Embed Size (px)
Citation preview
Archives ofDisease in Childhood 1990; 65: 1076-1081
CURRENT TOPIC
Bronchopulmonary dysplasia: then and now
William H Northway Jr
Bronchopulmonary dysplasia was first describedin 1967 in a series of 32 infants with severerespiratory distress syndrome who were treatedwith artificial ventilation and supplementaloxygen. 1 These infants had initially been givenantibiotics, the usual measures for control ofbody temperature, and glucose and sodiumbicarbonate intravenously to combat acidosis.They had not responded to this treatment, werecyanotic in 100% oxygen, looked moribund,and had had one or more prolonged apnoeicspells. The clinical and radiological progressionofrespiratory distress syndrome was significantlymodified by treatment with prolonged positivepressure ventilation, and 80-100% concen-trations of oxygen. What was remarkable wasthe appearance of a new syndrome of chroniclung disease that was called bronchopulmonarydysplasia. The usual course of respiratory dis-tress syndrome before the use of prolongedpositive pressure ventilation was that infantswho survived the first 3 days of life recoveredcompletely and by 7-10 days of life had normallungs radiographically.2 Those who died did sowithin four days. Chronic lung disease had notbeen seen as a sequel to respiratory distresssyndrome before the description of broncho-pulmonary dysplasia.The clinical, radiological, and pathological
progression of bronchopulmonary dysplasia wasinitially divided into four stages.' Stage I (days1-3) consisted of the initial clinical and radio-logical picture of respiratory distress syndrome.During stage II (days 4-10) there was increasingopacification of the lungs and, if the infant died,there was thick exudation into the lumen of theairway with patchy bronchiolar and alveolarepithelial necrosis with early stages of repair. Atthe end of stage II, weaning of the infants fromthe high concentrations of oxygen (80-100%)could usually be started. Stage III (days 10-20)was a period of transition to chronic lungdisease with the chest radiograph showing areticular network of small rounded areas ofradiolucency that represented areas of emphy-sematous alveoli adjacent to atelectatic alveoli,and pulmonary fibrosis. This stage could becomplicated by patent ductus arteriosus andcongestive heart failure. In stage IV (after 30days of age) there was persistent chronic lungdisease with hyperexpansion and cystic lookinglungs. The electrocardiogram at this stageusually showed right ventricular hypertrophyand cardiomegaly with cor pulmonale. Patho-logically, there was emphysema with thickening
of the lung interstitium, replacement of type Ipulmonary epithelial cells with type II pneumo-cytes, squamous metaplasia and ulceration ofbronchiolar epithelium, hypertrophy of bron-chiolar smooth muscle, and early vascularlesions indicating pulmonary hypertension withperiarteriolar thickening.
Since the original description of broncho-pulmonary dysplasia, it has been described allover the world in places where artificial ventil-ation and supplemental oxygen have been usedto treat infants with severe respiratory distresssyndrome. Bronchopulmonary dysplasia hasbecome the most common form of chronic lungdisease in infancy in the United States, withabout 7000 new cases occurring each year(35 000 cases of respiratory distress syndrome/year times a 0-20 incidence of bronchopulmon-ary dysplasia/per case of respiratory distresssyndrome).3
PathogenesisThe principal factors in the the pathogenesis ofbronchopulmonary dysplasia are (i) prematurebirth, (ii) respiratory failure, (iii) oxygen toxi-city, and (iv) barotrauma. Premature birth isassociated with immature lung structure, lack ofsurfactant, and inadequate respiratory drive, allof which contribute to respiratory failure.Respiratory failure is critical in the pathogenesisbecause it requires treatment with supplementaloxygen and artificial ventilation. The respiratoryfailure may be from any cause, but is mostcommonly from respiratory distress syndrome.The interaction ofthe concentration and durationof supplemental oxygen and the immaturity ofthe lung determines in part the development ofbronchopulmonary dysplasia.4 Since 1967 thesupplemental oxygen concentration used intreating respiratory distress syndrome has beenreduced, and many of the infants are lessmature. The premature infant who requiressupplemental oxygen is at risk of oxygen injuryto the lung because the immature antioxidantactivity, both enzymatic and non-enzymatic,may not be sufficient to protect against theincreased generation of oxygen radicals.5 Theeffects of prolonged exposure to concentrationsof supplemental oxygen of less than 60% on theimmature human or animal lung are not known.Positive pressure ventilation is important in thepathogenesis of bronchopulmonary dysplasiabecause it facilitates the delivery of supplementaloxygen and can further injure the lung by
Department ofDiagnostic Radiologyand Nuclear Medicine,Stanford UniversitySchool of Medicine,Stanford, California94305-5105, USACorrespondence to:Professor Northway.
1076
on 17 Novem
ber 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.10_Spec_N
o.1076 on 1 October 1990. D
ownloaded from
Bronchopulmonary dysplasia: then and now
barotrauma. Pulmonary interstitial emphysemaand pneumothorax are the most obvious clinicalfindings of barotrauma, but damage to the smallairways in the surfactant deficient lung can
occur without actual rupture of the wall ofthe airway.6 Factors that prolong artificialventilation and supplemental oxygen therapycontribute to the degree of severity of broncho-pulmonary dysplasia and include pulmonary airleak (interstitial emphysema, pneumomediasti-num, and pneumothorax), pulmonary oedema(patent ductus arteriosus, cor pulmonale, con-
gestive heart failure, and fluid overload), andpulmonary infection. Ureoplasma urealyticumhas recently been isolated more often from pre-maturely born infants who developed broncho-pulmonary dysplasia than those who did not,but respiratory distress at birth was not associ-ated with colonisation with the organism.7 Thepart played by U urealyticum in the pathogenesisof bronchopulmonary dysplasia remains to bedetermined.
PathologyThe changes in the bronchiolar regions inbronchopulmonary dysplasia have been attri-buted both to barotrauma and to pulmonaryoxygen toxicity. Overdistension of airways andirregular aeration of the alveoli can producesheer forces in the airway mucosa that lead todisruption of the epithelium during artificialventilation.8 Necrotising bronchiolitis andsquamous metaplasia similar to those seen inbronchopulmonary dysplasia are seen withexperimental pulmonary toxicity in newbornmice.9 The inflammatory cells that accumulateabout the small airways and in the alveolar wallsamplify the structural damage and enhance therecruitment and proliferation of fibroblasts,which leads to accumulation of type I collagenin these areas.'0 Derangement of pulmonarytissue with almost complete loss of the lung'snormal architecture associated with extensiveinterstitial and interalveolar fibrosis has consis-tently been described in pathological studies ofbronchopulmonary dysplasia. 11-'3 Increasednumbers of pulmonary inflammatory cells havebeen well documented in serial bronchoalveolarlavage fluid samples from newborn infants withrespiratory distress syndrome who subsequentlydeveloped bronchopulmonary dysplasia.4 15
Associated with the large numbers of neutro-phils in these infants are sustained high elastase,and low cxl-protease inhibitor, activities. Thiselastase-protease inhibitor imbalance promoteshydrolysis of the connective tissue matrix. Asthe inflammatory process progresses, alveolarmacrophages become more prominent inbronchoalveolar lavage fluid. They also produce
an elastase and, when injured, can accelerate therelease of neutrophil elastase. 6 Proteolyticenzymes released by inflammatory cells mayplay an important part in the damage ofepithelial and connective tissue in broncho-pulmonary dysplasia. Preterm infants may bemore susceptible to injury by the proteolyticenzymes because they have low concentrationsof serum proteins, including the antiproteases. 7
Because these proteolytic enzymes and thebyproducts of the injuries that they cause
appear in bronchoalveolar lavage fluid beforethere is clinical and radiological evidence ofbronchopulmonary dysplasia, they may prove
useful as early indicators of development of thedisease.
Animal experimentsA prematurely delivered immature baboonmodel for bronchopulmonary dysplasia hasbeen developed.'8 The prematurely deliveredbaboon develops a syndrome similar to respira-tory distress syndrome, and requires artificialventilation with supplemental oxygen to survive.Treatment with prolonged artificial ventilationand oxygen supplementation does result in theproduction of stage III bronchopulmonarydysplasia in the immature baboon. It has notbeen possible with this animal model, however,subsequently to eliminate any ofthe contributingfactors to test the hypothesis that any one ofthem alone can produce a continuum of patho-logy similar to bronchopulmonary dysplasia. Todate the only single factor that has been shownto produce a continuum of pathology similar tobronchopulmonary dysplasia in its acute,subacute, and chronic forms in a newbornmammalian lung is pulmonary oxygen toxicity.'9
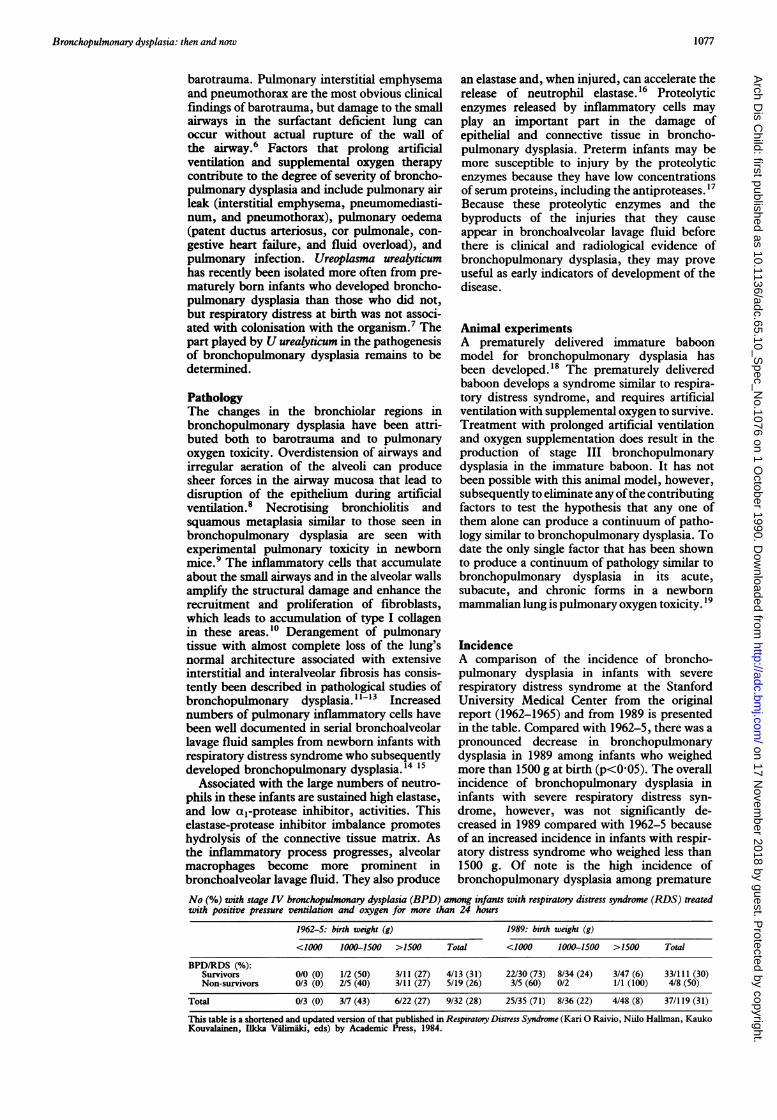
IncidenceA comparison of the incidence of broncho-pulmonary dysplasia in infants with severerespiratory distress syndrome at the StanfordUniversity Medical Center from the originalreport (1962-1965) and from 1989 is presentedin the table. Compared with 1962-5, there was a
pronounced decrease in bronchopulmonarydysplasia in 1989 among infants who weighedmore than 1500 g at birth (p<0 05). The overallincidence of bronchopulmonary dysplasia ininfants with severe respiratory distress syn-
drome, however, was not significantly de-creased in 1989 compared with 1962-5 becauseof an increased incidence in infants with respir-atory distress syndrome who weighed less than1500 g. Of note is the high incidence ofbronchopulmonary dysplasia among premature
No (%) with stage IV bronchopulmonary dysplasia (BPD) among infants with respiratory distress syndrome (RDS) treatedwith positive pressure ventilation and oxygen for more than 24 hours
1962-5: birth weight (g) 1989: birth weight (g)
<1000 1000-1500 >1500 Total <1000 1000-1500 >1500 Total
BPD/RDS (%):Survivors 0/0 (0) 1/2 (50) 3/11 (27) 4/13 (31) 22/30 (73) 8/34 (24) 3/47 (6) 33/111 (30)Non-survivors 0/3 (0) 2/5 (40) 3/11 (27) 5/19 (26) 3/5 (60) 0/2 1/1 (100) 4/8 (50)
Total 0/3 (0) 3/7 (43) 6/22 (27) 9/32 (28) 25/35 (71) 8/36 (22) 4/48 (8) 37/119 (31)
This table is a shortened and updated version of that published in Respiratory Distress Syndrome (Kari 0 Raivio, Niilo Hallman, KaukoKouvalainen, Ilkka V8limiki, eds) by Academic Press, 1984.
1077
on 17 Novem
ber 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.10_Spec_N
o.1076 on 1 October 1990. D
ownloaded from

Northway
infants with respiratory distress syndromeweighing less than 1000 g in 1989. In 1962-5,infants weighing less than 1000 g were notartificially ventilated, as the techniques werenot sufficiently developed to apply them tothese very low birthweight (VLBW) infants.The high incidence of bronchopulmonarydysplasia in VLBW premature infants is anincreasing problem.
Radiological changesThe progression of radiological change has beenmodified as stage IV bronchopulmonary dys-plasia has become more common in infantsweighing 1000 g or less, and as supplementaloxygen concentrations and peak inspiratorypressures and their durations have decreased.20The initial radiograph is usually of immaturelung or respiratory distress syndrome, but thelungs may not become completely opaque with-in the first few days of treatment as originallydescribed, but instead remain persistently hazyfor several weeks. At 3 or 4 weeks of age thehazy opacification changes into a fine reticularpattern, with or without hyperexpansion. Thisreticular pattern may first be noted at 30 days ofage, but can initially be seen even later. Itsinitial appearance may be masked by pulmonaryoedema, pneumonia, or poor inspiration. Thecharacteristic radiographic progression of bron-chopulmonary dysplasia that was originallydescribed still occurs in the more severely illinfants, particularly those whose course is com-plicated and prolonged by infection, congestiveheart failure, fluid overload, or interstitialemphysema.The incidence ofbronchopulmonary dysplasia
seems to be considerably higher in infants whodevelop pulmonary interstitial emphysema.2' Ifthe interstitial emphysema is diffuse and persis-tent, the characteristic radiographic appearanceof chronic bronchopulmonary dysplasia will bedifficult to differentiate from pulmonary inter-stitial emphysema. If pulmonary interstitialemphysema persists until the infant is 3 weeksof age, the patient invariably also has broncho-pulmonary dysplasia.
DiagnosisAs bronchopulmonary dysplasia has evolvedand the radiographic picture has been modified,the diagnostic criteria have become more clinicaland physiologically oriented. The diagnosis ofbronchopulmonary dysplasia (usually meaningstage IV or chronic disease) includes assessmentat 3 or 4 weeks of age, a history of artificialventilation and supplemental oxygen for at least24 hours, signs of respiratory distress includingan abnormal respiratory rate (greater than40/minute), persistent intercostal retractions,raised carbon dioxide tension (or requirementfor supplemental oxygen for longer than 3 or 4weeks), and persistent abnormalities on chestradiographs. This approach to the diagnosis ofbronchopulmonary dysplasia (recommended byFarrell and Palta) relies on signs and symptomsof the infant's respiratory disease rather thanon therapeutic decisions by the physician and
should be more replicable among neonatalintensive care nurseries.'
OutcomeIncreased airway resistance, increased airwayreactivity, low dynamic compliance, increasedfunctional residual capacity, increased respira-tory rate, high arterial carbon dioxide tension,low arterial oxygen tension, severe maldistribu-tion of ventilation, right or left (or both)ventricular hypertrophy, pulmonary hyperten-sion, and systemic hypertension have beenshown in surviving 1 to 2 year old infantswith bronchopulmonary dysplasia.22-3' Theseabnormalities of cardiopulmonary function canimprove with age but may not resolve.25 Airwayobstruction, airway hyper-reactivity, abnormalarterial capillary blood gas values, radiologicalabnormalities, increased lung volume, and elec-trocardiographic abnormalities have been foundin nine children with a history of broncho-pulmonary dysplasia at an average age of 8-4years.32 Increased lung volumes, airwayobstruction, and increased transcutaneouscarbon dioxide tension have been documentedin a group of 10 children with an average ageof 10 4 years who had bronchopulmonarydysplasia.33 We have recently shown that mostof 22 young adults age 14-23 years who had hadbronchopulmonary dysplasia, had pulmonarydysfunction consisting of airway obstruction,airway hyper-reactivity, and air trapping whencompared with 20 ex-prematurely born youngadults of the same age and 48 normal volunteersof the same age.34
Injury to small airways in premature infants'lungs has been a prominent feature and aparticularly disturbing aspect of the pathologyof bronchopulmonary dysplasia.9 The possiblerelationship between lower respiratory illness inchildhood and chronic airflow obstruction inadulthood was reviewed by Samet et al.35 Injuryto the small airways was the common feature ofthe respiratory illnesses in childhood, such asinfection with respiratory syncytial virus, whichmight be associated with chronic airwayobstruction. In a series of 40 prematurely borninfants who had survived artificial ventilationfor respiratory insufficiency, 70% had one ormore episodes of pneumonia or bronchitisduring the first 2 years of life.36 There was adirect relationship between the presence ofbronchopulmonary dysplasia and the number oflower respiratory tract infection. A four monthprospective study of 30 children less than2 years old with bronchopulmonary dysplasiashowed that 59% developed respiratory syncytialvirus infection and 70% of those requiredadmission to hospital.37 Premature infants whodevelop bronchopulmonary dysplasia may bepredisposed to have an increased incidence oflower respiratory illnesses and to developobstructive airways disease as adults.Many infants with bronchopulmonary dys-
lasia are below the third centile for height andweight during the first 2 years of life,3" andpersistent growth delay may persist throughoutearly childhood and beyond. Our follow upstudy of young adults who had had broncho-
1078
on 17 Novem
ber 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.10_Spec_N
o.1076 on 1 October 1990. D
ownloaded from
Bronchopulmonary dysplasia: then and now
pulmonary dysplasia indicated that, as a group,they were slightly but significantly shorter andlighter than the normal or prematurely born agematched control group.34
Neurodevelopmental deficits have also beenreported to occur more often in infants andchildren with bronchopulmonary dysplasia. It isnot clear whether these are caused by broncho-pulmonary dysplasia or by some perinatal orneonatal event.38 39 Neurological abnormalitieshave been reported in 0 to 38% of prematureinfants with a diagnosis of bronchopulmon-ary dysplasia.' Developmental abnormalitiesmeasured by the Bayley Scales Mental Develop-ment Index ranged from 14% to 80% in infantswith bronchopulmonary dysplasia. Only onestudy looked at children as old as 8 years of age,and no significant effect of bronchopulmonarydysplasia on neurodevelopmental outcome wasfound.4' Late evaluation of growth and develop-ment in young adults who had had broncho-pulmonary dysplasia deserves further attention.
TreatmentReducing the incidence of premature birthswould be the single most effective way ofreducing the incidence of bronchopulmonarydysplasia, and this is both a scientific and asocioeconomic problem. Medical complicationsof pregnancy and fetal factors leading to pre-mature delivery can be reduced, but not elimi-nated, by advances in medical science. Avail-ability and use of prenatal care is stronglyassociated with improved outcome of preg-nancy.42 Provision of adequate prenatal care forall pregnant women and reduction of adversematernal practices requires educational andsocial political action.Once an infant has been born prematurely,
the prevention of bronchopulmonary dysplasiarests on preventing the development of respira-tory distress. The use of exogenous surfactant asa means of preventing or decreasing the severityof respiratory distress syndrome is currentlyreceiving considerable attention. The effective-ness of several surfactant preparations is beinginvestigated, including those derived from calfand pig lungs, those artificially produced, andhuman surfactant from amniotic fluid. Com-parison of different clinical trials is difficultbecause of differences in prophylaxis and treat-ment regimens, gestational ages of the subjects,composition of the exogenous surfactants, out-come measures, and insufficient identificationof lung maturity.43The results from several controlled clinical
trials are equivocal. Surfactant given prophy-lactically has decreased the incidence andseverity of respiratory distress syndrome.4 8Many trials have reported reductions in mortalityand in the incidence of pulmonary air leak, andimproved gas exchange.43 A consistent signifi-cant reduction in the incidence of broncho-pulmonary dysplasia has not, however, beenshown. Surfactant seems to be a safe com-pound, although foreign proteins in someexogenous surfactants have the potential foractivating the immune system. Sensitisation hasnot been shown in humans to date. Three follow
up studies have been unable to identify any longterm adverse effects of surfactant treatment.495'The exogenous surfactant preparations in use inthe United States are considered to be underinvestigation and the most effective dose ofsurfactant has not been determined.The natural antioxidant protection of pre-
mature infants may well be inadequate. Becauseoxygen toxicity is believed to play a part in thepathogenesis of bronchopulmonary dysplasia,the lowest concentration ofsupplemental oxygenthat achieves an arterial oxygen tension of 8-0kPa or greater should be used to treat therespiratory distress. Enhancing antioxidant pro-tection with exogenous superoxide dismutasemay offer some protection against developingbronchopulmonary dysplasia, but this has notyet been thoroughly evaluated. Currently itseems reasonable to attempt to maintain'normal' levels of activity of antioxidant protec-tion in the face of continuing supplementaloxygen challenge. Nutritional factors that con-tribute to antioxidant protection such a vitaminE, vitamin C, and ,-carotene need to beprovided as part of the management of anypremature infant likely to develop broncho-pulmonary dysplasia.High frequency positive pressure ventilation,
high frequency jet ventilation, and high fre-quency oscillation have been developed toprovide artificial ventilation and reduce baro-trauma. It is unclear whether any of thesetechniques offer any advantages over conven-tional mechanical ventilation in the routinetreatment of respiratory failure of preterminfants. Their use does not seem to decrease theincidence of bronchopulmonary dysplasia, andmay be associated with undesirable side effectssuch as increased incidence of grade III or IVintracranial haemorrhage.52Once the infant has developed broncho-
pulmonary dysplasia, bronchodilators are oftenused in management. Their use has been basedon the clinical observation that many of theseinfants had bronchospasm, and infants whodied of bronchopulmonary dysplasia had hyper-trophied peribronchial smooth muscle.9 Theo-phylline has been shown to produce appreciableimprovements in airway resistance, specificconductance, complicance, and maximalexpiratory flow.53 The developmental variabilityin theophylline clearance requires that plasmaconcentrations be routinely monitored anddosages adjusted. Theophylline toxicity is aconcern because it has similar side effects tocaffeine, and death may result from serumconcentrations above 33 ig/ml.54 ,B-2 Adrenergicblocking agents have also been used in themanagement of bronchospasm in infants withbronchopulmonary dysplasia. The use ofinhaledisoproterenol has decreased airway resistanceand specific conductance and decreased thework of breathing55 56; subcutaneous terbuta-line, oral metaproterenol, and inhaled salbut-amol have produced similar results.57 58Accumulation of fluids may contribute to the
narrowing of small airways, altered pulmonarymechanics, and impairment of gas exchange ininfants with bronchopulmonary dysplasia.59Treatment with diuretics seems to improve lung
1079
on 17 Novem
ber 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.10_Spec_N
o.1076 on 1 October 1990. D
ownloaded from
1080 Northway
mechanics consistently and should decrease thework of breathing in infants with broncho-pulmonary dysplasia. This effect is seen in bothacute and chronic cases. Frusemide and chloro-thiazide are the most commonly used diuretics,and their side effects are related to electrolyteloss in the urine and include the formation ofrenal calculi.
Corticosteroids have been used in themanagement of bronchopulmonary dysplasiaduring the acute, subacute, and chronic phasesof the disease. Long acting corticosteroids suchas dexamethasone may lead to a short termimprovement in pulmonary function and facili-tate weaning from mechanical ventilation.59 Itsuse for as long as 42 days may improvepulmonary and neurodevelopmental outcome inVLBW infants at high risk ofbronchopulmonarydysplasia.60 The mechanism of action may be adecrease in lung oedema and polymorphonuclearinfiltration and an increase in surfactant. Themost serious short term side effects are increasedrisk of infection and hypertension, and with thelong term treatment there is the potential for anincreased incidence of pulmonary air leaks.Before steroids are used routinely in treatingbronchopulmonary dysplasia, further data areneeded regarding dose, duration of treatment,and the risk:benefit ratio.
Increasing attention is being paid to the roleof nutrition of infants with bronchopulmonarydysplasia.6' Infants with bronchopulmonarydysplasia at 60 days of age have been shown toabsorb energy as well as normal control infants,but they have a lower energy intake and a higherenergy expenditure, which results in poor weightgain.62 They may also have alterations in thecomposition of their body tissues, with arelatively high water content. Malnutrition hasdeleterious effects on patients with chronic lungdisease and close attention to the nutrition ofinfants with bronchopulmonary dysplasia isimportant. The effects of diuretics, gastro-oesophageal reflux, increased need of energy,and fluid restriction in infants with broncho-pulmonary dysplasia make it difficult to providethem with adequate nutrition.
Infants with bronchopulmonary dysplasiarequire long periods in hospital. There is,however, an increasing tendency to developprogrammes for earlier discharge ofthese infantswhile they are still dependent on supplementaloxygen.63 Infants with bronchopulmonarydysplasia are susceptible to sudden infant deathlate in their hospital course,64 and after dis-charge.65 Before early discharge is sanctioned,there should be careful review of the infant'scardiorespiratory state and management,including the oxygen requirement, weight gain,medication regimen, and feeding plan.66Parental attitude plays an important part in thesuccess of such a programme.Bronchopulmonary dysplasia remains an
appreciable problem for neonatologists. Thenumber of children with bronchopulmonarydysplasia seen by paediatricians is increasing.These children may present with reactive air-ways disease, recurrent pulmonary infections,and resemble patients with asthma. Thoughbronchopulmonary dysplasia is thought of as a
chronic lung disease of infancy, its results mayprove to be life long.
1 Northway WH Jr, Rosan RC, Porter DY. Pulmonary diseasefollowing respirator therapy of myaline membrane disease:bronchopulmonary dysplasia. N Engl J7 Med 1967;276:357-68.
2 PetersonHG Jr, Pendleton ME. Contrasting roentgenographicpulmonary patterns ofhyaline membraneand fetal aspirationsyndromes. AJR 1955;74:800-17.
3 Farrell PM, Palta M. Bronchopulmonary dysplasia. In:Farrell PM, Taussig LM, eds. Bronchopulmonary dysplasiaand isolated chronic respiratory disorders. Columbus, Ohio:Ross Laboratories, 1986:1-7.
4 Edwards DK, Dyer WM, Northway WH Jr. Twelve yearsexperience with bronchopulmonary dysplasia. Pediatrics1977;59:839-46.
5 Frank L, Groseclose EE. Preparation for birth into an 02 richenvironment: the antioxidant enzymes in the developingrabbit lung. Pediatr Res 1984;18:240-4.
6 Nilsson R, Grossman G, Berggren P, Robertson B. Patho-genesis of neonatal lung lesions induced by artificialventilation: evidence against the role of barotrauma.Respiration 1980;4:218-25.
7 Wang EE, Frayha H, Watts J, et al. Role of ureaplasmaurealyticum and other pathogens in the development ofchronic lung disease of prematurity. Pediatr Infect Dis1988;7:547-51.
8 Robertson B. Surface forces in respiratory bronchioles duringa first breath-model experiment and some theoreticalconsiderations. Scandinavian,Journal ofRespiratory Diseases1976;57:160-2.
9 Bonikos DS, Bensch KG, Northway WH Jr, et al. Broncho-pulmonary dysplasia: the pulmonary pathologic sequel ofnecrotizing bronchiolitis and pulmonary fibrosis. HumPathol 1976;7:643-66.
10 Shoemaker CT, Reiser KM, Goetzman B, et al. Elevatedratios of type I/III collagen in the lung of chronicallyventilated neonates with respiratory distress. Pediatr Res1984;18:1176-80.
11 Taghizadeh A, Reynolds EOR. Pathogenesis of broncho-pulmonary dysplasia following hyaline membrane disease.Am J Pathol 1976;82:241-58.
12 Anderson WR, Engel RR. Cardiopulmonary sequelae ofreparative stages of bronchopulmonary dysplasia. ArchPathol Lab Med 1983;107:603-8.
13 Rennard SI, Bitterman PB, Crystal RG. Mechanisms offibrosis. Am Rev Respir Dis 1984;130:492-6.
14 Ogden B, Murphy S, Saunders G, et al. Neonatal lungneutrophils and elastase/proteinase inhibitor inbalance. AmRev Respir Dis 1984;130:817-21.
15 Merritt TA, Cochrane CG, Holcomb K, et al. Elastase andalpha-l-proteinase inhibitor activity in tracheal aspiratesduring respiratory distress syndrome. Role of inflammationin the pathogenesis of bronchopulmonary dysplasia. J ClinInvest 1983;72:656-62.
16 Campbell EJ, Wald MS. Hypoxic injury to human alveolarmacrophages accelerates release of previously boundneutrophil elastase. Implications for lung connective tissueinjury including pulmonary emphysema. Am Rev RespirDis 1983;127:631-5.
17 Merritt TA, Hallman M. Interactions in the immature lung:protease-antiprotease mechanism oflung injury. In: MerrittTA, NorthwayWH Jr, Boynton BR, eds. Bronchopulmonarydysplasia. Boston: Blackwell, 1988:117-30.
18 Coalson JJ, Kuehl TJ, Escobedo MB, et al. A baboon modelof bronchopulmonary dysplasia. II. Pathologic features.Exp Mol Pathol 1982;37:335-50.
19 Bonikos DS, Bensch KG, Northway WH Jr. Oxygen toxicityin the newborn. The effect of chronic continuous 100 percent oxygen exposure on the lungs of newborn mice. Am JPathol 1976;85:623-50.
20 Edwards DK. The radiology of bronchopulmonary dysplasiaand its complications. In: Merritt TA, Northway WH Jr,Boynton BR, eds. Bronchopulmonary dysplasia. Boston:Blackwell, 1988:185-234.
21 Moylan FMB, Walker AM, Krammer SS, et al. Alveolarrupture as an independent predictor of bronchopulmonarydysplasia. Crit Care Med 1978;6:10-13.
22 Loeber NV, Morray JP, Kettrick RG, Downes JJ. Pulmonaryfunction in chronic respiratory failure of infancy. Crit CareMed 1980;8:596-601.
23 Motoyama EK, Fort MD, Klesh KW, et al. Early onset ofairway reactivity in premature infants with broncho-pulmonary dysplasia. Am Rev Respir Dis 1987;136:50-7.
24 Bryan MH, Hardie JJ, Reilly BJ, Swyer PR. Pulmonaryfunction studies during the first year of life in infantsrecovering from the respiratory distress syndrome. Pedi-atrics 1973;52:169-78.
25 Morray JP, Fox NW, Kettrick RG, Downes JJ. Improve-ment in lung mechanics as a function of age in the infantwith severe bronchopulmonary dysplasia. Pediatr Res1982;16:290-4.
26 Gerhardt T, Hehre D, Feller R, et al. Serial determination ofpulmonary function in infants with chronic lung disease.J Pediatr 1987-110:448-56.
27 Watt JL, Ariagno RL, Brady JL. Chronic pulmonary diseasein neonates after artificial ventilation: distribution ofventilation and pulmonary interstitial emphysema. Pedi-atrics 1977;60:273-81.
28 Harrod JR, L'Heureux P, Wangensteen OD, Hunt CE.Longterm follow up of severe respiratory distress syndrometreated with IPPB. J Pediatr 1974;84:277-86.
on 17 Novem
ber 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.10_Spec_N
o.1076 on 1 October 1990. D
ownloaded from
Bronchopulmonary dysplasia: then and now 1081
29 Melnick G, Pickoff AS, Ferrer PL, et al. Normal pulmonaryvascular resistance and left ventricular hypertrophy inyoung infants with bronchopulmonary dysplasia: an echo-cardiographic and pathologic study. Pediatrics 1980;66:589-96.
30 Berman W, Yabek SM, Dillon T, et al. Evaluation of infantswith bronchopulmonary dysplasia using cardiac catheteri-zation. Pediatrics 1982;70:708-12.
31 Abman SH, Warady BA, Lum GM, Koops BL. Systemichypertension in infants with bronchopulmonary dysplasia.J Pediatr 1984;104:928-31.
32 Smythe JA, Tabachnik E, Duncan WJ, et al. Pulmonaryfunction and bronchial hyper-reactivity in longterm sur-vivors of bronchopulmonary dysplasia. Pediatrics 1981;68:336-40.
33 Bader D, Ramos AD, Lew CD, et al. Childhood sequelae ofinfant lung disease: exercise and pulmonary functionabnormalities after bronchopulmonary dysplasia. J Pediatr1987;110:693-9.
34 Northway WH Jr, Moss RB, Carlisle KB, et al. Twenty-three year follow-up ofbronchopulmonary dysplasia (BPD).Pediatr Res 1989;25:370A.
35 Samet JM, Tager JB, Speizer FE. The relationship betweenrespiratory illness in childhood and chronic air flowobstruction in adulthood. Am Rev Respir Dis 1983;127:508-23.
36 Mortensson W, Lindroth M, Jonsson B, Sevnningsen U.Chest radiography and pulmonary mechanics in ventilatortreated low birth weight infants. Acta Radiologica: Diagnosis1983;24:71-9.
37 Groothius JR, Gutierrez KM, Lauer BA. Respiratory syn-cytial virus infection in children with bronchopulmonarydysplasia. Pediatrics 1988;82:199-203.
38 Markestad T, Fitzharding PM. Growth and developmentin children recovering from bronchopulmonary dysplasia.J7 Pediatr 1981;98:597-602.
39 Vohr BR, Bell EF, Oh W. Infants with bronchopulmonarydysplasia: growth pattern and neurologic and develop-mental outcome. Am J Dis Child 1982;136:443-7.
40 Sell EJ, Vaucher YE. Growth and neurodevelopmentaloutcome of infants who had bronchopulmonary dysplasia.In: Merritt TA, Northway WH Jr, Boynton BR, eds.Bronchopulmonary dysplasia. Boston: Blackwell, 1988:403-20.
41 Sauve RS, Singhal N. Longterm morbidity of infants withbronchopulmonary dysplasia. Pediatrics 1985;76:725-33.
42 Avery ME. Can RDS be eradicated. In: Raivo KO, HallmanN, Kouvalainen K, Valimaki I, eds. Respiratory distresssyndrome. New York: Academic Press, 1984:411-8.
43 Reynolds MS, Wallender KA. Use of surfactant in theprevention and treatment of neonatal respiratory distresssyndrome. Clin Pharm 1989;8:559-76.
44 Enhorning G, Shennan F, Possmayer E, et al. Prevention ofneonatal respiratory distress syndrome by tracheal instal-lation of surfactant: a randomized clinical trial. Pediatrics1985;76:145-53.
45 Kwong MS, Egan EA, Notter RH, et al. Double blindclinical trial of calf lung surfactant extract for the preven-tion of hyaline membrane disease in extremely prematureinfants. Pediatrics 1985;76:585-92.
46 Kendig JW, Notter RH, Cox C, et al. Surfactant replacementtherapy at birth: final analysis of a clinical trial andcomparison with similar trials. Pediatrics 1988;82:756-62.
47 Ten Centre study group. Ten Centre trial of artificial
See related papers on p 1082 and p 1089.
surfactant (artificial lung expanding compound) in verypremature babies. Br Med J 1987;294:991-6.
48 Horbar JD, Soil RF, Sutherland JM, et al. A multicenterrandomized placebo-controlled trial of surfactant therapyfor respiratory distress syndrome. N EnglJ Med 1989;320:959-65.
49 Dunn MS, Shennan AT, Hoskins EM, et al. Two yearfollowup of infants enrolled in a randomized trial ofsurfactant replacement therapy for prevention of neonatalrespiratory distress syndrome. Pediatrics 1988;82:543-7.
50 Halliday HL, McClure G, Reid MM. Growth and develop-ment two years after artificial surfactant replacement atbirth. Early Hum Dev 1986;13:323-7.
51 Vaucher YE, Merritt TA, HalUman M, et al. Neurodevelop-mental and respiratory outcome in early childhood afterhuman surfactant treament. Am J Dis Child 1988;142:927-30.
52 The HIFI study group. High frequency oscillatory ventilationcompared with conventional mechanical ventilation in thetreatment of respiratory failure in preterm infants. N EnglJ Med 1989;320:88-93.
53 Kao LC, Durand DJ, Phillips BL, et al. Oral theophyllineand diuretics improve pulmonary mechanics in infants withbronchopulmonary dysplasia. J Pediatr 1987;111:439-44.
54 Hendeles L, Weinberger M. Theophylline: a state of the artreview. Pharmacotherapy 1983;3:2-44.
55 Kao LC, Warburton D, Platzker ACG, et al. Effect ofisoproterenol inhalation on airway resistance in chronicbronchopulmonary dysplasia. Pediatrics 1984;73:509-14.
56 Logvinoff MM, Lemen RJ, Taussig LM, et al. Broncho-dilators and diuretics in children with bronchopulmonarydysplasia. Pediatr Pulmonol 1985;1: 198-203.
57 Cabal LA, Larrazabal C, Ramanathan R, et al. Effects ofmetaproterenol on pulmonary mechanics, oxygenation, andventilation in infants with chronic lung disease. J Pediatr1987;110:1 15-6.
58 Wilkie RA, Bryan MH. Effect of bronchodilators on airwayresistance in ventilator dependent neonates with chroniclung disease. J Pediatr 1987;111:278-82.
59 Katz R, McWilliams B. Bronchopulmonary dysplasia in thepediatric intensive care unit. Critical Care Clinics 1988;4:755-87.
60 Cummings JJ, Eugenio DB, Gross SJ. A controlled trial ofdexamethasone in preterm infants at high risk for broncho-pulmonary dysplasia. N Engl J Med 1989;320:1505-10.
61 Frank L, Sosenko IRS. Undernutrition as a major contribut-ing factor in the pathogenesis of bronchopulmonarydysplasia. Am Rev Respir Dis 1988;138:725-69.
62 Yeh TF, McClenan DA, Ajayi OA, et al. Metabolic rate andenergy balance in infants with bronchopulmonary dysplasia.Jf Pediatr 1989;114:448-51.
63 Koops BL, Abman SH, Accurso FJ. Outpatient managementand followup ofbronchopulmonary dysplasia. Clin Perinatol1984;11:100-22.
64 Abman SH, Burchell MF, Schaffer MS, et al. Late unexpecteddeaths in hospitalized infants with bronchopulmonarydysplasia. AmJ Dis Child 1989;143:815-9.
65 Werthammer J, Brown ER, Neff RK, et al. Sudden infantdeath syndrome in infants with bronchopulmonary dys-plasia. Pediatrics 1982;69:301-4.
66 Fiascone JM, Rhodes TT, Grandgeorge SR, et al. Broncho-pulmonary dysplasia: a review for the pediatrician. CurrProbl Pediatr 1989;19:177-227.
on 17 Novem
ber 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.10_Spec_N
o.1076 on 1 October 1990. D
ownloaded from