Embed Size (px)
DESCRIPTION
REFERENCE shwartz surgery prepared by dr.kucha
Citation preview

SHOCK
PREPARED BY DR.KUCHA

shock
• tissue hypoperfusion that is insufficient to maintain normal aerobic metabolism• consists of inadequate tissue perfusion marked by decreased delivery
of required metabolic substrates and inadequate removal of cellular waste products
• the resultant cellular injury is initially reversible; if the hypoperfusion is severe enough and prolonged, the cellular injury becomes irriversible
• the clinical manifestations are the result of:• stimulation of the sympathetic and neuro-endocrine stress responses• inadequate oxygen delivery• end-organ dysfunction

patho-physiology of shock
disruption host-microbial equilibrium trauma
neurologic injury
acute heart failurehemorrhage
tissue hypoperfusion
cellular hypoxia/ischemia
shock

neuro-endocrine response to hemorrhage • its goal is to maintain perfusion to the heart and brain , even at the expense of other organ systems• mechanisms include:• autonomic control of peripheral vascular tone and cardiac contractility• hormonal response to stress and volume depletion• local microcirculatory mechanisms that are organ specific and regulate regional blood flow
afferent signals• loss of circulating blood volume• pain, hypoxemia, hypercarbia, acidosis, infection, changes in temperature, emotional arousalm, hypoglycemia• baroreceptors
• within the atria of the heart which are sensitive to changes in chambert-pressure and wall stretch
• aortic arch and carotid bodies• chemoreceptors in the aorta and carotid bodies are sensitive to changes in O2 tension, H+ ion concentration, and carbon dioxide (CO2) levels
• stimulation of the chemoreceptors results in vasodilation of the coronary arteries, slowing of the heart rate, and vasoconstriction of the splanchnic and skeletal circulation
• a variety of protein and nonprotein mediators are produced at the site of injury as part of the inflammatory response, and they act as afferent impulses to induce a host response
cnsefferent signals• cardio-vascular response• hormonal response• circulatory homeostasis• microcirculatory respons

cardio-vascular response• hemorrhage results in diminished venous return to the heart and decreased cardiac output
• stimulation of sympathetic fibers innervating the heart leads to activation of beta1-adrenergic receptors that increase heart rate and contractility
• sympathetic stimulation of the peripheral circulation via the activation of alpha1-adrenergic receptors on arterioles induces vasoconstriction and causes a compensatory increase in systemic vascular resistance and blood pressure
• sympathetic stimulation also induces constriction of venous vessels, decreasing the capacitance of the circulatory system and accelerating blood return to the central circulation

hormonal response
• shock hypothalamus (CRH) pituitary gland (ACTH) adrenal cortex (cortisol)• cortisol stimulates gluconeogenesis and insulin resistance, resulting in hyperglycemia • cortisol stimulates muscle cell protein breakdown and lipolysis to provide substrates for
hepatic gluconeogenesis• cortisol causes retention of sodium and water by the nephrons of the kidneys
• renin-angiotensin system is activated in shock• decreased renal artery perfusion, beta-adrenergic stimulation, and increased renal
tubular sodium concentration cause the release of renin from the juxtaglomerular cells
• decreased renal artery perfusion• beta-adrenergic stimulation• increased renal tubular sodium concentration cause the release of renin from the juxtaglomerular cells
• angiotensin I has no significant functional activity• angiotensin II
• a potent vasoconstrictor of both splanchnic and peripheral vascular beds
• stimulates the secretion of aldosterone, ACTH, and antidiuretic hormone (ADH)
• aldosterone acts on the nephron to promote reabsorption of sodium water.
• potassium and hydrogen ions are lost in the urine in exchange for sodium.
• renin catalyzes the conversion of angiotensinogen (produced by the liver) to angiotensin I, which is then converted to angiotensin II by angiotensin-converting enzyme (ACE) produced in the lung
•release of renin from the juxtaglomerular cells

• ADH acts:
• on the distal tubule and collecting duct of the nephron to increase water permeability, decrease water and sodium losses, and preserve intravascular volume
• as a potent mesenteric vasoconstrictor, shunting circulating blood away from the splanchnic organs during hypovolemia
• this may contribute to intestinal ischemia and predispose to intestinal mucosal barrier dysfunction in shock states
• increases hepatic gluconeogenesis and increases hepatic glycolysis
• hypovolemia
• changes in circulating blood volume sensed by baroreceptors and left atrial stretch receptors
• increased plasma osmolality detected by hypothalamic osmoreceptors
• pituitary gland releases vasopressin or ADH
• epinephrine• angiotensin II• pain• hyperglycemia
increase the release of ADH

Microcirculation• the microvascular bed is innervated by the sympathetic nervous system and has a profound effect on the larger arterioles
• following hemorrhage larger arterioles vasoconstrict; small distal arterioles vasodilate
• other vasoactive proteins including:• vasopressin• angiotensin II• endothelin-1
• also lead to vasoconstriction to limit organ perfusion to organs such as skin, skeletal muscle, kidneys, and the GI tract to preserve perfusion of the myocardium and CNS
• flow in the capillary bed often is heterogeneous in shock states, which likely is secondary to multiple local mechanisms, including endothelial cell swelling, dysfunction, and activation marked by the recruitment of leukocytes
• decreased capillary hydrostatic pressure secondary to changes in blood flow and increased cellular uptake of fluid
• failure of the integrity of the endothelium of the microcirculation and development of capillary leak, intracellular swelling, and the development of an extracellular fluid deficit • intracellular swelling is multifactorial, but
dysfunction of energy-dependent mechanisms, such as active transport by the sodium-potassium pump contributes to loss of membrane integrity.

metabolic effects• cellular metabolism is based primarily on the hydrolysis of adenosine triphosphate (ATP)• majority of ATP is generated in our bodies through aerobic metabolism in the process of oxidative phosphorylation in the mitochondria
• dependent on the availability of O2 as a final electron acceptor in the electron transport chain
• O2 tension within a cell decreases, there is a decrease in oxidative phosphorylation, and the generation of ATP slows
• when oxidative phosphorylation is insufficient, the cells shift to anaerobic metabolism and glycolysis to generate ATP
• this occurs via the breakdown of cellular glycogen stores to pyruvate
• under hypoxic conditions in anaerobic metabolism, pyruvate is converted into lactate, leading to an intracellular metabolic acidosis
• depletion of ATP potentially influences all ATP-dependent cellular processes:
• maintenance of cellular membrane potential
• synthesis of enzymes and proteins
• cell signaling• DNA repair mechanisms
• decreased intracellular pH also influences vital cellular functions such as:• normal enzyme activity• cell membrane ion exchange• cellular metabolic signaling• acidosis leads to changes in calcium metabolism and calcium
signaling

immune and inflammatory responses
• a well regulated complex set of interactions between circulating soluble factors and cells that can arise in response to trauma, infection, ischemia, toxic, or autoimmune stimuli
• direct tissue injury or infection
• activation of the active inflammatory and immune responses by the release of bioactive peptides by neurons in response to pain and the release of intracellular molecules by broken cells, such as heat shock proteins, mitochondrial peptides, heparan sulfate, high mobility group box 1, and RNA
• intracellular products from damaged and injured cells can have paracrine and endocrine-like effects on distant tissues to activate the inflammatory and immune responses – DANGER SIGNALING HYPOTHESIS
• endogenous molecules (damage associated molecular patterns {DAMP}) are capable of signaling the presence of danger to surrounding cells and tissues
• DAMP:• Hyaluronan oligomers• Heparan sulfate• Extra domain A of
fibronectin• Heat shock proteins 60, 70, • Gp96 • Surfactant Protein A -
Defensin 2• Fibrinogen • Biglycan • High mobility group box 1 • Uric acid• Interleukin-1 S-100s
Nucleolin
• pattern recognition receptors (PRRs) - cell surface• Toll-like receptors (TLRs) • receptor for advanced glycation end products
• initiation of the repair process and the mobilization of antimicrobial defenses at the site of tissue disruption
• leads to intracellular signaling and release of cellular products including cytokines
• tissue-based macrophages or mast cells act as sentinel responders, releasing histamines, eicosanoids, tryptases, and cytokines

FORMS OF SHOCK

Hypovolemic/Hemorrhagic Shock
• most common cause of shock in the surgical or trauma patient is loss of circulating volume from hemorrhage
• acute blood loss
• decreased baroreceptor stimulation from stretch receptors in the large arteries
• decreased inhibition of vasoconstrictor centers in the brain stem, increased chemoreceptor stimulation of vasomotor centers, and diminished output from atrial stretch receptors
• induces sympathetic stimulation • epinephrine and norepinephrine release, activation of the renin-angiotensin cascade, and increased vasopressin release
• increase vasoconstriction and peripheral arterial resistance

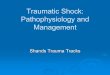
Class
Parameter I II III IV
Blood loss (mL) <750 750–1500 1500–2000 >2000
Blood loss (%) <15 15–30 30–40 >40
Heart rate (bpm) <100 >100 >120 >140
Blood pressure Normal Orthostatic Hypotension Severe hypotension
CNS symptoms Normal anxiousmild tachycardiatachypnea
confusedhypotension, marked tachycardia [i.e., pulse greater than 110 to 120 beats per minute (bpm)]
obtunded,immediately life threatening, and generally requires operative control of bleeding
Classification of Hemorrhage

• the appropriate priorities in patients with hemorrhagic shock are:• secure the airway• control the source of blood loss• IV volume resuscitation
• patients who fail to respond to initial resuscitative efforts should be assumed to have ongoing active hemorrhage from large vessels and require prompt operative intervention
• diagnostic and therapeutic laparotomy or thoracotomy
• patients who respond to initial resuscitative effort but then deteriorate hemodynamically frequently have injuries that require operative intervention
• patients who fail to respond to resuscitative efforts despite adequate control of ongoing hemorrhage• have ongoing fluid requirements despite adequate control of hemorrhage• have persistent hypotension despite restoration of intravascular volume necessitating vasopressor support• exhibit a futile cycle of uncorrectable hypothermia, hypoperfusion, acidosis, and coagulopathy that cannot be interrupted
despite maximum therapy
• these patients have deteriorated to decompensated or irreversible shock with peripheral vasodilation and resistance to vasopressor infusion
• mortality is inevitable once the patient manifests shock in its terminal stages
• transfusion of packed red blood cells and other blood products is essential in the treatment of patients in hemorrhagic shock• current recommendations in stable ICU patients aim for a target hemoglobin of 7 to 9 g/dL
• fresh frozen plasma (FFP) should also be transfused in patients with massive bleeding or bleeding with increases in prothrombin or activated partial thromboplastin times 1.5 times greater than control
• additional resuscitative adjuncts in patients with hemorrhagic shock include minimization of heat loss and maintaining normothermia
• development of hypothermia in the bleeding patient is associated with acidosis, hypotension, and coagulopathy• hypothermia in bleeding trauma patients is an independent risk factor for bleeding and death

Septic Shock (Vasodilatory Shock)
• vasodilatory shock is the result of dysfunction of the endothelium and vasculature secondary to circulating inflammatory mediators and cells or as a response to prolonged and severe hypoperfusion• hypotension results from failure of the vascular smooth muscle to constrict appropriately
• characterized by peripheral vasodilation with resultant hypotension and resistance to treatment with vasopressors
• the most frequently encountered form of vasodilatory shock is septic shock• other causes include:
• hypoxic lactic acidosis• carbon monoxide poisoning• decompensated and irreversible hemorrhagic shock• terminal cardiogenic shock• postcardiotomy shock
• vasodilatory shock seems to represent the final common pathway for profound and prolonged shock of any etiology
• in addition to fever, tachycardia, and tachypnea, signs of hypoperfusion such as confusion, malaise, oliguria, or hypotension may be present• these should prompt an aggressive search for infection, including a thorough physical examination,
inspection of all wounds, evaluation of intravascular catheters or other foreign bodies, obtaining appropriate cultures, and adjunctive imaging studies, as needed

• evaluation of the patient in septic shock begins with an assessment of the adequacy of their airway and ventilation• severely obtunded patients and patients whose work of breathing is excessive require intubation and
ventilation to prevent respiratory collapse
• vasodilation and decrease in total peripheral resistance may produce hypotension• fluid resuscitation and restoration of circulatory volume with balanced salt solutions is essential
• empiric antibiotics must be chosen carefully based on the most likely pathogens (gram-negative rods, gram-positive cocci, and anaerobes) because the portal of entry of the offending organism and its identity may not be evident until culture data return or imaging studies are completed• knowledge of the bacteriologic profile of infections in an individual unit can be obtained from most hospital
infection control departments and will suggest potential responsible organisms
• antibiotics should be tailored to cover the responsible organisms once culture data are available, and if appropriate, the spectrum of coverage narrowed
• after first-line therapy of the septic patient with antibiotics, IV fluids, and intubation if necessary, vasopressors may be necessary to treat patients with septic shock• catecholamines are the vasopressors used most often
• hyperglycemia and insulin resistance are typical in critically ill and septic patients, including patients without underlying diabetes mellitus















![SHOCK[1] - Hypovolemic Shock](https://img.pdfslide.net/doc/110x75/58edc1bc1a28abae538b4711/shock1-hypovolemic-shock.jpg)










