-
8/7/2019 Shock for the Internist
1/20
Indian Journal of Medicine 2011;1:4-23
Review article
Shock for the Internist
George John*, J V Peter, Kishore Pichamuthu, Binila Chacko
Medical Intensive Care Unit, Christian Medical College Hospital,
Vellore, India
*corresponding author email: [email protected]
Published online on 17th Feb 2011
Copyright 2011 George John. This is an open-access article . The
publisher and author permit unrestricted use, distribution, and
reproduction in any medium, provided the original work is
properly cited.
Abstract
The traditional approach to the correction of the
pathophysiology of shock was cardio-centric. In view of the
suboptimal clinical outcomes when clinical management was based
on the classical model, there was animpetus to change. This review
gives a new paradigm for understanding and managing shock.
Keywords: shock, sepsis, haemodynamics, critical care, organ
dysfunction
Indian J Med 2011;1:4-23
Definition:1
Shock is an acute, systemic clinical syndrome due to ineffective
tissue perfusion resulting in severe
dysfunction of organs vital for survival. The manifestations of
shock are:
1. arterial hypotension
2. altered temperature and colour of skin / mucous membranes;
prolonged capillary refill time
3. organ dysfunction
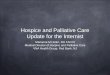
Classical paradigm:2,3
Traditional haemodynamic evaluation is cardiocentric. The
classical approach to understanding
cardiovascular physiology was to visualize the cardiovascular
system as being similar to an electrical
circuit (Figure 1). The heart (cardiac output) was considered as
the as the organ to be controlled
using preload and vascular resistance as the parameters to be
manipulated. Starlings Law of the
heart was used to explain the relationship between preload and
cardiac output. Inotropes wereconsidered if there was no response
to a change in preload (volume challenge).
On the basis of the above paradigm, the causes of shock (based
on deranged physiology) can be due
to 4 basic causes presenting as 3 haemodynamic patterns (Table
1).
4
-
8/7/2019 Shock for the Internist
2/20
Indian Journal of Medicine 2011;1:4-23
Figure 1: The Electrical Analogy
Table 1: Basic types of shock
Cause Pathophysiology* Patterns of abnormalities
Filling status Cardiac function Systemic resistance
Hypovolemic Loss of volume low low high
Vasogenic Vasodilation low high low
Cardiogenic Pump failure high low high
Obstructive Obstruction to flow Variable** low high
*primary problem mentioned in BOLD ; **depending on site of
obstruction
Cadiogenic (pump failure) and obstructive (massive pulmonary
embolism) causes have similar
clinical patterns but differing pathophysiology. Therapy based
on the above paradigm consisted of
measuring upstream pressures (preload), optimizing it using
fluid and then using inotropes if the
cardiac output was still suboptimal. In the traditional
perspective, the central venous pressure (or
the Left Atrial pressure or its surrogate, the pulmonary artery
occlusion pressure) was considered asa measure of preload which in
turn regulated cardiac output. However it is obvious that
Starlings
Law applied to cardiac myofiber length. The corresponding in
vivo surrogate for this was end
diastolic volume which was determined by the transmural pressure
and not the intramural pressure
measured by the CVP. Hence, in the next era, measures of end
diastolic volume were considered as
appropriate measures to control cardiac output. Subsequently the
concept of volume
responsiveness was introduced.
5
-
8/7/2019 Shock for the Internist
3/20
Indian Journal of Medicine 2011;1:4-23
THE NEW PARADIGM: 3,4,5,6
The new paradigm uses several concepts regarding cardiovascular
physiology which were already
known but not utilized because of the prevalent fashion to use
pressure measurements to
optimize haemodynamics. It was only when several studies showed
that traditional sophisticated
pressure measurements and their derived variables did not
improve clinical outcome in patients 7
that attention was refocused on a new perspective.
In the new paradigm, dynamic movement is not considered the same
as control. In a car, the moving
parts of the engine are impressive but it is the driver who
controls the car. The primary goal of the
cardiovascular system is to ensure tissue perfusion in order to
deliver adequate oxygen and
nutrients. The core function of the heart is to transfer blood
from a low energy system to a high
energy system. Therefore the final control of the system is with
the tissues which need perfusion.
The heart responds to the need by altering output as
required.
1. STRESSED AND UNSTRESSED VOLUMES:6
The major component (70%) of blood in the cardiovascular system
does not stretch the walls of the
vessels but merely fills the space. This is the unstressed
volume and does not contribute to vascular
pressure (except for the gravitational component). The remaining
30% of the blood volume stretches
the walls producing a measurable change in pressure the mean
circulatory filling pressure (MCFP).
This is known as the stressed volume. This is analogous to a
pneumatic tyre where the initial volume
of air does not increase pressure but does so only after the
tube is inflated to a certain volume
(Figure 2).
Figure 2: Volume vs Pressure
2. DISTRIBUTION OF BLOOD VOLUME:
The blood volume is distributed as follows in various vascular
compartments (Figure 3).
6
-
8/7/2019 Shock for the Internist
4/20
Indian Journal of Medicine 2011;1:4-23
Figure 3: Blood volume distribution
3. MEAN CIRCULATORY FILLING PRESSURE (MCFP):3,4,5,8
The MCFP is the mean pressure value for the entire circulation
when the heart stops beating. It is
the hydrostatic mean pressure of the circulation the pressure in
the circulation with no cardiac
activity. When there is no effective cardiac contraction, the
arteries recoil and about 4 ml/kg of
blood moves from the arterial side to the venous side (due to
elastic recoil) and an overall pressure
of 7 (+2) mm Hg is achieved. This value is less than the
capillary pressure but more than the venous
pressure. The pressure in the small veins (< 1mm diameter) is
the pivot locus as it does not
change. Conceptually, the MCFP (also known as Pmc) is the
resultant of two components the mean
systemic filling pressure (MSFP, Pms) and the mean pulmonary
filling pressure (MPFP, Pmp). The
difference in Pmc and Pms is accounted for by variation in Pmp.
The capacitance of the pulmonary
circulation is < 1/8 of the systemic but the blood volume in
the pulmonary circulation is only 1/10 of
systemic volume. Hence the Pmc and Pms are numerically almost
equal under normal conditions as
the mean pulmonary filling pressure does not significantly
contribute to the resultant pressure. It is
now possible to obtain a surrogate (analogue) of the Pms (known
as the Pmsa) in real time with
input from the circulatory variables (available from the bedside
monitors) using special software.4
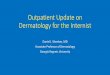
4.THE ROLE OF THE HEART:
First, the circulation is not controlled (as opposed to
energised) by the heart, but by the tissue flow
requirements for gas exchange and metabolism. Second, unlike
most pumps, the heart fills passively
- it is not a suction pump.
Consider the following analogy4 (Figure 4):
There are 2 water tanks connected by a pipe at the floor level.
The tanks have unequal heights of
water. Water drains continuously from the larger to the smaller
tank because the height of water in
the larger tank is more than in the smaller tank. This is
maintained by a pump which pumps water
continuously from the smaller tank to the larger one.
7
-
8/7/2019 Shock for the Internist
5/20
Indian Journal of Medicine 2011;1:4-23
Figure 4: The New Paradigm
Pms is the mean systemic filling pressure ;Pra is theRight
Atrial Pressure
Rvr is theResistance to Venous Return ;Flow is thevenous return
into the right atrium
The large reservoir of pressure head (Pms) has an exit pipe of
resistance Rvr at the base of the wall.The pipe fills a small
chamber of pressure head Pra. Within the chamber, a pump (the
heart) pumps
water back into the reservoir. The heart is careful to keep Pra
low and constant. The pumping
output thus equals the Venous Return Flow into the chamber.
When the right atrial pressure reaches the MCFP, venous return
ceases (Figure 5).
Figure 5: Venous return
Thus the true volume status of the body is reflected in the
MCFP.
The cardiac output is determined by the intersection of the two
curves (Figure 6) 5
8
-
8/7/2019 Shock for the Internist
6/20
Indian Journal of Medicine 2011;1:4-23
Figure 6: Cardiac output
The pump (the heart) has an efficiency denoted by EH (efficiency
of heart function)4
EH = (Pms Pra) / Pms = 1 (Pms / Pra )
This ratio EH is a clinically useful concept to assessing
cardiac performance. Consider two extreme
examples:
If the heart stops pumping, Pra = Pms and Pra/Pms = 1 and EH = 1
- 1 = 0.
If the heart is pumping well, Pra = 0; and (Pra / Pms) = 0 and
EH = 1- 0 = 1.
Thus, EH may be used as a parameter for assessing the need for
inotropes.
A functional perspective would be as follows (Figure 7):
Figure 7: Functional perspective of haemodynamics
9
-
8/7/2019 Shock for the Internist
7/20
Indian Journal of Medicine 2011;1:4-23
5. THE MICROCIRCULATION:
a. Systemic:
The average pressures (all in mm Hg) in the microcirculation are
summarized in Table 2.
Table 2: Pressures in the systemic microcirculation
SYSTEMIC (P)
HYDROSTATIC
Capillary Mean = plus 25 (40 = arterial end and 10 =venous
end)
Interstitial minus 2 (5 8) subcutaneous; plus 6 in brain;
positive in kidney / liver
ONCOTIC
Capillary plus 25 - 28
Interstitial plus 8 (0 10)
NET FORCE
Arterial end= [40 (-2)] [28 8]
= 42 20 = plus 22
(tending to force fluid from capillary into
interstitium)
Venous end=[10 (-2)]- [28 8]
= 12 20 = minus 8
(tending to force fluid back into capillary)
Note that as fluid leaves the capillary, the protein
concentration and hence the oncotic pressure rises
tending to pull back fluid (this is not shown in the
calculation) into the vessel.
The Interstitial Colloid Oncotic Pressure varies in the
different organs. Direct measurement is not
possible as samples will be contaminated. The estimation is
based on the presumption that
lymphatics drain the interstitial space and estimation of
protein content of lymph from various
organs will approximate the interstitial fluid protein.
The filtration reabsorbtion rates also differ in the various
organs. In the muscle, there is outward
movement at the arteriolar end and an inward movement at the
venous end as shown above. In the
glomeulus, the capillary hydrostatic pressure (CHP) is 50-60 mm
Hg and is always much higher than
the capillary colloid oncotic pressure (COP) - hence the flow is
outward through the whole length of
the glomerular capillary. In the intestine, the CHP is much less
than the COP, thus there is absorption
through the length of the capillary.
b. Pulmonary:
The functional pulmonary unit can be visualized as in Figure
8.
10
-
8/7/2019 Shock for the Internist
8/20
Indian Journal of Medicine 2011;1:4-23
CAPILLARY INTERSTITIUM ALVEOLI
Figure 8: The pulmonary microstructure
The permeability of pulmonary capillaries to protein is higher
than the permeability of systemic
capillaries. This results in more leakage of protein into the
pulmonary interstitium. The lymphatics
drain the interstitial space of about 30ml of fluid per
hour.
The pressures in the pulmonary microcirculation are given in
Table 3.
Table 3: Pressures in the pulmonary microcirculation
CAPILLARY INTERSTITIUM ALVEOLI
(Exposed to atmosphere)
HYDROSTATIC PLUS 7 MINUS 8 Surface tension
ONCOTIC PLUS 28 PLUS 14 Same as interstitial as there is
no protein barrier
NET EFFECT Fluid moves from capillary to interstitium and from
alveoli to interstitium; fluid
drained by lymphatics.
11
-
8/7/2019 Shock for the Internist
9/20
Indian Journal of Medicine 2011;1:4-23
The net negative interstitial hydrostatic pressure of about 1 mm
Hg along with the increase in the
interstitial colloid oncotic pressure along with the high
capacity for lymphatic drainage in the lungs
keeps the alveoli dry for optimum gas exchange. This also
explains why the low albumin in a
condition such as nephrotic syndrome can cause significant
peripheral oedema while there is no
pulmonary oedema. This is because:
-The oncotic pressure gradient does not balance out the
hydrostatic gradient as per Starlings law
they are on the same side of the equation.
-The permeability of pulmonary capillaries to protein equalizes
the oncotic pressure gradients to a
large extent. Hence pulmonary oedema occurs in response to
unbalanced hydrostatic pressures not
due to an imbalance of oncotic pressure.
MANAGEMENT OF SHOCK:1,9,10,11
The management of shock includes early definitive intervention
to stabilize haemodynamics, specific
therapy for the cause of shock (e.g transfusion for haemorrhagic
shock) and support of failed organ
systems.
The following are important principles:
1. Intervention in shock must be early and appropriate. Hence
devices which take time and expertise
(which may not be readily available) to insert are fine in
theory but are not likely to improve
outcome in reality.
2. Interventions must be evidence based not just on normalizing
physiology but on improving
outcome.
The following is the broad strategy:
1.EARLY RECOGNITION: The needle of clinical suspicion for shock
must have a very high sensitivity in
the appropriate scenario. This includes elderly patients,
patients admitted in ICUs, those with
indwelling devices or foreign bodies and post operative or post
trauma patients. Unwarranted
reliance on blood pressure numbers to diagnose shock will delay
initiation of therapy.
2.TARGET THE CAUSE (if feasible): As examples,
a. haemorrhage stop haemorrhage, replace blood; do not push up
blood pressure rapidly if the
source of bleed is not controlled (permissive hypotension)
b. anaphylaxis remove / stop offending antigen
c. sepsis drain any infected collection, short lag time (< 1
hour) from recognition to administer first
antibiotic dose
d. cardiogenic due to coronary occlusion: PTCA / thrombolysis as
appropriate
12
-
8/7/2019 Shock for the Internist
10/20
Indian Journal of Medicine 2011;1:4-23
e. pulmonary embolism: thrombolysis
f. tension pneumothorax / cardiac tamponade: evacuate air /
fluid
In some cases, it may not be possible to remedy the problem
immediately- e.g. septic shock in a
person with a prosthetic valve. In this case, the best available
options (adequate antibiotics, supportof failing organ systems)
must be implemented till definitive intervention is possible.
3. SUPPORT DYSFUNCTIONAL ORGAN SYSTEMS:
A.CARDIOVASCULAR:
The core principles to keep in mind for optimizing
cardiovascular physiology in shock are:
1.The Starling mechanism cannot by itself determine stroke
volume- it is not a control mechanism
but an executive mechanism which matches inflow to outflow. It
merely guarantees that it pumps
out whatever is put into it, if myocardial function is
normal
2.Cardiac output and venous return are interdependent
3.Cardiac output is the product of stroke volume and heart rate
and is the cause of arterial pressure
not its consequence. It makes no sense to write the equation as:
Cardiac Output = (Mean Arterial
Pressure RAP) / Systemic Resistance.
4.In a similar vein, the cardiac output is coupled to venous
return in a steady state, both are equal.
If venous return increases, RAP increases and so does Cardiac
Output till the output equals intake.
Increasing Cardiac Output will push more blood into the venous
system and increase venous return.
The reverse process also occurs.
5.The primary goal of the arterial system is to distribute blood
a fall in arterial pressure generates
two systemic responses: increase in cardiac output and increase
in peripheral resistance in addition
to a local response depending on tissue needs (regional changes
in resistance).
6.The primary goal of the venous system is to collect blood in
this context venous capacitance is
more important than venous resistance. Thus, in contrast to
arteriolar constriction (which increases
resistance to flow), venoconstriction does not result in an
increase in venous resistance with a
resultant decrease in return flow to the heart (with decreased
cardiac output). Venous constriction
reduces capacitance, shifts blood into the heart and increases
cardiac output.
The core haemodynamic goal in critical care is to keep the heart
optimally filled, the lungs dry (to
allow oxygenation) and the kidneys wet. In the absence of
appropriate measurable parameters,
this is a juggling act!
13
-
8/7/2019 Shock for the Internist
11/20
Indian Journal of Medicine 2011;1:4-23
Newer modes of assessment and intervention attempt to answer the
following questions:
a) Is the circulation underfilled / responsive to fluid?
b) Does this patient need a higher cardiac output to improve his
clinical condition?
c) Will fluid therapy be of benefit (ventricles are fluid
responsive)
or
will it do harm (flood the lungs)?
I)IS THE CIRCULATION UNDERFILLED / RESPONSIVE TO FLUID?
9,11,12,13,14
a. The Traditional Parameters: Pressure Measurements: CVP /
PAoP:
The CVP was the first parameter measured used to answer this
question. It was considered a
surrogate for the volume status of the body and hence the
filling pressures of the heart. However,
the CVP is only the filling pressure for the right heart. The
CVP by itself shown to be an insensitive
and non specific marker (Figure 9) of the bodys total volume
status. 6,9
Figure 9: CVP and body fluid status
CVP measurement was thereafter replaced by the PA catheter
measurement which also measured
the filling pressures of the left (pulmonary artery occlusion
pressure, PAoP) heart in addition to the
CVP. The classical protocol used was to normalize filling
pressures followed by the use of inotropes
/ vasoactive agents based on measured and calculated parameters
such as cardiac output and
peripheral resistance.
The PA catheter has not been shown to alter outcome in several
controlled clinical trials. 7
b. The New Parameters:11,12,13,14
Respiratory variation of parameters:
In the following discussion, variation is mathematically
calculated as follows:
14
-
8/7/2019 Shock for the Internist
12/20
Indian Journal of Medicine 2011;1:4-23
Variation % = [(Maximum minus Minimum) / Average] x 100
Variation % = [(Maximum minus Minimum) / {(Max + Min)/2}] x
100
1. IVC diameter variation:
The respiratory variation in superior and inferior vena caval
diameter have been used to predictvolume status (preload
responsiveness) in ventilated patients. The diameters are measured
using
bedside sonology.
The IVC collapse index (IVC-CI) is used:
IVC-CI = (IVCDmax IVCDmin) / IVCDmean.
In healthy subjects breathing spontaneously, the IVC has a
larger diameter in expiration and a
smaller diameter in inspiration.
For those on positive pressure ventilation, the changes in IVC
diameters in relation to the respiratory
cycle are the reverse of the measurements compared to those
breathing spontaneously (maximumduring positive pressure and
minimum during exhalation). The maximum and minimum
measurements can also be made without reference to the
respiratory cycle.
A IVC-CI value > 12% indicates that the vascular volume is
underfilled.
2.Stroke Volume Variation:
This is based on the fact that positive pressure ventilation
causes cyclic changes in intrathoracic
pressure which result in cyclic changes in LV output (stroke
volume). These changes are seen best in
mechanically ventilated patients. A value > 12% indicates
that the vascular space is underfilled.
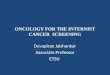
3.Pulse Pressure Variation (Figure 10):
Some invasive blood pressure monitors give the pulse pressure
variation on the monitor itself
making it a useful bedside parameter.
Figure 10: Pulse Pressure Variation
The threshold value for an underfilled vascular system using an
arterial pulse pressure variation is
> 12%.
15
-
8/7/2019 Shock for the Internist
13/20
Indian Journal of Medicine 2011;1:4-23
4. Pulse oximetry plethysmogram:
It has been shown that the respiratory changes in the amplitude
of the plethsmographic pulse wave
(pulse oximeter) allows the prediction of fluid responsiveness
in mechanically ventilated septic
patients. The threshold value for a patient who will respond to
volume for the plethysmographic
pulse pressure variation is > 14%.
5. Passive Leg Raising (PLR):
PLR is based on the principle that raising the lower limbs
induces an abrupt increase in venous return
secondary to auto-transfusion of peripheral blood from
capacitive veins of the lower part of the
body. This is equivalent to an internal fluid challenge
equivalent to a 300 - 500ml fluid bolus. The
lower limbs are both lifted in a straight line to an angle of 30
o - 45o for 4 minutes. It has the added
advantage that it is reversible on lowering the legs (if
pulmonary oedema occurs).
The maximal haemodynamic effects of PLR occurs within the first
minute of leg elevation. The value
to be noted is the change systolic blood pressure or the pulse
pressure not the change in mean or
diastolic blood pressure. This is intuitive as the systolic /
pulse pressure corresponds to the stroke
volume.
The PLR test can be used both for mechanically ventilated and
spontaneously breathing patients.
6. Fluid challenge:
This is done to assess the responsiveness of the cardiovascular
system to an increase in intravascular
volume. 200 500 ml of fluid is given over 10 minutes. Pulse
pressure variation or stroke volume
variation in response to the fluid challenge is then
measured.
Assessments of predictive tests for fluid responsiveness are
most relevant when focused in patients
with hypoxemic or cardiac failure.
II)Does this patient need a higher cardiac output to improve his
clinical condition?
The primary goal of any therapeutic intervention is to maintain
tissue oxygenation and perfusion.The
finding that a persons vascular space is underfilled or fluid
responsive does not imply that fluid
administration is useful or necessary. Even healthy walking
persons are fluid responsive!! In addition,
administration of fluid will not result in better perfusion if
the myocardium cannot cope with the
increased load. In this case, inotropes will be needed.
The available technology to monitor regional perfusion is
neither easily available nor clinicallyvalidated. It is also
possible that regional circulations may show heterogeneity of
perfusion in shock.
The current measures used are global indicators for adequacy of
oxygenation & perfusion. These
are:
a)arterial lactate (a value >2mmmol/L) implies that the
tissues have switched to anaerobic
metabolism due to inadequate oxygen delivery (it can also be
because of reduced clearance, hence
an overall perspective is essential)
b)ScvO2 is the oxygen saturation of haemoglobin in blood
returning to the heart. If the tissues do
not receive adequate oxygen, they will extract more of the
oxygen being delivered and the blood
returning to the heart will show more desaturation (SvO2 <
70%) as compared to those with better
perfusion. The limitation is that if blood is shunted in the
periphery (the tissues are bypassed) thevenous blood may not show
desaturation even though the tissues are not getting adequate
oxygen.
16
-
8/7/2019 Shock for the Internist
14/20
Indian Journal of Medicine 2011;1:4-23
A recent study15 shows that a high central venous oxygen may
also be a surrogate for impaired
tissue oxygenation as the unused / unusable oxygen is being
returned. In the observational
study published in 2011, in patients undergoing cardiac surgery,
it was shown that both low
(< 60.8%) and supranormal (>77.4%) ScvO2 were predictors
of a complicated post operative period.
Lactate was comparably increased in the patients who died
irrespective of whether they had low or
supranormal ScvO2. Lactate was higher in patients who had a
supranormal ScvO 2.15
However, thisfinding needs to be confirmed in patients with
sepsis.
Hence a low as well as a supranormal ScvO2 may be signs of
inadequate tissue oxygenation.
c) Veno- arterial carbon dioxide difference:
The veno- arterial carbon dioxide difference is a surrogate
marker for cardiac output. It has been
shown in a study that the cardiac output is inversely correlated
with the venous-arterial PCO 2. In
states of decreased flow (cardiac output), there is an increase
in the difference. As a rule of thumb, if
the difference is >7 mm Hg, the cardiac index is low (<
2.5 l/min/m2).
III) Will fluid therapy be of benefit (ventricles are fluid
responsive) or will it do harm (flood thelungs)?16
If a maneuver to increase cardiac output results in arterial
hypoxia by flooding the lungs, the whole
purpose of improving tissue oxygenation / perfusion is lost. The
core of the problem in managing
fluid balance is to achieve a balancing act between sufficient
filling of the cardiovascular system
while avoiding pulmonary oedema. The main concern in giving
additional fluid is that the lungs will
get wet which in turn will affect oxygenation. This would defeat
the primary purpose of the goal to
improve tissue oxygenation.
It is also well documented16 that the amount of Extravascular
Lung Water (EVLW) is an independent
predictor of prognosis. Techniques to estimate EVLW) are
available. Those with EVLW > 15ml / kg
had a mortality rate of about 65% while those with an EVLW <
10ml / kg had a survival rate of about67%.
The PICCO (Pulse Contour Cardiac Output) technique utilizes a
standard CVP line and a special
arterial catheter with a thermistor to measure EVLW.
Dynamic studies are also useful to answer this question.
1. PLR & S/F ratio:
If the SpO2 is simultaneously noted during PLR and there is no
drop in oxygen saturation, there is
likely to be good tolerance to volume expansion. If the SpO 2
drops significantly, it is likely that fluid
administration may cause more harm (pulmonary oedema as the left
ventricle cannot cope with theadded volume) than good and inotropes
may be indicated.
However, it should be remembered that the SpO2 must be < 97%
for the test to be useful because
the S/F ratios and P/F ratios are concordant only if SpO 2 is
< 97%. This is because the maximum
numerical value for SpO2 is 100 while the PaO2 may be 500. If
there is good oxygenation, but the
heart cannot take an additional load, an increase in lung water
with a drop in PaO 2 from 500 to 200
will not be reflected in the SpO2 which will remain at 100.
The Passive Leg Raising test can answer the two questions stated
above but in different time frames.
The change in pulse pressure/systolic blood pressure takes place
within a minute but changes in
oxygenaton (as seen in the SpO2) can take up to 5 minutes.
17
-
8/7/2019 Shock for the Internist
15/20
Indian Journal of Medicine 2011;1:4-23
2. Fluid bolus administration (Fluid Challenge) &
Oxygenation Indices:
If the oxygen transfer indices (P/F ratio / PA-a difference) is
normal, fluid challenge can beconsidered safe. However, a low P/F
ratio or PA-a difference does not rule out the need for fluid
administration. The oxygen transfer may improve with increasing
cardiac output as pulmonary
perfusion improves.
Repeated evaluation of the P/F ratio with bolus administration
of fluid will give an idea as to
whether the lungs are becoming wet with fluid therapy. Hence the
P/F ratio will need to be
reassessed at regular intervals to check for any deleterious
increase in lung water with interference
of oxygenation.
It should be noted that these methods of evaluating safe to fill
have not been clinically validated.
The bedside ECHO17 (Bedside sonology) can also be used to assess
cardiac contractility, cardiacoutput, lung water and response to
fluid therapy.
Remember:
IF
The peripheral tissues need an increase in perfusion
AND
The circulatory system is not fluid responsive OR It is not safe
to fill
THEN
inotropes have to be used.
B) RESPIRATORY:
Is the Respiratory System able to meet the need of the body in
order to:
1. oxygenate
2. maintain pH
If this is not possible, Mechanical Ventilatory Support may be
needed.
C)RENAL:
Is renal function adequate to maintain fluid, electrolyte and
acid base homeostasis.
If not, Renal Replacement Therapy is indicated. Acidosis results
in a suboptimal response to
inotropes/vasopressors. The exception is vasopressin which acts
even in an acidic environment.
D)LIVER:
Is hepatic function adequate to maintain metabolic
homeostasis?
Avoid hepatotoxic drugs if hepatic function is impaired.
18
-
8/7/2019 Shock for the Internist
16/20
Indian Journal of Medicine 2011;1:4-23
E) TARGET MEDIATORS OF INFLAMMATION (if evidence is
adequate):
These include activated Protein C (rhAPC), Immunoglobulins or
hemoperfusion through a column ofimmobilized polymyxin B (PMX-B).
There is controversy regarding the usefulness of these modes of
therapy.
COMPONENTS FOR INTERVENTION:
FLUID :18,19
The choice of fluid for resuscitation has been the subject of
intense debate for many years.
Physiologically, colloids expand intravascular volume more than
crystalloids. Hence, these were
considered, to be the fluid of choice in shock. Others opined
that in shock, vascular permeability wasimpaired, thus allowing
colloid particles to leak into the interstitium thereby pulling
more fluid out of
the vascular system into the interstitium.
Clinical trials showed that crystalloid solutions had less
complications (renal dysfunction) when used
in resuscitation. The adverse effects are probably related to
hyperoncotic colloids which were used
and hence colloid solutions which have lower oncotic pressure
are now being suggested for
resuscitation.
INOTROPES: 20,21,22,23,24
The choice of inotropic/vasoactive drugs should be based not
only on the pattern of physiological
abnormalities (profile analysis) but also on the evidence of
randomized trials showing improvedoutcome (and not just improvement
in measured parameters). Good quality clinical trials for
inotropes are now available. Appropriate inotropes tailored to
the situation should used. Careful
monitoring of the response is mandatory as significant inter
individual variability can exist.
Adrenaline vs Noradrenaline:
It has been shown that there is no difference between adrenaline
(epinephrine) and noradrenaline
(norepinephrine) plus dobutamine in terms of efficacy or safety
when used in patients with septic
shock.
Dopamine vs Noradrenaline / other inotropes:
There is no renal protection in using low dose dopamine in
critically all patients.
Early small observational studies had suggested that treatment
with dopamine may be detrimental
for patients with septic shock. In a comparison of dopamine and
noradrenaline, the results showed
that there was no significant difference in mortality. However,
there were more arrhythmic events
among the patients treated with dopamine than in those treated
with noradrenaline.
Vasopressin:
Low-dose vasopressin did not reduce mortality rates as compared
with norepinephrine among
patients with septic shock. The advantage is that it maintains
its action even if there is acidosis.
19
-
8/7/2019 Shock for the Internist
17/20
Indian Journal of Medicine 2011;1:4-23
First use protocol - Fluids or Inotropes?
It is important to remember that a numerically acceptable MAP at
the cost of intense
vasoconstriction does not achieve the goal of optimising tissue
perfusion. Keeping this in mind, fluids
should generally be used first if it is safe (patient not in
pulmonary oedema). However, if the blood
pressure is crashing with an impending cardiac arrest, it would
be best to start fluids and inotropes
simultaneously, stabilize the blood pressure and then do the
tests for fluid responsiveness prior to
further fluid administration.
PUTTING IT ALL TOGETHER A SYN-OPTIC VIEW:
A syn-optic view of managing a patient in shock, termed by its
acronym, SITEMAP, is given.
SITEMAP stands for STRUCTURED INTERVENTION by TARGETED
EVALUATION to MAINTAIN
ADEQUATE PERFUSION (Figure 11).
Figure 11: SITEMAP
The conceptual points are not to be seen in serial order but
simultaneously. Continuing monitoring
and intervention are necessary to ensure that tissue perfusion
continues to be optimized.
The central starting conceptual point is the lack of tissue
perfusion. This lack of tissue perfusion
should intuitively include significant hypotension but not be
the sole criterion. A Mean Arterial
Pressure (MAP) below 60mm Hg will be an inadequate pressure head
for perfusion in most people.
Some (e.g chronic hypertensives) will need a higher mean
arterial pressure to maintain tissue
perfusion while others (e.g. those with chronic congestive
cardiac failure) can manage with a lower
MAP as they have adapted to the low pressure state with time.
The other starting point will be
abnormal markers of suboptimal tissue perfusion (lactate,
ScvO2).
20
-
8/7/2019 Shock for the Internist
18/20
Indian Journal of Medicine 2011;1:4-23
PATTERNS OF SCVO2 AND LACTATE LEVELS:
This may be seen as one of several possible patterns (Table
4).
Table 4: SCVO2 and lactate patterns:
HAEMOGLOBIN:
In a critically ill septic patient, the optimum haemoglobin is
7-8 g%. A higher level of 10 g% may be
needed in a critically ill patient with myocardial or cerebral
ischemia .
ADEQUATE CARDIAC OUTPUT:
The cardiac output should be optimized to the need for tissue
perfusion not to a numerically normal
value.Assessment of Cardiac Output should be done only after the
Mean Arterial Pressure is
normalized (with vasopressors if needed). In the presence of
significant reduction in peripheral
resistance, even if the myocardium is hypofunctioning, the
cardiac output may be in the
numerically normal range . If the systemic vascular resistance
is increased using vasopressors, the
myocardium will then reveal its true colours as it is now
pumping against an increased resistance
to maintain an adequate MAP. However, most vasopressors used in
critical care (dopamine,
noradrenaline, adrenaline) are in fact inopressors and not pure
vasopressors. Thus the cardiac
output estimated while giving these inopressors will have a
component of inotropic effect (it may
show a higher value).Dobutamine is an inodilator as it has a
peripheral vasodilator action in addition
to its inotropic effect.
21
ScvO2 Lactate level Pathophysiological Diagnosis
High15
(> 77%)
High
Peripheral shunt, increased lactate production,
decreased lactate clearance, mitochondrial poison
interfering with oxidation pathway
Low10,15
(
-
8/7/2019 Shock for the Internist
19/20
Indian Journal of Medicine 2011;1:4-23
Conflict of interest: None declared
References:
1. Antonelli M, Levy M, Andrews PJD, Chastre J, Hudson LD,
Manthous C, et al. Haemodynamic monitoring in shock
and implications for management. International Consensus
Conference, Paris, France, 27 28 April, 2006.
Intensive Care Med. 2007; 33: 575 590
2. Levick JR et al. Haemodynamics: flow, pressure &
resistance in An Introduction to Cardiovascular Physiology.
Great
Britain: Arnold. 2003(4 Edition); pp104 130
3. Parkins WG. Volume State Control A New Approach. Crit Care
& Resuscitation. 1999;1:311-321
4. Parkins WG & Leaning MS. Therapeutic control of the
circulation. Journal of Clinical Monitoring and Computing.
2008;
http://dx.doi.org/10.1007/s10877-008-9147-7 (accessed on 3
February 2011)
5. Magder S. Pathophysiology of Cardiovascular Failure. In:
Albert RK, Slutsky A, Ranieri M, Takala J, Torres A, editors.
Clinical Critical Care Medicine. Philadelphia: Mosby. 2006; pp
283 299
6. Gelman S. Venous Function and Central Venous Pressure. A
Physiologic Story. Anaesthesiology 2008; 108: 735 748
7. Rubenfeld GD, McNamara-Aslin E, Rubinson L. The Pulmonary
Artery Catheter 1967-2007 Rest in Peace? JAMA 2007;
298: 458 - 461
8. Rothe CF. Mean Circulatory Filling Pressure: its meaning and
measurement. Journal of Applied Physiology 1993; 74:
499 509
9. Marik PE, Baram M, Vahid B. Does Central Venous Pressure
Predict Fluid Responsiveness? A Systematic Review of the
Literature and the Tale of Seven Mares. Chest 2008;
134:172178
10. Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich
B et al. Early goal directed therapy in the treatment of
sepsis and septic shock. N Engl J Med 2001; 345: 1368 1377
11. Nichols D &Carlson RW, editors. Optimising haemodynamic
support in severe sepsis and septic shock. Critical Care
Clinics 2010; 26: 239 - 421
12. Monnet X & Teboul JL. Volume responsiveness. Current
Opinion in Critical Care 2007; 13: 549 553
13. Michard F. Volume management using dynamic parameters. The
Good, the Bad and the Ugly. Chest 2005; 128: 1902
1904
14. Pinsky MR & Payen D. Functional Haemodynamic Monitoring.
Critical Care 2005; 9: 566 572
(http://dx.doi.org/10.1186/cc3927, accessed 3 February,
2011)
15. Perz S, Uhlig T, Kohl m, Bredle DL, Reinhart K, Bauer M,
Kortgen A. Low and supranormal central venous oxygen
saturation and markers of tissue hypoxia in cardiac surgery
patients: a prospective observational study. Intensive Care
Med 2011; 37: 52 - 59
16. Sakka SG, Klein M, Reinhart K, Meier-Hellman R. Prognostic
value of Extravascular Lung Water in Critically Ill patients.Chest
2002; 122: 2080 - 2086
17. Price S, Nicol E, Gibson DG, Evans TW. Echocardiography in
the critically ill: current and potential roles. Intensive Care
Med. 2006; 32: 48 59
18. The Safe Study Investigators. A comparison of Albumin and
Saline for Fluid Resuscitation in the Intensive Care Unit.
The New Engl. J Med. 2004; 350: 2247 2256
19. Brunkhorst FM, Engel C, Bloss F, Meier-Hellmann A, Ragaller
M, Weiler N et al. Intensive Insulin therapy and
Pentastarch resuscitation in severe sepsis. (VISEP trial):Volume
Substitution and Insulin Therapy in Severe Sepsis ) New
Engl J Med 2008; 358:125 139.
20. Myburgh JA. An appraisal of selection and use of
catecholamines in septic shock old becomes new again. Crit Care
and Resuscitation 2006; 8: 353 360
22
-
8/7/2019 Shock for the Internist
20/20
Indian Journal of Medicine 2011;1:4-23
21. Boulain T, Runge I, Bercault N, Benzekri-Lefevre D, Wolf M,
Fleury C. Dopamine therapy in septic shock: detrimental
effect on survival? J Crit Care 2009; 24: 575- 582.
22. Pvoa PR, Carniero AH, Ribeiro OS, Pereira AC. Portuguese
Community-Acquired Sepsis Study Group. Influence of
vasopressor agent in septic shock mortality: results from the
Portuguese Community-Acquired Sepsis Study (SACiUCI
study). Crit Care Med 2009; 37: 410-416.
23. De Backer D, Biston P, Devriendt J, Madl C, Chochvad D,
Aldecoa C et al. Comparison of Dopamine and Norepinephrinein the
Treatment of Shock. The New Engl. J Med. 2010; 362: 779 789
24. Gordon AC, Russel JA, Walley KR, Singer J, Ayers D, Storms
MM et al. The effects of vasopressin on acute kidney injury
in septic shock (VASST, vasopressin and septic shock trial).
Intensive Care Medicine 2010; 36: 83 91
23