Embed Size (px)
Citation preview
Nephrotic & Nephritic Syndromes
By:Dawit AyeleMD,Internist
objectives
• Understand the difference betweennephrotic and nephritic syndrome• Understand the biology of the glomerularfiltration barrier• Differentiate primary from secondarynephrotic syndromes• Approach to management of nephroticsyndromes
• WHAT MAKES THESE DISORDERS DIFFERENT?
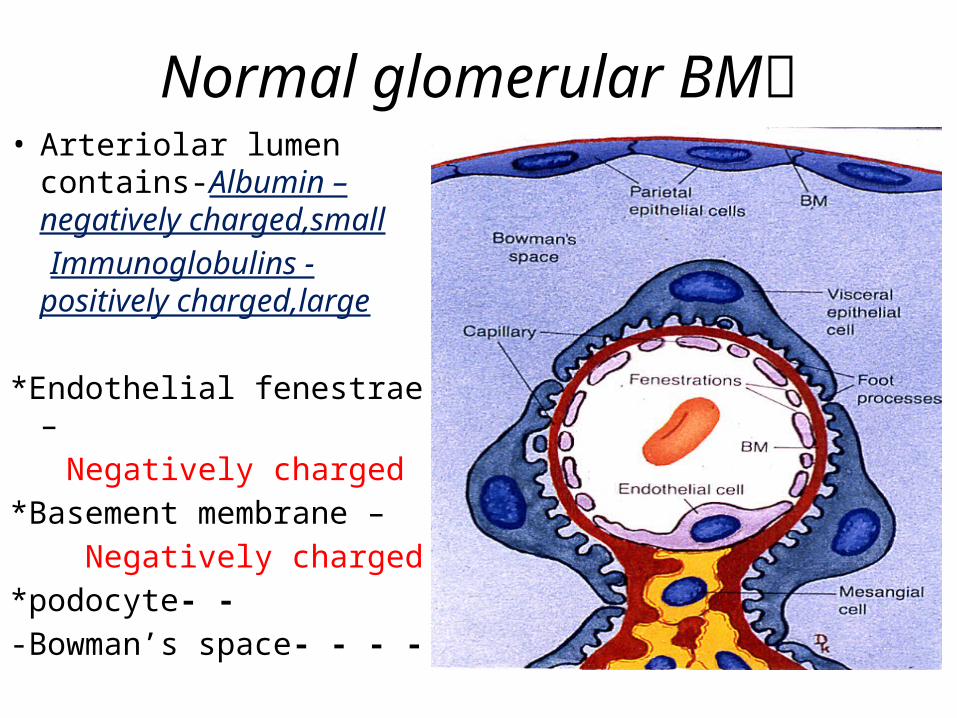
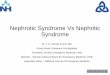
Normal glomerular BM• Arteriolar lumen contains-
Albumin –negatively charged,small
Immunoglobulins -positively charged,large
*Endothelial fenestrae – Negatively charged*Basement membrane – Negatively charged*podocyte- --Bowman’s space- - - -
How do we make a diagnosis?
• Clinically, at thebed side?• Investigations?
Nephrotic syndrome
• Proteinuria > 3g/day (adult)• Proteinuria >40mg/h/m2 (child)• Hypoalbuminemia• Edema• Hyperlipidemia• Lipiduria
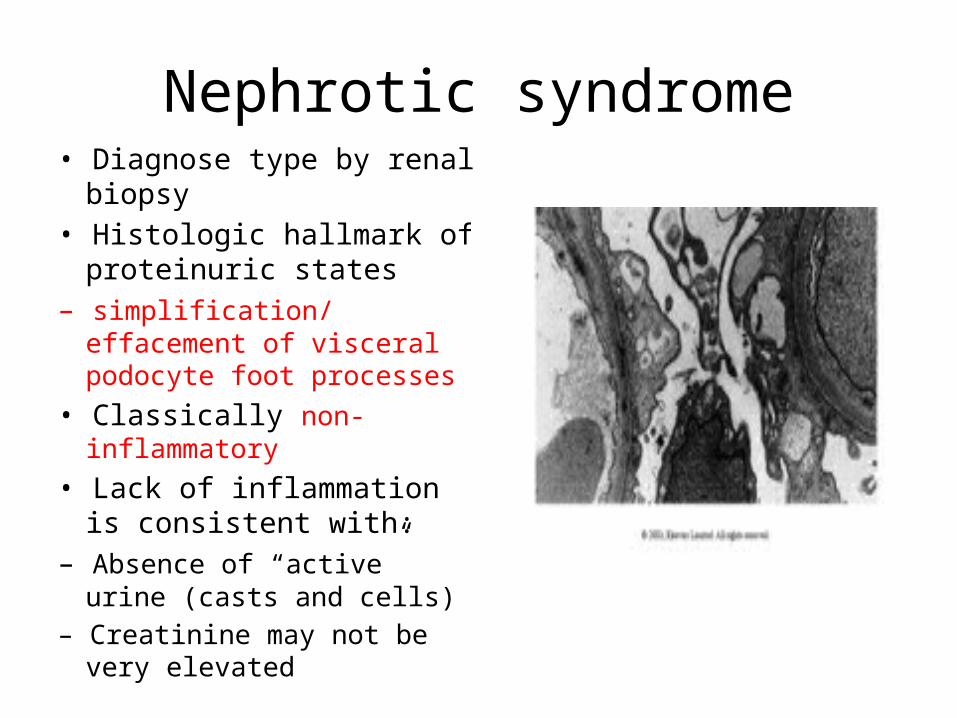
Nephrotic syndrome• Diagnose type by renal biopsy• Histologic hallmark of
proteinuric states– simplification/ effacement of
visceral podocyte foot processes
• Classically non-inflammatory• Lack of inflammation is
consistent with:– Absence of “active” urine (casts
and cells)– Creatinine may not be very
elevated
Proteinuria
Depends on charge and size of molecules• Small negatively charged molecules e.g..albumin are repelled by negatively chargedcapillary wall• Loss of charge but no overt structural injury can
cause→ albuminuria (minimal change disease)• Immunoglobulins are positively charged but toobig to get through unless structural injury
Urine Protein
• A normal person has 7200g(180Lx 40g/L albumin) passthrough the glomerulus every day(not filtered)• Normal excretion of < 20mg/day =fractional excretion of0.00028%!!!!!!!!!!!!!!!!!!!!!!!!!• Even a nephrotic patient excreting3g a day = 0.42%
Diagnosing Proteinuria
• Dipstick positive:– Likely > 150 – 300 mg/24h– Measure protein: creatinine ratio (PCR) 24h Urine Protein ≈PCR• Dipstick negative:– Cannot exclude proteinuria, especially in DMand HT– Send albumin : creatinine ratio (ACR) ifavailable (expensive)

Categories of nephrotic syndrome
• Primary renal:– Minimal change disease– Focal Segmental Glomerulosclerosis– Membranous• Secondary– Diabetes– Amyloid– HIV– Drug associated: NSAIDS, gold, pamidronate– Etc…

Diagnoses made clinically and onbiopsy
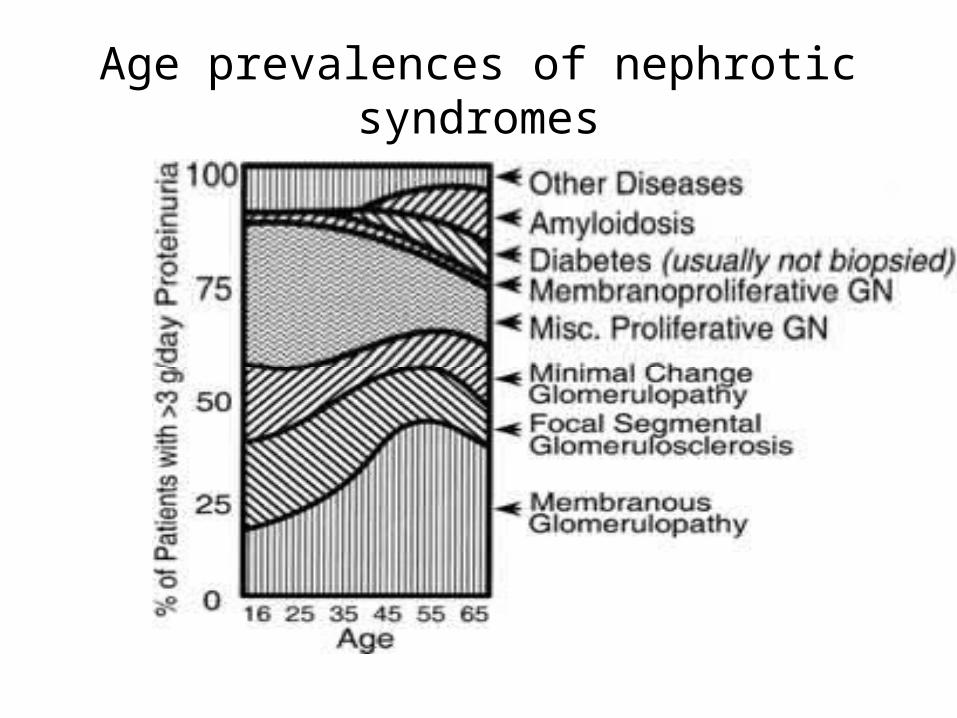
Age prevalences of nephroticsyndromes
Minimal change disease (MCD)
• 90% of nephrotic syndrome in children• 20% of nephrotic syndrome in adults• May not need biopsy• Trial of steroids is part of diagnosis• May be beginning of spectrum ranging to FSGSespecially in black children• Secondary forms may be associated withallergies, drugs (NSAIDS!!!), hematologicmalignancies, viral infections

Minimal Change Disease
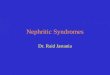
• Light microscopy normal• Normal immunostaining• • Electron microscopy
shows fusion of podocyte foot processes
• There is loss of negative charge
Specific treatment of 1° MCD
• 90% respond to steroids with 4-6 weeks– Taper over 6 weeks– Proteinuria resolves before albumin improves• Implies not only decreased oncotic pressure driving
edema…• 25 % long term remission• 25-30% infrequent relapses• 20% chronically relapse – steroid dependent• 5% don’t respond – steroid resistant
Membranous Nephropathy
• Most common cause of 1°nephrotic syndrome inadults (25%)• Peak incidence in 4-5th decade (adult: child26:1)• 2-3:1 male predominance at ESRD• Affects all races• Differences in secondary causes may causegeographic differences in presentation
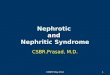
Membranous
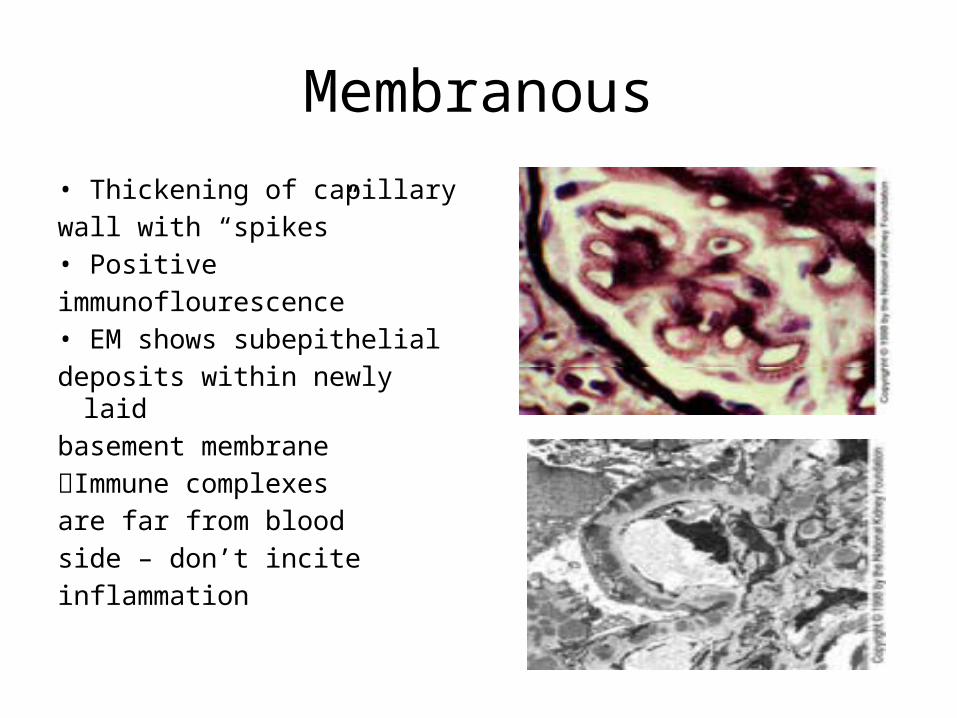
• Thickening of capillarywall with “spikes”• Positiveimmunoflourescence• EM shows subepithelialdeposits within newly laidbasement membraneImmune complexesare far from bloodside – don’t inciteinflammation
Clinical features
• Usually presents as nephrotic syndrome but 10-20% have < 2g/d proteinuria• HT from 13-55%• Most have slightly decreased renal function• Usually progresses slowly → must investigateabrupt change in renal function– Crescents 1/3 have anti GBM, some have ANCA– Renal vein thrombosis (4-52%)– Drug-induced injury: NSAIDS, diuretics, antibiotics
Clinical features
• Microscopic haematuria in 30-50%• Impaired renal function at presentation <10%• C3 and C4 typically normal• Hyperfibrinogenaemia and decreasedantithrombin 3– Renal vein thrombosis in 5-63%– Deep vein thromboses 9-44%– Consider anticoagulation if albumin < 20g/L
Causes of Membranous Nephropathy
1° • Idiopathic2°• Malignancy (colon, lung, gastrointestinal)• Autoimmune diseases: SLE, rheumatoid arthritis,
autoimmune thryroiditis• Drugs: penicillamine, gold• Infections: Hep B virus, Syphilis (congenital and
secondary), Hep C, Hepatosplenic schistosomiasis• Chronic transplant rejection• Rarely sarcoid, captopril• Other Glomerulonephritides

Treatment of membranous
• Determine whether idiopathic or 2°• Decision should be based on anunderstanding of natural history:– Spontaneous remission in 5-30%– Partial remission (Proteinuria<2g/d) in 25-40%– Relapse rate 30-50% but only 5% → ESRD– Renal survival:• 86% at 5 years• 65% at 10 years
Treatment of membranous
• If poor prognositic factors or progressing– Hypertension– Male– Elevated creatinine• Steroids chlorambucil or otherimmunosuppression, ? Rituximab, ?mycophenolate
Nonimmunologic therapy of allnephrotic syndromes
• Treatment of hypertension esp. ACEI, ARB– Target < 120/75• Treatment of hypercholesterolemia– Target LDL < 2.0• Low sodium diet• Calcium and vit D to reduce bone loss if steroidtherapy is prolonged• Bactrim for PCP prophyllaxis if steroids• INH for TB prophyllaxis if immunosuppressed• Anticoagulate if high risk• Treat underlying cause if secondary
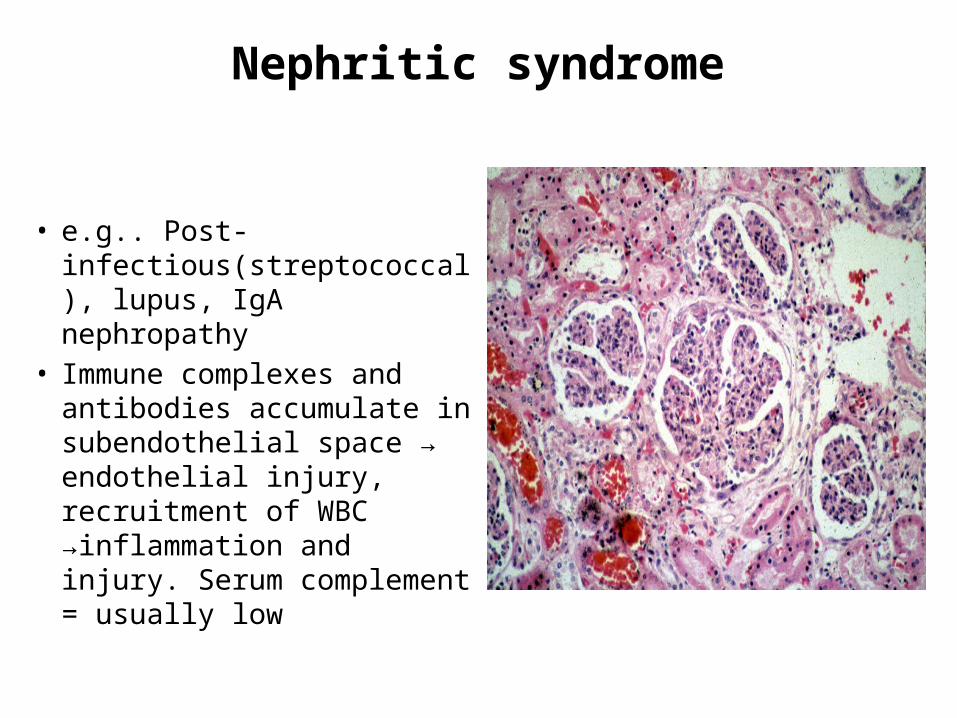
Nephritic syndrome
• e.g.. Post-infectious(streptococcal), lupus, IgA nephropathy
• Immune complexes and antibodies accumulate in subendothelial space → endothelial injury, recruitment of WBC →inflammation and injury. Serum complement = usually low
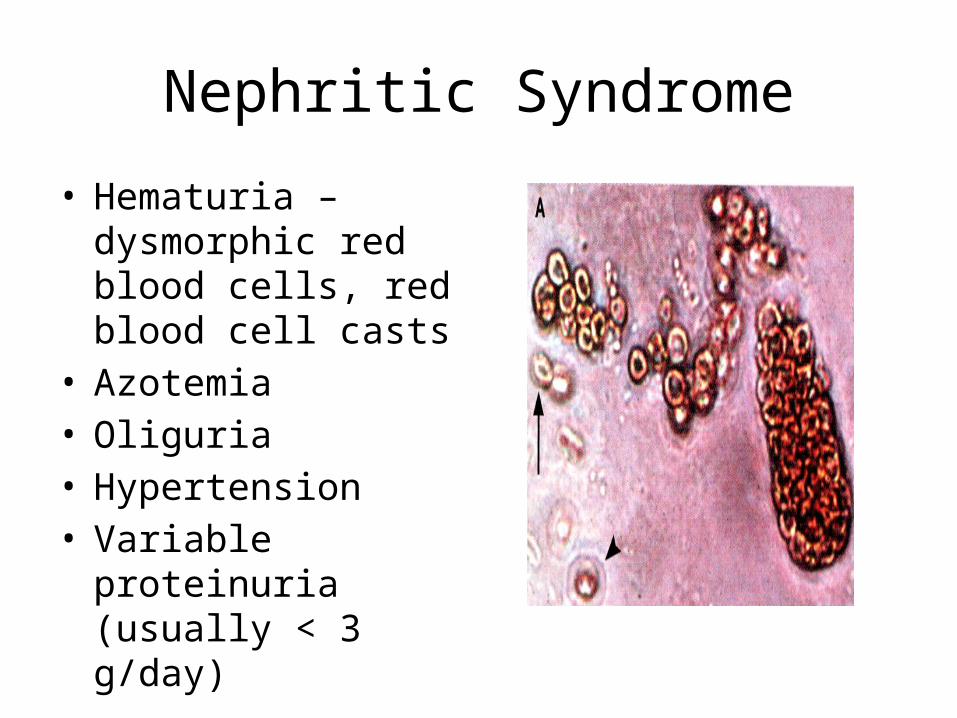
Nephritic Syndrome
• Hematuria – dysmorphic red blood cells, red blood cell casts
• Azotemia• Oliguria• Hypertension• Variable proteinuria
(usually < 3 g/day)
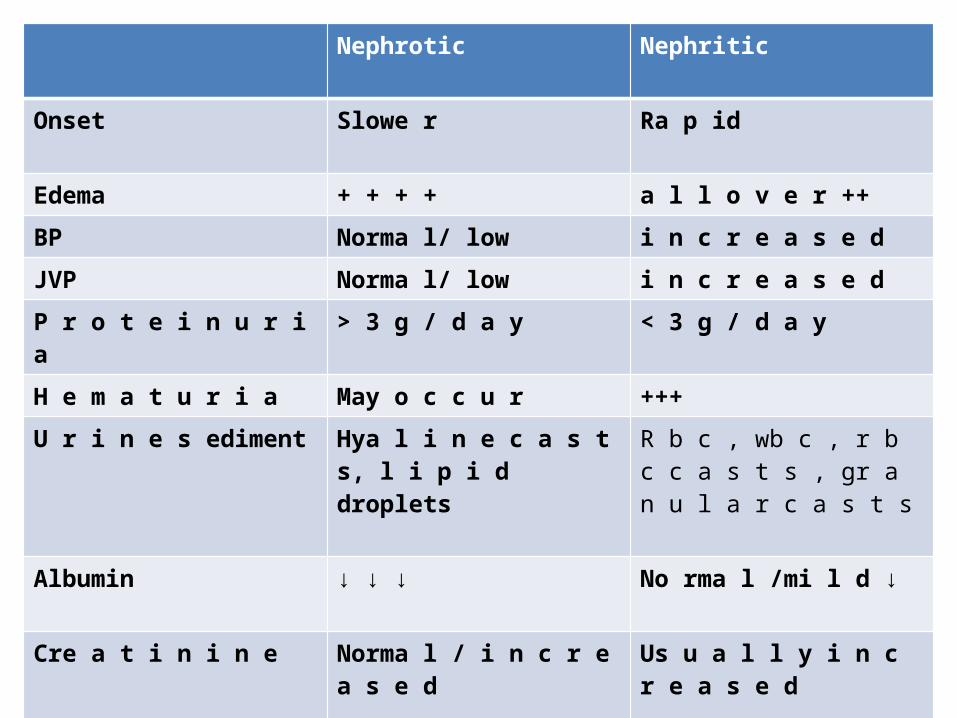
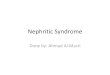
Nephrotic Nephritic
Onset Slowe r Ra p id
Edema + + + + a l l o v e r ++
BP Norma l/ low i n c r e a s e d
JVP Norma l/ low i n c r e a s e d
P r o t e i n u r i a > 3 g / d a y < 3 g / d a y
H e m a t u r i a May o c c u r +++
U r i n e s ediment Hya l i n e c a s t s, l i p i d droplets
R b c , wb c , r b c c a s t s , gr a n u l a r c a s t s
Albumin ↓ ↓ ↓ No rma l /mi l d ↓
Cre a t i n i n e Norma l / i n c r e a s e d Us u a l l y i n c r e a s e d
Ser u m sodium Ma y b e ↓ ↓ Ma y b e ≈ ↓
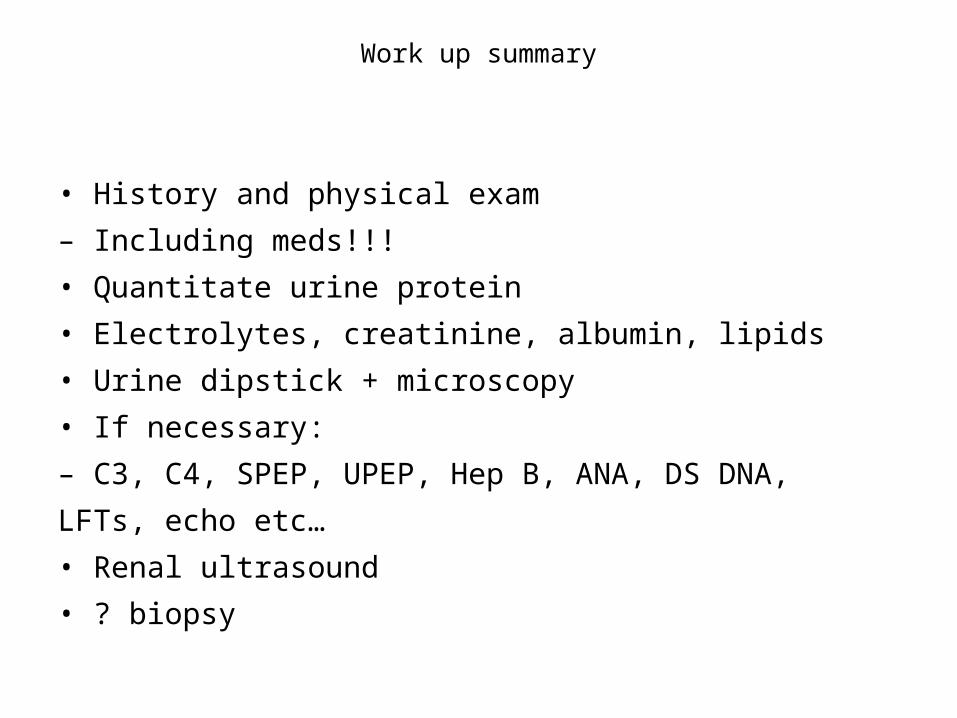
Work up summary
• History and physical exam– Including meds!!!• Quantitate urine protein• Electrolytes, creatinine, albumin, lipids• Urine dipstick + microscopy• If necessary:– C3, C4, SPEP, UPEP, Hep B, ANA, DS DNA,LFTs, echo etc…• Renal ultrasound• ? biopsy
Thanks