Embed Size (px)
Citation preview
Severity of Aortic Atheromatous Disease Diagnosed by Transesophageal Echocardiography Predicts Stroke and Other Outcomes Associated with Coronary Artery Surgery: A Prospective Study Gregg S. Hartman, MD, Fun-Sun F. Yao, MD, Mathias Bruefach III, MD, Denise Barbut, MD,
Janey C. Peterson, MA, RN, Mary Helen Purcell, BA, RN, Mary E. Charlson, MD, Jeffrey P. Gold, MD, Stephen J. Thomas, MD, and Ted P. Szatrowski, MD
Departments of Anesthesiology, Neurology, Medicine, and Cardiothoracic Surgery, the CCABOT Group,’ The New York Hospital, Cornell University Medical College, New York, New York
Advanced atheromatous disease of the thoracic aorta the 189 patients with TEE examinations had periop- identified by transesophageal echocardiography (TEE) erative strokes by 1 wk. At 1 wk, no strokes had oc- is a major risk factor for perioperative stroke. This study curred in the 123 patients with atheroma Grades I or investigated whether varying degrees of atherosclero- II, while the I-wk stroke rate was 5.5% (2/36), 10.5% sis of the descending aorta, as assessed by TEE, are an (2/19), and 45.5% (5/11) for Grades III, IV, and V, independent predictor of cardiac and neurologic out- respectively (Fisher’s exact test, P = 0.00001). For come in patients undergoing coronary artery bypass 6-mo outcome, advancing aortic atheroma grade was grafting (CABG). Intraoperative TEE of the descending a univariate predictor of stroke (P = 0.00001) and aorta was performed on 189 of 248 patients participat- death (P = 0.03). By 6 mo there were one additional ing in a randomized controlled trial of low (50-60 mm stroke, three additional deaths, and one additional Hg) or high (So-100 mm Hg) mean arterial pressure major cardiac event. Atheromatous disease of the de- during cardiopulmonary bypass for elective CABG. scending aorta was a strong predictor of stroke and Aortic atheromatous disease was graded from I to V in death after CABG. TEE determination of atheroma order of increasing severity by observers blinded to grade is a critical element in the management of pa- outcome. Measured outcomes were death, stroke, and tients undergoing CABG surgery. major cardiac events assessed at 1 wk and 6 mo. Nine of (Anesth Analg 1996;83:701-8)
C oronary artery bypass grafting (CABG) pro- longs life for patients with severe triple vessel or left main coronary artery disease (1,2). Stroke,
however, remains one of the most devastating com- plications after this procedure (3). Overall postopera- tive cardiac morbidity has been declining over the past
Supported in part by the National Heart, Lung, and Blood Insti- tute, National Institutes of Health Grant HL44719.
Accepted for publication June 17, 1996. Address correspondence to Gregg S. Hartman, MD, Department
of Anesthesiology, A-1018, The New York Hospital-Cornell Medical Center, 525 E. 68th St., New York, NY 10021.
i The CCABOT (Cornell Coronary Artery Bypass Outcomes Trial) Group consists of the following: Mary E. Charlson, MD, and Jeffrey P. Gold, MD (principal investigators), Denise Barbut, MD, Mathias Bruefach III, MD, Larry Gorkin, PhD, Gregg S. Hartman, MD, James P. Hollenberg, MD, Joseph G. Hayes, MD, 0. Wayne Isom, MD, Karl H. Kreiger, MD, Steven Mattis, PhD, Janey C. Peterson, MA, RN, Paul A. Pirraglia, BD, Martin Post, MD, Mary Helen Purcell, BA, RN, Pamela Williams-Russo, MD, Ted P. Szatrowski, MD, Stephen J. Thomas, MD, and Fun-Sun F. Yao, MD.
years, in part because of advances in anesthetic and surgical techniques. However, the incidence of neuro- logic complications has been largely unchanged, with stroke occurring in 1% to 5% of patients (4-6). Risk factors for perioperative stroke include increased age (4), previous cerebrovascular accidents, carotid steno- sis (51, atria1 fibrillation, patent foramen ovale and other intracardiac shunts (7), the presence of intracar- diac thrombus, valvular disease, and atheromatous disease of the ascending thoracic aorta and aortic arch (6,s). Transesophageal echocardiography (TEE) was superior to chest radiograph and cardiac catheteriza- tion in detecting aortic atheromatous disease and ath- eroma correlated with the occurrence of stroke (9). Previous studies have demonstrated the significance of ascending aorta and aortic arch atheromata in pre- dicting stroke after cardiopulmonary bypass (CPB) (9,lO). In elderly patients, risk of perioperative stroke
01996 by the International Anesthesia Research Society 0003-2999/96/$5.00 Anesth Analg 1996;83:701-8 701

702 CARDIOVASCULAR ANESTHESIA HARTMAN ET AL. TEE PREDICTS STROKE ASSOCIATED WITH CABG
ANESTH ANALG 1996;83:701-8
was significantly increased when atheromata had mo- bile components (9). However, these studies did not prospectively evaluate neurologic outcome by observ- ers blinded to intraoperative TEE results, or control for confounding variables.
The goal of this study was to determine whether atheromatous disease of the descending thoracic aorta, as diagnosed by TEE, is independently predic- tive of stroke and other morbidity or mortality in patients undergoing elective CABG. We also at- tempted to identify clinical predictors of atheroma grade. The study was performed in the context of a prospective, randomized, controlled trial which evalu- ated the effect of blood pressure management during CPB on cardiac and neurologic outcome (11). Patients were observed prospectively, evaluated preoperatively and postoperatively by blinded observers, and assessed for mortality, and cardiac and neurologic outcome at one week and six months after surgery (11).
Methods Patient Eligibility and Baseline Aleurologic Evaluation
Between October 1991 and February 1994,248 patients undergoing elective multivessel CABG were enrolled in a study examining the influence of mean arterial pressure (MAP) during CPB on cardiac and neuro- logic morbidity and quality of life after CABG (11). Exclusion criteria included inability to complete neu- rologic testing, participation in other studies, and in- ability to return for follow-up evaluation. Preopera- tively, all patients underwent detailed cardiologic and neurologic examinations by a study cardiologist and neurologist blinded to blood pressure randomization. Detailed demographic, cardiac, and neurologic char- acteristics were compiled. Symptom duration was the time from the onset of angina1 symptoms to the time of surgery. The Charlson comorbidity score, a meas- ure of comorbid illness, with a higher score represent- ing a greater burden of comorbidity (121, was also calculated for each patient. Institutional review board approval and informed, written consent were obtained.
TEE Examination
TEE evaluation of the descending thoracic aorta was performed intraoperatively after anesthetic induction and intubation on a cohort of 189 patients from the 248patient study group, based on availability of TEE equipment, the ability to insert the TEE probe, and the absence of contraindications to TEE, (e.g., esophageal disease). All examinations were performed with either monoplane or biplane 5 MHz TEE probes (Acuson, Mountain View, CA) and Acuson 128 Xl’@ systems (Acuson) and recorded on VHS tapes for later off-line
interpretation. Aortic pathology was graded off-line, based on transverse images of the descending thoracic aorta just distal to the arch and complemented by longitudinal images when obtainable. Aortic grade was determined by the consensus evaluation of two anesthesiologists experienced in TEE, blinded to intra- operative blood pressure management, using an in- creasing scale from I to V, according to the following criteria (10): Grade I, normal to mild intimal thicken- ing; Grade II, severe intimal thickening without pro- truding atheroma; Grade III, atheroma protruding less than 5 mm; Grade IV, atheroma protruding greater than or equal to 5 mm; Grade V, atheroma of any size with mobile components. The reproducibility of this scale has been demonstrated (13).
Intraoperative Course and Management
In the parent study, patients were randomly assigned on arrival to the operating room to one of two MAP strategies during CPB: low (50-60 mm Hg) or high (80-100 mm Hg) MAP group. Subsequent analysis of the data from the parent study demonstrated that patients were balanced with respect to demographics and perioperative management except for MAP dur- ing CPB (11). All hemodynamic variables were down- loaded every 10 s from a Marquette 7000@ monitor (Marquette, Milwaukee, WI) to a laptop computer. All operative events, pharmacological agents, and CPB variables were recorded on-line by a research assistant using a locally developed program that was synchro- nized with Marquette downloading. Anesthesia was induced with thiopental (l-2 mg/kg) and fentanyl (25 pg/kg). Pancuronium provided muscle relaxation. Anesthesia was maintained with a combination of the following: fentanyl boluses (l-5 pg/kg, to a total of 50-70 pg/kg), midazolam boluses (1 mg) and/or isoflurane (pre- and post-CPB periods only).
Perfusion techniques used during CPB were identi- cal for both groups and are detailed elsewhere (11). Nonpulsatile CPB, membrane oxygenation, 40-p blood filter, systemic cooling to 30-32”C, and a-stat pH management were common features of perfusion. A centrifugal or a roller pump was used, based on availability. Flow rates were predetermined at 1.6 and 2.4 L * min-’ . mP2 during cooling and warming, re- spectively. Pump flow was constant except for tran- sient alterations to facilitate surgical exposure. Target MAP on CPB for the intervention group MAP was 80-100 mm Hg and for the control group 50-60 mm Hg. If the MAP increased above target level, unre- sponsive to additional anesthetics (fentanyl and mida- zolam), sodium nitroprusside was administered; if MAP remained below target range, norepinephrine or metaraminol was infused. The surgeons were blinded to the descending aortic atheroma grade, as the clas- sification was performed later, off-line.
ANESTH ANALG CARDIOVASCULAR ANESTHESIA HARTMAN ET AL. 703 1996;83:701-8 TEE PREDICTS STROKE ASSOCIATED WITH CABG
There were no differences in technical aspects of the CABG procedure between the high and low pressure groups; operative mortality, aortic cross-clamp time, duration of CPB, and number of grafts did not differ (11).
Follow-up and Outcome Definition
The study cardiologist evaluated patients on postop- erative Days 1 or 2, and 7, and the neurologist evalu- ated patients preoperatively, and on postoperative Days 2 and 7. Both were blinded to the intraoperative management and the TEE atheroma grades. Standard- ized blinded examinations were also performed at 6 mo postoperatively.
Stroke was defined as a fixed, focal neurologic def- icit (12). Death was any which occurred within 6 mo after surgery. Major cardiac events included myocar- dial infarction, pulmonary edema, adult respiratory distress syndrome, low flow state/cardiogenic shock, or cardiopulmonary arrest (11).
Statistical Analysis
In order to ascertain whether selection bias might have occurred, the characteristics of the 189 patients who had TEE examinations performed and those of the 59 patients who did not have TEE performed were com- pared using large-sample 2 or t-testing as appropriate to the distribution of these variables.
For the main analysis, the relationship between the principal outcomes and atheroma grade was analyzed in a univariate fashion using standard 2 testing for a 2 x 5 contingency table, and Fisher’s exact test when more than 50% of cells had expected counts that were less than 5. A 2 test for linear trend of proportions was used to test the quantitative association between atheroma grade and outcome.
Clinical variables of interest listed in Table 2 were assessed for their value as predictors of outcome and atheroma grade using similar methods. To determine whether atheroma grade remained an independent predictor of outcomes, variables identified as predic- tive of outcome in the univariate analysis were incor- porated into standard multivariate logistic regression analysis (14).
Statistical analyses were done using SAS software for PC, version 6.08 (SAS Institute, Cary, NC) and all P values were two-sided.
Results Baseline Characteristics of Patients Evaluated by TEE
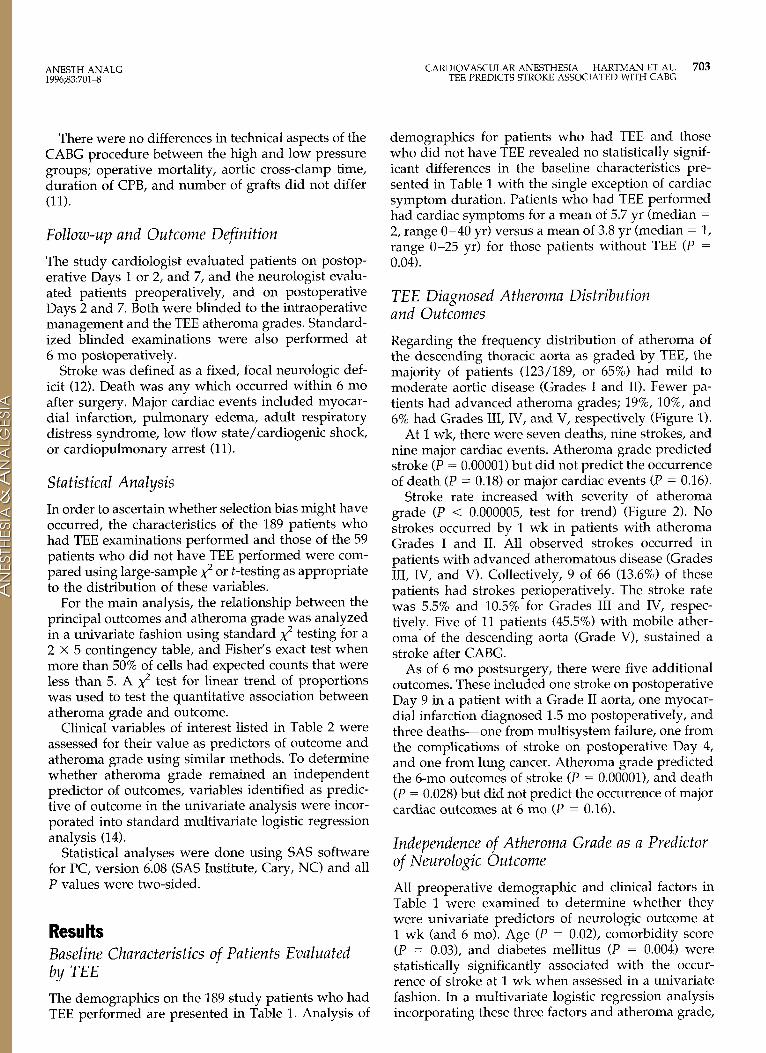
The demographics on the 189 study patients who had TEE performed are presented in Table 1. Analysis of
demographics for patients who had TEE and those who did not have TEE revealed no statistically signif- icant differences in the baseline characteristics pre- sented in Table 1 with the single exception of cardiac symptom duration. Patients who had TEE performed had cardiac symptoms for a mean of 5.7 yr (median = 2, range O-40 yr) versus a mean of 3.8 yr (median = 1, range O-25 yr) for those patients without TEE (P = 0.04).
TEE Diagnosed Atheroma Distribution and Outcomes
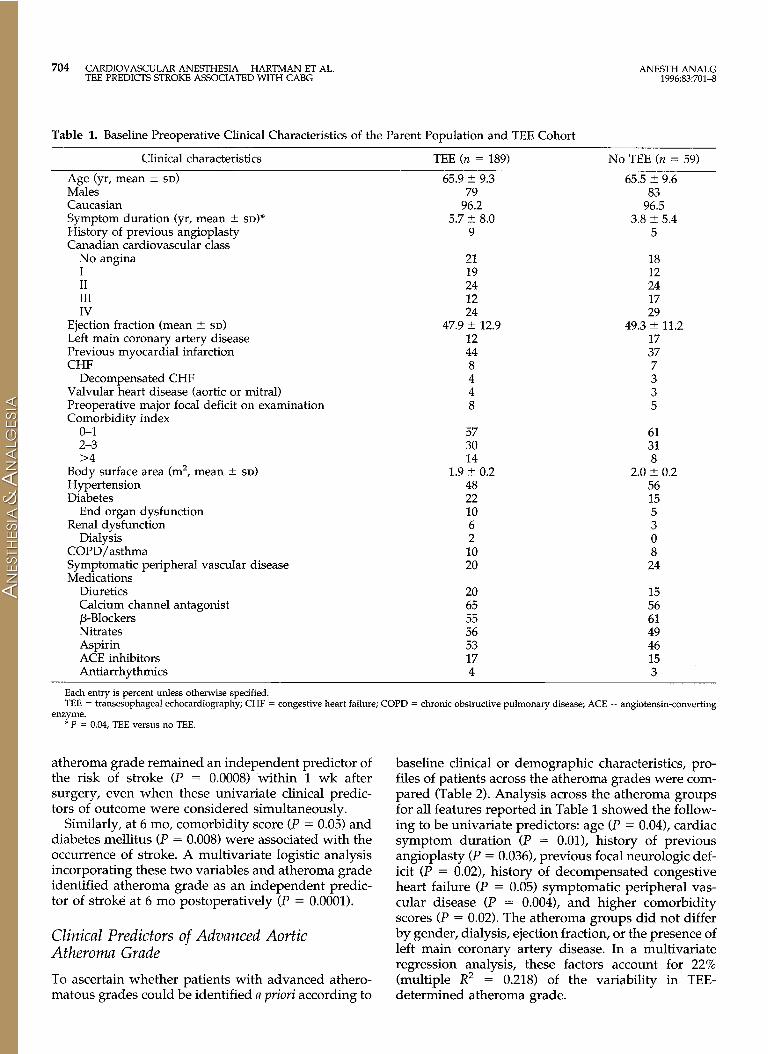
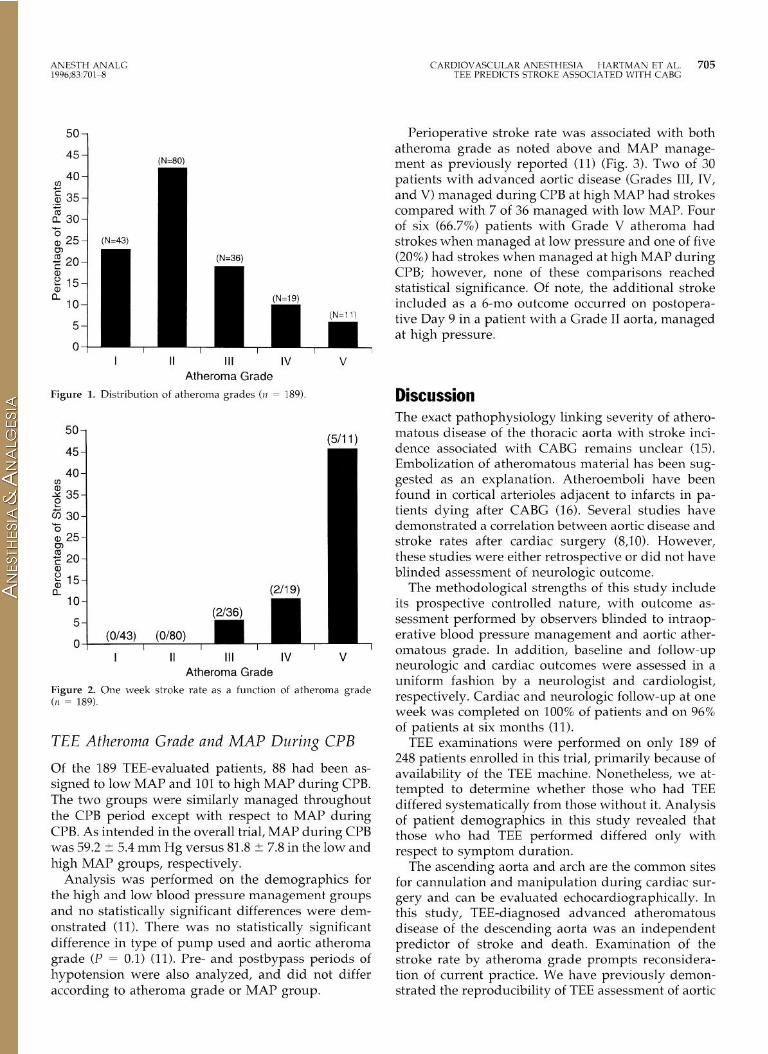
Regarding the frequency distribution of atheroma of the descending thoracic aorta as graded by TEE, the majority of patients (123/189, or 65%) had mild to moderate aortic disease (Grades I and II). Fewer pa- tients had advanced atheroma grades; 19%, lo%, and 6% had Grades III, IV, and V, respectively (Figure 1).
At 1 wk, there were seven deaths, nine strokes, and nine major cardiac events. Atheroma grade predicted stroke (P = 0.00001) but did not predict the occurrence of death (P = 0.18) or major cardiac events (P = 0.16).
Stroke rate increased with severity of atheroma grade (P < 0.000005, test for trend) (Figure 2). No strokes occurred by 1 wk in patients with atheroma Grades I and II. All observed strokes occurred in patients with advanced atheromatous disease (Grades III, IV, and V). Collectively, 9 of 66 (13.6%) of these patients had strokes perioperatively. The stroke rate was 5.5% and 10.5% for Grades III and IV, respec- tively. Five of 11 patients (45.5%) with mobile ather- oma of the descending aorta (Grade V), sustained a stroke after CABG.
As of 6 mo postsurgery, there were five additional outcomes. These included one stroke on postoperative Day 9 in a patient with a Grade II aorta, one myocar- dial infarction diagnosed 1.5 mo postoperatively, and three deaths-one from multisystem failure, one from the complications of stroke on postoperative Day 4, and one from lung cancer. Atheroma grade predicted the 6-mo outcomes of stroke (P = O.OOOOl), and death (P = 0.028) but did not predict the occurrence of major cardiac outcomes at 6 mo (P = 0.16).
Independence of Atheroma Grade as a Predictor of Neurologic Outcome
All preoperative demographic and clinical factors in Table 1 were examined to determine whether they were univariate predictors of neurologic outcome at 1 wk (and 6 mo). Age (P = 0.02), comorbidity score (P = 0.03), and diabetes mellitus (P = 0.004) were statistically significantly associated with the occur- rence of stroke at 1 wk when assessed in a univariate fashion. In a multivariate logistic regression analysis incorporating these three factors and atheroma grade,
704 CARDIOVASCULAR ANESTHESIA HARTMAN ET AL. ANESTH ANALG TEE PREDICTS STROKE ASSOCIATED WITH CABG 1996;83:701-8
Table 1. Baseline Preoperative Clinical Characteristics of the Parent Population and TEE Cohort
Clinical characteristics
Age (yr, mean + SD)
Males Caucasian Symptom duration (yr, mean + SD)*
History of previous angioplasty Canadian cardiovascular class
No angina I II III IV
Ejection fraction (mean 2 SD) Left main coronary artery disease Previous myocardial infarction CHF
Decompensated CHF Valvular heart disease (aortic or mitral) Preoperative major focal deficit on examination Comorbidity index
o-1 2-3 >4
Body surface area (m’, mean ? SD) Hypertension Diabetes
End organ dysfunction Renal dysfunction
Dialysis COPD/asthma Symptomatic peripheral vascular disease Medications
Diuretics Calcium channel antagonist P-Blockers Nitrates Aspirin ACE inhibitors Antiarrhythmics
TEE (n = 189) No TEE (n = 59)
65.9 ? 9.3 65.5 +- 9.6 79 83
96.2 96.5 5.7 -+ 8.0 3.8 2 5.4
9 5
21 18 19 12 24 24 12 17 24 29
47.9 ? 12.9 49.3 ? 11.2 12 17 44 37 8 7 4 3 4 3 8 5
57 61 30 31 14 8
1.9 t- 0.2 2.0 + 0.2 48 56 22 15 10 5 6 3 2 0 10 8 20 24
20 15 65 56 55 61 56 49 53 46 17 15 4 3
Each entry is percent unless otherwise specified. TEE = tramesophageal echocardiography; CHF = congestive heart failure; COl’D = chronic obstructive pulmonary disease; ACE = angiotensin-converting
enzyme. * P = 0.04, TEE versus no TEE.
atheroma grade remained an independent predictor of the risk of stroke (P = 0.0008) within 1 wk after surgery, even when these univariate clinical predic- tors of outcome were considered simultaneously.
Similarly, at 6 mo, comorbidity score (P = 0.05) and diabetes mellitus (P = 0.008) were associated with the occurrence of stroke. A multivariate logistic analysis incorporating these two variables and atheroma grade identified atheroma grade as an independent predic- tor of stroke at 6 mo postoperatively (P = 0.0001).
Clinical Predictors of Advanced Aortic Atheroma Grade
To ascertain whether patients with advanced athero- matous grades could be identified a priori according to
baseline clinical or demographic characteristics, pro- files of patients across the atheroma grades were com- pared (Table 2). Analysis across the atheroma groups for all features reported in Table 1 showed the follow- ing to be univariate predictors: age (P = 0.04), cardiac symptom duration (P = O.Ol), history of previous angioplasty (P = 0.036), previous focal neurologic def- icit (P = 0.02), history of decompensated congestive heart failure (P = 0.05) symptomatic peripheral vas- cular disease (P = 0.004), and higher comorbidity scores (P = 0.02). The atheroma groups did not differ by gender, dialysis, ejection fraction, or the presence of left main coronary artery disease. In a multivariate regression analysis, these factors account for 22% (multiple R2 = 0.218) of the variability in TEE- determined atheroma grade.
ANESTH ANALG 1996,83 701-S
50
45
40 cn .$i 35
2 30 1
(N-+30)
-5 a, 25- (N=43)
ii? E 20- (N=36)
E z15-
a io- (N=19)
(N=ll) 5-
I II III IV v Atheroma Grade
Figure 1. Distribution of atheroma grades (n = 189)
I II III IV V Atheroma Grade
Figure 2. One week stroke rate as a function of atheroma grade (n = 189).
TEE Atheroma Grade and MAP During CPB
Of the 189 TEE-evaluated patients, 88 had been as- signed to low MAP and 101 to high MAP during CPB. The two groups were similarly managed throughout the CPB period except with respect to MAP during CPB. As intended in the overall trial, MAP during CPB was 59.2 2 5.4 mm Hg versus 81.8 2 7.8 in the low and high MAP groups, respectively.
Analysis was performed on the demographics for the high and low blood pressure management groups and no statistically significant differences were dem- onstrated (11). There was no statistically significant difference in type of pump used and aortic atheroma grade (P = 0.1) (11). R-e- and postbypass periods of hypotension were also analyzed, and did not differ according to atheroma grade or MAP group.
CARDIOVASCULAR ANESTHESIA HARTMAN ET AL. 705 TEE PREDICTS STROKE ASSOCIATED WITH CABG
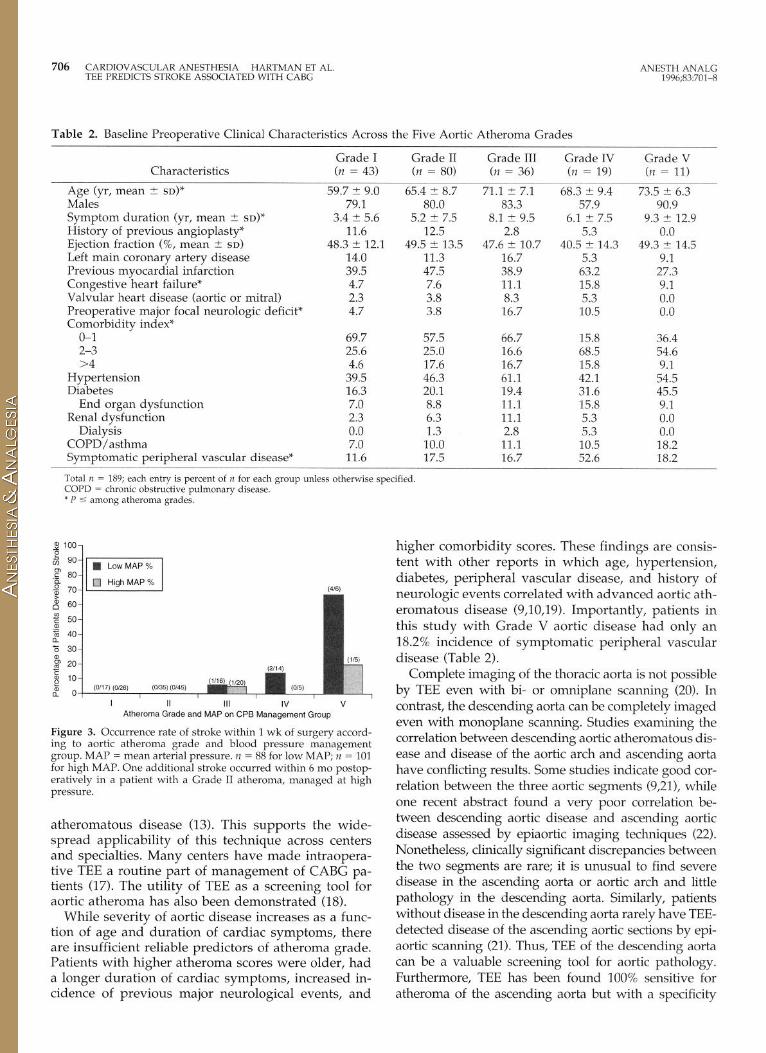
Perioperative stroke rate was associated with both atheroma grade as noted above and MAP manage- ment as previously reported (11) (Fig. 3). Two of 30 patients with advanced aortic disease (Grades III, IV, and V) managed during CPB at high MAP had strokes compared with 7 of 36 managed with low MAP. Four of six (66.7%) patients with Grade V atheroma had strokes when managed at low pressure and one of five (20%) had strokes when managed at high MAP during CPB; however, none of these comparisons reached statistical significance. Of note, the additional stroke included as a 6-mo outcome occurred on postopera- tive Day 9 in a patient with a Grade II aorta, managed at high pressure.
Discussion The exact pathophysiology linking severity of athero- matous disease of the thoracic aorta with stroke inci- dence associated with CABG remains unclear (15). Embolization of atheromatous material has been sug- gested as an explanation. Atheroemboli have been found in cortical arterioles adjacent to infarcts in pa- tients dying after CABG (16). Several studies have demonstrated a correlation between aortic disease and stroke rates after cardiac surgery (8,101. However, these studies were either retrospective or did not have blinded assessment of neurologic outcome.
The methodological strengths of this study include its prospective controlled nature, with outcome as- sessment performed by observers blinded to intraop- erative blood pressure management and aortic ather- omatous grade. In addition, baseline and follow-up neurologic and cardiac outcomes were assessed in a uniform fashion by a neurologist and cardiologist, respectively. Cardiac and neurologic follow-up at one week was completed on 100% of patients and on 96% of patients at six months (11).
TEE examinations were performed on only 189 of 248 patients enrolled in this trial, primarily because of availability of the TEE machine. Nonetheless, we at- tempted to determine whether those who had TEE differed systematically from those without it. Analysis of patient demographics in this study revealed that those who had TEE performed differed only with respect to symptom duration.
The ascending aorta and arch are the common sites for cannulation and manipulation during cardiac sur- gery and can be evaluated echocardiographically. In this study, TEE-diagnosed advanced atheromatous disease of the descending aorta was an independent predictor of stroke and death. Examination of the stroke rate by atheroma grade prompts reconsidera- tion of current practice. We have previously demon- strated the reproducibility of TEE assessment of aortic
706 CARDIOVASCULAR ANESTHESIA HARTMAN ET AL. ANESTH ANALG TEE PREDICTS STROKE ASSOCIATED WITH CABG 1996.83.701-8
Table 2. Baseline Preoperative Clinical Characteristics Across the Five Aortic Atheroma Grades
Characteristics
Age (yr, mean I SD)” Males Symptom duration (yr, mean -C SD)* History of previous angioplasty” Ejection fraction (%, mean ? SD)
Left main coronary artery disease Previous myocardial infarction Congestive heart failure* Valvular heart disease (aortic or mitral) Preoperative major focal neurologic deficit* Comorbidity index*
o-1 2-3 >4
Hypertension Diabetes
End organ dysfunction Renal dysfunction
Dialysis COPD/asthma Symptomatic peripheral vascular disease*
Grade I (n = 43)
Grade II (n = 80)
Grade III (n = 36)
Grade IV (n = 19)
Grade V (n = 11)
59.7 t 9.0 65.4 -c 8.7 71.1 -c 7.1 68.3 t 9.4 73.5 -c 6.3 79.1 80.0 83.3 57.9 90.9
3.4 t 5.6 5.2 -c 7.5 8.1 t 9.5 6.1 I? 7.5 9.3 1. 12.9 11.6 12.5 2.8 5.3 0.0
48.3 k 12.1 49.5 t 13.5 47.6 t 10.7 40.5 t- 14.3 49.3 t 14.5 14.0 11.3 16.7 5.3 9.1 39.5 47.5 38.9 63.2 27.3 4.7 7.6 11.1 15.8 9.1 2.3 3.8 8.3 5.3 0.0 4.7 3.8 16.7 10.5 0.0
69.7 57.5 66.7 15.8 36.4 25.6 25.0 16.6 68.5 54.6 4.6 17.6 16.7 15.8 9.1
39.5 46.3 61.1 42.1 54.5 16.3 20.1 19.4 31.6 45.5 7.0 8.8 11.1 15.8 9.1 2.3 6.3 11.1 5.3 0.0 0.0 1.3 2.8 5.3 0.0 7.0 10.0 11.1 10.5 18.2
11.6 17.5 16.7 52.6 18.2
Total n = 189; each entry is percent of n for each group unless otherwise specified COPD = chronic obstructive pulmonary disease * P c among atheroma grades.
I II III IV V Atheroma Grade and MAP on CPB Management Group
Figure 3. Occurrence rate of stroke within 1 wk of surgery accord- ing to aortic atheroma grade and blood pressure management group. MAP = mean arterial pressure. n = 88 for low MAP; n = 101 for high MAP. One additional stroke occurred within 6 mo postop- eratively in a patient with a Grade II atheroma, managed at high pressure.
atheromatous disease (13). This supports the wide- spread applicability of this technique across centers and specialties. Many centers have made intraopera- tive TEE a routine part of management of CABG pa- tients (17). The utility of TEE as a screening tool for aortic atheroma has also been demonstrated (18).
While severity of aortic disease increases as a func- tion of age and duration of cardiac symptoms, there are insufficient reliable predictors of atheroma grade. Patients with higher atheroma scores were older, had a longer duration of cardiac symptoms, increased in- cidence of previous major neurological events, and
higher comorbidity scores. These findings are consis- tent with other reports in which age, hypertension, diabetes, peripheral vascular disease, and history of neurologic events correlated with advanced aortic ath- eromatous disease (9,10,19). Importantly, patients in this study with Grade V aortic disease had only an 18.2% incidence of symptomatic peripheral vascular disease (Table 2).
Complete imaging of the thoracic aorta is not possible by TEE even with bi- or omniplane scanning (20). In contrast, the descending aorta can be completely imaged even with monoplane scanning. Studies examining the correlation between descending aortic atheromatous dis- ease and disease of the aortic arch and ascending aorta have conflicting results. Some studies indicate good cor- relation between the three aortic segments (9,211, while one recent abstract found a very poor correlation be- tween descending aortic disease and ascending aortic disease assessed by epiaortic imaging techniques (22). Nonetheless, clinically significant discrepancies between the two segments are rare; it is unusual to find severe disease in the ascending aorta or aortic arch and little pathology in the descending aorta. Similarly, patients without disease in the descending aorta rarely have TEE- detected disease of the ascending aortic sections by epi- aortic scanning (21). Thus, TEE of the descending aorta can be a valuable screening tool for aortic pathology. Furthermore, TEE has been found 100% sensitive for atheroma of the ascending aorta but with a specificity

ANESTH ANALG 1996;83:701-8
CARDIOVASCULAR ANESTHESIA HARTMAN ET AL. 707 TEE PREDICTS STROKE ASSOCIATED WITH CABG
rate of 60% (18), and significant plaque detected any- where in the thoracic aorta is a very sensitive screening tool for significant plaque in the ascending aorta (18). This may explain the poor correlation found by Guzzetta et al. (22).
Identification of patients with advanced atheroma- tous disease of the descending thoracic aorta should prompt detailed examination of the ascending aorta and aortic arch, preferably with epiaortic scanning (23). Detection of advanced disease in these segments in the vicinity of aortic cannulation and cross-clamp application levels warrants reconsideration of the risks of the proposed procedure. Previously, modifi- cations in anesthetic and surgical techniques to lessen stroke incidence have been attempted but not vali- dated. These modifications include alternate aortic cannulation sites and cannulae (9), “no touch,” single aortic cross-clamp techniques (24), circulatory arrest, and aortic atherectomy (10,251.
Our data suggest that patients with mobile ather- oma (Grade V) appear to represent a particularly vul- nerable subset for developing stroke after CABG. Re- examination of the risk-benefit ratios of surgery versus medical management of these patients is warranted. In addition, patients with severe aortic atheromatous disease who require CABG procedures may benefit from modifications in surgical techniques directed at reducing stroke risk. These technical modifications (e.g., circulatory arrest, aortic atherectomy), may in turn increase risk, but may prove to be the best option since conventional management itself carries such a high risk of stroke.
While many modifications in surgical technique have been proposed, performance of CPB at higher MAP may be an easily achievable alternative without significant drawbacks. The optimal range of MAP dur- ing CPB however, remains controversial. Proponents of low MAP during CPB stress a long history of safe practice (26). Hypothetically, high MAP during CPB may predispose to turbulence and embolization in the presence of aortic atheromatous disease. Other studies have also demonstrated the feasibility of increasing MAP while not adversely affecting patient outcome (27). While a concern of higher MAP particularly dur- ing the cross-clamp period is the potential for cardiac warming and wash out of cardioplegic solution be- cause of enhanced collateral flow, the previously re- ported study confirmed that higher MAP during CPB can be achieved without increased surgical or techni- cal difficulty, while diminishing cardiac and neuro- logic morbidity and mortality (11).
In this study, one of five patients with Grade 5 atheroma managed at high MAP developed stroke, while four of six similar patients managed at low MAP developed stroke. The data suggest the utility but do not prove the importance of managing patients with advanced aortic atheromatous disease at higher MAP
during CPB. Although based on a small number of patients, which precluded statistical significance, these findings support the need for additional study in larger populations to define whether higher MAP dur- ing CPB is beneficial to patients with advanced ather- omatous disease.
The importance of maintaining MAP within the nor- mal autoregulatory range on cardiac and renal out- comes has been demonstrated in studies of noncardiac surgery (28). Higher MAP (closer to the right-shifted autoregulatory range), while potentially more me- chanically traumatic, may improve cerebral perfusion and lessen the likelihood of hypoperfusion injury. Higher cerebral perfusion pressure may improve col- lateral blood flow to the territory of vessels occluded by emboli thus attenuating hypoperfusion injury. In addition, some degree of cerebral protection may be afforded by higher perfusion pressures, lessening im- pact on “watershed” areas. These pressures more closely approximate those wherein cerebral autoregu- lation is preserved. Importantly, no patients with Grade I or II aortic atheroma suffered an adverse outcome. This may reflect a protective effect of normal vasculature and a vulnerability of patients with dis- eased vasculature.
In conclusion, this study demonstrates that ather- oma grade of the descending aorta is a strong inde- pendent risk factor for stroke within one week of CABG surgery and for both stroke and death within six months postoperatively. While increased MAP during CPB has been shown to be generally beneficial for cardiac and neurologic outcome (111, in particular, we note that patients with advanced atheromatous disease of the aorta may benefit from increased per- fusion pressures. TEE determination of atheroma grade is a critical element in the management of pa- tients undergoing CABG surgery.
References 1.
2.
3.
4.
5.
6.
7.
CASS Principle Investigators and Their Associates. Myocardial infarction and mortality in the Coronary Artery Surgery Study (CASS) randomized trial. N Engl J Med 1984;310:750-8. European Coronary Surgery Study Group. Long-term results of prospective randomized study of coronary artery bypass sur- gery in stable angina pectoris. Lancet 1982;2:1173-180. Shaw PJ, Bates D, Cartlidge NEF, et al. Early neurological com- plications of coronary artery bypass surgery. BMJ 1985;291: 1384-7. Gardner TJ, Horneffer PJ, Manolio TA, et al. Stroke following coronary artery bypass grafting: a ten-year study. Ann Thorac Surg 1985;40:574-81. Reed GL, Singer DE, Pilard EH. Stroke following coronary artery bypass surgery: a case-control estimate of the risks of carotid bruits. N Engl J Med 1988;319:1246-50. Culliford AT, Colvin SB, Rohrer K, et al. The atherosclerotic ascending aorta and transverse arch: a new technique to prevent cerebral injury during bypass: experience with 13 patients. Ann Thorac Surg 1986;41:27-35. Alfieri A, Kotler M. Noncardiac complications of open-heart surgery. Am Heart J 1990;119:149-58.

708 CARDIOVASCULAR ANESTHESIA HARTMAN ET AL ANESTH ANALG TEE PREDICTS STROKE ASSOCIATED WITH CABG 1996;83:701-8
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
Wareing TH, Davila-Roman VG, Barzilai B, et al. Management of the severely atherosclerotic ascending aorta during cardiac operations: a strategy for detection and treatment. J Thorac Cardiovasc Surg 1992;103:453-62. Marshall K, Kanchuger M, Kessler K, et al. Superiority of trans- esophageal echocardiography in detecting aortic arch atheroma- tous disease: identification of patients at increased risk of stroke during cardiac surgery. J Cardiothorac Vast Anesth 1994;8:5-13. Katz ES, Tunick PA, Rusinek H, et al. Protruding aortic athero- mas predict stroke in elderly patients undergoing cardiopulmo- nary bypass: experience with intraoperative transesophageal echocardiography. J Am Co11 Cardiol 1992;20:70-7. Gold JP, Charlson ME, Williams-Russo P, et al. Improvement of outcomes after coronary artery bypass: a randomized trial com- paring intraoperative high vs low mean arterial pressure. J Tho- rat Cardiovasc Surg 1995;110:1302-14. Charlson M, Akels K, Pompei I’, MacKenzie C. A new method of classification of prognostic comorbidity for longitudinal studies: development and validation. 1 Chron Dis 1987;40:373-83. Hartm’an GS, Peterson J, Konstadt SN, et al. High reproducibil- ity in the interpretation of intraoperative transesophageal echo- cardiographic evaluation of aortic atheromatous disease. Anesth Analg 1996;82:539-43. SAS. SAS/STAT user’s guide, version 6, chapter 27, the logistic procedure. 1989;2:1071-126. Nussmeier NA. Neuropsychiatric complications of cardiac sur- gery. J Cardiothorac Vast Anesth 1994;8:13-8. Taylor K. Pathophysiology of brain damage during open heart surgery. Tex Heart Inst J 1986;13:91-6. Rafferty TD, Lippmann H. Intraoperative two-dimensional echocardiography and color-flow Doppler imaging: a basic transesophageal single plane patient examination. Yale J Biol Med 1994;66:349-83. Konstadt SN, Reich DL, Kahn R, Viggianti R. Transesophageal echocardiography can be used to screen for ascending aortic atherosclerosis. Anesth Analg 1995;81:225-8.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
Blanchard DG, Kimura BJ, Dittrich HC, DeMaria AN. Trans- esophageal echocardiography of the aorta. JAMA 1994;272: 546-51. Konstadt SN, Reich DL, Quintana C, Levy M. The ascending aorta: how much does transesophageal echocardiography see? Anesth Analg 1994;78:240-4. Hartman GS, Bruefach M, Yao FS, et al. Relationship between TEE assessed atheromatous disease of the descending aorta and stroke in CABG patients [abstract]. Anesthesiology 1994;81:A109. Guzzetta NA, Lee E, Sadel SM, et al. Does the degree of ather- omatous disease in the descending thoracic aorta correlate with atheromatous disease in the ascending aorta? [abstract]. Anesth Analg 1995;80(Suppl):SCA95. Kanchuger M, Marshall K, Tissot M, et al. Epiaortic ultrasonog- raphy is superior to biplane transesophageal echocardiography or surgical palpation in detecting ascending aortic atherosclero- sis [abstract]. Anesthesiology 1994;81:AllO. Savage E, Cohn L. “No touch” dissection, antegrade-retrograde blood cardioplegia, and single aortic cross-clamp significantly reduce operative mortality of reoperative CABG. Circulation 1994;90:140-3. Kouchoukos NT. Adjuncts to reduce the incidence of embolic brain injury during operations on the aortic arch. Ann Thorac Surg 1994;57:243-5. Slogoff S, Reul GJ, Keats AS. Role of perfusion pressure and flow in major organ dysfunction after cardiopulmonary bypass. Ann Thorac Surg 1990;50:911-8. Akins CW. Noncardioplegic myocardial preservation for coro- nary revascularization. J Thorac Cardiovasc Surg 1986;88: 174-81. Charlson ME, MacKenzie CR, Gold JP, et al. Pre-operative and intra-operative hemodynamic predictors of post-operative myo- cardial infarction or ischemia in patients undergoing non- cardiac surgery. Ann Surg 1989;210:637-48.