Embed Size (px)
Citation preview

S
TMa
b
c
d
a
ARR2A
KMIPC
1
Dusigtbpp
sf
1d
Journal of Clinical Virology 50 (2011) 125–129
Contents lists available at ScienceDirect
Journal of Clinical Virology
journa l homepage: www.e lsev ier .com/ locate / j cv
erological evidence of Merkel cell polyomavirus primary infections in childhood
ingting Chena, Lea Hedmana,d, Petri S. Mattilab, Tuomas Jartti c, Olli Ruuskanenc,aria Söderlund-Venermoa, Klaus Hedmana,d,∗
Department of Virology, Haartman Institute, University of Helsinki, BOX 21, FIN-00014, Helsinki, FinlandDepartment of Otorhinolaryngology, University of Helsinki and Helsinki University Central Hospital, Haartmaninkatu 4E, FIN 00290, Helsinki, FinlandDepartment of Pediatrics, Turku University Hospital, FIN 20520, Turku, FinlandDepartment of Virology and Immunology, Helsinki University Central Hospital Laboratory Division, Haartmaninkatu 3, FIN 00290, Helsinki, Finland
r t i c l e i n f o
rticle history:eceived 11 June 2010eceived in revised form9 September 2010ccepted 18 October 2010
eywords:erkel cell polyomavirus
gGrimary infectionhildhood
a b s t r a c t
Background: Merkel cell polyomavirus (MCPyV) was identified newly (2008) and is believed to be anetiologic factor of Merkel cell carcinoma (MCC). Recent molecular and serological data suggest that MCPyVinfection is common in the general population.Objectives: The aim of this study was to investigate the age of primary exposure to MCPyV.Study design: A MCPyV-IgG EIA was developed using the MCPyV major capsid protein VP1 expressedand self-assembled into virus-like particles (VLPs) in insect cells. The assay was used to detect serumIgG antibodies in two groups of children. Group 1 comprised paired and 5–8 year follow-up sera from217 children (3–13 years) with acute lower respiratory tract infection. Group 2 comprised sera from 158children (1–4 years) with otitis media; 86 children underwent adenoidectomy and 72 did not, whereafterfollow-up sera were obtained 3 years later.Result: The prevalence of MCPyV-IgG was 9% at 1–4 years, and increased to 35% at 4–13 years amongsubjects from Group 1, with a 33% seroconversion rate during 5–8 years. Among Group 2, the sero-
conversion rate was 16% during 3 years. The IgG prevalence at 4–7 years as well as the IgG levelsshowed an apparent gender difference, with male preponderance prevailing among the children withoutadenoidectomy.Conclusion: MCPyV primary infections occur ubiquitously in childhood, and the first exposure takes placeat young age. The serology showed no evidence for a causative role of MCPyV in lower respiratory tractinfection manifesting as acute wheezing, but was compatible with the notion of MCPyV persistence in tonsils.. Background
Merkel cell polyomavirus (MCPyV) is a small double-strandedNA virus recently identified in Merkel cell carcinoma (MCC), anncommon and aggressive skin cancer.1 The virus DNA has beenhown to be present in 24–89% of MCCs in populations of var-ed geographic origins,2–5 and integrated clonally into the MCCenome,1,6 strongly suggesting that the virus is an etiologic fac-
or in the pathogenesis of MCC. Recently, MCPyV DNA has alsoeen detected in the upper respiratory tracts of children and adults,ointing to an infection route shared by all human PyVs, and to theossibility of persistent carriage in tonsillar tissue.7–10Abbreviations: A, adenoidectomy; NA, without adenoidectomy.∗ Corresponding author at: Department of Virology, Haartman Institute, Univer-
ity of Helsinki, BOX 21, FIN-00014, Helsinki, Finland. Tel.: +358 9 19126473;ax: +358 9 19126491; mobile: +358 50 5249086.
E-mail address: [email protected] (K. Hedman).
386-6532/$ – see front matter © 2010 Elsevier B.V. All rights reserved.oi:10.1016/j.jcv.2010.10.015
© 2010 Elsevier B.V. All rights reserved.
So far only few serological studies have been carried outon MCPyV. Kean et al. set up an EIA based on a prokaryoticVP1 fusion protein antigen, and found a MCPyV-IgG prevalenceof 25–42% among the general population, with primary expo-sure in childhood.11 Tolstov et al. developed a conformationalcapsid epitope assay using virus like particles (VLPs) of coex-pressed VP1 and VP2 and found that patients with MCPyV-positiveMCC tumors as a rule have higher IgG levels than those withMCPyV-negative tumors.12 Two subsequent serological studies,with VP1 fusion protein and the other with VLPs confirmed theprevious ones.13,14 Also a highly sensitive neutralization assaywas developed to quantitate the MCPyV-specific antibodies inhumans.15
2. Objectives
The aims of this study were to develop serological assays basedon MCPyV VLPs generated in the baculovirus system by the cap-sid protein VP1 alone, to examine the conformational dependence

1 nical V
os
3
3
b2mahf(5sbct
pnwnwi1
3
iiSb(
3
Ia1pfsi1cwsawMES
3
acaTf
26 T. Chen et al. / Journal of Cli
f immunoreactivity, and to assess the antibody prevalence anderoconversion rates in pediatric populations.
. Study design
.1. Samples
Group 1: 217 pairs of sera were collected between Septem-er 2000 and May 2002 at the time of hospital admission and
weeks later from children (median age 1.6 years; range 3onths to 13 years) with lower respiratory tract infection and
cute wheezing.16–18 These children’s nasopharyngeal aspiratesave been examined by PCR for 18 respiratory viruses,18 and sera
or human bocavirus antibodies.16,19,20 For 72 of these childrenmedian age 2.0 years; range 0.3–3.4), follow-up sera were obtained–8 years later (median age 7.8 years; range 6–10). Altogether, 506era of this group were studied. The study protocol was approvedy the Ethics Committee of the Turku University Hospital, and thehildren were recruited only after obtaining informed concent fromhe guardian.
Group 2: 217 children aged 12–48 months with recurrent orersistent otitis media were randomly selected to undergo ade-oidectomy between March 2001 and December 2002 and the seraere collected at this time.21 From 158 children (86 with ade-oidectomy and 72 without), a 3-year (mean: 3.1) follow-up serumas available. The initial and follow-up sera from 158 children were
ncluded in this study. The gender and age distributions of Groupsand 2 are shown in Table S1.
.2. Plasmid and recombinant baculoviruses
Based on MCV339 (accession number EU375804), the VP1 cod-ng sequence was chemically synthesized (GenScript, USA). Formproved expression, the codon usage was optimized for that ofpodoptera frugiperda. Recombinant baculoviruses were generatedy the Bac-to-Bac system in accordance to the manufacturer’sInvitrogen) instructions.
.3. Virus-like particle production
Sf9 cells were infected with recombinant virus and grown innsect Express medium (Lonza, Basel, Switzerland) for 4–5 dayst 27 ◦C. Cell lysates were prepared by a two-step method. Lysis: the cell pellet was resuspended in buffer 1 (20 mM Tris–HCl,H 7.5; 150 mM NaCl; 1% Triton) and kept on ice for 10 min,ollowed by centrifugation at 10,000 × g for 10 min. Lysis 2: theupernatant was removed, and the pellet was resuspended in son-cation buffer (10 mM Tris–HCl, pH 8.0; 500 mM NaCl; 1 mM CaCl2;mM MgCl2; 0.01% Triton) supplemented with a protease inhibitorocktail (complete EDTA-free; Roche). After sonication, the lysateas collected by centrifugation at 13,000 rpm for 3 min. 1 ml of
onicate was centrifuged in 28% CsCl in a Beckman SW4Ti rotort 24,200 rpm at 4 ◦C for 48 h. The visible band containing VLPsas collected and dialysed three times against PBS. Expression ofCPyV VP1 and assembly of VLPs were confirmed by SDS-PAGE and
M. For use as antigen, the VLPs were biotinylated with the EZ-Linkulfo-NHS-LC-Biotinylation kit (Pierce, Rockford, IL) as described.16
.4. Dot blotting
The post-sonication lysate and the purified VLPs (before and
fter biotinylation) were examined by dot blotting. Briefly, nitro-ellulose membranes (Whatman Protran BA 85) spotted with thentigens were blocked in 5% BSA in Tris buffered saline with 0.1%ween 20 (TBS-T) for 30 min at ambient temperature. One serumrom a MCC patient and six sera from Group 2, with varying IgGirology 50 (2011) 125–129
levels in EIA, were diluted 1:100 and 1:500 in 0.1% BSA/TBS-T andkept on the membranes for 30 min. After washes with TBS-T, themembranes were treated with peroxidase-conjugated anti-humanIgG (DakoCytomation, Denmark) diluted 1:1000 in 5% BSA/TBS-Tfor 30 min. After washes with TBS-T, the bound antibody was visu-alized with 3,3′-diaminobenzidine (Sigma) and H2O2. To detectbiotinylated VLPs, the blocked membranes were incubated withhorseradish peroxidase-conjugated streptavidin (Dako, Glostrup,Denmark) at 1:10,000 in 5% BSA/TBS-T and visualized as above. Topre-denature the purified VLPs, 2% SDS was applied for 5 min at95 ◦C.
3.5. Antibody assay
The MCPyV IgG EIA was conducted essentially as those forparvovirus B19 or human bocavirus.16,20,22 Specific signal wasobtained by subtraction of antigen-free background as with ourparvovirus 4 IgG EIA.23 Briefly, the streptavidin-coated plates(Thermo Scientific) with the biotinylated VLPs (60 ng/well) wereprecoated with a sample diluent (Anilabsystems, Finland). Theserum samples diluted 1:200 were applied in duplicate and theabsorbances at 492 nm were recorded.
The MCPyV IgG EIA cut off values were calculated byabsorbances lower than 0.162 (Fig. S1). The lower cutoff(mean + 3SD) was 0.120 absorbance units and the higer cutoff(mean + 4SD) was 0.150 absorbance units. All sera with absorbancevalues above the lower cutoff were reexamined, and those withmean values exceeding the higher cutoff were considered MCPyVIgG positive. For the sera with mean values between the two cut-offs, VLP-competition assays12 were performed to distinguish truefrom false positivity.
3.6. Statistics
The seroprevalence and seroconversion rate differencesbetween males and females were compared by logistic regression.OD values were compared by a non parametric Mann–Whitneytest with the tied P-value used. The seronegative subjects weregiven the OD value = 0 and seropositive subjects were given themeasured OD values.
4. Results
4.1. Expression and purification of MCPyV VP1-VLPs
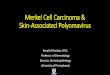
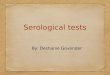
The synthetic MCPyV339 VP1 gene was cloned into a recombi-nant baculovirus and expressed in Sf9 cells. After 4 days of culture,a major protein band of 46 KDa was seen in SDS-PAGE of the wholecell lysate, and as the sole constituent of the CsCl gradient-purifiedmaterial (Fig. 1). In EM, the purified VLPs had an icosahedral shape,and diameter of 42–58 nm, as shown in Fig. 2.
4.2. Conformational dependence of VP1-VLP antibodies
Immunoreactivity of the purified VP1-VLPs – before and afterbiotinylation – with human IgG (7 sera with varying IgG levels)was examined with dot-blotting, in native vs. denaturing condi-tions. The EIA-seropositive samples showed strong reactivity withthe native as well as the biotinylated VLPs that had been han-dled before and during the assay in nondenaturing conditions, but
showed no reactivity with the same VLPs that had been denatured(Fig. 3). The EIA-seronegative samples showed in correspondingexperiments uniformly negative results. Peroxidase-streptavidinverified the presence of the biotinylated antigens before and afterdenaturation (Fig. 3).
T. Chen et al. / Journal of Clinical Virology 50 (2011) 125–129 127
Fig. 1. Detection of MCPyV VP1 expression by Coomassie blue staining in VP1-Bac-infected Sf9 cells. Lane1: the whole cell lysate, lane 2: the supernatant of firstlysis, lane 3: the supernatant of second lysis, lane 4: puried MCPyV VLPs after CsClultracentrifugation, lane 5: GST-Bac-infected control Sf9 cells, arrow: MCPyV VP1.
Fig. 2. EM of recombinant MCPyV VP1 virus like particles. Scale bar = 200 nm.
Table 1MCPyV- IgG seroprevalence among wheezing children.
Age (years) Male Female Total
>0, ≤0.5 0/19 (0%) 1/11 (9%) 1/30 (3%)>0.5, ≤1 1/14 (7%) 0/7 (0%) 1/21 (5%)
4
Mshtt
Fig. 3. Dot blotting for conformational dependence of MCPyV IgG reactivity; (a) and(b) human serum samples diluted at 1:100 and 1:500. A: sonication lysate of VP1-Bac-infected Sf9 cells; B: purified MCPyV VLPs; C: cell lysate of GST-Bac-infected Sf9cells; D: denatured puried MCPyV VLPs; 1: human serum 606A, EIA-seropositive;2: human serum 3011, EIA-seropositive; 3: human serum 3002, EIA-seronegative;4: human serum 3004, EIA-seronegative. (c) A: purified MCPyV VLPs; B: denaturedpuried MCPyV VLPs; C: biotinylated purified VLPs; D: denatured biotinylated puri-fied VLPs; 1–7: human serum samples with series of OD values tested in EIA. Humanserum diluted at 1:500; 8: biotinylated VLPs detected by peroxidase-streptavidin.
Table 3aMCPyV-IgG seroprevalence in Subgroup A (adenoidectomy) and Subgroup NA (noadenoidectomy).
Serum 0 Serum 3 Seroconversion
n IgG + (n) Rate IgG + (n) Rate n Rate
Subgroup A 86 3 3% 14 16% 11 13%
Among 158 initial (median age 1.8, range 1.0–4.0 years) serafrom Group 2, 6 (4%) contained MCPyV IgG (Table 3). During 3-year
TM
>1, ≤2 4/52 (8%) 3/27 (11%) 7/79 (9%)>2, ≤4 4/35 (11%) 2/26 (8%) 6/61 (10%)>4, ≤13 5/17 (29%) 4/9 (44%) 9/26 (35%)
.3. IgG seroreactivity among wheezing children
Overall, among the 217 children of Group 1, 11% (24/217) wereCPyV-IgG seropositive. The IgG prevalence with respect to age is
hown in Table 1. In the infants below one year of age, only 4% (2/51)
ad IgG, possibly of maternal origin. The seroprevalence increasedo 9% among the children aged 1–2 years (n = 79), and to 35% amonghose (n = 26) aged 4–13 years.able 2CPyV-IgG seroconversion rates among wheezing children.
Age years 1st-sera n n. IgG-1st-sera Mean ye
>0, ≤1 20 20 6.32>1, ≤2 36 33 6.47>2, ≤3 15 14 6.48Total 71 67 6.44
Subgroup NA 72 3 4% 15a 21% 13 19%Total 158 6 4% 29 18% 24 16%
a One initially positive child was negative at 3-year follow-up.
Follow-up samples obtained 5–8 years after the initial pair wereavailable for 72 children (at median age 7.8 years, range 6–11). Theinitial (at age 0–3 years) MCPyV IgG positivity rate of 6% in thesechildren rose to 37% (26/71) during follow-up. Of note, among the67 children that in the first samples were seronegative, 22 (33%)seroconverted during observation (Table 2).
4.4. IgG seroreactivity among adenoidectomy and controlchildren
(mean: 3.1) follow-up, the seropositivity increased to 18%. Of theinitially seronegative children, 16% seroconverted during an aver-age of 3 years (age range 3.9–7.3 years). The IgG prevalence and
ars of follow up n. IgG + follow up Seroconversion rate
5 5/20 (25%)15 12/33 (36%)
6 5/14 (36%)26 22/67 (33%)

128 T. Chen et al. / Journal of Clinical Virology 50 (2011) 125–129
0 %
5 %
10 %
15 %
20 %
25 %
30 %Subgroup A
Subgroup NA
total
(a)
0 %
5 %
10 %
15 %
20 %
25 %female
male
total
(b)
A. (b)
ssnsif2
q((iN3wm
5
gVal
MeMiwshsd
t
TC(
European pediatric populations. The seroprevalence was 9% among79 wheezing children of 1–2 years, and 35% among those aged4–12 years. These findings are consistent with previous reports onthe presence of MCPyV IgG in childhood, though lower than the
0
1
2
3
Optical D
ensity U
nits
Female, serum 0
Male, serum 0
Female, serum 3
Male, serum 3
mean
(a)
3
s
Female Male MaleFemale
serum 0 serum 3
(b)
Fig. 4. (a) Comparison of IgG positivity rates in Subgroup A and Subgroup N
eroconversion rates in Subgroup A and Subgroup NA showed notatistically significant differences (Fig. 4a; Table 3a). As opposed too significant difference between males and females in the initialera, apparent gender differences were seen during follow-up bothn IgG seroprevalence and IgG seroconversion rates (male 89 vs.emale 69, P = 0.08); these respective figures for males were 22% and0%, as opposed to 13% and 10% for females (Fig. 4b and Table 3b).
Besides the seroprevalence and seroconversion rates, also theuantities of MCPyV-IgG at the end of follow-up tended to be higherP = 0.1) in males (mean OD value 0.751, SD 0.825) than in femalesmean OD value 0.464, SD 0.411). Of note, the gender differencen the OD values at 3-year follow-up was significant in SubgroupA (P = 0.044), but not among Subgroup A (P = 0.7). Furthermore, at-year follow-up, the children with the highest MCPyV IgG levelsere males; for example, all five subjects with OD > 1.5 units wereales (Fig. 5).
. Discussion
We developed a MCPyV-IgG EIA based on virus like particlesenerated in the baculovirus system by MCPyV capsid proteinP1 alone, examined the conformational dependence of the VLPntigenicity by immunoblotting, and assessed by EIA the seropreva-ences among two groups of children followed up for several years.
Tolstov et al. first produced MCPyV VLPs by coexpression ofCV339 VP1 and VP2, and acquired VLPs with a uniform diam-
ter of 55–58 nm.12 Recently, Touzé et al. succeeded in generatingCPyV VLPs of VP1 alone using the MKT21 strain, with the codon
dentical to that of MCV339.14 Our VLPs were of the strain MCV339,hich is homologous to the strains recently identified in healthy
kin.24 In EM our VLPs had a diameter of 42–58 nm, similar to otheruman polyomavirus VLPs with a diameter of 45–50 nm,25 but
lightly different from Touzé’s of 20–45 nm, a difference possiblyue to staining.We fractionally purified the VLPs by modifying Bodaghi’swo-step method,25 in which the cytosolic and nuclear lysates
able 3bomparison of IgG positivity rates between males and females from Group 2P = 0.08).
Serum 0 Serum 3 Seroconversion
n IgG + (n) Rate IgG + (n) Rate n Rate
Male 89 4 4% 20a 22% 17 20%Female 69 2 3% 9 13% 7 10%Total 158 6 4% 29 18% 24 16%
a One initially positive male child was negative at 3-year follow-up.
Comparison of IgG positivity rates between males and females in Group 2.
are prepared separately. Interestingly, our VP1-VLPs were barelyreleased in the hypotonic buffer with detergent (cytosolic), butabundantly after sonication (nuclear). This points to nuclear local-ization, as with JC and BK polyomaviruses, the VLPs of whichassemble in the nucleus.25,26
We furthermore disclosed the conformational dependence ofMCPyV antibodies with dotblotting. With peptide library screeningand Western blotting, Tolstov et al. reached a similar conclusion.12
Recent serological studies showed that MCPyV infection is com-mon in the general population, and suggested that first exposuremay occur at a young age.11,12 To investigate the time and extentof primary exposure in more detail, we followed up two Northern
0
1
2
Optical D
ensity U
nit
Subgroup A, female
Subgroup A, male
Subgroup NA, female
Subgroup NA, male
A A NA NA
serum 0 serum 3
Fig. 5. Dot plot of OD values of MCPyV- IgG positive serum samples in Group 2. (a)Comparison of positive OD values between males and females from Subgroup A andSubgroup NA. Bars: mean OD values. (b) Comparison of positive OD values in Group2. Serum 0: first sera; serum 3: 3-year follow-up sera. A: with adenoidectomy; NA:without adenoidectomy.

nical V
22awengdiMwn
ohAgtsmi
C
A
ttAF
tM
A
t
R
T. Chen et al. / Journal of Cli
0.5% of Kean et al. at 1–5 years and the 43% of Tolstov et al. at–5 years. We showed that almost one third of children seroneg-tive at <3 years of age serocoverted during 5–8 years, similar tohat has been shown for other human polyomaviruses.11,27,28 Sev-
ral recent studies have shown the presence of MCPyV DNA inon-tumor tissues including upper airways7–10 and upper aerodi-estive tract,29 pointing to respiratory transmission. However, ourata showing no seroconversions in the paired sera obtained dur-
ng acute wheezing16,18 rule strongly against a causative role forCPyV in lower respiratory tract infection manifesting as acuteheezing. A similar conclusion has been reached for the other twoewly found polyomaviruses KIPyV and WUPyV.28,30
Interesting gender differences were seen in the children withtitis media at 3-year follow-up. The males showed apparentlyigher seroconversion and seroprevalence rates than the females.mong the children who had not undergone adenoidectomy, theender difference in IgG levels was statistically significant. Whetherhe explanation is behavioral or microbiological remains to behown. That the highest MCPyV-IgG levels occurred among theales without adenoidectomy is in line with our earlier PCR find-
ngs suggesting long-term persistence of MCPyV in tonsillar tissue.7
onflict of interest
None.
cknowledgments
This study was supported by Helsinki University Central Hospi-al Research and Education, and Research and Development Funds,he Sigrid Jusélius Foundation, the Medical Society of Finland, thecademy of Finland (project 1122539), and the Turku Universityoundation (OR).
Note: After this work was completed and submitted for publica-ion, a new human polyomavirus TSPyV was identified by van der
eijden (PLoS Pathog 2010; 6:e1001024).
ppendix A. Supplementary data
Supplementary data associated with this article can be found, inhe online version, at doi:10.1016/j.jcv.2010.10.015.
eferences
1. Feng H, Shuda M, Chang Y, Moore PS. Clonal integration of a polyomavirus inhuman Merkel cell carcinoma. Science 2008;319:1096–100.
2. Foulongne V, Kluger N, Dereure O, Brieu N, Guillot B, Segondy M. Merkelcell polyomavirus and Merkel cell carcinoma, France. Emerg Infect Dis2008;14:1491–3.
3. Becker JC, Houben R, Ugurel S, Trefzer U, Pföhler C, Schrama D. MC polyomavirusis frequently present in Merkel cell carcinoma of European patients. J InvestDermatol 2009;129:248–50.
4. Ridd K, Yu S, Bastian BC. The presence of polyomavirus in non-melanoma skincancer in organ transplant recipients is rare. J Invest Dermatol 2009;129:250–2.
5. Garneski KM, Warcola AH, Feng Q, Kiviat NB, Leonard JH, Nghiem P. Merkel cellpolyomavirus is more frequently present in North American than AustralianMerkel cell carcinoma tumors. J Invest Dermatol 2009;129:246–8.
6. Shuda M, Feng H, Kwun HJ, Rosen ST, Gjoerup O, Moore PS, et al. T antigenmutations are a human tumor-specific signature for Merkel cell polyomavirus.Proc Natl Acad Sci U S A 2008;105:16272–7.
irology 50 (2011) 125–129 129
7. Kantola K, Sadeghi M, Lahtinen A, Koskenvuo M, Aaltonen LM, MöttönenM, et al. Merkel cell polyomavirus DNA in tumor-free tonsillar tissues andupper respiratory tract samples: implications for respiratory transmission andlatency. J Clin Virol 2009;45:292–5.
8. Bialasiewicz S, Lambert SB, Whiley DM, Nissen MD, Sloots TP. Merkel cell poly-omavirus DNA in respiratory specimens from children and adults. Emerg InfectDis 2009;15:492–4.
9. Goh S, Lindau C, Tiveljung-Lindell A, Allander T. Merkel cell polyomavirus inrespiratory tract secretions. Emerg Infect Dis 2009;15:489–91.
10. Babakir-Mina M, Ciccozzi M, Lo Presti A, Greco F, Perno CF, Ciotti M. Identi-fication of Merkel cell polyomavirus in the lower respiratory tract of Italianpatients. J Med Virol 2010;82:505–9.
11. Kean JM, Rao S, Wang M, Garcea RL. Seroepidemiology of human poly-omaviruses. PLoS Pathog 2009;5:e1000363.
12. Tolstov YL, Pastrana DV, Feng H, Becker JC, Jenkins FJ, Moschos S, et al. HumanMerkel cell polyomavirus infection II. MCV is a common human infection thatcan be detected by conformational capsid epitope immunoassays. Int J Cancer2009;125:1250–6.
13. Carter JJ, Paulson KG, Wipf GC, Miranda D, Madeleine MM, Johnson LG, et al.Association of Merkel cell polyomavirus-specific antibodies with Merkel cellcarcinoma. J Natl Cancer Inst 2009;101:1510–22.
14. Touzé A, Gaitan J, Arnold F, Cazal R, Fleury MJ, Combelas N, et al. Generationof Merkel cell polyomavirus virus-like particles and their application to thedetection of MCV antibodies. J Clin Microbiol 2010;48:1767–70.
15. Pastrana DV, Tolstov YL, Becker JC, Moore PS, Chang Y, Buck CB. Quantita-tion of human seroresponsiveness to Merkel cell polyomavirus. PLoS Pathog2009:e1000578.
16. Söderlund-Venermo M, Lahtinen A, Jartti T, Hedman L, Kemppainen K, Lehti-nen P, et al. Clinical assessment and improved diagnosis of bocavirus-inducedwheezing in children, Finland. Emerg Infect Dis 2009;15:1423–30.
17. Allander T, Jartti T, Gupta S, Niesters HG, Lehtinen P, Osterback R, et al.Human bocavirus and acute wheezing in children. Clin Infect Dis 2007;44:904–10.
18. Jartti T, Lehtinen P, Vuorinen T, Osterback R, van den Hoogen B, Oster-haus AD, et al. Respiratory picornaviruses and respiratory syncytial virus ascausative agents of acute expiratory wheezing in children. Emerg Infect Dis2004;10:1095–101.
19. Kantola K, Hedman L, Allander T, Jartti T, Lehtinen P, Ruuskanen O, et al. Sero-diagnosis of human bocavirus infection. Clin Infect Dis 2008;46:540–6.
20. Hedman L, Söderlund-Venermo M, Jartti T, Ruuskanen O, Hedman K. Datingof human bocavirus infection with protein-denaturing IgG-avidity assays-secondary immune activations are ubiquitous in immunocompetent adults.J Clin Virol 2010;48:44–8.
21. Hammarén-Malmi S, Saxen H, Tarkkanen J, Mattila PS. Adenoidectomy doesnot significantly reduce the incidence of otitis media in conjunction with theinsertion of tympanostomy tubes in children who are younger than 4 years: arandomized trial. Pediatrics 2005;116:185–9.
22. Kaikkonen L, Lankinen H, Harjunpää I, Hokynar K, Söderlund-Venermo M,Oker-Blom C, et al. Acute-phase-specific heptapeptide epitope for diagnosisof parvovirus B19 infection. J Clin Microbiol 1999;37:3952–6.
23. Lahtinen A, Kivelä P, Hedman L, Kumar A, Kantele A, Lappalainen M, et al.Serodiagnosis of Primary Infections with Human Parvovirus 4. Emerg Infect Dis2011;17. doi:10.3201/eid1701.100750.
24. Schowalter RM, Pastrana DV, Pumphrey KA, Moyer AL, Buck CB. Merkel cellpolyomavirus and two previously unknown polyomaviruses are chronicallyshed from human skin. Cell Host Microbe 2010;7:509–15.
25. Bodaghi S, Comoli P, Bösch R, Azzi A, Gosert R, Leuenberger D, et al. Antibodyresponses to recombinant polyomavirus BK large T and VP1 proteins in youngkidney transplant patients. J Clin Microbiol 2009;47:2577–85.
26. Li TC, Takeda N, Kato K, Nilsson J, Xing L, Haag L, et al. Characterization ofself-assembled virus-like particles of human polyomavirus BK generated byrecombinant baculoviruses. Virology 2003;311:115–24.
27. Nguyen NL, Le BM, Wang D. Serologic evidence of frequent human infectionwith WU and KI polyomaviruses. Emerg Infect Dis 2009;15:1199–205.
28. Kantola K, Sadeghi M, Ewald MJ, Weissbrich B, Allander T, Lindau C, et al.Expression and serological characterization of polyomavirus WUPyV and KIPyVstructural proteins. Viral Immunol 2010;23:385–93.
29. Loyo M, Guerrero-Preston R, Brait M, Hoque MO, Chuang A, Kim MS, et al.Quantitative detection of Merkel cell virus in human tissues and possible modeof transmission. Int J Cancer 2010;126:2991–6.
30. Norja P, Ubillos I, Templeton K, Simmonds P. No evidence for an associationbetween infections with WU and KI polyomaviruses and respiratory disease. JClin Virol 2007;40:307–11.