Embed Size (px)
Citation preview
1
Setting Water Quality Standards – A Global Perspective
John Fawell
Visiting Professor, Cranfield Institute of Water
2
Safe Water is Vital
• No safe drinking-water: almost 1 billion people lack access to an improved supply
• Diarrhoeal disease: 2 million annual deaths attributable to unsafe water, sanitation and hygiene
• Cholera: more than 50 countries still report cholera to WHO
• Millions exposed to unsafe levels of naturally-occurring arsenic and fluoride
• Emerging challenges: increasing use of wastewater in agriculture is important for livelihood opportunities, but also associated with serious public health risks including drinking water
3
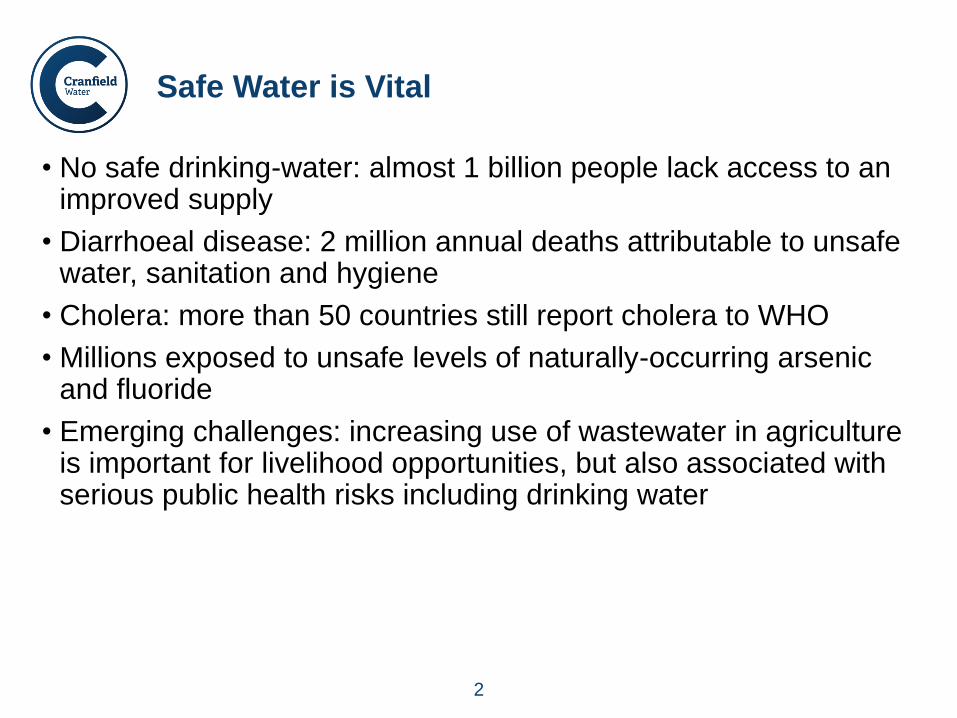
Not all Drinking Water Supplies are the Same
Water quality standards need to recognise this
4
WHO Guidelines – A benchmark for standards.
• WHO have been publishing Guidelines for Drinking Water Quality since 1984. Before that we had WHO European and International Standards.
• Recognition that they have no legal force but provide a scientific point of departure for the development of national water quality standards.
• The Guidelines have evolved over time with increasing numbers of chemical parameters.
• The primary source of guidance.
5
Major Change in the Third Edition
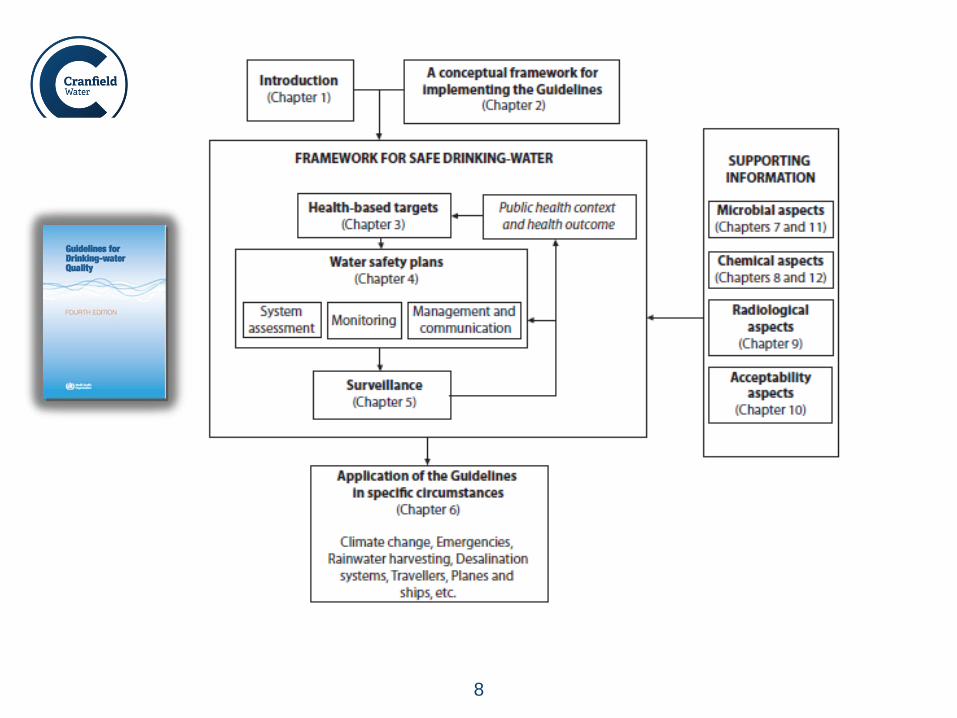
• Introduced a framework for safe water encouraging countries to put water quality in the context of overall health priorities.
• Underpinned by the concept of drinking water safety plans.
• Proactive prevention of problems throughout the supply chain. Managing systems, large or small to ensure safe water. Change from concentrating on end of pipe standards – too little, too late.
• The other elements, such as guideline values provide support.
• Re-emphasised the need to adapt the guidelines to meet local circumstances. That means taking into account practicality and affordability.
• It also means developing national standards that include relevant parameters rather than slavishly copying all the guidelines into standards.
6
How do the Guidelines deal with variation
• Huge variation in types of source from large well-run municipal supplies to small resource poor rural sources that may supply just a few people.
• Emphasises do what you can and aim for continuous improvement.
• Provides guidance on priorities for those with few resources.
• Not just about measuring standards at the end of pipe
• Drinking-water can be delivered by large municipal supplies, often with significant resources, particularly in developed countries who tend to also provide the experts for developing the Guidelines..
• There are also many small rural community supplies that are often poorly resourced and very basic.
• This means that the capability to monitor or screen for contaminants is in general variable, and for small supplies it usually varies from very limited to none.
7
WHO Guidelines for Drinking-water Quality
Aim Protection of human health
–Support setting of national standards and regulations
Target Audience Regulators + (water suppliers, practitioners . . .)
Approach Best available evidence - science and practice
Risk-benefit philosophy (advisory in nature)
Local adaptation considering overall health protection
strategies
– Social, cultural, economic and environmental context
Preventive incorporating multiple barriers
Incremental improvement
Evidence-based
8
9
Waterborne Microbial Pathogens
• Remain the top priority. We can count the bodies!
• The problem is that reliable measurement of actual pathogens is difficult and in most cases prohibitively expensive.
• We still use indicators of faecal contamination for surveillance (E.coliand faecal streptococci) but on their own they are not enough. (Not total coliforms).
• Hence the preventive strategy of Water Safety Plans - identifying the possible threats and putting in procedures (barriers) to deal with them. Must also ensure that the barriers are working efficiently all of the time (operational monitoring).
• This approach can be applied to any water supply, however small and however primitive.
• For more sophisticated (and wealthy) supplies then quantitative microbial risk assessment can be used to determine the necessary level of treatment, for others there is a need for identifying the hazards and to put in barriers to reduce the risks.
10
Chemical contaminants
• Differ from pathogens which are essentially acute and a very low dose can cause infection in susceptible individuals.
• Almost exclusively unlikely to cause any adverse effects except following long-term exposure.
• Only a small number have been shown to actually cause adverse effects through drinking water – arsenic, fluoride, nitrate, lead. Possibly chlorination by-products, manganese.
• Significant margins of safety or negligible risk used in developing guideline values.
• Important considerations:
Small differences in standards can make a huge practical/cost difference while delivering little or no benefit to health.
Monitoring/surveillance is costly and often difficult, need routine and available methods.
• Resources and common sense dictate that only the most important chemicals are considered – occurrence and toxicity.

11
WHO Guidelines for Chemicals - development
• Consideration is given of need, does it occur at significant concentrations in drinking water in a reasonable number of countries or is there a reasonable chance of it being present. (Chicken and egg?)
• A background document is prepared usually from a peer reviewed international review, e.g. JECFA, JMPR, or if that is not available an internationally recognised and peer reviewed national document, e.g. Health Canada. Last resort is a de novo review – takes time.
• Proposals reviewed by Guidelines expert committee by e-mail and discussed at meeting of the committee. Document and approach agreed. Finalised and re-reviewed by expert committee members.
• External peer review by experts. Document and guideline revised as necessary.
• “Public” consultation and revision if necessary. Finalised by expert committee.
• Published as a guideline.
12
Development of Health-based Values
• Use suitable animal studies or possibly suitable epidemiological studies.
• Tolerable or Acceptable daily intake (TDI/ADI) determined by applying uncertainty factors to reflect extrapolation from high to low doses, animals to man, gaps in the database.
• Allocation of a proportion of the TDI/ADI to drinking water to allow for exposure from other sources such as food. WHO default is 20%.
• Guideline value is usually based on 60 kg adult drinking 2 litres of water per day. Under some circumstances may use child or infant if they are the vulnerable sub-population. (10kg and 1 litre, 5 kg and 0.75 litre).
• For carcinogens that are considered to operate through a genotoxicmechanism use a linearised mathematical model to extrapolate from high to low doses. Level of risk that is used by WHO is 1 additional cancer per 100,000 population exposed for 70 years – essentially negligible. Models are conservative and do not include a number of mitigating biological factors. Some chemicals actually show non-linearity.
13
Development of Guideline Values
• In developing the GV take into account the practical considerations such as treatment and control and analytical methods.
• May be designated provisional which is important.
For some the GV is set at a level above the health-based value taking into account practical considerations – e.g. lead.
May also be designated provisional if major uncertainties regarding the toxicological data – e.g. chromium, arsenic.
• In setting standards and interpreting what an exceedence means it is important to understand what the standard is based on and how much room for manoeuvre there is. Do not want damaging and unnecessary decisions on what to do and do not want to unnecessarily undermine consumer confidence in the supply.
• Guideline values are not hard and fast values below which the water is safe and above which it isn’t.
14
Chemical contaminants – the role of standards
• National Standards are needed to provide a benchmark for water quality.
Protect public health (without excessive cost)
Public reassurance (compliance)
Implement policy (pesticides)
Benchmark for operations management, acceptability (turbidity, aluminium, iron, PAH, THMs)
• They may provide a target for the future reflecting the need for progressive improvement, e.g. lead in Europe.
• They also need to be revised at intervals to reflect new knowledge on exposure, newly recognised contaminants and new scientific knowledge.
• There is no point in including many chemicals in standards and then doing no monitoring/surveillance. Equally no point in measuring lots of zeros so targeted and risk-based monitoring are important.

15
Influences on Standards – Behind the Numbers
• Quasi-scientific considerations (uncertainty factors, exposure, acceptable risk.)
• Socio-political climate (public and politician chemophobia)
• Practicalities and costs (point of control, diffuse or point source), historical or current contaminant.

16
Developing a Risk-Based Monitoring Programme.
• What are the hazards from the catchment (source water), treatment and distribution?
• What is the likelihood of each parameter (hazard) reaching consumers at concentrations of concern/close to the standards – risk assessment?
• What data are available to show current concentrations over time and trends? (Existing monitoring data.)
• Flexibility to allow supply by supply modification of surveillance.
17
Assessing Monitoring Needs
• Is a substance present?
• If so is it present at say < 50% of the standard/guideline?
•Does the concentration change or is it stable?
Stable over time not just a couple of samples.
• Is there operational monitoring, e.g. Al?
•Can it be controlled by product specification, e.g. acrylamide.
•Might start at higher frequency then adjust.
18
European Union Standards
• Seeking harmonisation across member states but the number of member states has increased significantly. Standards in the current Directive are based on the second edition of the Guidelines and we are now on the fourth edition.
• Standards and guidelines continue changing and developing in the light of new knowledge and changes in policy and achievability but need some stability where long-term investment.
• We have a list of parameters in Annex I but also a clause that covers anything else that might be a threat to health.
• Significant responsibilities lie with water suppliers.
• Requirement for review and revision recognised and process initiated.
• Already introduced the concept of Water Safety Plans and risk-based monitoring in the revision of Annex II

19
Final Remarks
• Standards are important for drinking water and the WHO Guidelines provide the point of departure/basis for standards in a significant proportion of countries around the world.
• Encouraging countries to establish standards and surveillance is an important step in meeting the challenges of waterborne disease.
• Wealthy countries can’t afford to be complacent – things can go horribly wrong – Walkerton, Flint.
• We need to think of drinking water as part of the managed water cycle. Wastewater is a significant source of pathogens and emerging contaminants. Re-use of wastewater is increasingly important for helping to meet pressure on water resources.
• We need more interdisciplinary/sector collaboration to make the most of our knowledge and to meet new challenges, not just identifying problems but providing cost-effective solutions for a wide range of circumstances.
20
The Guidelines Work Continues
•First addendum to the Fourth edition later this year
•Fifth edition planned for 2020