Embed Size (px)
Citation preview
Shock,Shock,Shock…EverybodyShock
AHA2015Scien8ficUpdate KellyCounts,ACNP-BC,FNP-C
WashingtonUniversityofSt.LouisEmergencyServices
Objec8ves
• Reviewscien8ficupdatesthatwillimpactcardiopulmonaryresuscita8onandemergencycardiovascularcare.
• Discusshowthechangeswillimpactourdailyprac8ce.
• Iden8fica8onofthenew2015AHAguidelinesforopioidoverdose
Backintheday…….
• TheACLSguidelineswerefirstpublishedin1974“squad51”
• 1980,1986,1992• 2000ChainofSurvivalandAED• 200530:2&StrokeGuidelines• 2010CAB• 2015………
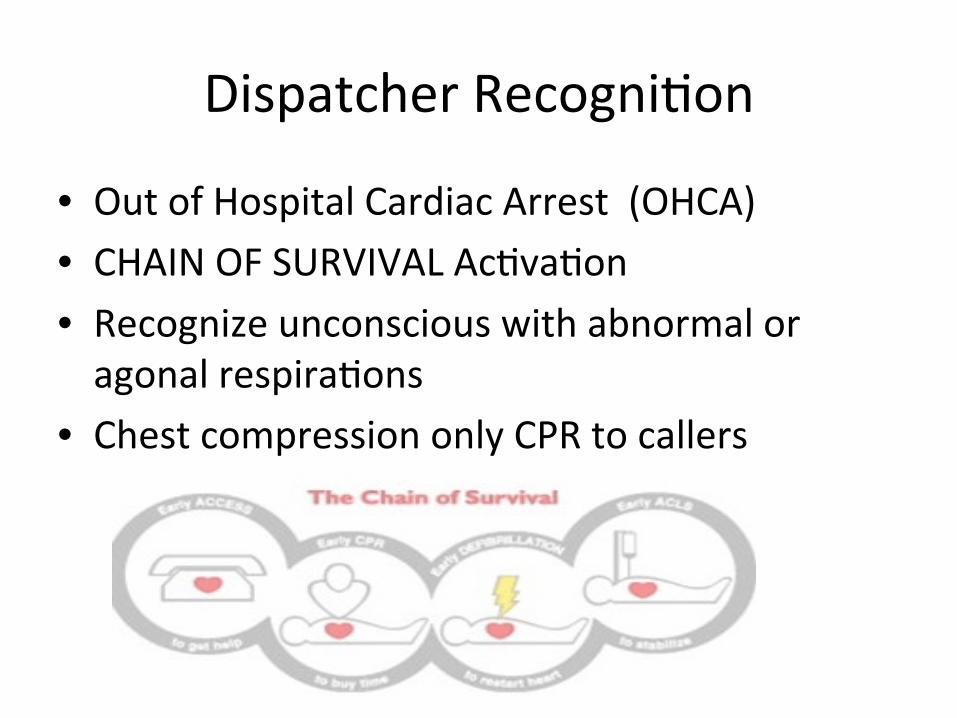
DispatcherRecogni8on
• OutofHospitalCardiacArrest(OHCA)• CHAINOFSURVIVALAc8va8on• Recognizeunconsciouswithabnormaloragonalrespira8ons
• ChestcompressiononlyCPRtocallers

Compressions
• 2010…EarlyCPR100compressions/minute
• 2015…..100-120compressions/minute
• 2010Depthofcompressionofatleast2”
• 2015Depthofcompressionofatleast2”,whileavoidingexcessivedepths>2.4”
AncillaryDevicesforCPR
• ImpedenceThresholdDevices-àOUT• Thumpers….Bands….NotRecommended

V
OpioidOverdose
• CABbeforeNarcan• Ifvic8mrespondstoNarcan…s8lltransport…• Empiricadministra8onofNarcanIMorIN
Yes
© 2015 American Heart Association
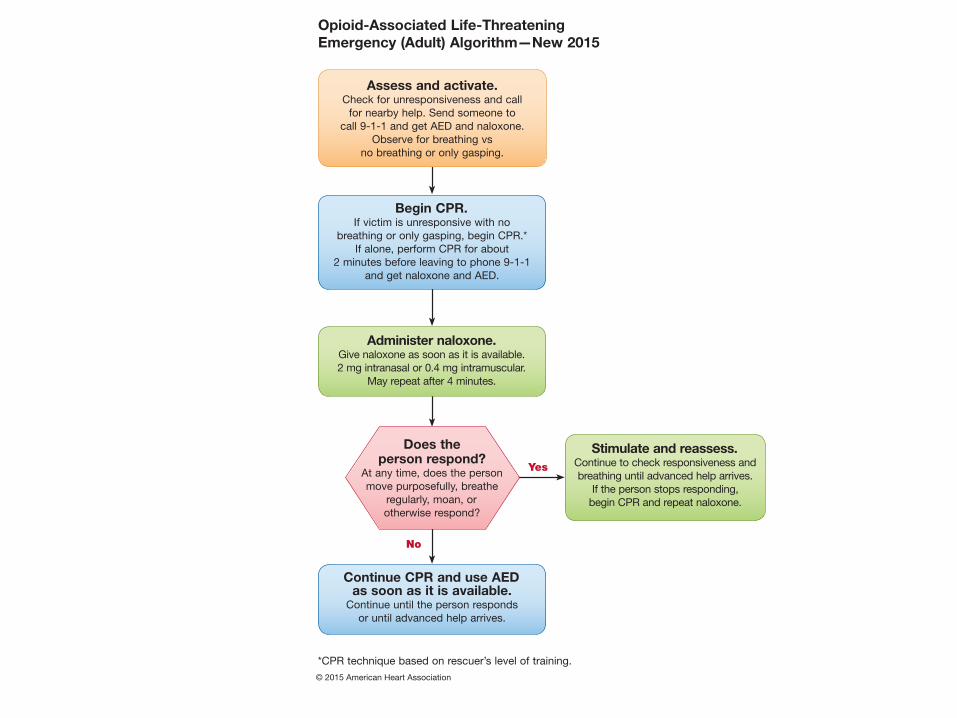
Opioid-Associated Life-Threatening Emergency (Adult) Algorithm—New 2015
Stimulate and reassess.Continue to check responsiveness and breathing until advanced help arrives.
If the person stops responding, begin CPR and repeat naloxone.
Begin CPR.If victim is unresponsive with no
breathing or only gasping, begin CPR.*If alone, perform CPR for about
2 minutes before leaving to phone 9-1-1 and get naloxone and AED.
Assess and activate.Check for unresponsiveness and call
for nearby help. Send someone to call 9-1-1 and get AED and naloxone.
Observe for breathing vs no breathing or only gasping.
Does the person respond?
At any time, does the person move purposefully, breathe
regularly, moan, or otherwise respond?
No
Administer naloxone.Give naloxone as soon as it is available.2 mg intranasal or 0.4 mg intramuscular.
May repeat after 4 minutes.
Continue CPR and use AEDas soon as it is available.
Continue until the person responds or until advanced help arrives.
*CPR technique based on rescuer’s level of training.
AcuteCoronarySyndrome
• Pre-hospital12leadECGshouldbeacquiredearlyforpa8entswithpossibleACS
• Computergeneratedinterpreta8on…..Goodorbad?
• MONA….”O”• Reperfusion…<120minutes
Pediatrics
• RATE—sameasadults• Toomuchfluidmaybebad• Premedica8ngwithatropinepriortointuba8on
• AmiodaroneORlidocaineacceptableforVF/VT
2015(Updated):Priori8esforthepregnantwomanincardiacarrestareprovisionofhigh-qualityCPRandreliefofaortocavalcompression.Ifthefundusheightisatorabovetheleveloftheumbilicus,manuallemuterinedisplacementcanbebeneficialinrelievingaortocavalcompressionduringchestcompressions.2010(Old):Torelieveaortocavalcompressionduringchestcompressionsandop8mizethequalityofCPR,itisreasonabletoperformmanuallemuterinedisplacementinthesupineposi8onfirst.Ifthistechniqueisunsuccessful,andanappropriatewedgeisreadilyavailable,thenprovidersmayconsiderplacingthepa8entinalemlateral8ltof27°to30°,usingafirmwedgetosupportthepelvisandthorax.Why:Recogni8onofthecri8calimportanceofhigh-qualityCPRandtheincompa8bilityofthelateral8ltwithhigh-qualityCPRhaspromptedtheelimina8onoftherecommenda8onforusingthelateral8ltandthestrengtheningoftherecommenda8onforlateraluterinedisplacement.
CardiacArrestinPregnancy:ProvisionofCPR
Summary
• hops://eccguidelines.heart.org/index.php/circula8on/cpr-ecc-guidelines-2/
• NEWWeb-BasedIntegratedGuidelines• Con8nuouslyupdatedinsteadofevery5years• Renewalmaybemorefrequentthanevery2years
• Faster……Deeper……SAVESLIVES
References
• hop://www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC1485990/
• hop://circ.ahajournals.org/content/102/suppl_1/I-1.full
• hop://www.aafp.org/afp/2006/0501/p1644.html
• hops://eccguidelines.heart.org/index.php/circula8on/cpr-ecc-guidelines-2/





















![₪[martin gardner] aha aha insight](https://img.pdfslide.net/doc/110x75/568cad201a28ab186daa6515/martin-gardner-aha-aha-insight.jpg)






