosculation with a systemicarterial supply to an otherwise normal area oflung. Theremay be normal or anomalous venous drainage. Evidence ofanassociated abnormality of the bronchopulmonary tree wouldalter this to bronchoarterial pulmonary malinosculation(fig 3).
Normal venous drainage Anomalous venous drainage
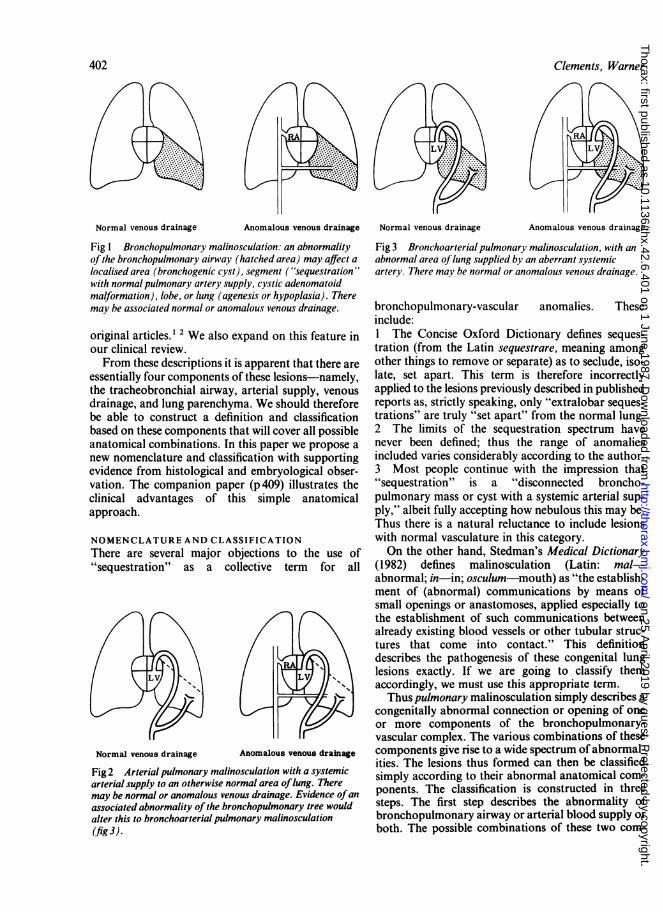
Fig 3 Bronchoarterial pulmonary malinosculation, with an
abnormal area oflung supplied by an aberrant systemicartery. There may be normal or anomalous venous drainage.
bronchopulmonary-vascular anomalies. Theseinclude:I The Concise Oxford Dictionary defines seques-
tration (from the Latin sequestrare, meaning among
other things to remove or separate) as to seclude, iso-late, set apart. This term is therefore incorrectlyapplied to the lesions previously described in publishedreports as, strictly speaking, only "extralobar seques-
trations" are truly "set apart" from the normal lung.2 The limits of the sequestration spectrum havenever been defined; thus the range of anomaliesincluded varies considerably according to the author.3 Most people continue with the impression that"sequestration" is a "disconnected broncho-pulmonary mass or cyst with a systemic arterial sup-ply," albeit fully accepting how nebulous this may be.Thus there is a natural reluctance to include lesionswith normal vasculature in this category.On the other hand, Stedman's Medical Dictionary
(1982) defines malinosculation (Latin: mal-abnormal; in-in; osculum-mouth) as "the establish-ment of (abnormal) communications by means ofsmall openings or anastomoses, applied especially tothe establishment of such communications betweenalready existing blood vessels or other tubular struc-tures that come into contact." This definitiondescribes the pathogenesis of these congenital lunglesions exactly. If we are going to classify themaccordingly, we must use this appropriate term.Thus pulmonary malinosculation simply describes a
congenitally abnormal connection or opening of oneor more components of the bronchopulmonary-vascular complex. The various combinations of thesecomponents give rise to a wide spectrum ofabnormal-ities. The lesions thus formed can then be classifiedsimply according to their abnormal anatomical com-
ponents. The classification is constructed in threesteps. The first step describes the abnormality ofbronchopulmonary airway or arterial blood supply or
both. The possible combinations of these two com-
402
Normal venous drainage
on 25 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.42.6.401 on 1 June 1987. D
ownloaded from
Pulmonary sequestration and related congenital bronchopulmonary vascular malformationsponents form a spectrum of lesions, as illustrated infigures 1-3. At one end of the spectrum is absence orabnormality of bronchopulmonary airway with nor-mal pulmonary artery blood supply (fig 1); this isbronchial pulmonary malinosculation or bron-chopulmonary malinosculation. At the other end ofthe spectrum (fig 2) is an anomalous arterial supply toan area of lung with a normal bronchopulmonary air-way; this is arterial pulmonary malinosculation. Inbetween we have all the combinations and gradationsof abnormal bronchial and arterial connection. Theserepresent bronchoarterial pulmonary malin-osculations (fig 3).The second step in the classification defines the
associated anomalies of venous drainage. Theclassification is then completed by describing anyassociated abnormalities of lung parenchyma. Eachof these steps will now be reviewed in more detail.
TRACHEOBRONCHOPULMONARYMALINOSCULATIONDisruption of normal airway communication canoccur at any level from the trachea down to the alveo-lus. Disruption may be incomplete (for example,stenosis) or complete (for example, atresia). Thelesion may be localised or extend distally to affect avariable segment of the bronchopulmonary tree.These lesions are conveniently divided into thoseaffecting proximal major airways (tracheopulmonarymalinosculation), such as tracheal stenosis and tra-cheal cysts, and those affecting the distal airwaysdown to respiratory bronchioles and alveoli (bron-chopulmonary malinosculation). This latter groupincludes lesions such as bronchial stenosis and bron-chogenic cysts, and parenchymal lesions with normalpulmonary artery blood supply, such as congenitallung cysts, cystic adenomatoid malformation, andlobar emphysema. Each of these entities may haveassociated anomalies of venous drainage and lungparenchyma. 12
ARTERIAL PULMONARY MALINOSCULATIONArterial pulmonary malinosculation refers to an aber-rant systemic arterial supply to an area of otherwisenormal lung.' 17 Most of these lesions, however, alsoaffect the tracheobronchopulmonary airway to someextent, which will mean that they are classified in thefollowing category.
BRONCHOARTERIAL PULMONARYMALINOSCULATIONHere there is an abnormality of both the bron-chopulmonary airway and the arterial blood supplyto an area of lung. The abnormality of bron-chopulmonary communication may range fromabsent connection with a blind ending bronchus
(agenesis) or atretic membrane to apparently normalpatency with a gradation of abnormality inbetween.49 1012 Abnormal branching patterns,reduced numbers of bronchial branches, or gener-alised hypoplasia may also occur.'2 18 The aberrantarterial blood supply can arise as one or more trunks,usually from the abdominal or thoracic aorta.3 11 Anabnormal area of lung sharing a mixed pulmonaryand systemic arterial blood supply has been described(see paper on p409). In addition, part of the sur-rounding normal lung may be supplied by the anoma-lous artery.'
Entities found in this group include sequestrations,lung cysts with aberrant systemic arterial supply, andcongenital cystic bronchiectasis. Again, each of theselesions may have associated anomalies of venousdrainage or lung parenchyma, or both (for example,scimitar syndrome).'8
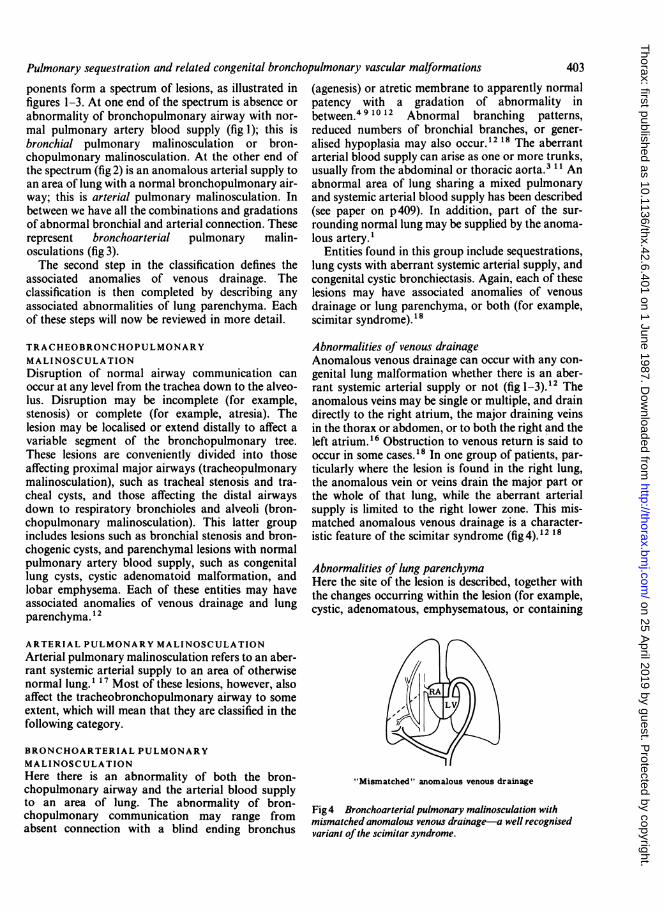
Abnormalities of venous drainageAnomalous venous drainage can occur with any con-genital lung malformation whether there is an aber-rant systemic arterial supply or not (fig 1-3). 12 Theanomalous veins may be single or multiple, and draindirectly to the right atrium, the major draining veinsin the thorax or abdomen, or to both the right and theleft atrium.'6 Obstruction to venous return is said tooccur in some cases.'8 In one group of patients, par-ticularly where the lesion is found in the right lung,the anomalous vein or veins drain the major part orthe whole of that lung, while the aberrant arterialsupply is limited to the right lower zone. This mis-matched anomalous venous drainage is a character-istic feature of the scimitar syndrome (fig 4).12 18
Abnormalities of lung parenchymaHere the site of the lesion is described, together withthe changes occurring within the lesion (for example,cystic, adenomatous, emphysematous, or containing
"Mismatched" anomalous venous drainage
Fig 4 Bronchoarterialpulmonary malinosculation withmismatched anomalous venous drainage-a well recognisedvariant of the scimitar syndrome.
403
on 25 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.42.6.401 on 1 June 1987. D
ownloaded from

404 Clements, Warner
Classification ofpulmonary malinosculation (first step defining basic abnormality oftracheobronchopulmonary airwayconnection or arterial blood supply or both, followed by description ofassociated anomalies of venous drainage and lungparenchyma)
Abnormality oftracheobronchopulmonary airway and/or arterial blood supply Venous drainage Lung parenchymal abnormalities
BRONCHOPULMONARY MALINOSCULATION(normal pulmonary artery blood supply)
ARTERIAL PULMONARY MALINOSCULATION(normal bronchopulmonary airway)
BRONCHOARTERIAL PULMONARYMALINOSCULATION(abnormal bronchopulmonary airway withsystemic arterial blood supply)
Examples ofrecognised entitiesTracheal-tracheal stenosis NormalBronchial-bronchial stenosis Anomalousor atresia, bronchogenic cyst MultipleParenchymal-congenital Mixedlung cyst, cystic adenomatoid Mismatchedmalformation, lobaremphysemaArea of lung with systemicblood supply
Bronchopulmonary airwaypatent but abnormal-congenital cystic bronchiectasis,lobar emphysema with systemicarterial supply, scimitarsyndromeBronchopulmonary connectionabsent-classical sequestration,congenital lung cysts withsystemic arterial blood supply
Site of the lesionIntrapulmonary, extrapulmonary
Within the lesionCystic, adenomatous, emphysematous,ectopic, foregut inclusionsAssociated abnormalities ofsurrounding lungAbnormal lobation, lobulation,hypoplasia
foregut inclusions) and associated abnormalities ofsurrounding lung parenchyma (for example, hypo-plasia and abnormal lobation). The site of the lesionmay be intrapulmonary (within the boundary formedby the pleural layer surrounding the lung) or extra-pulmonary (ectopic lung tissue lying outside theboundary formed by the pleural layer surroundingthe rest of the lung).The classification of pulmonary malinosculation is
summarised in table 1. The distinct clinical entitieswithin the classification should all retain their com-mon nomenclature. The purpose of this classificationis not to replace their accepted terminology but to aidcategorisation of these lesions, particularly the morecomplex varieties. In turn, it is hoped that this willimprove the understanding and management of thesecomplicated malformations. A good example of acomplex lesion affecting all four major components oflung tissue is a well recognised variant of the scimitarsyndrome usually presenting in infancy.'6 18-20 Thislesion is situated in the lower half of the right lungwith abnormal lobation and bronchial branching,anomalous systemic arterial supply and venous drain-age, and associated lung hypoplasia. A characteristicfeature is the "mismatch" between the aberrant sys-temic arterial supply to the right lower zone and theanomalous venous drainage of the whole or majorportion of the right lung (fig4).8 -20 According toour terminology, this malformation would beclassified as bronchoarterial pulmonary malin-osculation with mismatched anomalous venousdrainage and ipsilateral lung hypoplasia. In a clinicalcontext, each component would then need to be fur-ther defined-for example, in terms of the degree of
disruption in airway communication and the site ofanomalous venous return. The information, with theclinical history and haemodynamic data, is essentialfor appropriate patient management.
Discussion
Application of a unifying concept to congenital lungmalformations is certainly not new. In 1974 Buntainsuggested that lobar emphysema, cystic adenomatoidmalformation, pulmonary sequestration, and bron-chogenic cysts in children were a clinical group.2'Sade's spectrum ranged from an area of "sequesteredlung with normal pulmonary artery supply" to "anarea of normal lung with systemic artery supply,"much as we have described.'0 Heitzman went evenfurther, defining the sequestered lung with normalpulmonary artery supply as including congenital mal-formations previously classified elsewhere-such aslobar emphysema, congenital lung cysts, and evencystic adenomatoid malformation.'3 He warned that,although the terminology suggests that these are dis-crete entities, their morphological characteristicsoverlap to a considerable degree. Demos removedfrom a five month old infant a lobe whose tissue, bothgrossly and microscopically, showed characteristicsof "intra- and extralobular sequestration, bronchialatresia and cystic adenomatoid malformation."22 Asearly as 1969 Culiner, when comparing cases of "con-genital bronchial cystic disease, sequestration andcongenital cystic bronchiectasis," suggested that thesethree entities were variants of a single primary com-plex of bronchovascular anomalies.8 It would cer-tainly assist our understanding of their pathogenesis
on 25 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.42.6.401 on 1 June 1987. D
ownloaded from
Pulmonary sequestration and related congenital bronchopulmonary vascular malformations
if they could be regarded in this way.Fundamental to the subject of all malformations is
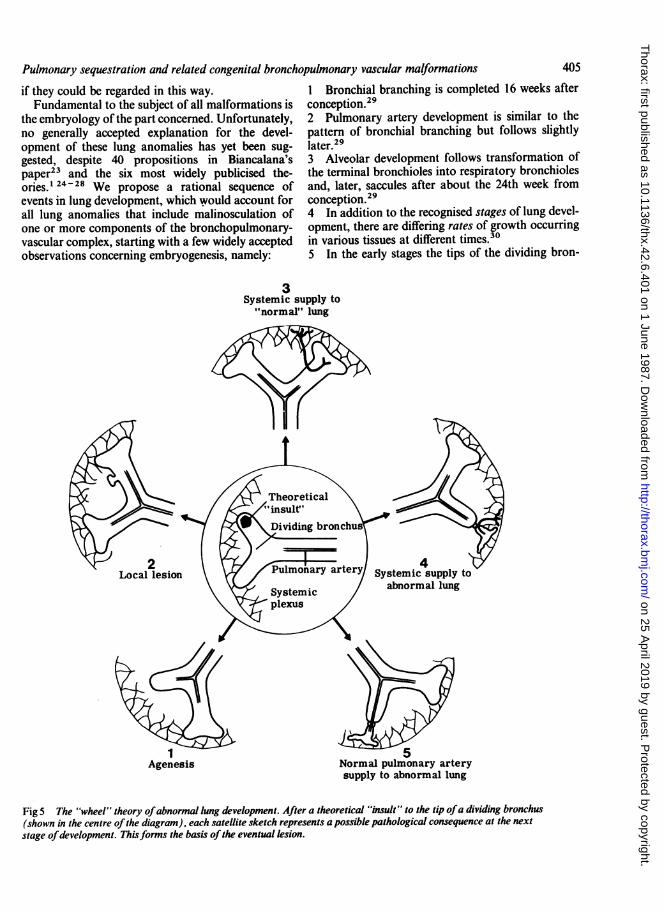
the embryology of the part concerned. Unfortunately,no generally accepted explanation for the devel-opment of these lung anomalies has yet been sug-gested, despite 40 propositions in Biancalana'spaper" and the six most widely publicised the-ories. 24-28 We propose a rational sequence ofevents in lung development, which would account forall lung anomalies that include malinosculation ofone or more components of the bronchopulmonary-vascular complex, starting with a few widely acceptedobservations concerning embryogenesis, namely:
I Bronchial branching is completed 16 weeks afterconception.292 Pulmonary artery development is similar to thepattern of bronchial branching but follows slightlylater.293 Alveolar development follows transformation ofthe terminal bronchioles into respiratory bronchiolesand, later, saccules after about the 24th week fromconception.294 In addition to the recognised stages of lung devel-opment, there are differing rates of growth occurringin various tissues at different times.305 In the early stages the tips of the dividing bron-
3Systemic supply to"normal" lung
1 5Agenesis Normal pulmonary artery
supply to abnormal lung
Fig 5 The "wheel" theory ofabnormal lung development. After a theoretical "insult" to the tip ofa dividing bronchus(shown in the centre ofthe diagram), each satellite sketch represents a possible pathological consequence at the nextstage ofdevelopment. Thisforms the basis ofthe eventual lesion.
405
on 25 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.42.6.401 on 1 June 1987. D
ownloaded from
406
chial buds are supplied by a systemic capillary plexusderived from the primitive aorta. This plexusregresses as the growing lung advances, the devel-oping pulmonary artery taking over.25 29 31The pathological options that follow an insult to
the tip of a developing bronchus can be graphicallyrepresented by the spokes of a wheel (fig 5). The"insult" is undetermined and could take the form oflocalised trauma, ischaemia, infection, adhesions, orany non-specific injury. It is not only the nature of theinsult, however, but also-and probably moreimportantly-the timing and severity that determinethe morphology of the eventual lesion.30The first possibility (I in fig 5) is that development
of the bronchus and its pulmonary artery supply istotally arrested, leading to agenesis of that lung, lobe,lobule, or segment. The timing will determine howdistal the lesion is.A second possibility (2 in figS) is that the insult
may be minor, resulting in a localised abnormalityfollowed by normal development of the distal bron-chial tree, lung parenchyma, and pulmonary artery.This will result in a local lesion, such as bronchialstenosis or a bronchogenic cyst.A third possibility (3 in figS) is that there is no
interference with continued development of the bron-chial tree, but pulmonary artery growth is arrested.Devoid of pulmonary blood supply, continuedgrowth of the developing bronchial branch could besupported only by vessels retained from its normallyregressing systemic capillary network. Growing alongwith the developing bronchial tree, these systemic ves-sels would become substantial channels, single ormultiple, and establish a systemic arterial supply tothe area of lung concerned. The sites of origin of thesevessels move distally with the caudal "shift" of thegrowing primitive aorta from which they arise, endingup in the lower thorax or upper abdomen. Such ananomalous area of "normal" lung with systemicartery supply has been very well shown in a 41 mmembryo by Boyden.25 These aberrant arteries are dis-tinct from bronchial arteries, which are found tooccur normally in these patients.25
In most instances, in an area of lung with an abnor-mal arterial blood supply the tracheobronchial treewill be affected to some degree, so that there will beoverlap with the following category.32 33
In a fourth possibility (4 in fig 5), the insult is severeenough to disrupt both airway and pulmonary arte-rial development so that a systemic arterial supply isretained to the subsequent abnormal area of lungparenchyma. This is a combined bronchoarterial pul-monary malinosculation, and in its purest formwould comply with most descriptions of "classical"sequestration.The final possibility (5 in figS) is that, although
Clements, Warner
there is considerable or complete disruption of thetracheobronchial connection, the pulmonary arterycontinues to develop and supply the abnormal lungsegment. This will result in tracheopulmonary orbronchopulmonary malinosculation with normal pul-monary artery blood supply, and include such entitiesas congenital lung cysts, so called sequestration withnormal pulmonary artery supply, and cystic ade-nomatoid malformation. Peripheral lesions of termi-nal and respiratory bronchioles and alveoli (forexample, congenital lobar emphysema) suggest adefect occurring late in development. Congenitallobar emphysema with systemic arterial blood supplyhas been described, supporting its embryologicalrelationship to other forms of malinosculation.
This leaves extrapulmonary lung anomalies. In theearly stages the developing lung bud, with its sur-rounding mesenchyme, lies in close proximity to theprimitive foregut, from which it is derived.24 28 Anyinsult or adhesion in an area where these two devel-oping organs are adjacent is therefore likely to affectboth structures; again, the timing and severity of theinsult is important to the eventual outcome. Nor-mally, the lung develops along genetically determinedlines, the dividing epithelial cells being influenced byhumoral factors from the surrounding mesen-chyme.10 34 Differentiating lung epithelial cells,drawn by adhesions towards the primitive foregut,may come to lie in mesenchyme, which is not condu-cive to their normal development. This would resultin dysmorphogenesis of the misplaced tissue.10 34Primitive communications between this ectopic tissueand adjacent organ may develop at any stage.10 26Subsequent development of the pleura could seques-trate this tissue from its parent organ, either partiallyor completely, resulting in extrapulmonary seques-tration or, alternatively, ectopic foregut derivativeswithin the lung. This hypothesis supports the con-tentions of ourselves and others3 6 8 15 27 that intra-pulmonary and extrapulmonary lesions have a similarorigin, without the need for an "accessory lung bud"theory.28 It also explains the high incidence of associ-ated congenital foregut anomalies occurring withextrapulmonary lung anomalies.The development of the venous drainage is less well
understood; but when anomalies of venous drainageoccur in association with pulmonary malinosculationthey are likely to be secondary to the primary lesion,and must be incorporated in the classification. Pri-mary congenital anomalous venous drainage andanomalous systemic pulmonary artery collaterals sec-ondary to congenital heart disease are not associatedwith any primary lung problem35 36 and are thereforenot included in the pulmonary malinosculation spec-trum.An interesting point is the absence of secondary
on 25 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.42.6.401 on 1 June 1987. D
ownloaded from
Pulmonary sequestration and related congenital bronchopulmonary vascular malformationsparenchymal changes in patients with pulmonary sys-temic collaterals secondary to congenital heart dis-ease (for example, in pulmonary atresia) even aftermany years. This confirms that the secondary changesthat occur in malinosculation syndromes are not dueto systemic pressures alone, but that there must besome underlying, inherent connective tissue abnor-mality within the lung neonatally.3" This is contraryto earlier hypotheses that parenchymal changes inmalinosculation syndromes were primarily a systemicpressure effect.24
Summary
The pulmonary sequestration spectrum and relatedcongenital lung anomalies present an extremely com-plex and varied group of bronchopulmonary-vascularmalformations. Previous attempts at nomenclatureand classification have proved inadequate. In thisarticle we present a classification of the newly namedpulmonary malinosculation spectrum, which includesall congenital lung anomalies where there is abnormalconnection (that is, malinosculation) of one or moreof the four major components of lung tissue-namely, tracheobronchial airway, lung parenchyma,arterial supply, and venous drainage, which in vari-ous combinations make up these lesions.We feel that this simple descriptive approach will
improve our understanding and management of thesecomplicated lesions and this is supported by the clin-ical experience we report in the next article.
We would like to thank Professor Brian Corrin,Department of Pathology, for his helpful advice andcriticism.
References
I Pryce DM. Lower accessory pulmonary artery withintralobular sequestration of lung: a report of sevencases. J Pathol 1946;58:457-67.
2 Pryce DM, Holmes Sellors T, Blair LG. Intralobarsequestration of lung associated with an abnormalpulmonary artery. Br J Surg 1947;35: 18-29.
3 Carter R. Pulmonary sequestration. Ann Thorac Surg1969;7:68-83.
4 Choplin RH, Siegel MJ. Pulmonary sequestration: sixunusual presentations. Am J Radiol 1980;134:695-700.
5 Flisak ME, Chandrasekar AJ, Marsan RE, Ali MM.Systemic arterilisation of lung without sequestration.Am J Radiol 1982;138:751-3.
6 Haller JA, Golladay ES, Pickard LR, Tepas JJ, ShorterNA, Shermeta DW. Surgical management of lung budanomalies: lobar emphysema, bronchogenic cyst, cys-tic adenomatoid malformation, and intralobar pul-monary sequestration. Ann Thorac Surg 1979;28:33-43.
7 Chiu RCJ, Herba MJ, Voloria J, Mulder DS. Tho-racopulmonary hypogenesis with systemic artery-pulmonary vessel fistulae: report of a case. Ann ThoracSurg 1981;31:360-3.
8 Culiner MM. Intralobar bronchial cystic disease, the"sequestration complex" and cystic bronchiectasis.Dis Chest 1968;53:462-9.
9 Takahashi M, Ohno M, Mihara K, Matsuura K, Sum-iyoshi A. Intralobar pulmonary sequestration. Radiol-ogy 1975;114:543-9.
10 Sade RM, Clouse M, Ellis FH. The spectrum of pul-monary sequestration. Ann Thorac Surg 1974;18:644-55.
11 Derksen OS. Scimitar syndrome and pulmonary seques-tration. Radiol Clin 1977;46:81-93.
12 Thilenius OG, Ruschhaupt DG, Replogle RL, Bharati S,Herman T, Arcilla RA. Spectrum of pulmonarysequestration: association with anomalous pulmonaryvenous drainage in infants. Pediat Cardiol1983;4:97-103.
13 Heitzman ER. The lung: radio-pathologic correlationsanomalies of pulmonary parenchymal and peripheralvascular development: the sequestration spectrum. 2nded. Philadelphia: CV Mosby, 1984:17-38.
14 Macpherson RI, Whytehead L. Pseudosequestration. JCan Assoc Radiol 1977;28:17-25.
15 Golding MR, Kwon K, Chiu CJ, Nicastri AD. Pul-monary sequestration. J Thorac Cardiocasc Surg1967;54:121-5.
16 Alivizatos P, Cheatle T, de Leval M, Stark J. Pulmonarysequestration complicated by anomalies of pulmonaryvenous return. J Pediat Surg 1985;20:76-9.
17 Kirks DR, Kang PE, Free EA, etal. Systemic arterialsupply to normal basilar segments of the left lowerlobe. Am J Roentgenol 1976;126:817-21.
18 Neill CA, Ferencz C, Sabiston DC, Sheldon H. Thefamilial occurrence of hypoplastic right lung with sys-temic arterial supply and venous drainage "scimitarsyndrome". Bull John Hopkins Hosp 1960; 107: 1-21.
19 Folger GM. The scimitar syndrome: physiologic, devel-opment and therapeutic considerations. Angiology1976;27:373-407.
20 Kuiper-Oosterwal CH, Moulaert A. The scimitar syn-drome in infancy and childhood. Eur J Cardiol1973;1:55-61.
21 Buntain WL, Isaacs H, Payne VC, Lindesmith GG,Rosenkrantz JG. Lobar emphysema, cystic ade-nomaloid malformation, pulmonary sequestration,and bronchogenic cyst in infancy and childhood: aclinical group. J Pediat Surg 1974;9:85-93.
22 Demos NJ, Teresi A. Congenital lung malformations: aunified concept. J Thorac Cardiovasc Surg1975;70:260-4.
23 Biancalana L. Die Lungenzysten. Thorax-Chirurge1963;9:511-31.
24 Abbey Smith R. A theory of the origin of intralobarsequestration of lung. Thorax 1956;11:10-24.
25 Boyden EA. Bronchogenic cysts and the theory of intra-lobar sequestration: new embryologic data. J ThoracSurg 1958;35:604-15.
26 Gerle RD, Jaretzki A, Ashley CA, Berne AS. Congenitalbronchopulmonary-foregut malformation. N Engl J
407
on 25 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.42.6.401 on 1 June 1987. D
ownloaded from
408Med 1968;278:1413-7.
27 Iwai K, Shindo G, Hajikano H, etal. Intralobar pul-monary sequestration, with special reference to devel-opmental pathology. Am Rev Respir Dis1973;107:911-20.
28 Eppinger H, Schauenstein W. Krakbeitene der Lungen.Erg Allg Pathol 1902;8:267.
29 Reid LM. Lung growth in health and disease. Br J DisChest 1984;78:1 13-34.
30 Stovin PGI. Early lung development. Thorax1985;40:401-4.
31 Gerbeaux J. Paediatric respiratory disease. 3rd ed. Lon-don: Wiley, 1985:185.
32 Blesovsky A. Pulmonary sequestration. Thorax
Clements, Warner
1967;22:351-7.33 Shimuzi K. Pulmonary sequestration, with special refer-
ence to pathogenesis of polycystic changes. Trans SocPathol Jap 1969;58: 180-6.
34 Dameron F. The influence of various mesenchyma onthe differentiation of the pulmonary epithelium of thechick embryo in culture in vitro. J Embryol Exp Mor-phol 1961;9:268-74.
35 Neill CA. Development of pulmonary veins with refer-ence to the embryology of anomalous venous return.Pediatrics 1956;18:880-8.
36 Edwards JE. Pathologic and development considerationsin anomalous pulmonary venous return. Mayo ClinicProc 1953;28:441-8.
on 25 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.42.6.401 on 1 June 1987. D
ownloaded from