Embed Size (px)
Citation preview

CLINICAL MICROBIOLOGY REVIEWS, JUly 1990, p. 247-268 Vol. 3, No. 30893-8512/90/030247-22$02.00/0Copyright © 1990, American Society for Microbiology
Serology of CoccidioidomycosisDEMOSTHENES PAPPAGIANIS* AND BARBARA L. ZIMMER
Department of Medical Microbiology and Immunology, School of Medicine, University of California,Davis, California 95616
INTRODUCTION ..................................... 247NATURE OF C. IMMITIS..................................... 247SPECTRUM OF DISEASE ..................................... 248HOST RESPONSE TO C. IMMITIS ..................................... 249
Allergy..................................... 249Antibody..................................... 250
ANTIGEN PREPARATION AND ANALYSIS ..................................... 254Historical Development......................................254Subcellular Localization..................................... 255Antigen Characterization ..................................... 256
BODY FLUIDS TESTED..................................... 257SEROLOGIC TESTS..................................... 258
Detection of Early Precipitin IgM Antibody ..................................... 258TP..................................... 258ID..................................... 258LA..................................... 260
Detection of the CF IgG Antibody ..................................... 260CF..................................... 260IDCF..................................... 260QID ..................................... 261
Miscellaneous/Experimental Tests for Antibody ..................................... 261Agar gel precipitation-inhibition test ..................................... 261CIE..................................... 261FA..................................... 261RIA..................................... 262ELISA..................................... 262
CROSS-REACTIVITY..................................... 263ANTIGEN DETECTION ..................................... 263EXOANTIGEN TESTING ..................................... 264FUTURE DIRECTIONS..................................... 264ACKNOWLEDGMENT ..................................... 264LITERATURE CITED..................................... 264
INTRODUCTION
The terricolous fungus Coccidioides immitis is well en-sconced in the soil of the New World. The expanding humanand nonhuman populations of the Sun Belt area of thesouthwestern United States and of other endemic regionsprovide a continuing supply of individuals who are suscep-tible to infection with C. immitis.
Serologic tests have served for several decades as aids inthe diagnosis and management of coccidioidomycosis.Among the serologic tests available for the mycoses, thosefor coccidioidomycosis have been the most reliable (139,141). These have proved useful in veterinary as well ashuman medicine (101, 122).The following serologic tests have been used for diagnos-
ing coccidioidomycosis: complement fixation (CF); precip-itin reaction in several versions, i.e., tube precipitin (TP),immunodiffusion TP (IDTP), IDCF, and quantitative IDCF(QIDCF), agar gel precipitin-inhibition test, and counterim-munoelectrophoresis (CIE); latex particle agglutination(LA); fluorescent antibody (FA); radioimmunoassay (RIA);
* Corresponding author.
and, more recently, enzyme-linked immunosorbent assay(ELISA).
NATURE OF C. IMMITIS
C. immitis exists in nature and in the usual culture mediain its saprobic form: septate hyphae 2 to 4 Rm in diameterwhich, in 5 to 7 days, yield a chain of multinucleate arthro-conidia which usually alternate with smaller, nonviable,brittle cells (Fig. 1). The latter degenerate, thus releasing thearthroconidia, which readily become airborne. The arthro-conidia can germinate to yield new hyphae or can serve asthe form infecting humans and other hosts. When inhaled,the arthroconidia, in the presence of the phagocytic cells (42)and increased CO2 (80), convert into a different morphologicform. Shedding an outer wall layer and all but one nucleus,the arthroconidia round up and enlarge to produce animmature spherule. The nucleus undergoes division, whichis followed by partitioning of the cytoplasm by inwardextension of the cell wall. Completion of the nuclear divisionand segmentation produce a mature spherule with endo-spores within 48 h in vivo and at 30 to 96 h in vitro.Following the segmentation, the endospores become
247
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

248 PAPPAGIANIS AND ZIMMER
ARTHROCONIDIA
LIFE CYCLE ofCoccidioides immitis
FIG. 1. Various morphologic forms of C. immitis.
rounded within the mature spherule. The spherule wallcontains glucans and chitin, which are also found in theendospore wall (50), as well as polymers containing man-nose, 3-O-methylmannose, and galactose, as described byWheat et al. (150) and Cole et al. (19). The spherule thenopens to release the endospores, which, in vivo, enlarge toform endosporulating spherules repeating the cycle: spher-ule -> endospore -- spherule. The mechanism of release ofthe endospores from spherules has not been established;however, in cultures, chitinase and glucanases become de-tectable at about the time that endospores are released (R. F.Hector, B. L. Zimmer, and D. Pappagianis, Abstr. Annu.Meet. Am. Soc. Microbiol. 1985, F61, p. 374; B. L. Zimmerand D. Pappagianis, Abstr. Annu. Meet. Am. Soc. Micro-biol. 1987, F48, p. 397). Shortly thereafter, protease(s)becomes detectable in culture medium and increases as thechitinase and glucanases diminish in concentration (102, 123)and could therefore influence the morphologic evolution ofC. immitis. This phenomenon has not yet been demon-strated. Cole et al. (23) proposed that the protease(s) servesa role in morphogenesis.On occasion, the hyphal form and even arthroconidia have
been observed in vivo. For example, hyphae are sometimesseen in coccidioidal pulmonary cavities and infrequently intissues other than lung (94, 152).At least two kinds of antibody (discussed later) are pro-
duced in response to infection with C. immitis: an earlyantibody detected by TP, IDTP, and LA; and a later anti-body detected by CF and IDCF.
SPECTRUM OF DISEASE
Coccidioidomycosis may be manifest or occult. It may bewithout apparent detriment to the host, or it may progress todeath in an insidious or fulminating manner. No case ofrespiratory human-to-human transmission has been re-ported.
In the noncompromised host, infection is followed bysymptoms in about 40% of patients. The approximately 60%of persons who are without acknowledged symptoms can bedetected by a positive skin test with coccidioidal antigen; insome, detection of prior coccidioidal infection results whena pulmonary lesion is detected by routine chest roentgeno-gram, and subsequent laboratory tests confirm its etiology.Smith et al. (139) found only 7% seropositivity in a smallsample of asymptomatic skin test converters without evi-dence of disease.
In those who develop symptoms, onset of illness occurs 7to 28 days (usually 10 to 16 days) after exposure to arthro-conidia of C. immitis. The disease can be roughly catego-rized as (i) primary acute (pulmonary) disease, (ii) dissemi-nated (metapulmonary) disease, and (iii) pulmonary residua.
Early in the course of disease various rashes may occur,the most prominent of which is erythema nodosum. Thistransient eruption lasts only a few days and may be the resultof formation of immune complexes present for only a shortperiod of time. Its occurrence usually is associated with agood prognosis, but disseminated coccidioidomycosis hasfollowed erythema nodosum. Some rashes appear as ur-
CLIN. MICROBIOL. REV.
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

SEROLOGY OF COCCIDIOIDOMYCOSIS 249
0°r090
7~6J
30
2pI0
0
SKIN TEST
-~~ ~ ~ ~ ~ ~ ~ ~ .
f~~~~~~~.-;D -e---
I ,'~~~~~~~~~~~~~I4 CCF
I#Ar
aI I I I1 2 3 4 5 6
WEEK OF ILLNESS
I-7 8
., CF
PRECIP
I I I I
1 2 3 4 5 6 7MONTH OF ILLNESS
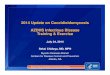
FIG. 2. Temporal sequence of immunologic changes in primary nondisseminating coccidioidomycosis. Precip, Tube precipitins; CF,complement-fixing antibodies. After Smith (135) and Smith et al. (100, 139, 141), with permission of the publishers.
ticaria, suggesting a histamine-releasing mechanism; how-ever, an immunoglobulin E (IgE)-mediated reaction has notbeen demonstrated with these early brief rashes. Cox et al.(27) have related increased anticoccidioidal IgE to moresevere coccidioidal disease. Peripheral eosinophilia may beseen: the higher the eosinophilia, the worse the prognosis;pulmonary eosinophilia also is seen (90).The usual primary pulmonary disease can present in a
variety of forms, often with hilar lymphadenopathy, andsometimes with pleural or pleuropericardial effusion. Occa-sionally no pulmonary lesions are detected by standardroentgenography (newer computerized axial tomography(CAT) and magnetic resonance imaging (MRI) examinationmay reveal them), and hilar lymphadenopathy alone may bedetected. Complete resolution of the primary pulmonarydisease usually occurs; however, some 5 to 10% of sympto-matic primary pulmonary coccidioidomycosis is followed bypersistence of a pulmonary residual (cavity, solitary nodule,or bronchiectasis). In a few patients the primary pulmonaryinfection may be sufficiently extensive or severe to causedeath (56, 126). Because recovery from infection usuallyresults in resistance to exogenous second infection, vaccineshave been developed which have a protective effect in somespecies (89), but these have not yet been shown to protecthumans (D. Pappagianis and the Vaccine Study Group,Program Abstr. 26th Intersci. Conf. Antimicrob. AgentsChemother., abstr. no. 784, 1986).
In a small fraction of patients with symptomatic disease,C. immitis spreads outside the thorax. Dissemination occurswithin weeks of the primary pulmonary infection but may bedelayed (or manifestation of spread may be delayed) forsome months, infrequently for years. Metapulmonary spreadis usually evident from the development of some metastaticlesion, but occult dissemination has also been reported (6,117). The endocardium and intestinal mucosa are rarelyaffected (149); virtually all other tissues can be affected.Metastasis may be represented by a single pustular lesion inthe skin or by extensive involvement of many organs andtissues. The meningeal form of coccidioidomycosis repre-sents the worst form of the disease, always leading to deathif untreated; therapy for this form is often only partiallyeffective.The frequency of dissemination is increased by certain
risk factors: ethnic background (Filipino and other Asiansand African Americans appear at greater risk than other
groups); acquisition of a primary acute infection during thelater stages of pregnancy; and immunosuppressive states(iatrogenic as in renal transplantation; or acquired immuno-deficiency state, such as acquired immunodeficiency syn-drome (AIDS) or lymphoma). While complete recovery fromprimary infection is usually followed by lasting resistance toexogenous reinfection, such resistance may be diminishedby a superimposed immunosuppressive condition leading toexacerbation and dissemination of the disease previouslyconsidered healed (35, 99). In the immunocompromisedhost, progression of the disease is often more rapid than inthe noncompromised host.
Certain forms of disseminated disease, e.g., osseous orjoint involvement, appear to undergo partial resolution onlyto become clinically evident later, and such improvementand worsening may occur repeatedly for many years.
In most cases of coccidioidomycosis, serologic findingsare of help in diagnosis and prognosis. Occasionally, sero-logic failures are recognized in patients with certain immu-nocompromising states or when progression of disseminateddisease is very rapid and antibody is not detected.
HOST RESPONSE TO C. IMMITIS
Allergy
The host generates delayed cutaneous hypersensitivity tococcidioidin or spherulin (see below) within 3 days to 3weeks after onset of symptoms (10 days to 6 weeks afterexposure). A positive skin test indicates current or priorinfection, but only conversion from negative to positivedemonstrates the former. Some individuals produce an im-mediate wheal and erythema reaction but this may be eitherto the coccidioidal antigen or to the preservative thimerosal.Smith et al. (142) could show no passive transfer (Prausnitz-Kustner test) of immediate-type hypersensitivity from fiveindividuals with current and prior coccidioidal infections andpositive coccidioidin skin tests to coccidioidin-negative re-cipients. In these studies (142), it was apparent that, inprimary nondisseminating coccidioidomycosis, skin reactiv-ity to coccidioidin usually preceded by a few days theformation of early antibody (detected by TP test), which inturn was followed by development of CF antibodies (139,141) (Fig. 2). In recent years, for unknown reasons, early
100
90
r 80n 70
0.0 50
u. 400
z,20
w 10a.
0
VOL. 3, 1990
I
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

250 PAPPAGIANIS AND ZIMMER
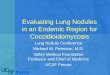
FIG. 3. TP test. Left tube contains human serum plus undilutedcoccidioidal antigen, middle tube contains serum plus coccidioidalantigen diluted 1:10, and right tube contains serum plus culturemedium control. The button of precipitate has been dislodged fromthe bottom of the tube for photographic clarity. Reprinted fromreference 159 with the permission of the publisher.
antibody has often been detected in the serum at a time whenthe skin test has been negative. In part, this may be due toimprovement in tests such as LA and ID that are moresensitive in detecting antibody than the TP test (60, 61, 65).A negative skin test does not rule out coccidioidomycosisand should not preclude serologic and other tests (biopsy orculture) to detect the disease. Ordinarily, if a patient has hada positive coccidioidal skin test for several months or longerand develops an illness accompanied by negative serology,the illness is not likely coccidioidal except in the immuno-suppressed patient whose skin test reactivity has faded andin whom serologic reactivity never developed. Administra-tion of a coccidioidal skin test does not induce or increasethe titer of coccidioidal antibody (34, 113, 142).
Antibody
Over a 15-year period, the serologic studies of Smith et al.(139, 141) involved some 39,500 tests on patients, including5,579 with primary nondisseminating coccidioidal infections,722 with disseminated infections, 271 with noncavitatingpulmonary residuals, and 577 with pulmonary cavities. Thetemporal sequence of antibody detected by TP (Fig. 3) andCF tests has been described above. Rarely, the CF antibodyis detected before TP. The antigens differ in that the TPantigen is heat stable, retaining potency even after autoclav-ing, whereas the CF antigenic activity is destroyed by heat.Subsequent studies making use of immunoelectrophoresis
indicated that the major antibodies involved are IgM in theTP and IgG in the CF reactions (109, 128).
In 1958, Heiner (51) showed that, when coccidioidin andserum from a patient with coccidioidomycosis diffuse towardeach other in an agar gel immunodiffusion test, a band ofprecipitate forms. Various fractions derived from coccidioi-din yielded multiple bands when diffused toward humanpatients' sera (111). Schubert and Hampson (132) demon-strated an ID reaction between human serum and coccidi-oidin. Huppert and Bailey (60, 61) refined the ID test anddemonstrated that, in the gel milieu, reactions correspondingto the TP and CF reactions (IDTP and IDCF, respectively)could be detected (Fig. 4). This observation posed theseeming paradoxes that the CF antigen-antibody reaction,which produces no precipitate in liquid, forms a precipitatein a gel (complement is not required for this); nor do the TPand IDTP reactions involving IgM require intact comple-ment despite the usual description of IgM as more efficientthan IgG in binding complement. The ability of CF antibodyto form a precipitate in a gel has created some confusionbecause the reaction has been referred to correctly as a"precipitin" reaction; however, the clinical and temporaldefinition of a precipitin (139, 141) has been that of the earlyIgM antibody response detected by TP test. Therefore, somelaboratories may report the presence of precipitins detectedby ID and mean a reaction produced by IgG (Fig. 4, bottom)from a patient with a longstanding coccidioidal infectionrather than IgM produced during a recent primary coccidi-oidal infection.The data depicted in Fig. 2 indicate that it is important to
test for IgM antibody as this may be the only means ofreadily confirming the presence of an early acute coccidioi-dal infection. Smith et al. (134, 136) found that during thefirst week of illness 53% of patients with primary nondissem-inating coccidioidomycosis had detectable antibody by TP(of a subgroup who had erythema nodosum, 75% were TPpositive within week 1 of illness); this percentage increasedto a maximum of 91% during weeks 2 and 3 of illness. TheIDTP and LA tests showed a greater sensitivity than the TPtest in detecting early antibody (61, 62, 65; D. Pappagianis,S. Lindsay, and S. Beall, Abstr. Annu. Meet. Am. Soc.Microbiol. 1986, F19, p. 400). Of 24 specimens testedsimultaneously by TP and IDTP, 18 were reactive by bothmethods, but 6 (25%) were reactive only by IDTP. Of 36specimens positive by IDTP, 21 were reactive by both IDTPand TP but 15 (42%) were reactive only by IDTP (62). It islikely, therefore, that the IgM antibody is detectable earlier,and in a greater fraction of patients than shown by Smith etal., using the TP test alone (139, 141). The greater sensitivityof the IDTP than the TP is also inferred from our findings ofpersistence (or "reappearance") ofIgM antibody in patientswith coccidioidal pulmonary cavities (97). Smith et al. (139,141) had pointed out that TP reactivity may reappear aftercoccidioidal hydropneumothorax resulting from rupture of acoccidioidal pulmonary cavity. Our studies have indicatedthat chronic coccidioidal pulmonary cavities are often ac-companied by antibody detectable by IDTP. Thus, theapparent reappearance of IgM noted by Smith et al. (139,141) is likely the result of an increase in already persistingprecipitins that are detectable by IDTP but below the thresh-old of detection by TP. TP and IDTP reactivity can also bedemonstrated in the pleural effusion of acute pulmonarydisease.
In the study by Smith et al. (141), TP reactivity wasdetected in 91% of patients with primary nondisseminatinginfections at week 3 of illness and declined to only 4% 7
CLIN. MICROBIOL. REV.
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

SEROLOGY OF COCCIDIOIDOMYCOSIS 251
FIG. 4. ID of serum from a patient at different stages of coccid-ioidomycosis. (Top) Serum of a patient with acute primary coccid-ioidomycosis showing presence of IDTP (IgM) reactivity. (Middle)Serum of a patient still in a relatively early stage of disease showingpresence of IgM (near serum well) and IDCF (IgG) reaction furtherfrom serum well each showing line of identity with respectivecontrol sera. (A similar pattern may accompany a chronic coccid-ioidal pulmonary cavity.) (Bottom) Serum of a patient in the courseof coccidioidomycosis showing only IDCF (IgG) antibody. Wells Aand C contained heated coccidioidal antigen reactive with IgM;wells B and D contained unheated antigen reactive with both IgMand CF (IgG) antibodies. Well 1, Control IDTP (IgM)-positiveserum; well 2, patient serum; well 3, control IDCF (IgG)-positiveserum.
months after onset of illness. However, TP-positive reac-tions persisted in 347 of 722 (48%) patients with disseminat-ing infections, sometimes for several years; 8 patients wereTP positive in the second year, 3 in the fourth year, and 1was still positive during the ninth year after infection anddissemination. Thus, persistence of TP (and IDTP) antibodymay be of partial assistance (in addition to CF titer) injudging severity of coccidioidal disease. Some workers haveindicated that reactivation of disseminated coccidioidal dis-ease is accompanied by reappearance of IgM; however, it islikely that by concentration of the serum, in most instances,persistence rather than de novo renewed production of IgMcan be demonstrated. IgM can reappear in the serum whenthere is systemic reinfection from the meninges via a ven-triculoperitoneal or ventriculoatrial shunt (101).The persistence or reappearance ofIgM may reflect spher-
ule proliferation and release of endospores. In vitro, theantigen responsible for IDTP reactivity is liberated into theculture medium at a stage of the life cycle in which youngendospores are present before their evolution to spherules(156).The presence ofIgM antibody has been noted infrequently
in the cerebrospinal fluid (CSF). Smith et al. (141) obtaineda positive TP with CSF in only 1 of 92 patients withcoccidioidal meningitis. Our experience has been similar(103); for example, we have now detected IgM antibody byIDTP in the CSF of 4 of 311 patients with coccidioidalmeningitis. This test may provide another marker for diag-nosing meningitis when the CF test is negative.Smith et al. (139, 141) detected CF antibody in cord blood
of babies born to serologically positive mothers but made nocomment regarding TP reactivity. We have recently receivedcord bloods from two babies (whose mothers had coccidioi-domycosis during pregnancy) both of which gave positiveIDTP reactions. We feared that this presence ofIgM mightindicate in utero infection; however, both infants haveremained without clinical evidence of coccidioidomycosisthrough many months of postpartum follow-up. Both moth-ers had detectable IgM and IgG in their sera at the time ofparturition. Whether the IDTP reactivity represented mater-nalIgM that had contaminated infant blood because of rentsin the placenta or its separation from the uterus (95) orwhether it was of fetal origin is unknown. Its presence inthese cases had no connotation of in utero infection with C.immitis as indicated by the subsequent clinical course.
If IgG antibody alone is detected and it yields a low CFtiter (e.g., 2 to 8), it is important to know whether the patienthas had a recent acute illness. Such a low titer may persist inpatients with a well-focalized coccidioidal pulmonary resid-ual that has been present for many months or even years. Asubsequent serum sample should provide evidence (appear-
VOL. 3, 1990
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

252 PAPPAGIANIS AND ZIMMER
ance of IgM or change in CF titer) that would indicate arecent coccidioidal infection. A stable, low CF titer and noIgM detected in a subsequent serum sample provides evi-dence that the coccidioidal infection had been acquired atleast many weeks earlier. Smith et al. (139), however, hadnoted that a few patients had TP-reactive sera persistingeven after the CF titer had reverted to negative.
Detection of CF antibody is useful in diagnosing acutecoccidioidomycosis and offers supportive information to thatprovided by detection of IgM. Detection of the IgG by IDand its quantitation by the CF or quantitative ID test areimportant in ascertaining the course followed by the disease.CF reactivity at any titer is significant provided it has beenconfirmed as coccidioidal by prior detection of coccidioidalIgM or by positive IDCF.There is generally a reliable correlation between the CF
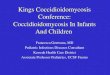
titer in serum and the severity (extent) of coccidioidaldisease (Fig. 5). CF titers of above 16 in the serum shouldalert one to the possibility of disseminated coccidioidomy-cosis. This level is based on the studies of Smith et al. (139,141), who used a Kolmer CF test with complement bindingfor 2 h at 370C. We routinely use 2-h binding of complementat 370C for sera because of the extensive clinical correlationestablished by these workers. As pointed out by Smith et al.(140, 141), overnight (18-h) binding of complement at 4 to50C yields higher titers. This greater sensitivity prompted usto adopt binding of complement at 4 to 50C to detectantibody in the CSF. Several other methods make use ofbinding of complement in the cold, including that of theLaboratory Branch Complement Fixation Test (LBCF) ofthe Centers for Disease Control (98). (The trade-off is greatersensitivity with low-temperature binding of complement formore rapid results and probably better clinical correlationwith 2-h binding at 370C.) (See below regarding serologicfailures.) When dissemination is extensive, the titer gener-ally is >128 unless the infection is so fulminating that thereis insufficient time to mount an antibody response or the hosthas an immunocompromising limitation of humoral re-sponse.
If the disease is limited to a portion of lung or even alimited focus of extrapulmonary dissemination, e.g., thewrist joint or even the meninges, the serum CF titer may bein the low range of 2 to 8. On the other hand, withinvolvement of lungs or mediastinal lymph nodes or both,serum CF titers may be 128 to 256, which usually denotesdissemination. When sera are tested, the usual startingdilution is 1:2, with subsequent twofold dilutions. However,to increase sensitivity when testing CSF, we and some otherlaboratories begin the CF antibody titration with undilutedCSF when sufficient specimen is provided. However, to ourknowledge no correlation has been established betweenfixation of complement by undiluted CSF and activity of themeningitis. Indeed, when concentrated by evaporation, evenCSF from patients with nonmeningeal coccidioidomycosismay yield an IDCF reaction (112). Therefore, CF reactivityby undiluted CSF does not establish the presence of menin-gitis. However, in the patient known to have meningitis,decrease in CF antibody and reversion of the CF test tonegative provide proportionately favorable information.With the presence of coccidioidal antibody established by
TP, IDTP, or IDCF, there is little to be gained clinically byrepeating these qualitative tests. These tests may be re-peated when the patients who have had positive serologicfindings, e.g., CF, that become equivocal or negative as aresult of healing subsequently are believed to have relapsed
CLIN. MICROBIOL. REV.
patient with a ventriculoperitoneal or ventriculoatrial shunt(indicative of systemic reinfection).
Thus, quantitation of antibody by CF or quantitativeIDCF provides guidance on the course of the disease.Specimens should be tested at 3- to 4-week intervals as thereis usually no significant serologic change in less time. Posi-tive specimens should be frozen at -15 to -20TC and thawedfor retesting when a subsequent specimen from the sameanatomical source (e.g., serum, CSF, or pleural fluid) isobtained. Thus, two sequential specimens should be testedsimultaneously to control any test variations that may occurin the CF or quantitative IDCF. A fourfold change in titer issignificant, with an increase indicating worsening of diseaseand a decrease indicating improvement. In the usual nonim-munocompromised patient, the titer continues to rise withworsening disease even in the moribund patient who hasdeveloped anergy to the coccidioidal skin test.
Negative serologic findings in the face of cultural orhistopathologic confirmation of coccidioidal disease havebeen infrequent. Smith et al. (141) indicated that, of 722patients with disseminating disease, only 2 had negativeserologic findings. Two others with disseminated infectionswere CF negative when complement binding was carried outfor 2 h at 37TC but positive when binding was carried out at40C for 18 h. The authors speculated that their standardantigen may have lacked antigenic components present inthe patients' own C. immitis isolates. The isolate from onepatient was used to prepare "autogenous" coccidioidin.However, that patient's serum exhibited an even lower CFtiter with the autogenous antigen than with the standardmultiple-strain coccidioidin.
In general, coccidioidal serologic tests are highly sensi-tive. We have noticed two patient groups in particular forwhom the potential for serologic failure is great: patientsundergoing organ transplants, and patients with AIDS. Inthe former group, for example, 3 of 13 with disseminatedcoccidioidomycosis had negative serum CF tests and 1 of 5with pulmonary disease only had a negative serum CF test(18). In another report, three of seven renal transplantpatients with coccidioidal lesions were negative by CF test,but two of these were positive by ID (the third was not testedserologically) (9). One of four patients who had coccidioido-mycosis complicating a cardiac transplant was negative bycomplement fixation (8, 9). Of 48 patients with AIDS andcoccidioidomycosis (18 published cases, 30 from our serodi-agnostic work), 4 have been seronegative. Also, in ourexperience, the number of negative serologic findings inother patients has been small. These occurred in (i) twoapparently immunologically normal female patients withcoccidioidal inguinal adenopathy (one of these showed afaintly positive IDCF reaction with concentrated serum); (ii)one female patient with hypogammaglobulinemia; (iii) onemale with coccidioidal meningitis; and (iv) one female withcoccidioidal meningitis (several weeks after onset of hermeningitis, antibody could be detected in her CSF but wasnever detected in her serum).
In a very few patients, we observed a negative CF resultwith serum that yielded a substantial IgG titer by QID. Byadjusting the CF reagents, we found that these sera reactedpositively in the CF test. Thus, the usual standardizedcombination of complement, hemolysin, and antigen may beappropriate for most sera but may be poised incorrectly fora few specific sera. In some instances, patients may notgenerate an expected CF antibody response because theyhave a selective deficiency of IgGl and IgG3 subclasses,
or to determine the reappearance of IgM antibody in a which are efficient complement binders, or they may gener-
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

SEROLOGY OF COCCIDIOIDOMYCOSIS 253
256r
SEE0CLE0
0
S
00
0:5
S
.CE8
E
zf
128 .
64
32
4
2
a
0 10 20 30 40 50 60 70 80 90
Cumulative percentage4O Dissemination extensive 00 Dissemination alt
A-- Dissemination meningitis h-- * Dissemination single lesion-4 Primary infection *-* Pulmonary cavity006 Pulmonary residuals without cavity
100
Progressive dise;with metapulmondissemination
/
aseIy Favorable responseary <N~/ \ A/ to therapy
/\/ Chronic persisting/ \. Disseminated disease
I// \_i 04/ \/ \\/%a* I
e~~Single metapulmonaryfocus - e.g., meningesor skin; or chronic
11-10 pulmonary cavity
1 2 3 4 2 4 6 8
Week Month
10 12 2 3 4 5
Year
Time After Onset of Primary IllnessFIG. 5. (Top) Maximal titers of complement-fixing antibodies in sera of patients with various types of coccidioidal disease based on tests
on 39,500 sera. Reprinted from reference 141 with permission of the publisher. Symbols: 0, dissemination extensive; A, disseminationmeningitis; , primary infection; O, pulmonary residuals without cavity; 0, dissemination all; A, dissemination single lesion; *, pulmonarycavity. (Bottom) Patterns of serum CF titers with various clinical phases of coccidioidomycosis. Reprinted from reference 101 with permissionof the publisher.
ate IgG4, a nonbinder of complement. To our knowledge, wehave tested sera from only a single patient with a selectivedeficiency (of IgGl). After concentration, her serum was
positive for both IgM and IgG antibodies by ID, but was
negative by CF; the QID titer was 2.Serum concentrated by evaporation and tested by ID will
yield positive findings despite negative CF results. The ID
method was not available when Smith et al. (141), in thepretransplant era, reported their two serologic "misses"among 722 patients with disseminated disease, a failure rateof0.28%. Kozub et al. (82) described negative serologic tests(CF, ID, TP, and CIE) in seven patients. Five had culture-proven C. immitis infection. However, neither the nature oftheir disease (acute, chronic, or cavitary) nor the presence of
211
210
2 9
2 8I
2 6I-A._LL
2 4
222
2 1
VOL. 3, 1990
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

254 PAPPAGIANIS AND ZIMMER
FIG. 6. Positive ID reactions between toluene-autolyzed coccid-ioidal mycelial antigen (top two wells) and pooled human serum in agel consisting of bovine fibrin. The sera in the pool had CF titersbetween 32 and 64. This illustrates a possible setting in which anantigen-antibody precipitate can form in vivo with certain immuno-logic consequences such as activation of complement and chemo-taxis of granulocytes.
any underlying disease was given. The other two patientswere negative by CF tests but positive by one or more of theother tests.
In some cases, either very early in the course of acutecoccidioidomycosis or in immunocompromised patients,tests for antibody may be negative. Tests for antigen mayfulfill the serodiagnostic requirements in such cases (seesection on serology).
Application of serologic tests in veterinary medicine hasshown antibody responses in dogs (55, 120, 121, 129, 133,155), horses (33), and nonhuman primates (4, 54, 88, 92, 110,120, 134, 145) generally similar to those in humans. Serologictests in other species (e.g., llamas) (96) have also shown thatthe methods are useful, but the numbers of animals testedhave been too few to provide for complete evaluation ofserology.The possible protective or harmful role of coccidioidal
antibodies in vivo has not been defined. The CF (IgG)antibody that produces a precipitate with its correspondingantigen in agar or gellan gum gels also produces a precipitatein a fibrin gel (Fig. 6). Such an antigen-antibody precipitateformed in fibrin in vivo could, by activation of complement,evoke an inflammatory cell response. The IgM-reactiveantigen on the surface of spherules (24) may serve as anopsonizing reactant. Antibody may influence cell-mediatedresponsiveness.
ANTIGEN PREPARATION AND ANALYSIS
Historical Development
In 1914, Cooke was the first to use C. immitis derivativesfor serologic testing (26). He used triturated culturedmycelium and spherules from "human lesions" in a precip-itin reaction with patient sera. Davis (32) prepared a suspen-sion of C. immitis for successful testing by CF. Additionalcrude antigens, which could be called "coccidioidins," were
prepared from culture filtrates and evaluated by skin testingwith little clinical application. Hirsch and d'Andrea (52, 53)prepared filtrates from mycelial C. immitis grown in bothcomplex (extract of placenta) and chemically defined (ammo-nium lactate) media but used them primarily to show skin testreactions in humans and animals with coccidioidomycosis.From the late 1920s to the 1940s, various other coccidi-
oidins were prepared from culture filtrates in nonchemicallydefined media and used for skin testing (3, 44, 45, 68, 69, 79).A simple synthetic ammonium chloride-sodium acetate me-dium was used by Stewart and Kimura (144) for skin tests.However, Smith et al., who considered that these were not"sufficiently potent," tried other formulations, finally set-tling on modifications of the synthetic Bureau of AnimalIndustry medium long used for preparation of tuberculin(142).
In the 1930s, C. E. Smith and his mentor Ernest Dicksonthought that it would be necessary to produce antigen fromthe spherule (in vivo or "parasitic" form) for a serologicaltest and that mycelial antigen would not likely be satisfac-tory. However, having no method available to produce thespherule or endospore phase at that time, Smith proceededwith mycelial cultures. Smith's initiation of serologic stud-ies, which proved to be so useful, came about as a result ofhis interest in the skin test reactivity of guinea pigs infectedwith C. immitis. He wanted to learn whether serum frominfected guinea pigs would, when mixed with coccidioidin,"inactivate" the latter with respect to its skin test reactivity(137, 139). The mixture, allowed to sit for a week, showed a"discrete button in the bottom of the tubes." Serum fromnormal guinea pigs gave no precipitate. In retrospect, theobservation was somewhat remarkable in that the precipitatewas not bulky and was translucent and closely applied to thebottom of the tube. In further use of the precipitin test,Smith showed that a sharp flick of the tube to dislodge thebutton of precipitate was often needed to detect it (Fig. 2).Smith and colleagues then found that the coccidioidin andserum from patients with coccidioidomycosis would fixcomplement. Adaptation of the Kolmer CF test which wasused for quantitation of antibody in patients with syphilispermitted similar titration of antibody in patients with coc-cidioidomycosis (139).The modified Bureau of Animal Industry medium was
inoculated with hyphae and arthroconidia, which led tosurface growth. Cultures were incubated static for manyweeks, usually 4, but for up to 3 months if the antigenicpotency was considered inadequate. However, it was latershown that serologically active antigen could be detected asearly as the second week of incubation in the modifiedBureau of Animal Industry medium (101). Ajello et al. (2)prepared a coccidioidin that was reactive in both CF and IDtests by collecting 3-week-old culture filtrates of C. immitisgrown in peptone-glucose-yeast extract broth. The durationof incubation resembles that of Smith's original coccidioidinpreparation (142), but it was carried out on an incubator-shaker. Rowe et al. (124, 125) also produced antigen active inID in defined synthetic and complex media in culturesincubated for 45 days on a shaker. In Smith's studies, fourisolates of C. immitis from various geographic regions wereused initially to assure antigenic coverage; later, this numberwas increased to 10 and then to >24 (138, 139, 142).Considerable variation in CF antigenic potency was ob-served by us among culture filtrates and toluene-inducedautolysates of 25 strains of C. immitis. Huppert (57) reportedthat nine different strains produced variable amounts of fourdifferent antigens detectable by ID, but as yet there has been
CLIN. MICROBIOL. REV.
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

SEROLOGY OF COCCIDIOIDOMYCOSIS 255
no demonstration that strain differences pose a problem insensitivity or specificity of serologic tests. In fact, in ID testsof >70,000 human sera, we have found that an antigenpreparation from a single strain (Silveira) of C. immitis hasbeen as sensitive as a multistrain antigen reagent for detect-ing antibody. Nevertheless, serologic antigens, includingcommercial preparations, are still made from many strains ofC. immitis.When preparing coccidioidin by the method described,
Smith et al. (139) noted that despite seemingly identicalinoculation and incubation the antigenic potency and anti-complementary activity varied among culture flasks. It wasnecessary to sample the filtrate from each flask to ascertainits suitability as serologic antigen. Numerous lots wereanticomplementary and could not be used for CF tests.The macerated undersurface of the floating mycelial mat
indicated that autolysis was taking place during the pro-longed incubation (105) and, depending on the strain, antigenactive in the TP test was detected in 2-week-old, but not1-week-old, cultures. In 1957, deliberate autolysis undercontrolled conditions was carried out to determine whetherantigen could be liberated quickly and consistently (115).The method was adapted from one used to prepare yeastautolysate (118). C. immitis Silveira mycelial phase wascultured in 2% glucose-1% yeast extract (Difco Laborato-ries) for 3 days at 34 to 350C on a shaker. The hyphae werecollected by filtration on Whatman no. 1 paper, washed withsterile water, and suspended in water in a cotton-pluggedflask to give a thick slurry. Toluene, 3% (vol/vol), was addedto the slurry. A paper or aluminum foil cap was placed overthe cotton plug and the flask was incubated at 370C for 3days. This led to autolysis and liberation of antigen active inskin testing and in the TP and CF tests (114, 115). CF activity(titer, >64) was evident immediately and after toluene addi-tion, and this increased progressively throughout the 72-hautolysis period (106). The lysed cellular debris was re-moved by filtration on Whatman no. 1 paper, and theautolysate was retained as antigen solution. Aqueousthimerosal was added to a final concentration of 1:10,000 asa preservative.
Originally, the culture filtrate from 2% glucose-1% yeastextract medium used to produce the cells for autolysis wasdiscarded after collection of the mycelium. However, Hup-pert and Bailey (59) found that the 3-day culture filtrate alsopossessed serologic activity. Because the Difco yeast extractused in the culture medium is itself "the water solubleportion of yeast autolysate" (36), Huppert and Bailey (60)routinely dialyzed the yeast extract against water at 800C toavoid cross-reactive antigens. The retentate was discarded,and glucose was added to the dialysate to produce a mediumsimilar to 2% glucose-1% yeast extract. Both autolysate andculture filtrate can be used as a source of TP, IDTP, CF, andIDCF antigens, although the autolysate is more concen-trated.
In 1957, Converse (25) developed a medium later modifiedby Levine et al. (87) that would support in vitro growth of thespherule-endospore phase of C. immitis; thus, it becamepossible to prepare serologic antigens from this growthphase. Landay et al. (84, 85) found that thimerosal-preservedspherules induced antibody in rabbits which reacted by bothCF and ID with sonicated and autoclaved spherule extractsand arthroconidial antigens. However, in ID tests, antiseruminduced by arthroconidia reacted only with arthroconidialantigens, although in CF tests it reacted also with spheruleantigen. Subsequently, Levine et al. (86) prepared antigenfrom spherules grown in vitro by allowing them to lyse in
distilled water for 40 days. Initially called "spherule coccid-ioidin," this antigen was given the name spherulin in analogywith coccidioidin (129). Spherulin appears to have serologicreactivity at least equivalent to that of coccidioidin, and inthe CF test it actually detected a higher antibody titer inhuman sera than did coccidioidin (130). However, spherulinshowed greater cross-reactivity than coccidioidin in the CFtest (64). Moreover, we have demonstrated that sera whichwere negative by CF with both spherulin and coccidioidinyielded positive ID tests with coccidioidin when concen-trated by evaporation. Therefore, it has not been demon-strated that spherule-derived antigens should supplant myce-lial coccidioidins.The spherule-endospore-phase antigens are also active in
CIE, ELISA, CF, and FA (22, 74, 84, 85, 124, 130).Endospores inoculated into modified Converse medium pro-duce, within a few hours, antigens in the medium reactive byIDTP and IDCF (152). We have shown that toluene-inducedautolysis at 350C of mature spherules in vitro also yieldsantigens active in the IDTP and IDCF reactions. By expos-ing first-generation spherules grown in vitro to toluene at40TC, Galgiani et al. (39) produced an antigen reactive byIDTP but lacking IDCF activity. Antigens useful in serologictests for coccidioidomycosis are available from a number ofcommercial sources. Their addresses may be obtained byinquiry sent to the Division of Mycotic Diseases, Centers forDisease Control, Atlanta, GA 30333.
Subcellular Localization
The cellular location of coccidioidal antigens has beenstudied. Kong et al. (81) concluded that the antigen (of wholespherules) important in inducing immunity in mice andmonkeys is located in the wall of spherules. The presence ofantigen corresponding to that active in the IDCF and theactive antigen in the TP and IDTP are released from bothmature spherules and endospores produced in vitro. Therelease of these antigens was hastened by exogenous chiti-nase or lysozyme. The mechanically disrupted spherule wallfragments, when digested with chitinase, adsorbed quantita-tively the antibody participating in the IDTP reaction. How-ever, these fragments of chitinase-treated spherule walls, didnot adsorb CF (or IDCF) antibody (24). This last and otherobservations suggest that the antigen(s) reactive in the CF orIDCF tests is not associated with the cell wall but may becytoplasmic (157). Cultures inoculated with endospores des-tined to yield spherules show very early that the IDTPantigen is liberated before and persists through the formationof spherules, and IDCF antigen is found in the culturemedium slightly later at a time when cleavage planes areformed (156). Cox et al. (31) also obtained an antigenic,alkali-soluble, water-soluble substance from the wall of C.immitis which reacted with IgM antibody.Cole et al. (20) described the presence of a "membra-
nous" fraction on the surface of the outer wall of spherulesgrown in vitro that readily sloughed and could be extractedwith a detergent, N-octyl-p-D-glucopyranoside. This mate-rial reacted with both human IDTP-positive and IDCF-positive sera but formed a line of identity only with IDTPand not the IDCF. This suggests that the membranoussurface antigen includes IDTP-reactive antigen. However,antibody to this detergent-solubilized surface antigen alsoreacted with cytoplasmic vesicles as well as spherule wall.The membranous layer may contain molecules that aresynthesized in the cytoplasm, transported, and then incor-porated into the spherule wall (22). A soluble wall fraction of
VOL. 3, 1990
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

256 PAPPAGIANIS AND ZIMMER
arthroconidia with a relative molecular weight of 62,000under nonreducing conditions was found to have proteolyticactivity (as a serine protease) (23). This protease was iden-tified as "antigen 11" (Agli) by reaction with a burroanticoccidioidin serum in two-dimensional immunoelectro-phoresis, but did not react in an ELISA with serum fromhumans with coccidioidomycosis (the stage of disease orconventional serologic test results were not reported). Thisantigen showed proteolytic activity against human IgG andsecretary IgA. Similar proteolytic activity was manifestedby a 19-kilodalton (kDa) fraction of another soluble antigen,termed AgCS, from arthroconidial walls. AgCS, which in-cluded a 39-kDa fraction that largely lacked proteolyticactivity, reacted by ELISA with sera from humans withcoccidioidomycosis. The proteolytic activity of the Agli andAgCS against human immunoglobulins makes it likely thatthese antigens would digest the antibodies participating inconventional serologic tests.
Antigen Characterization
Characteristics of coccidioidal antigens have been studiedby a number of workers. Hirsch and d'Andrea (52) precip-itated skin-test-active antigen from C. immitis culture filtratewith 95% ethanol. They detected 20 to 40% reducing sugars,an osazone identified as glucosazone, and 3 to 4% nitrogen.Hassid et al. (49) also identified glucose as the majorcomponent of the alcohol-precipitated fraction of coccidioi-din. They detected galacturonic and another unidentifiedreducing sugar. The saccharide components glucose, galac-turonic acid, and unknown sugar were present in a ratio of6:1:3, respectively. The total nitrogen content of their mate-rial was approximately 3.2%, with 0.6% as amino nitrogen.However, their tests for protein (Millon, xanthoproteic,glyoxylic acid, and biuret; and precipitation by hot trichloro-acetic acid) were negative.
Subsequently, we reported that precipitation of coccidi-oidin with 80% ethanol yielded a serologically active mate-rial with an average molecular weight of 31,700. This mate-rial was 60 to 70% polysaccharide, based on mannose as astandard, and contained 3 to 4% nitrogen (111; D. Pappagi-anis, Ph.D. thesis, University of California, Berkeley, 1955).Mannose was the predominant sugar representing 90 to98.5% of the polysaccharide, with galactose at <10%. Athird sugar was detected in a very low concentration, andthis migrated (by paper chromatography) similarly to rham-nose, a methyl pentose, in one solvent system and similarlyto dihydroxyacetone in other solvent systems. We coulddemonstrate little glucose and no uronic acid. The crudepolysaccharide was negative by biuret test, was not precip-itated by hot trichloroacetic acid, and gave no reaction withninhydrin, bromcresol green, or mercuric chloride-methylorange (111). All of these tests suggested the absence ofprotein as had been concluded previously by Hassid et al.(49). However, when the crude polysaccharide was hydro-lyzed with acid and subjected to paper chromatography,ninhydrin-reactive spots were observed which correspondedto the mobility values of six amino acids, including tyrosineand methionine (111). Furthermore, the Folin-Ciocalteauphenol reagent (93) for protein produced a reaction indica-tive of 15 to 20% peptide material, which approximates theexpected content of protein or derivatives of protein basedon the 3 to 4% nitrogen detected.Goldschmidt and Taylor (Abstr. Annu. Meet. Soc. Am.
Bacteriol. 1958, P. 98, p. 127) confirmed the presence ofmannose and galactose; they, too, found an unknown sugar
which they reported as monomethylmannose. Later, thiswas shown to be 3-O-methylmannose accompanied by glu-cose as well as mannose and galactose (119, 131). Cole et al.(21) studied the dialyzed retentate of 16-day-old mycelialculture filtrates by gas-liquid chromatography. They de-tected 3-O-methylmannose, mannose, galactose, and glu-cose in a ratio of approximately 3:10:1:10. Precipitation ofthe nitrogenous polysaccharide with varying concentrationsof ethanol produced chemically varied antigens that reactedwith human antiserum by TP and ID (107).
Recently, we carried out immunoaffinity isolation of anti-gen reactive in the TP and IDTP tests by collecting precip-itate produced in the TP test, using human serum (159). Theantigen was liberated from the antibody by treatment withpronase and further purified by chromatographic proce-dures, which yielded two serologically active fractions.These were studied by high-performance liquid chromatog-raphy and gas-liquid chromatography after acid hydrolysis.One fraction (peak I) contained mannose, 3-O-methylman-nose, and glucose in a ratio of 8:1.2:1, and the secondfraction (peak II) contained 3-O-methylmannose, mannose,glucose, and galactose in a ratio of 1:1:1:1. Several aminoacids were present, their aggregate at a ratio of 1:5 withpolysaccharide. However, despite the presence of the aminoacids, or because of its size or charge, the polysaccharide(s)did not electrophoretically enter a sodium dodecyl sulfate-polyacrylamide gel (SDS-PAGE) and remained within the3% polyacrylamide stacking gel. By gel filtration, peak I wasestimated to have an average molecular size of 140 kDa;peak II had an average molecular size of 225 kDa (154).Some of these properties are reminiscent of those noted byWeiner (148): coccidioidal glycoprotein antigens detected bya RIA and presumed to correspond to TP antigen chromato-graphically were in the molecular weight range of 140,000 to240,000 and could not be sharply resolved by PAGE with theantigen(s) remaining close to the origin. Calhoun et al. founda 100-kDa antigen separable by SDS-PAGE that was reac-tive with IDTP-positive sera in immunoblot analysis (10).
Kruse and Cole (83) have recently isolated two TP anti-gens from a concanavalin A-bound, alkali-soluble, water-soluble fraction of inner arthroconidial wall. The sameantigens were also isolated from mycelial culture filtrate.One of the antigens was characterized as being a 240-kDadimer of a 120-kDa component and the second was charac-terized as being a 110-kDa antigen. These polymers wereelectroeluted from SDS-PAGE separations.Another approach to the study of soluble serologically
active antigens of C. immitis entails two-dimensional immu-noelectrophoresis as well as crossed- or tandem-immuno-electrophoresis (66). This study demonstrated 26 antigens incoccidioidin and 12 in spherulin. Of these, 10 appearedcommon to both antigen preparations, 16 were found only incoccidioidin, and 2 were unique to spherulin. Antigenicanalysis of an alkali-soluble, water-soluble fraction of C.immitis cell walls, coccidioidin, and spherulin by immuno-electrophoresis showed IDTP activity in two peaks, the firstof which has a cathodal but only a partial anodal leg andwhich parallels the second major polymeric peak, designatedantigen 2 in this system (28, 66). A monoclonal antibodyobtained by immunizing mice with spherulin recognizedepitopes on the components of both of these peaks (38).Immunoblotting of coccidioidin with this monoclonal anti-body revealed a molecular size range of 130 to 330 kDa,consistent with the size range observed by Kruse and Cole(83), Weiner (148), and Zimmer and Pappagianis (159).
Characterization of both spherule-endosphore-phase and
CLIN. MICROBIOL. REV.
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

SEROLOGY OF COCCIDIOIDOMYCOSIS 257
mycelial culture filtrates by SDS-PAGE and immunoblotanalysis revealed electrophoretically separate antigens de-tected with IDCF/CF-positive sera. A 48-kDa band commonto all filtrates was strongly reactive with the serum, asdemonstrated by immunoblot reaction with anti-IgG (10,157). Prior heat treatment of the antigens at 60°C for 30 min,which destroys CF and IDCF activity, altered or destroyedthe component detected as the 48-kDa band (157). Thiscomponent was further characterized by using size exclusionchromatography followed by ID and denaturing SDS-PAGE,as well as nondenaturing PAGE, and shown to be derivedfrom a 110-kDa protein nonreactive with lentil lectin orconcanavalin A (158). Cox et al. (30) isolated an antigenreactive with IDCF antiserum by using a combination ofconcanavalin A affinity and immunoaffinity chromatography.This antigen was assayed by immunoelectrophoresis andcorresponded to antigen 3 in the reference system of Hup-pert et al. (66). Both two-dimensional immunoelectrophore-sis and immunoblotting systems showed similarity betweenantigens derived from coccidioidin and those derived fromspherulin (29). Table 1 summarizes the characteristics ofcoccidioidal antigens.
BODY FLUIDS TESTED
Serum should be tested in all cases of suspected coccidi-oidomycosis. Changes in the serologic findings with serumusually correlate with clinical changes. Nevertheless, testingCSF and pleural, peritoneal, and joint fluids (along withserum) is appropriate when their corresponding anatomicalsites of origin may be affected.Antibody can be detected in blood obtained from the
umbilical cord or by venepuncture from the newborn infant(139, 141). The CF titer may be the same as or slightly lowerthan that of the mother's serum and will decline with time aswould be expected by transplacentally transmitted maternalIgG. As described previously above, we have detected IDTP(IgM) as well as CF (IgG) antibody in the sera of two humanneonates. However, neither of these two babies manifestedclinical evidence of coccidioidomycosis.
Fixation of complement by CSF at 1:2 or higher dilutionsusually indicates the presence of coccidioidal meningitis(139, 141). (CF by undiluted CSF may also indicate menin-gitis, but this has not yet been substantiated.) The significantexception is when there is juxtadural coccidioidal disease, inwhich case the pachymeninges may be sufficiently affectedto permit CF antibody to penetrate from serum or inflam-matory fluid into the CSF. Juxtadural disease can be distin-guished by an increased CSF protein and normal glucose andcell count, whereas in meningitis protein and cells areincreased and glucose is decreased.CSF may be obtained from the lumbar or lateral cervical
subarachnoid space, cisterna magna, or lateral cerebralventricles. Differences in concentration of protein and glu-cose normally exist among these compartments. Similarly,differences in antibody concentrations may be detected inCSF from these different anatomic loci. For example, theventricular fluid may have normal cell and chemical valuesand be negative for coccidioidal antibody by CF despiteactive basilar meningitis accompanied by chemical, cyto-logic, and serologic evidence of meningitis in cisternal orlumbar fluid (46). If the ventricular fluid fixes complement, itindicates either a block to the outflow of CSF or a coccid-ioidal ventriculitis-ependymitis.Because of the differences in constituents of CSF from
different anatomical compartments, it is important for com-
TABLE 1. Characteristics of antigens used in coccidioidalserologic tests
Antigen Characteristics
TP/IDTP 1. Present in spherules, endospores, hyphae andarthroconidia in vitro; probable cell wall loca-tion.
2. Present in both mycelial and spherule/endo-spore culture filtrate, and autolysates. IDTPantigen liberated before spherule maturity andpersists through spherule development.
3. Released from spherule wall by chitinase. Re-leased from mycelial, spherule, and arthro-conidial wall by alkali treatment. Chitinase-digested spherule walls adsorb TP/IDTPantibodies.
4. Reactive with concanavalin A and lentil lec-tins. Heat, pronase stable. Contains mannose,glucose, galactose, and 3-O-methylmannose.The latter is not specific to C. immitis.
5. At least two separable antigens (epitopes?)involved. Molecular weights reported as (i)140,000 and 225,000, with different ratios ofmannose and 3-O-methylmannose; (ii) 110,000and a 240,000 dimer.
6. In two-dimensional immunoelectrophoresis,activity in two peaks: one, designated "incom-plete precipitating antigen 1," with a cathodalbut only partial anodal leg which parallels thesecond major peak, designated antigen 2. Thelatter is not specific for C. immitis.
7. Same antigen reactive in LA test?
CF/IDCF 1. Present in mature spherules and endospores,and hyphae in vitro; probable cytoplasmic lo-cation.
2. Present in both mycelial and spherule/endo-spore culture filtrates only after spontaneousautolysis, or toluene induced, or spherule mat-uration with subsequent wall lysis and endo-spore release.
3. Chitinase-digested spherule walls do not reactwith CF/IDCF antibodies.
4. Nonreactive with concanavalin A and lentillectins. Heat (60°C) and pronase sensitive.
5. Has reported molecular weight of 110,000, butfollowing reduction and subsequent SDS-PAGE immunoblotting, a 48-kDa band stronglyreactive with IDCF/CF antiserum is detected.
6. Immunoelectrophoretic activity in one peak,designated antigen 3.
Exoantigen(heat stable)
1. Present in mycelial culture filtrates and tolueneautolysates, and spherule/endospore phase fil-trates and lysates.
2. Nonreactive with concanavalin A. Heat stable.Reaction is different and distinct from IDTP orIDCF.
3. Immunoelectrophoretic activity reported in (i)peak designated Agil (?) or (ii) peak desig-nated AgCS (?).
parisons of CF titers to be made between successive speci-mens from the same compartment, e.g., lumbar fluid com-pared with lumbar fluid, cisternal with cisternal, etc.The initial CSF specimen may be negative by the CF test,
but overall, 95% of CSF specimens are positive by CF incoccidioidal meningitis (103). Smith et al. (139) indicated thatthe CSF of one patient did not become positive by CF until6 months after meningitis developed. In our study of coccid-
VOL. 3, 1990
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

258 PAPPAGIANIS AND ZIMMER
FIG. 7. ID of lumbar CSF from a patient with coccidioidalmeningitis. (Top) Presence of IgG (IDCF), which is common, andIgM (IDTP), which is uncommon. (Bottom) Same patient's CSFafter treatment with dithiothreitol, which dissolves the IDTP pre-cipitate. (Wells as described for Fig. 4. CSF in center wells.)
ioidomycosis resulting from a dust storm (104, 108), the CSFbecame seropositive in all of 22 cases of meningitis (occur-ring outside usual endemic areas) by 9 weeks after onset ofprimary acute illness (101). In the absence of a serumspecimen, a positive CSF serologic test indicates coccidioi-dal infection, though not necessarily meningitis. The pres-ence of detectable IgM antibody in the CSF is infrequent;however, in our experience, its presence has always beenassociated with meningitis (Fig. 7). An increasing CF titer ofthe CSF indicates disease progression, and a decreasing titerindicates improvement. Complement-fixing antibody maypersist even after return of the cellular and chemical constit-uents to normal, and this provides a suitable reason forcontinuing therapy for meningitis. The CF titer of the lumbarCSF may reach high levels (e.g., 256) accompanied by highconcentrations of protein as a result of CSF loculation, e.g.,as with a cervical lesion leading to a block in the circulationof the CSF. In patients with a ventriculoperitoneal or ven-triculoatrial shunt, the serum as well as CSF should be tested
periodically as rising serum CF titer (with or without reap-pearance of TP or IDTP reactivity) indicates systemic rein-fection from the meninges via the shunt (101). Antibody canbe detected in the CSF by ID as well as CF. However,caution is needed in the interpretation of a positive ID test,particularly when the sample has been concentrated, as theCSF may contain detectable IgG antibody even in non-meningitic coccidioidomycosis (112). The coccidioidal LAtest should not be used to test CSF because of a high rate offalse-positives (107).
Pleural and pericardial effusions occur in patients withacute primary coccidioidomycosis. Both TP and IDTP anti-bodies may be detected in pleural fluid and the titer of CFand IDCF antibodies may be determined. Titers may be ashigh as in the serum, but more often they are lower (139,141). Serologically reactive pleural fluid in patients withunreactive serum has not been reported. Smith (136) de-scribed a patient with a tuberculous pleural effusion on oneside who then developed a coccidioidal pleural effusion onthe opposite side. However, no information was offered as tothe coccidioidal serologic activity of the fluid of the twosides.
Coccidioidal peritonitis can occur, with the peritonealfluid showing CF or precipitin and CF antibodies. The CFtiter may be the same or lower than that of the serum.Frequently, the serum CF titer is very high with coccidioidalperitonitis but the clinical prognosis is usually good.
Synovial fluid can also be used to support, by serologicreactivity, a diagnosis of coccidioidal synovitis or arthritis. Itis not known, however, whether the joint fluid of patientswith coccidioidal joint disease can be seronegative whiletheir serum is seropositive.
SEROLOGIC TESTS
Detection of Early Precipitin IgM AntibodyTP. The TP test is carried out by adding 0.2 ml of serum to
0.2 ml of coccidioidin solution (139, 141). Antigen comparedwith a reference lot of antigen should be of such a concen-tration that undiluted and 1:10 dilutions of antigen will reactwith known TP-positive sera. Smith et al. (139, 141) orig-inally included 1:40 and 1:100 dilutions of antigens to coverthe "zone of equivalence" usually expected in a quantitativeprecipitin test, but these are not required. As a control, thepatient's serum is added to culture medium similar to that inwhich coccidioidin was produced. The tubes are then shakenvigorously and placed in the 350C incubator. The test hasincorrectly been described as one in which antigen is over-laid on the serum (13, 132, 145). The tubes are incubated for24 h and then examined for presence of a translucentgelatinous button of precipitate by flicking the tube sharplyto dislodge the button from the bottom of the tube (Fig. 3). Ifno reaction is noted, the tubes are incubated again and readdaily for the next 3 days. In 85 to 90% of instances, the TPtest will show a precipitate in 24 h; only rarely will a reactionnot be evident within 48 h. Although various dilutions ofantigen have been used, the TP test has not been clearlystandardized as a quantitative test. Presence or absence ofTP reactivity is significant. The TP test is no longer recom-mended because of the greater sensitivity of the IDTP.
ID. In 1958, the double diffusion (Ouchterlony test) wasshown to yield a band of precipitate when coccidioidin wasdiffused through agar toward serum from a patient withcoccidioidomycosis (51). Subsequently, multiple bands ofprecipitation were obtained when various fractions derived
CLIN. MICROBIOL. REV.
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

SEROLOGY OF COCCIDIOIDOMYCOSIS 259
from coccidioidin were tested against sera from patients withcoccidioidomycosis (111). Huppert and Bailey (59-61) devel-oped the ID so that it could be used to detect antibody thatcorrelated with CF (the IDCF) and TP (the IDTP). Theyused culture filtrate antigen solution (FAS or F) for the IDCFtest and toluene lysate antigen solution (LAS or L) (110, 111)for the IDTP test, but in reality either of these antigensolutions can detect both kinds of antibody. The antigensolutions were concentrated, washed by ultrafiltration, andtitrated to obtain the optimal dilution for serologic tests.However, Huppert et al. (62) indicated that ultrafiltrationremoved most of the TP antigen. Based on the earlierobservations of Smith et al. (139) that the TP antigen is heatstable, Huppert and Bailey (61) heated the toluene or lysateantigen to 60'C for 30 min to inactivate CF (or IDCF)antigen. Their ID tests were carried out in 50-mm plasticpetri dishes containing 5 ml of agar. Seven wells, 4.5 mm indiameter, were cut in the agar in a hexagonal pattern withone well in the center. The wall to wall distance betweenwells was 5 mm. The volume required per well was 40 to 50RI. Other methods such as that of Kaufman and colleaguespermit the testing of smaller volumes of many specimens ina single 90-mm petri dish (76, 98). The serum (or other bodyfluid) is placed in the appropriate well and allowed toprediffuse at room temperature for 2 h, followed by additionof the appropriate antigen dilution. This prediffusion may beunnecessary for the detection of the IDCF reaction butappears essential in order to have the IDTP reaction, whichis dependent on slowly diffusing IgM, occur approximatelymidway between serum and antigen wells.Huppert and Bailey (60, 61) showed that ID reactions
could be read in 24 h with 69% of sera; 84% were positive at48 h and 100% were positive at 72 h. In our experience withconcentrated specimens, 85 to 90% of reactions detectableby ID are apparent in 24 h, most of the remainder becomingdetectable within 48 h. Only infrequently does a reactionappear with longer incubation. Nevertheless, we recom-mend that final readings be made at 96 h.Because the IDTP reaction depends on IgM, the concen-
tration of which is normally about 120 mg/dl (10-' M) ofserum (that of IgG is about 10-fold higher [wt/vol], 10-1 M)and because the IDTP reaction was often less clear than theIDCF, we adopted a method of evaporatively concentratingserum or other body fluids prior to the ID test. Because thisalso effected an increase in IgG reactive with coccidioidalantigen, it improved the sensitivity for both kinds of anti-body (109, 112). Our modification of the Huppert and Baileymethod also includes the use of heated and unheated anti-gens (in different wells) to detect IDTP (IgM) and IDCF(IgG), respectively. Using control human sera positive forIDTP and IDCF in the same ID plate allows testing for bothkinds of antibody in the same specimen (Fig. 4. middle).Huppert and Bailey (61) had proposed mixing optimal dilu-tions of IDTP and IDCF antigens to provide a single prepa-ration to detect both types of antibody. For most seracontaining both types of antibody, a single unheated antigensolution (e.g., selected at the optimal dilution to detect theIDCF reaction) can also detect IDTP antibody. However,when some sera with a low titer of CF antibody (e.g., 2 to 8)are tested, the IDCF reaction is obscured by the IDTPreaction. This can be shown by treating the bands with 0.05M dithiothreitol (in 0.2 M Tris hydrochloride buffer, pH 8.6)which damagesIgM and leads to dissolution of the IDTPband (Pappagianis et al., Abstr. Annu. Meet. Am. Soc.Microbiol. 1986). As a result, the underlying IDCF reactionis revealed because the IgG remains intact (Fig. 8).
FIG. 8. ID of serum that showed both IDTP and IDCF reactiv-ity. The latter was obscured by the IgM-antigen precipitate (top),but became evident following dissolution of theIgM-antigen precip-itate with dithiothreitol (bottom). (Wells as in legend to Fig. 4.)
Occasionally, interference has been noted in the ID test bythe formation of a band of precipitation resembling thatproduced by the IDTP reaction. The cause of the problem isunknown; however, we surmise that it may be the result ofreaction between coccidioidal antigens and C-reactive pro-tein (or related substances in serum) Such a reaction hadbeen reported with preparations derived from Aspergillusfumigatus (7, 16, 91, 116). The addition of an aqueoussolution (1.5%) of sodium EDTA leads to dissolution ofbands that may resemble IDTP, while the authentic IDTPbands are unaffected by such treatment. An additional bandof precipitation is frequently encountered with both heatedand unheated antigen. It does not form a line of identity witheither the IDTP or IDCF control and is not dissolved by
VOL. 3, 1990
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

260 PAPPAGIANIS AND ZIMMER
FIG. 9. Serum of a patient with coccidioidomycosis which showspresence of IgM and IgG reactions and has an additional undefinedreaction lying between the IgM and IgG bands. (Wells as describedin the legend to Fig. 4.)
EDTA or dithiothreitol (Fig. 9). Its identity and significanceare unknown.The substrate for ID tests can be agar, agarose, or gellan
gum, a polysaccharide produced by a Pseudomonas species.
We have used the last agent for over 3 years (approximately20,000 specimens tested) and have found it a satisfactorysubstitute for agar or agarose when testing human andanimal sera. (Rabbit serum, however, may not show thesame reactions in gellan gum that it does in agar.)LA. For the LA test, latex particles are coated with
coccidioidal antigen obtained by toluene autolysis of myce-
lial C. immitis or from culture filtrates. Originally, polysty-rene latex particles 0.15 to 0.35 [Lm in diameter were used(C. Mulder, S. Kiddy, and K. Lou, Abstr. Annu. Meet. Am.Soc. Microbiol. 1966, RT20, p. 141), but in more recentpreparations 0.8-gm particles are used. The antigen solutionis heated at 60'C to inactivate the antigenic components)reactive with complement. The commercial distributors alsohave recommended that the serum to be tested be heated at560C for 30 min to inactivate complement. Agglutination isread after 4 min.The LA test is more sensitive than TP, but it has yielded
at least 6% false-positive reactions (65). Results of LA testsreported to us from several different laboratories indicatethat, in general use, the rate of false-positives is higher.Because of this, a confirmatory test(s), preferably ID, mustfollow any positive LA. Very high rates of false-positive LAoccur with CSF or with sera that have been diluted (107)whether obtained from patients with coccidioidomycosis or
not. Because of this, the attempted application of LA as 4quantitative test (146) is likely to provide spurious informa-tion. While the LA test is designated as a test to detectantibody (IgM) corresponding to that detectable by TP, ourexperience shows that some LA-positive reactions are re-
ported with sera that are positive by IDCF (IgG) but not forIgM. The LA test has been useful in diagnosis of coccidioi-domycosis in the dog (155).
Detection of the CF IgG Antibody
CF. Smith et al. (139, 141) adapted the Kolmer CF test,mixing 0.25 ml of various dilutions of inactivated serum(560C for 30 min) with 0.25 ml of antigen and 0.5 ml ofcomplement adjusted to contain 2 U. Initially, complementbinding was effected by incubation for 2 h at 370C followedby addition of hemolysin-sensitized sheep erythrocytes andincubation for 1 h. The endpoint 4+ fixation of complementwas the last tube in which there was no evidence of hemo-lysis to the naked eye. This method permitted an earlyreading; however, Smith et al. (141) recognized that comple-ment binding carried out overnight at 40C resulted in CFtiters approximately twofold higher. Tests in several collab-orating laboratories affirmed the higher titer obtained withovernight binding at 40C (140), but because the different CFmethods were used, disparities in titers were seen.To develop a standardized procedure that could be uni-
versally adopted, comparisons of different CF methods (63)were carried out. The Smith CF macromethod, using over-night binding of complement at 4 to 50C, gave more repro-ducible results than the LBCF procedure (also using com-plement binding at 50C) in either its macro- or microdilutionversion (98). This result was unexpected because the LBCFmethod, although more complex, makes use of more objec-tive methods; e.g., extent of hemolysis is interpreted withhemoglobin color standards and a 50% hemolytic endpoint isused. In the LBCF, the last tube or well showing 30% or lesshemolysis is considered positive. The micro-LBCF requiresapproximately one-tenth the volume of serum, CSF, or otherfluid required by the Kolmer or macro-LBCF, and it hasbeen widely adopted. No direct comparison between themicro-LBCF and the original method of Smith et al. has beenreported; however, binding at 40C provides higher titers than2-h binding at 370C. In some instances, positive results areobtained after overnight test incubation at 40C but not at370C after 2 h (135). As ordinarily described, the LBCFtitration may begin with a 1:8 dilution of serum. Therefore,sera that are positive but only with titers of 2 or 4 wouldappear negative at the 1:8 dilution (98). Such low titers maybe encountered in early coccidioidal disease, limited dissem-ination, pulmonary residua, or late disease when the titer hasdeclined. The LBCF should begin with a 1:2 dilution if theIDCF is positive.Because CF titers of 2 to 8 may represent antibody
reacting with another, cross-reactive antigen (64, 139, 141),the presence of coccidioidal CF antibody should be verifiedin the initial specimen by the more specific ID test (76).Simultaneous testing of paired sequential sera is essential inview of possible test-to-test variation of CF and quantitativeID titers (135). Human serum from confirmed cases ofcoccidioidomycosis has served as a positive control for CFtests. Serum samples from horses injected intravenouslywith the hyphal-arthroconidial-phase C. immitis appeared tobe satisfactory for the CF test but were never put to routineuse (140). Serum samples from rabbits infected with C.immitis were also proposed as a reference standard (5) butnot adopted. The CF test has been applied to species otherthan humans and appears to yield results of similar signifi-cance to those found with human sera; i.e., the titers areproportional to severity of disease (4, 54, 55, 88, 92, 110, 120,121, 134, 145).IDCF. The evolution and use of the ID test have been
described above. In 1962, Schubert and Hampson (132)showed that CF-positive sera reacted in an ID test withcoccidioidin as antigen. Huppert and Bailey (59, 60) set forth
CLIN. MICROBIOL. REV.
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

SEROLOGY OF COCCIDIOIDOMYCOSIS 261
appropriate conditions for the performance of the IDCF,which detected antibody corresponding to that detected byCF. The test relied on selection of the appropriate dilution ofantigen, known to be heat labile, for the detection of IDCF.The dilution of antigen chosen, after 2-h prediffusion, yieldsa precipitate with antibody approximately midway betweenthe wells. The IDCF test can be carried out without predif-fusion of the serum. The higher the concentration of anti-body, the closer to the antigen well will be the antigen-antibody precipitate. The location of the precipitate can evenprovide a rough estimate of how many dilutions of serummay be needed to obtain the endpoint titer in the CF test.While many coccidioidal sera yield a positive IDCF resultwithout prior concentration, some specimens, e.g., fromwell-focalized pulmonary nodules or cavities, will not showIDCF reaction unless concentrated first. A control CF-positive human serum is used in each test.QID. The QID test for IDCF antibody is carried out by
diffusing various dilutions of serum against a fixed concen-tration of antigen previously determined to have appropriatereactivity. Several workers have studied the QID (48, 62, 71,151, 153). By refilling the antigen and serum wells 24 and 48h after the original filling and taking a final reading at 72 h,Wieden et al. (151) found that agreement between QID andCF titers (±+1 two-fold dilution) was 84.7%. The QID wastested with consecutive sera from the same patients. Al-though it tended to yield slightly lower titers than the CF testperformed by 2-h binding of complement at 370C, over timethe changes in titer were comparable. Others found similaragreement between CF and QID tests: 80% (61), 87% (I.Krasnow and M. Huppert, Abstr. Annu. Meet. Am. Soc.Microbiol. 1977, F54, p. 127), and 82% (147). The QID testrequires fewer reagents and smaller volumes than the CFtest. The manipulations are simpler, but no automation hasbeen used and the results are delayed (final reading after 48to 72 h). The QID test is practical for the laboratory thatcarries out few serologic determinations, but for large num-bers of specimens the CF test is more practical. QID isneeded when serum is anticomplementary and will not yielda readable titer by CF (frequent with canine sera) and forthose unusual sera that do not show fixation of complementbut yield a titer by QID (Fig. 10).
Table 2 summarizes pertinent characteristics of serologictests for coccidioidomycosis.
Miscellaneous/Experimental Tests for Antibody
Agar gel precipitation-inhibition test. The agar gel precip-itation-inhibition test is carried out by mixing serial dilutionsof serum with a suitable concentration of antigen to permitbinding of serum antibody to antigen. The mixture is thendiffused against a serum of known titer relative to thedilution of antigen. The endpoint is taken as the highestdilution of the patient's serum that bound antigen andprevented it from reacting with the reference serum ofknown titer. The endpoint is read after 48 h. No advantagewas apparent when compared with CF testing (120).CIE. CIE has been used for both qualitative and quanti-
tative antibody determination. With coccidioidin as antigen,both IDTP and IDCF antibodies were detected in sera ofdogs with coccidioidomycosis (133). All canine sera thatwere positive by CF (titers, 2 to 128) were positive by CIE.Human sera and CSF were tested by CIE, using spherulin;the CIE provided 100% correlation with ID and 98% corre-lation with CF results (1). The mean titer by CIE was 1 serialdilution lower than that obtained by CF. The nature of the
FIG. 10. QID test of human serum containing both IDTP andIDCF reactivity. The former is positive at 1:2 and 1:4 dilutions; thelatter is reactive through 1:32. Well C contains control IDCF-positive serum. The antigen (Ag) is unheated coccidioidin. Wells 2through 32 represent dilutions of patient serum 1:2 through 1:32.
antigens used in two other studies is uncertain as onereferred to a "toluene extract of culture filtrates" (82) andthe other referred to "spherule coccidioidin" (47). Theformer study found that 100% of sera with CF titers of >16were positive by CIE, but at lower CF titers CIE wasproportionately less sensitive, detecting only 64% when thetiter was 2. As Kozub et al. (82) pointed out, the sensitivityof the CIE would probably be improved by appropriateselection of reagents. However, if the sensitivity does notexceed that of ID, the advantage of more rapid results byCIE (1 to 2 h) may be of particular importance only in theinfrequent cases of rapidly progressing coccidioidomycosis.FA. FA methods have been used for the detection of both
C. immitis in infected tissue (74) and antibody in human sera(75). Histologic staining was accomplished by preparingantisera in rabbits injected with viable or nonviable arthro-conidia of C. immitis. The globulin fraction was separatedfrom the sera and conjugated with fluorescein isothiocya-nate. With this conjugate, endospores and the contents ofspherules fluoresced but the walls of spherules in infectedtissues did not, perhaps because antibody was alreadypresent on the surface of spherules in vivo. However, thewalls of spherules produced in vitro did react with thefluorescein-labeled antibody. This reagent provided a sensi-tive histologic method for the detection of C. immitis intissue and exudates. Its specificity was enhanced by prioradsorption with yeast cells of Histoplasma capsulatum or bydiluting antibody globulin induced by injection of rabbitswith viable (but not with killed) C. immitis arthroconidia(72).The one-step FA inhibition test was used to detect the
presence of coccidioidal antibody in human sera. Smears ofendospores prepared from the cut surface of infected mouselungs were exposed to a mixture (A) of fluorescein-labeledrabbit antibody plus unlabeled unknown serum. The inten-sity of staining was compared with that of endosporesexposed to a mixture (B) of fluorescein-labeled globulin andnormal serum (the negative control). In A, coccidioidal
VOL. 3, 1990
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

262 PAPPAGIANIS AND ZIMMER
TABLE 2. Serologic tests for coccidioidomycosis
Test Antigen Special considerations Detects Clinical correlation
TP Coccidioidin culture Patient serum mixed with IgM Valuable in acute disease, can revealfiltrate/autolysate "undiluted" and "1:10" the only serum antibody produced
antigen; control patient in early stages; rarely positive withserum plus culture me- CSF.dium. Now rarely used,supplanted by IDTP.
IDTP Same as TP; antigen Serum or other fluid con- IgM As above, but more sensitive thanshould be heated centrated and prediffused TP. Antibody detectable with someto eliminate reac- before antigen is placed chronic pulmonary cavities. Whentivity with IgG. in well. positive with CSF, acute meningitis
present.
LA or LPA Latex particles Very sensitive, but false- IgM (some reactions Valuable in acute disease for detec-coated with heat- positives occur; requires occur with sera tion of antibody in serum.treated toluene confirmatory test. Not showing only IgGautolysate useful with diluted serum by other test)
or with CSF.
CF (Cocsidioldin culture Valuable ter 4uantitation of IgG Later developing antibody but morehltrate/autolysate antibody in serum and persistent than IgM; rising titer re-
other body fluids; 2 h lates to extending disease, reduc-biiidirig ot complement at tion in titer relates to clinical im-3 7i useful with seia, piovement. Serum CF titer >16more sensitive 18-h bind- often associated with dissemina-ing of complement at 40C tion. CF-positive CSF usually indi-useful with CSF or serum. cates meningitis.
IDCF, qualitative Coccidioidin culture Serum or other fluid may be IgG Good qualitative screening test foror quantitative filtrate/autolysate tested unconcentrated IgG; when serum or CSF concen-
and without prediffusion, trated, more sensitive than CF (maybut sensitivity of qualita- show IgG in CSF even in absencetive test enhanced by of meningitis). Can be used as aconcn and prediffusion; quantitative test; titers approximatedilutions of specimen for those obtained by CF.quantitative IDCF.
antibody in the patient serum inhibited the uptake of thefluorescent tag by endospores. The FA inhibition testshowed a 93% correlation with CF-positive sera and waspositive with sera from some cases of coccidioidomycosisthat were negative by CF as well as some that were reactiveonly by TP.FA reagent produced against killed arthroconidia was also
used to visualize arthroconidia in the soil (72). This approachhas not yet been used for the direct identification of themycelial form of C. immitis (73) as has the exoantigenmethod (see below).RIA. A solid-phase RIA method was tested by Catanzaro
and Flatauer (15) as a means of detecting antibody in humansera. RIA values correlated well with the clinical status ofpatients with pulmonary coccidioidomycosis (type of pulmo-nary disease not given) and with the CF titer in disseminatedinfections.ELISA. Several groups of workers have studied detection
of coccidioidal antibody by ELISA (S. P. Lindsay, N.Bodie, and D. Pappagianis, Proc. Annu. Meet. Coccidioido-mycosis Study Group 1981, p. 1; S. I. Freeman, C. Burke,and R. Talbot, Proc. Annu. Meet. CoccidioidomycosisStudy Group 1982, p. 4; R. C. Talbot, R. C. Johnson, and J.Leonard, Proc. Annu. Meet. Coccidioidomycosis StudyGroup 1986, p. 3; J. Leonard and R. Talbot, Proc. Annu.Meet. Coccidioidomycosis Study Group 1987, p. 11; J. N.Galgiani, L. Lundergan, G. Grace, and K. 0. Dugger, Proc.Annu. Meet. Coccidioidomycosis Study Group 1989, p. 1).
A consistent shortcoming, found in about 10% of sera tested,is the inability to distinguish clearly between patient (posi-tive) and control (negative) sera, as determined by conven-tional tests. Thus far, the closest correlation has beenobtained between IDTP and ELISA. In a study of 792 sera,Leonard and Talbot reported an 89% agreement betweenELISA and the TP test but 100% agreement between IDTPand ELISA, using anti-human globulin as the secondaryantibody. In a separate study, Talbot et al. found that a largenumber of patients had CSF antibodies detectable by ELISAbut not by CF. None of these patients ever developedcoccidioidal meningitis, indicating that the greater sensitivityof the ELISA makes it unreliable for the detection ofmeningitis. This finding resembles that noted earlier forIDCF tests with concentrated CSF. The IDCF was overlysensitive because it detected IgG antibody in the CSF ofpatients with nonmeningitic coccidioidomycosis (112). Coleet al. tested antibody response to an isolated immunoreac-tive spherule wall antigen (20). Using anti-IgM in the ELISAthey found overlapping optical density values between serafrom patients and controls. When anti-IgG was the detectingantibody, there was clear differentiation between CF-posi-tive and -negative sera; however, there was no correlationbetween CF titers and ELISA values, as noted also byLindsay et al.We recently studied various coccidioidin, spherule-endo-
spore, and synthetic (3-O-methylmannose-based) antigens inthe conduct of coccidioidal ELISA, using 400 sera. The use
CLIN. MICROBIOL. REV.
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

SEROLOGY OF COCCIDIOIDOMYCOSIS 263
of 20% normal goat serum as an ELISA diluent rather thantraditional phosphate-buffered saline with Tween 20 pro-vided a better distinction between IDTP-positive and-negative sera and a 97% correlation between ELISA andIDTP in serum when anti-IgM was used. Levels of anticoc-cidioidal IgG did not correlate with CF activity regardless ofELISA reagents (B. Zimmer, D. Pappagianis, K. VanHoo-sear, and M. B. Goren, Abstr. Annu. Meet. Am. Soc.Microbiol. 1990, F56, p. 418).
CROSS-REACTIVITY
The issue of serologic specificity and cross-reactivity ofcoccidioidal reagents has been raised in a number of reports.Smith et al. (139) obtained negative coccidioidal serologictests from patients with tuberculosis, brucellosis, primaryatypical (mycoplasmal) pneumonia, actinomycosis, influ-enza, syphilis, typhoid fever, tularemia, leptospirosis, per-tussis, Q fever, smallpox, measles, and psittacosis. Negativeserologic tests were also obtained with sera from patientswith blastomycosis and cryptococcosis. However, Smith etal. as well as Campbell and Binkley (13), Salvin et al. (127),and Heiner (51) observed cross-reactions (positive coccidi-oidal serology, using coccidioidin) with sera from patientswith histoplasmosis. Campbell and Binkley (13) studied theproblem of cross-reactivity systematically and concludedthat sera from patients with histoplasmosis rarely cross-reacted with coccidioidin in the CF test, and when suchcross-reactions occurred, they yielded low titers comparedwith those produced with histoplasmal antigen. However,sera from "mild" and primary cases of coccidioidomycosisgave higher CF titers with Histoplasma and Blastomycesantigens than with Coccidioides antigen (11, 12). As coccid-ioidal CF titers increased in patients with coccidioidomyco-sis, heterologous CF titers decreased. When a toluene-induced autolysate of C. immitis hyphae was used as antigenin the CF test, no cross-reactivity was shown by a smallnumber of sera from humans with histoplasmosis (114).Coccidioidin used in the CF test yielded cross-reactions withsera from cases of histoplasmosis and from a patient withblastomycosis and candidiasis (76). Huppert et al. (64) foundthat both spherulin and coccidioidin in CF tests yieldedreactions with sera from several other mycoses caused byPseudallescheria boydii, Aspergillus spp., B. dermatitidis,H. capsulatum, Phialophora (Fonsecaea) pedrosoi, Can-dida albicans, Candida parapsilosis, Cryptococcus neofor-mans, and Torulopsis glabrata. Recently, we noted anatypical IDTP reaction with serum from a patient with activehistoplasmosis and no known coccidioidomycosis.
Sera from patients with various nonmycotic diseases werereported to fix complement in tests with coccidioidin (76,132). These diseases included actinomycoses, tuberculosis,pneumococcal pneumonia, staphylococcal empyema, cen-tral nervous system malacia, macular degeneration, pulmo-nary carcinoma, and regional enteritis. Serum from patientswith sarcoidosis did not react with coccidioidal antigen (17,70).Huppert et al. (63) reported that 20%o of sera from patients
with noncoccidioidal mycoses gave positive reactions by CFtests when coccidioidin was used, and 48% gave positivereactions when spherulin was used. These are inordinatelyhigh percentages considering the reported specificity ofcoccidioidin. Nevertheless, these and other data affirm theneed for performing concomitant ID tests, at least with initialsera to confirm the presence of coccidioidal antibody (76).Based on the data of Huppert et al. (64), we should have
detected a sizable proportion of sera positive by CF butnegative by ID, i.e., disease not confirmed by the latter,more specific test. Indeed, among 80,000 specimens wetested over the past 8.5 years, including some 6,000 newlyrecognized and several thousand old cases of coccidioido-mycosis, 3 were positive by CF and not by ID, a muchsmaller fraction of false-positives than reported by Huppertet al. (64).The explanation for cross-reacting antibody in sera from
patients with mycoses and nonmycotic diseases has not yetbeen provided. By ID, Heiner (51) demonstrated a reactionbetween coccidioidal antigen and the serum of one of severalpatients with histoplasmosis. He concluded that a reactiveantigenic component, "c," was present also in histoplasmin.Kaplan and Clifford (74) prepared anticoccidioidal globulinfrom rabbits for FA tests. The globulin reacted with H.capsulatum and B. dermatitidis, but the cross-reactive com-ponent was removed by adsorption with H. capsulatumyeast cells. By two-dimensional immunoelectrophoresis,Huppert et al. (58) showed 9 H. capsulatum and 11 B.dermatitidis antigens in coccidioidal antigen preparations.The 3-O-methylmannose present in coccidioidal antigen
could explain cross-reactivity with some organisms, e.g.,Streptomyces griseus (14), members of the family Entero-bacteriaceae (97), mycobacteria (S. K. Maitra and C. E.Ballou, Fed. Proc. 33:1686, 1974), or the fungus Mal-branchea dendritica (19). However, 3-O-methylmannose hasnot been demonstrated in H. capsulatum or B. dermatitidis.Infrequently, sera yield reactions in ID tests with coccidi-oidin but no line of identity with control sera from patientswith coccidioidomycosis. Recently, we observed such areaction with serum from a man with Mycobacterium aviumpulmonary disease. Whether these sera contain antibodyproduced against one of the heterologous organisms contain-ing 3-O-methylmannose or a similar sugar (e.g., 3-O-meth-ylgalactose, which is the madurose from Actinomaduramadurae) has not been determined.
ANTIGEN DETECTION
Detection of antigen would be useful in two particularsituations: very early coccidioidomycosis (probably 1 week),between onset of symptoms and delectability of IgM; and inpatients whose humoral responsiveness is delayed or want-ing. The latter group includes those with hypogammaglobu-linemia or another immunodeficient state.Weiner (148) developed a RIA for coccidioidal antigen in
human sera. Immunoreactive fractions of molecular weightsbetween 200,000 and 230,000 (see section on antigens) wereobtained by chromatographic separation, and these wereconjugated to tyramine and radiolabeled with 1251I. Theantigen appeared to be a protein-carbohydrate conjugate inwhich the carbohydrate represented a critical epitope be-cause mild periodate oxidation led to loss of antigenicactivity. Sera were tested after acidification and heating at96°C for 20 min. All nine patients studied by Weiner haddetectable antibody at the time the test for antigen wascarried out, except a renal transplant recipient who wasnegative for both antigen and antibody. This patient subse-quently developed detectable antibody by the IDTP test.
Galgiani et al. (40) used an inhibition ELISA to detectantigen. Human serum obtained during primary coccidioidalpneumonia was mixed with rabbit antibody to spherulin topermit the antigen in the human serum to react with lapineantibody. The concentration of rabbit antibody remainingunreacted was then measured in spherulin-coated cuvettes.
VOL. 3, 1990
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

264 PAPPAGIANIS AND ZIMMER
Normal human serum to which known amounts of antigenwere added was used to construct a standard curve. Antigenactivity was highest at 2 and 6 weeks after onset of illnessand declined thereafter through 4 months and beyond.Immunoglobulin isotype antibody levels measured in the
ELISA showed changes in IgM (but not IgG or IgA) virtuallyparallel to antigen levels in the patient sera. This led theauthors to suggest that this relationship resulted from im-mune complex formation. They noted, however, that normalhuman serum, immune human serum, or fetal calf serum (toa lesser extent) could interfere with antigen assays in thatthese sera reacted nonspecifically with spherulin adsorbed tothe plastic cuvette (41). Of the three major isotypes, IgMexerted the greatest degree of interference. This interferencecould be largely overcome by acidification and heating of theserum (147, 148). All of 14 sera from 13 patients with acutepulmonary coccidioidomycosis had detectable antigen; how-ever, no quantity was presented as the minimum level ofdetectable antigen. Therefore, there is uncertainty as to thesignificance of several readings given as "<0.1" or "<0.2"pug/ml. Three of 13 serum samples tested had antigen detect-able in the absence of detectable IDTP or IDCF antibody inunconcentrated specimens. One serum sample with detect-able antigen was not tested for antibody. Of the 10 serumsamples positive for antibody, 3 had antigen levels of <0.2pug/ml. The authors concluded that the assay of antigen insera had not been sufficiently developed to use as a diagnos-tic method.
In part, the problem of establishing an assay for antigenmay lie in the occurrence of varying immune complexes.Gamble and Ruggles (43) demonstrated the presence of amixed cryoglobulin (IgAl-IgG3,4) associated with glomeru-lonephritis in a patient with a history of coccidioidomycosissome 30 years previously and a pulmonary lesion that morerecently underwent cavitation. The IgG portion of the cry-oglobulin reacted with coccidioidin, indicating the probableparticipation of immune complexes of coccidioidal antigenand IgG in the formation of IgA-IgG glomerular deposits.Furthermore, Yoshinoya et al. (154) demonstrated coccidi-oidal antigen-antibody complexes which, by ultracentrifuga-tion, sedimented in the range of 6.6S to 19S and theconcentration of which correlated with CF antibody titers.Subsequently, Cox et al. (27) reported that the concentrationof immune complexes was proportional to IgG concentrationand to CF titer only at low and intermediate titers, but less soat high titers. The acid-heat treatment of Weiner (148) and ofWack and colleagues (147) would inactivate the CF-reactiveantigen and probably destroy its delectability by antibody inan ELISA or similar assay.
Antigen detection may thus best be accomplished by amethod that would permit nonimmunologic detection of bothheat-stable and heat-labile coccidioidal antigen or a deriva-tive of coccidioidal antigens. Detection of the 3-0-methyl-mannose of coccidioidal antigen may obviate the problemsinherent in detection of intact antigen.
EXOANTIGEN TESTING
Exoantigen serologic testing developed by Standard andKaufman (143) has permitted identification of mycelial-phaseC. immitis without the tedious necessity of converting it tothe spherule-endospore phase in vivo or under special invitro conditions. It has even been used to identify C. immitisin the presence of contaminating organisms (37). Mycelial-phase cultures produce an exoantigen that is heat stable (HS)at 56°C for 30 min and specific for this fungus (67, 143). HS
exoantigen is used for rapid identification of C. immitis inculture by testing a filtrate of the suspected fungus by IDagainst a reference antiserum produced against heat-stableexoantigen (77). This IDHS reaction is different and distinctfrom reactions classified as IDTP (also involving a heat-stable antigen) or IDCF in human sera. The occurrence ofIDHS antibody in these human sera is rare (78).Antigen resembling HS antigen was demonstrated in (i)
Formalin-treated mycelial culture filtrate, (ii) toluene autoly-sate and a mixture of non-Formalin-treated mycelial culturefiltrate, and (iii) toluene autolysate and a mixture of non-Formalin-treated mycelial culture filtrate plus toluene au-tolysate (28). This antigen did not bind to concanavalin Aand was considered likely to correspond to the Agli de-scribed by Huppert et al. (66). However, other work hintedat a relationship between HS antigen and antigen designatedCS which differs from Agli (22).
FUTURE DIRECTIONS
Future directions in coccidioidal serology should includemolecular genetics methods that can lead to purified andwell-characterized reagents. Methods should be devised forthe reliable detection of antigen to permit diagnosis beforeantibody is produced or in patients whose production ofantibody is insufficient. While specific antibody for thedetection of antigen, e.g., one that contains 3-0-methylman-nose, may provide desirable specificity, there may be a needfor greater breadth of antigen detection for appropriatesensitivity. ELISA and other as yet undeveloped methodsmay provide an approach to greater test sensitivity, but theymust be able to detect antigen or antibody at various stagesof coccidioidomycosis and must provide the prognosticquantitative results currently available from the venerableCF test. The rapid, specific identification of C. immitis incultures as well as in sputum, exudate, or tissue should beenhanced by application of FA or enzyme-linked methods.Whatever means are adopted for serodiagnosis of coccidioi-domycosis must also be consonant with environmentalsafety.
ACKNOWLEDGMENT
We are very grateful to Lynn Diaz for her role in the preparationof this review.
LITERATURE CITED1. Aguilar-Torres, F. G., L. J. Jackson, J. E. Ferstenfeld, D.
Pappagianis, and M. W. Rytel. 1976. Counterimmunoelectro-phoresis in the detection of antibodies against Coccidioidesimmitis. Ann. Intern. Med. 85:740-744.
2. Ajello, L., K. Walls, J. C. Moore, and R. Falcone. 1959. Rapidproduction of complement fixation antigens for systemic my-cotic diseases. I. Coccidioidin: influence of media and mechan-ical agitation on its development. J. Bacteriol. 77:753-756.
3. Beck, M. D., E. C. Dickson, and E. Rixford. 1931. Coccidioidalgranuloma. Calif. State Dep. Public Health Bull. 57.
4. Biddle, M., E. M. Butt, G. Jacobson, and J. F. Kessel. 1953.Pathogenesis of coccidioidomycosis in Macacca mulatta. AttiVI Congr. Int. Microbiol. (Rome) 4:80-86.
5. Bieberdorf, F. W., and K. W. Chambliss. 1955. A positive testfor coccidioidin complement fixation. Public Health Rep. 70:771-774.
6. Blumenkranz, M. S., and D. A. Stevens. 1980. Endogenouscoccidioidal endophathlmitis. Ophthalmology 87:974-984.
7. Borglum-Jensen, T. D., H. Schonheyder, P. Anderson, and A.Stenderup. 1986. Binding of C-reactive protein to Aspergillusfumigatus fractions. J. Med. Microbiol. 21:173-177.
8. Brewer, J. H., C. L. Parrott, and D. Rimland. 1982. Dissemi-
CLIN. MICROBIOL. REV.
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

SEROLOGY OF COCCIDIOIDOMYCOSIS 265
nated coccidioidomycosis in a heart transplant recipient. Sab-ouraudia 20:261-265.
9. Calhoun, D. L., J. N. Galgiani, C. Zukoski, and J. G. Copeland.1985. Coccidioidomycosis in recent renal or cardiac transplantrecipients, p. 312-318. In H. E. Einstein and A. Catanzaro(ed.), Proceedings of the Fourth International Symposium on
Coccidioidomycosis. National Foundation for Infectious Dis-ease, Washington, D.C.
10. Calhoun, D. L., E. 0. Osir, K. 0. Dugger, J. N. Galgiani, andJ. H. Law. 1986. Humoral antibody responses to specificantigens of Coccidioides immitis. J. Infect. Dis. 154:265-272.
11. Campbell, C. C. 1960. The accuracy of serologic methods indiagnosis. Ann. N.Y. Acad. Sci. 89:163-177.
12. Campbell, C. C. 1968. Use and interpretation of serologic andskin tests in the respiratory mycoses. Dis. Chest 54(Suppl.1):305-310.
13. Campbell, C. C., and G. E. Binkley. 1953. Serologic diagnosiswith respect to histoplasmosis, coccidioidomycosis and blas-tomycosis and the problem of cross reactions. J. Lab. Clin.Med. 42:896-906.
14. Candy, D. J., and J. Baddiley. 1966. 3-O-methyl-D-mannosefrom Streptomyces griseus. Biochem. J. 98:15-18.
15. Catanzaro, A., and F. Flatauer. 1983. Detection of serumantibodies in coccidioidomycosis by solid-phase radioimmuno-assay. J. Infect. Dis. 147:32-39.
16. Chaparas, S. D., L. Kaufman, S. J. Kim, and D. W. McLaugh-lin. 1980. Characterization of antigens from Aspergillus fumi-gatus. V. Reactivity in immunodiffusion tests with serumsfrom patients with aspergillosis caused by Aspergillus flavus,A. niger and A.fumigatus. Am. Rev. Respir. Dis. 122:647-648.
17. Chapman, J. S. 1961. Mycobacterial and mycotic antibodies insera of patients with sarcoidosis. Ann. Intern. Med. 55:918-924.
18. Cohen, I. M., J. N. Galgiani, D. Potter, and D. A. Ogden. 1982.Coccidioidomycosis in renal replacement therapy. Arch. In-tern. Med. 142:489-494.
19. Cole, G. T., J. W. Chinn, L. M. Pope, and P. Starr. 1985.Characterization and distribution of 3-O-methylmannose inCoccidioides immitis, p. 130-145. In H. E. Einstein and A.Catanzaro (ed.), Proceedings of the Fourth International Con-ference on Coccidioidomycosis. The National Foundation forInfectious Diseases, Washington, D.C.
20. Cole, G. T., T. N. Kirkland, M. Franco, S. Zhu, L. Yuan, S. H.Sun, and V. N. Hearn. 1988. Immunoreactivity of a surfacewell fraction produced by spherules of Coccidioides immitis.Infect. Immun. 56:2695-2701.
21. Cole, G. T., L. M. Pope, M. Huppert, S. H. Sun, and P. Starr.1985. Wall composition of different cell types of Coccidioidesimmitis, p. 112-129. In H. E. Einstein and A. Catanzaro (ed.),Coccidioidomycosis. Proceedings of the Fourth InternationalConference on Coccidioidomycosis. The National Foundationfor Infectious Disease, Washington, D.C.
22. Cole, G. T., K. R. Seshan, M. Franco, E. Bukownik, S. H. Sun,and V. M. Hearn. 1988. Isolation and morphology of animmunoreactive outer wall fraction produced by spherules ofCoccidioides immitis. Infect. Immun. 56:2686-2694.
23. Cole, G. T., S. Zhu, S. Pan, L. Yuan, D. Kruse, and S. H. Sun.1989. Isolation of antigens with proteolytic activity from Coc-cidioides immitis. Infect. Immun. 57:1524-1534.
24. Collins, M. S., D. Pappagianis, and J. Yee. 1977. Enzymaticsolubilization of precipitin and complement fixing antigen fromendospores, spherules and spherule fractions of Coccidioidesimmitis, p. 429-444. In L. Ajello (ed.), Coccidioidomycosis.Current clinical and diagnostic status. Symposia Specialists,Miami.
25. Converse, J. L. 1957. Effect of surface active agents onendosporulation of Coccidioides immitis in a chemically de-fined medium. J. Bacteriol. 74:106-107.
26. Cooke, J. V. 1914. Immunity tests in coccidioidal granuloma.Proc. Soc. Exp. Biol. Med. 12:35.
27. Cox, R. A., B. S. Baker, and D. A. Stevens. 1982. Specificity ofimmunoglobulin E in coccidioidomycosis and correlation withdisease involvement. Infect. Immun. 37:609-616.
28. Cox, R. A., and L. A. Britt. 1986. Isolation of a coccidioidincomponent that reacts with immunoglobulin M precipitin anti-body. Infect. Immun. 53:449-453.
29. Cox, R. A., and L. A. Britt. 1987. Antigenic identity ofbiologically active antigens in coccidioidin and spherulin. In-fect. Immun. 55:2590-2596.
30. Cox, R. A., L. A. Britt, and R. A. Michael. 1987. Isolation ofCoccidioides immitis F antigen by immunoaffinity chromatog-raphy with monospecific antiserum. Infect. Immun. 55:227-232.
31. Cox, R. A., M. Huppert, P. Starr, and L. A. Britt. 1984.Reactivity of alkali-soluble, water-soluble cell wall antigen ofCoccidioides immitis with anti-Coccidioides immunoglobulinM precipitin antibody. Infect. Immun. 43:502-507.
32. Davis, D. J. 1924. Coccidioidal granuloma with certain sero-logic and experimental observations. Arch. Dermatol. Syph-ilol. 9:577-587.
33. Demartini, J. C., and W. E. Riddle. 1969. Disseminated coc-cidioidomycosis in two horses and a pony. J. Am. Vet. Med.Assoc. 155:149-156.
34. Deresinski, S. C., H. B. Levine, P. C. Kelly, R. J. Creasman,and D. A. Stevens. 1977. Spherulin skin testing and histoplas-mal and coccidioidal serology: lack of effect. Am. Rev. Respir.Dis. 116:1116-1118.
35. Deresinski, S. C., and D. A. Stevens. 1975. Coccidioidomycosisin compromised hosts. Medicine (Baltimore) 54:377-395.
36. Difco Laboratories. 1953. Difco manual, p. 270-271. DifcoLaboratories, Detroit.
37. DiSalvo, A. F., A. A. Terreni, and A. K. Wooten. 1981. The useof the exoantigen test to identify Blastomyces dermatitidis,Coccidioides immitis, and Histoplasma capsulatum in mixedcultures. Am. J. Clin. Pathol. 75:825-826.
38. Dolan, M. J., R. A. Cox, V. Williams, and S. Woolley. 1989.Development and characterization of a monoclonal antibodyagainst the tube precipitin antigen of Coccidioides immitis.Infect. Immun. 57:1035-1039.
39. Galgiani, J. N., K. 0. Dugger, N. M. Ampel, S. H. Sun, andJ. H. Law. 1988. Extraction of serologic and delayed hyper-sensitivity antigens from spherules of Coccidioides immitis.Diagn. Microbiol. Infect. Dis. 11:65-80.
40. Galgiani, J. N., K. 0. Dugger, J. I. Ito, and M. A. Wieden.1984. Antigenemia in primary coccidioidomycosis. Am. J.Trop. Med. Hyg. 33:645-649.
41. Galgiani, J. N., J. I. Ito, and K. 0. Dugger. 1985. Enzyme-linked immunosorbent assay detection of coccidioidal antigensin human serum, p. 239-249. In H. E. Einstein and A.Catanzaro (ed.), Coccidioidomycosis. Proceedings of theFourth International Conference on Coccidioidomycosis. TheNational Foundation for Infectious Diseases, Washington,D.C.
42. Galgiani, J. N., R. Hayden, and C. M. Payne. 1982. Leukocyteeffects on the dimorphism of Coccidioides immitis. J. Infect.Dis. 146:56-63.
43. Gamble, C. N., and S. W. Ruggles. 1978. Immunopathogenesisof glomerulonephritis associated with mixed cryoglobulinemia.N. Engl. J. Med. 299:81-84.
44. Gifford, M. A. 1936. Annual Report Kern County HealthDepartment for the Fiscal Year July 1, 1935 to June 30, 1936,p. 22-23. Kern County Health Department, Bakersfield, Calif.
45. Gifford, M. A., W. R. Buss, and R. J. Douds. 1937. AnnualReport Kern County Health Department for the Fiscal YearJuly 1, 1936 to June 30, 1937, p. 39-54. Kern County HealthDepartment, Bakersfield, Calif.
46. Goldstein, E., M. J. Winship, and D. Pappagianis. 1972. Ven-tricular fluid and the management of coccidioidal meningitis.Ann. Intern. Med. 77:243-246.
47. Graham, A. R., and K. J. Ryan. 1980. Counterimmunoelectro-phoresis employing coccidioidin in serologic testing for coccid-ioidomycosis. Am. J. Clin. Pathol. 73:574-577.
48. Hampson, C. R., and T. R. Larwood. 1967. Observations oncoccidioidomycosis immunodiffusion tests with clinical corre-lations, p. 211-214. In L. Ajello (ed.), Coccidioidomycosis.University of Arizona Press, Tucson.
VOL. 3, 1990
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

266 PAPPAGIANIS AND ZIMMER
49. Hassid, W. Z., E. E. Baker, and R. M. McCready. 1943. Animmunologically active polysaccharide produced by Coccidi-oides immitis Rixford and Gilchrist. J. Biol. Chem. 149:303-311.
50. Hector, R. F., and D. Pappagianis. 1982. Enzymatic degrada-tion of the walls of spherules of Coccidioides immitis. Exp.Mycol. 6:136-152.
51. Heiner, D. C. 1958. Diagnosis of histoplasmosis using precip-itin reactions in agar gel. Pediatrics 22:616-627.
52. Hirsch, E. F., and D. d'Andrea. 1927. The specific substance ofCoccidioides immitis. J. Infect. Dis. 40:634-637.
53. Hirsch, E. F., and D. d'Andrea. 1927. Sensitization of guineapigs with broth culture filtrates and with killed mycelium ofCoccidioides immitis. J. Infect. Dis. 40:638-640.
54. Hood, H. B., and J. N. Galgiani. 1985. Treatment of a malelowland gorilla for coccidioidomycosis with ketoconazole atthe Phoenix Zoo, p. 288-291. In H. E. Einstein and A.Catanzaro (ed.), Proceedings of the Fourth International Sym-posium on Coccidioidomycosis. National Foundation for In-fectious Diseases, Washington, D.C.
55. Hugenholtz, P. G., R. E. Reed, K. T. Maddy, R. J. Trautman,and J. D. Barger. 1958. Experimental coccidioidomycosis indogs. Am. J. Vet. Res. 19:433-439.
56. Huntington, R. W. 1977. Acute fatal coccidioidal pneumonia,p. 127-137. In L. Ajello (ed.), Coccidioidomycosis. Currentclinical and diagnostic status. Symposia Specialists, Miami.
57. Huppert, M. 1970. Serology of coccidioidomycosis. Myco-pathologia 41:107-113.
58. Huppert, M., J. P. Adler, E. H. Rice, and S. H. Sun. 1979.Common antigens among systemic disease fungi analyzed bytwo-dimensional immunoelectrophoresis. Infect. Immun. 23:479-485.
59. Huppert, M., and J. W. Bailey. 1963. Immunodiffusion as ascreening test for coccidioidomycosis serology. Sabouraudia2:284-291.
60. Huppert, M., and J. W. Bailey. 1965. The use of immunodif-fusion tests in coccidioidomycosis. I. The accuracy and repro-ducibility of the immunodiffusion test which correlates withcomplement fixation. Am. J. Clin. Pathol. 44:364-368.
61. Huppert, M., and J. W. Bailey. 1965. The use of immunodif-fusion tests in coccidioidomycosis. II. An immunodiffusiontest as a substitute for the tube precipitin test. Am. J. Clin.Pathol. 44:369-373.
62. Huppert, M., J. W. Bailey, and P. Chitjian. 1967. Immunodif-fusion as a substitute for complement fixation and tube precip-itin tests in coccidioidomycosis, p. 221-225. In L. Ajello (ed.),Coccidioidomycosis. University of Arizona Press, Tucson.
63. Huppert, M. H., P. A. Chitjian, and A. J. Gross. 1970.Comparison of methods for coccidioidomycosis complementfixation. Apple. Microbiol. 20:328-330.
64. Huppert, M. H., I. Krasnow, K. R. Vukovich, S. H. Sun, E. H.Rice, and L. J. Kutner. 1977. Comparison of coccidioidin andspherulin in complement fixation tests for coccidioidomycosis.J. Clin. Microbiol. 6:33-41.
65. Huppert, M., E. T. Peterson, S. H. Sun, P. A. Chitjian, andW. J. Derrevere. 1968. Evaluation of a latex particle aggluti-nation test for coccidioidomycosis. Am. J. Clin. Pathol. 49:96-102.
66. Huppert, M., N. S. Spratt, K. R. Vukovich, S. H. Sun, andE. H. Rice. 1978. Antigenic analysis of coccidioidin and spher-ulin determined by two-dimensional electrophoresis. Infect.Immun. 20:541-551.
67. Huppert, M., S. H. Sun, and E. H. Rice. 1978. Specificity ofexoantigens for identifying cultures of Coccidioides immitis. J.Clin. Microbiol. 8:346-348.
68. Hurwitz, S., J. E. Young, and B. V. Eddie. 1938. Coccidioidesimmitis intradermal skin reaction; preliminary report of 449cases. Calif. West. Med. 48:87-89.
69. Jacobson, H. P. 1928. Coccidioidal granuloma: specific allergiccutaneous reaction; experimental and clinical observations.Arch. Dermatol. Syphilol. 18:562-567.
70. Johnson, J. E., R. A. DeRemee, F. Kueppers, and G. D.Roberts. 1977. Prevalence of fungal complement-fixing anti-
bodies in sarcoidosis. Am. Rev. Respir. Dis. 116:145-147.71. Johnson, J. E., B. Jeffrey, and M. Huppert. 1985. Detection of
Coccidioides immitis antibody by five commercially availableimmunodiffusion kits, p. 264-272. In H. E. Einstein and A.Catanzaro (ed.), Proceedings of the Fourth International Sym-posium on Coccidioidomycosis. National Foundation for In-fectious Diseases, Washington, D.C.
72. Kaplan, W. 1967. Application of the fluorescent antibodytechnique to the diagnosis and study of coccidioidomycosis, p.227-232. In L. Ajello (ed.), Coccidioidomycosis. University ofArizona Press, Tucson.
73. Kaplan, W. 1973. Direct fluorescent antibody tests for thediagnosis of mycotic diseases. Ann. Clin. Lab. Sci. 3:25-29.
74. Kaplan, W., and M. K. Clifford. 1964. Production of fluores-cent antibody reagents specific for the tissue form of Coccid-ioides immitis. Am. Rev. Respir. Dis. 89:651-658.
75. Kaplan, W., M. Huppert, D. E. Kraft, and J. Bailey. 1966.Fluorescent antibody inhibition test for Coccidioides immitisantibodies. Sabouraudia 5:1-6.
76. Kaufman, L., and M. J. Clark. 1974. Value of the concomitantuse of complement fixation and immunodiffusion tests in thediagnosis of coccidioidomycosis. Appl. Microbiol. 28:641-643.
77. Kaufman, L., and P. Standard. 1978. Improved version of theexoantigen test for identification of Coccidioides immitis andHistoplasma capsulatum cultures. J. Clin. Microbiol. 8:42-45.
78. Kaufman, L., P. G. Standard, M. Huppert, and D. Pappagianis.1985. Comparison and diagnostic value of the coccidioidin heatstable (HS and tube precipitin) antigens in immunodiffusion. J.Clin. Microbiol. 22:515-518.
79. Kessel, J. F. 1939. The coccidioidin skin test. Am. J. Trop.Med. 19:199-204.
80. Klotz, S. A., D. J. Drutz, M. Huppert, S. H. Sun, and P. L.DeMarsh. 1984. The critical role of CO2 in the morphogenesisof Coccidioides immitis in cell-free subcutaneous chambers. J.Infect. Dis. 150:127-134.
81. Kong, Y.-C. M., H. B. Levine, and C. E. Smith. 1963. Immu-nogenic properties of nondisrupted and disrupted spherules ofCoccidioides immitis in mice. Sabouraudia 2:131-142.
82. Kozub, W. R., N. Leas, R. J. Otto, and C. K. Dutt. 1977.Application of counterimmunoelectrophoresis in coccidioido-mycosis, p. 445-452. In L. Ajello (ed.), Coccidioidomycosis.Current clinical and diagnostic status. Symposia Specialists,Miami.
83. Kruse, D., and G. T. Cole. 1990. Isolation of tube precipitinantibody-reactive fractions of Coccidioides immitis. Infect.Immun. 58:169-178.
84. Landay, M. A., R. W. Wheat, N. F. Conant, and E. P. Lowe.1967. Serological comparison of the three morphologicalphases of Coccidioides immitis by the agar gel diffusionmethod. J. Bacteriol. 93:1-6.
85. Landay, M., R. W. Wheat, N. F. Conant, E. P. Lowe, and J. L.Converse. 1967. Studies on the comparative serology of thespherule and arthrospore growth forms of Coccidioides immi-tis, p. 233-236. In L. Ajello (ed.), Coccidioidomycosis. Uni-versity of Arizona Press, Tucson.
86. Levine, H. B., J. M. Cobb, and G. M. Scalarone. 1969.Spherule coccidioidin in delayed dermal sensitivity reactionsof experimental animals. Sabouraudia 7:20-32.
87. Levine, H. B., J. M. Cobb, and C. E. Smith. 1960. Immunity tococcidioidomycosis induced in mice by purified spherule,arthrospore, and mycelial vaccines. Trans. N.Y. Acad. Sci.22:436-449.
88. Levine, H. B., R. L. Miller, and C. E. Smith. 1962. Influence ofvaccination on respiratory coccidioidal disease in Cynomol-gous monkeys. J. Immunol. 89:242-251.
89. Levine, H. B., D. Pappagianis, and J. M. Cobb. 1970. Devel-opment of vaccines for coccidioidomycosis. Mycopathologia41:177-185.
90. Lombard, C. M., H. D. Tazelaar, and D. L. Krasne. 1987.Pulmonary eosinophilia in coccidioidal infections. Chest 91:734-736.
91. Longbottom, J. J., and J. Pepys. 1964. Pulmonary aspergillosis:diagnostic and immunological significance of antigens and C-
CLIN. MICROBIOL. REV.
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

SEROLOGY OF COCCIDIOIDOMYCOSIS 267
substances in Aspergillus fumigatus. Pathol. J. Bacteriol.88:141-151.
92. Lowe, E. P., J. L. Converse, G. P. Blundell, and M. W.Castleberry. 1959. Experimental respiratory infection withCoccidioides immitis, p. 14-15. In L. Wayne (ed.), Transac-tions of the 4th Annual Meeting, VA-Armed Forces Coopera-tive Study Group. Veterans Administration, Los Angeles,Calif.
93. Lowry, 0. H., N. J. Rosebrough, A. L. Farr, and R. J. Randall.1951. Protein measurement with the Folin phenol reagent. J.Biol. Chem. 193:265-275.
94. Meyer, P. R., A. N. Hui, and M. Biddle. 1982. Coccidioidesimmitis meningitis with arthroconidia in the cerebrospinalfluid: report of the first case and review of the arthroconidialiterature. Hum. Pathol. 13:1136-1138.
95. Miller, M. J., P. J. Sunshine, and J. Remington. 1969. Quanti-tation of cord serum IgM and IgA as a screening procedure todetect congenital infection-results in 5006 infants. J. Pediatr.75:1287-1291.
96. Muir, S., and D. Pappagianis. 1982. Coccidioidomycosis in thellama: a case report and epidemiologic survey. J. Am. Vet.Med. Assoc. 181:1334-1337.
97. Nimmich, W. 1979. Occurrence of 3-O-methylmannose inlipopolysaccharides of Klebsiella and Escherichia coli. Bio-chim. Biophys. Acta 215:189-191.
98. Palmer, D. F., L. Kaufman, W. Kaplan, and J. J. Cavallaro.1977. Serodiagnosis of mycotic diseases. Charles C Thomas,Publisher, Springfield, Ill.
99. Pappagianis, D. 1975. Opportunism in coccidioidomycosis, p.221-234. In E. Chick, A. Balows, and M. L. Furcolow (ed.),Opportunistic fungal infections. Charles C Thomas, Publisher,Springfield, Ill.
100. Pappagianis, D. 1980. Serology and serodiagnosis of coccidioi-domycosis, p. 97-112. In D. A. Stevens (ed.), Coccidioidomy-cosis. Plenum Publishing Corp., New York.
101. Pappagianis, D. 1988. Coccidioidomycosis, p. 600-623. In A.Balows, W. J. Hausler, Jr., and E. H. Lennette (ed.), Labo-ratory diagnosis of infectious diseases, principles and practice,vol. 1. Springer-Verlag, New York.
102. Pappagianis, D. 1988. Enhancement of host resistance bycontrol of fungal growth, p. 186-194. In G. G. Jackson, H. D.Schlumberger, and H. J. Zieler (ed.), Perspectives in antiinfec-tive therapy. Friedr. Vieweg and Sohn, Braunschweig/Wies-baden, Federal Republic of Germany.
103. Pappagianis, D., and R. Crane. 1977. Survival in coccidioidalmeningitis since introduction of amphotericin B, p. 223-237. InL. Ajello (ed.), Coccidioidomycosis. Current clinical and diag-nostic status. Symposia Specialists, Miami.
104. Pappagianis, D., and H. E. Einstein. 1978. Tempest fromTehachapi takes toll or, coccidioides conveyed aloft and afar.West. J. Med. 129:527-530.
105. Pappagianis, D., and G. S. Kobayashi. 1958. Production ofextracellular polysaccharide in cultures of Coccidioides immi-tis. Mycologia 10:229-238.
106. Pappagianis, D., and G. S. Kobayashi. 1960. Approaches to thephysiology of Coccidioides immitis. Ann. N.Y. Acad. Sci.89:109-121.
107. Pappagianis, D., I. Krasnow, and S. Beall. 1976. False-positivereactions of cerebrospinal fluid and diluted sera with thecoccidioidal latex agglutination test. Am. J. Clin. Pathol.66:916-921.
108. Pappagianis, D., S. Lindsay, S. Beall, and P. Williams. 1979.Ethnic background and the clinical course of coccidioidomy-cosis. Am. Rev. Respir. Dis. 120:959-961.
109. Pappagianis, D., N. J. Lindsey, C. E. Smith, and M. T. Saito.1965. Antibodies in human coccidioidomycosis: immunoelec-trophoretic properties. Proc. Soc. Exp. Biol. Med. 118:118-122.
110. Pappagianis, D., R. L. Miller, C. E. Smith, and G. S. Koba-yashi. 1960. Response of monkeys to respiratory challengefollowing subcutaneous inoculation with Coccidioides immitis.Am. Rev. Respir. Dis. 82:244-250.
111. Pappagianis, D., E. W. Putman, and G. S. Kobayashi. 1961.
Polysaccharide of Coccidioides immitis. J. Bacteriol. 82:714-723.
112. Pappagianis, D., M. T. Saito, and K. VanHoosear. 1972.Antibody in the cerebrospinal fluid in non-meningitic coccidi-oidomycosis. Sabouraudia 10:173-179.
113. Pappagianis, D., C. E. Smith, and C. C. Campbell. 1967.Serologic status after positive coccidioidin skin reactions. Am.J. Respir. Dis. 96:520-523.
114. Pappagianis, D., C. E. Smith, G. S. Kobayashi, and M. T. Saito.1961. Studies of antigens from young mycelia of Coccidioidesimmitis. J. Infect. Dis. 108:35-44.
115. Pappagianis, D., C. E. Smith, M. T. Saito, and G. S. Kobayashi.1957. Preparation and property of a complement-fixing antigenfrom mycelia of Coccidioides immitis. Public Health Serv.Publ. 575:57-63.
116. Pepys, J., and J. L. Longbottom. 1971. Antigenic and C-substance activities of related glycopeptides from fungal, par-asitic and vegetable sources. Int. Arch. Allergy 41:219-221.
117. Petersen, E. A., B. A. Friedman, E. D. Crowder, and D.Rifkind. 1976. Coccidioidouria: clinical significance. Ann. In-tern. Med. 85:34-38.
118. Phaff, H. J., M. W. Miller, and E. M. Mrak. 1978. The life ofyeasts, 2nd ed. Harvard University, Cambridge, Mass.
119. Porter, J. F., E. R. Scheer, and R. W. Wheat. 1971. Charac-terization of 3-O-methylmannose from Coccidioides immitis.Infect. Immun. 4:660-661.
120. Ray, J. G., Jr. 1967. The agar-gel precipitin-inhibition test usedin serum titration of human and animal coccidioidomycosis, p.215-220. In L. Ajello (ed.), Coccidioidomycosis. University ofArizona Press, Tucson.
121. Reed, R. E. 1956. Diagnosis of disseminated canine coccidioi-domycosis. J. Am. Vet. Med. Assoc. 128:196-201.
122. Reed, R. E., E. J. Bicknell, and H. B. Hood. 1985. A thirty-yearrecord of coccidioidomycosis in exotic pets and zoo animals inArizona, p. 275-281. In H. E. Einstein and A. Catanzaro (ed.),Proceedings of the Fourth International Conference on Coc-cidioidomycosis. National Foundation for Infectious Disease,Washington, D.C.
123. Resnick, S., D. Pappagianis, and J. H. McKerrow. 1987.Proteinase production by the parasitic cycle of the pathogenicfungus Coccidioides immitis. Infect. Immun. 55:2807-2815.
124. Rowe, J. R., V. D. Newcomer, and J. W. Landau. 1963. Effectsof cultural conditions on the development of antigens byCoccidioides immitis. J. Invest. Dermatol. 41:343-350.
125. Rowe, J. R., V. D. Newcomer, and E. T. Wright. 1963. Studieson the soluble antigens of Coccidioides immitis by immunodif-fusion. J. Invest. Dermatol. 41:225-233.
126. Rowland, V. S., R. E. Westfali, W. A. Hinchcliffe, and P. B.Jarretl. 1977. Acute respiratory failure in miliary coccidioido-mycosis, p. 139-155. In L. Ajello (ed.), Coccidioidomycosis.Current clinical and diagnostic status. Symposia Specialists,Miami.
127. Salvin, S. B., M. L. Furcolow, and J. Nishio. 1954. Serologicstudies on an outbreak of pulmonary disease at Camp Gruber,Oklahoma. Arch. Intern. Med. 93:906-910.
128. Sawaki, Y., M. Huppert, J. W. Bailey, and Y. Yagi. 1966.Patterns of human antibody reactions in coccidioidomycosis.J. Bacteriol. 91:422-427.
129. Scalarone, G. M., H. B. Levine, S. D. Chaparas, and J. M.Cobb. 1973. Properties and assay of spherulins from Coccid-ioides immitis in delayed sensitivity responses of animals.Sabouraudia 11:222-234.
130. Scalarone, G. M., H. B. Levine, D. Pappagianis, and S. D.Chaparas. 1974. Spherulin as a complement-fixing antigen inhuman coccidioidomycosis. Am. Rev. Respir. Dis. 110:324-328.
131. Scheer, E., T. Terai, S. Kulkarni, N. F. Conant, R. Wheat, andE. P. Lowe. 1970. An unusual reducing sugar from Coccidi-oides immitis. J. Bacteriol. 103:525-526.
132. Schubert, J. H., and C. R. Hampson. 1962. An appraisal ofserologic tests for coccidioidomycosis. Am. J. Hyg. 76:144-148.
133. Shifrine, M., D. Pappagianis, and J. Neves. 1975. Double
VOL. 3, 1990
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

268 PAPPAGIANIS AND ZIMMER
electroimmunodiffusion: a rapid diagnostic test for caninecoccidioidomycosis. Am. J. Vet. Res. 36:819-820.
134. Sinski, J. T., E. P. Lowe, M. W. Castleberry, L. F. Maire, J. E.DelFavero, S. P. Pakes, and J. L. Converse. 1963. Comparisonof serologic reactions in experimental canine and simian coc-cidioidomycosis. Sabouraudia 3:106-113.
135. Smith, C. E. 1955. Coccidioidomycosis. Pediatr. Clin. N. Am.2:109-125.
136. Smith, C. E. 1958. Coccidioidomycosis, p. 285-316. In J. B.Coates (ed.), Preventive medicine in World War II, vol. 4.Communicable diseases. Office of the Surgeon General, Med-ical Dept., U.S. Army, Washington, D.C.
137. Smith, C. E. 1967. Reminiscences of the flying chlamydosporeand its allies, p. xiii-xxii. In L. Ajello (ed.), Coccidioidomy-cosis. University of Arizona Press, Tucson.
138. Smith, C. E., and C. C. Campbell. 1957. Question and answerperiod on serology of coccidioidomycosis. Proceedings of theSymposium on Coccidioidomycosis. Public Health Serv. Publ.575:53-56.
139. Smith, C. E., M. T. Saito, R. R. Beard, R. M. Kepp, R. W.Clark, and B. U. Eddie. 1950. Serological tests in the diagnosisand prognosis of coccidioidomycosis. Am. J. Hyg. 52:1-20.
140. Smith, C. E., M. T. Saito, C. C. Campbell, G. B. Hill, S.Saslaw, S. B. Salvin, J. E. Fenton, and M. A. Krupp. 1957.Comparison of complement fixation tests for coccidioidomy-cosis. Public Health Rep. 72:888-894.
141. Smith, C. E., M. T. Saito, and S. A. Simons. 1956. Pattern of39,500 serologic tests in coccidioidomycosis. J. Am. Med.Assoc. 160:546-552.
142. Smith, C. E., E. G. Whiting, E. E. Baker, H. G. Rosenberger,R. R. Beard, and M. T. Saito. 1948. The use of coccidioidin.Am. Rev. Tuberc. 57:330-360.
143. Standard, P. G., and L. Kaufman. 1977. Immunological proce-dure for the rapid and specific identification of Coccidioidesimmitis. J. Clin. Microbiol. 5:149-153.
144. Stewart, R. A., and F. Kimura. 1940. Studies in the skin test forcoccidioidal infection. 1. Preparation and standardization ofcoccidioidin. J. Infect. Dis. 66:212-217.
145. Taylor, R. L. 1967. Serological response of Rhesus monkeys toHistoplasma, Blastomyces and Coccidioides antigens. J. Bac-teriol. 94:1-5.
146. Teel, K. W., M. D. Yow, and T. W. Williams, Jr. 1970. Alocalized outbreak of coccidioidomycosis in southern Texas. J.Pediatr. 17:65-73.
147. Wack, E. E., K. 0. Dugger, and J. N. Galgiani. 1988. Enzyme-linked immunosorbent assay for antigens of Coccidioides im-mitis: human sera interference corrected by acidification-heat
extraction. J. Lab. Clin. Med. 111:560-565.148. Weiner, M. H. 1983. Antigenemia detected in human coccidi-
oidomycosis. J. Clin. Microbiol. 18:136-142.149. Weisman, I. M., A. J. Moreno, A. L. Parker, W. C. Sippo, and
W. J. Liles. 1986. Gastrointestinal dissemination in coccidioi-domycosis. Am. J. Gastroenterol. 81:589-593.
150. Wheat, R. W., C. Tritschler, N. F. Conant, and E. P. Lowe.1977. Comparison of Coccidioides immitis arthrospore,mycelium, and spherule cell walls and influence of growthmedium on mycelial cell wall composition. Infect. Immun.17:91-97.
151. Wieden, M., J. N. Galgiani, and D. Pappagianis. 1983. Com-parison of immunodiffusion techniques with standard comple-ment fixation assay for quantitation of coccidioidal antibodies.J. Clin. Microbiol. 18:529-534.
152. Wolf, J. E., J. R. Little, D. Pappagianis, and G. S. Kobayashi.1986. Disseminated coccidioidomycosis in a patient with ac-quired immune deficiency syndrome. Microbiol. Infect. Dis.5:331-336.
153. Wood, J., G. Friendly, M. Zartarian, S. Arnaes, and L. M. deLa Maza. 1982. Alternative to the standardized laboratorybranch complement fixation test for detection of antibodies toCoccidioides immitis. J. Clin. Microbiol. 16:1030-1033.
154. Yoshinoya, S., R. Cox, and R. M. Pope. 1980. Circulatingimmune complexes in coccidioidomycosis. J. Clin. Invest.66:655-663.
155. Yturraspe, D. 1971. Clinical evaluation of latex particle agglu-tination test in the diagnosis of canine coccidioidomycosis. J.Am. Vet. Med. Assoc. 158:1249-1256.
156. Zimmer, B. L., K. Johnson, and D. Pappagianis. 1985. Char-acterization of soluble proteins released during the growth ofspherule-endospore phase Coccidioides immitis, p. 88-98. InH. E. Einstein and A. Catanzaro (ed.), Proceedings of theFourth International Conference on Coccidioidomycosis. Na-tional Foundation for Infectious Disease, Washington, D.C.
157. Zimmer, B. L., and D. Pappagianis. 1986. Comparison ofimmunoblot analyses of spherule-endospore-phase extracellu-lar protein and mycelial-phase antigen of Coccidioides immitis.Infect. Immun. 53:64-70.
158. Zimmer, B. L., and D. Pappagianis. 1988. Characterization of asoluble protein of Coccidioides immitis with activity as animmunodiffusion-complement fixation antigen. J. Clin. Micro-biol. 26:2250-2256.
159. Zimmer, B. L., and D. Pappagianis. 1989. Immunoaffinityisolation and partial characterization of the Coccidioides im-mitis antigen detected by the tube precipitin and immunodiffu-sion-tube precipitin tests. J. Clin. Microbiol. 27:1759-1766.
CLIN. MICROBIOL. REV.
on Septem
ber 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from