Embed Size (px)
Citation preview
Kianmanesh 2021
Should we resect the primary tumor in metastatic NENs?
Prof. Reza Kianmanesh, MD, PhD.
(Hopital Robert Debre, Reims, France, University of Champagne Ardenne, France)
Kianmanesh 2021
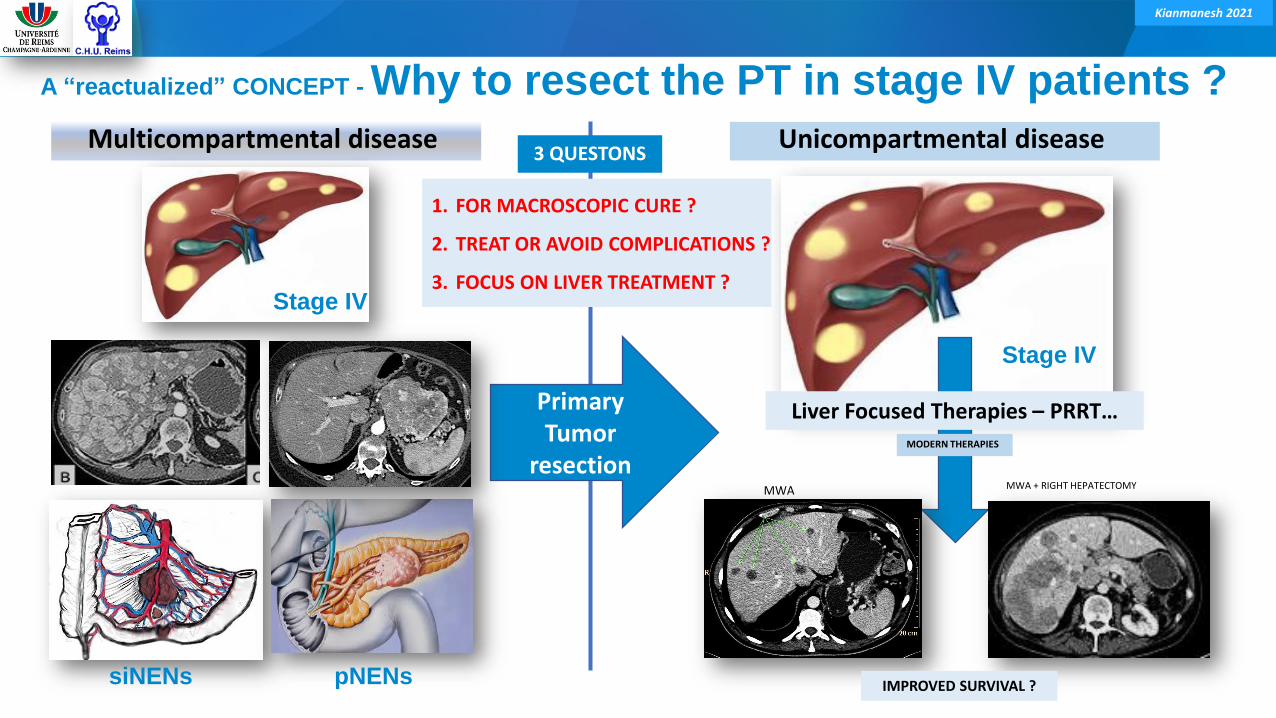
A “reactualized” CONCEPT - Why to resect the PT in stage IV patients ?
PrimaryTumor
resection
Multicompartmental disease
siNENs pNENs
Stage IV
Unicompartmental disease
MWA MWA + RIGHT HEPATECTOMY
Liver Focused Therapies – PRRT…
Stage IV
MODERN THERAPIES
IMPROVED SURVIVAL ?
1. FOR MACROSCOPIC CURE ?
2. TREAT OR AVOID COMPLICATIONS ?
3. FOCUS ON LIVER TREATMENT ?
3 QUESTONS
Kianmanesh 2021
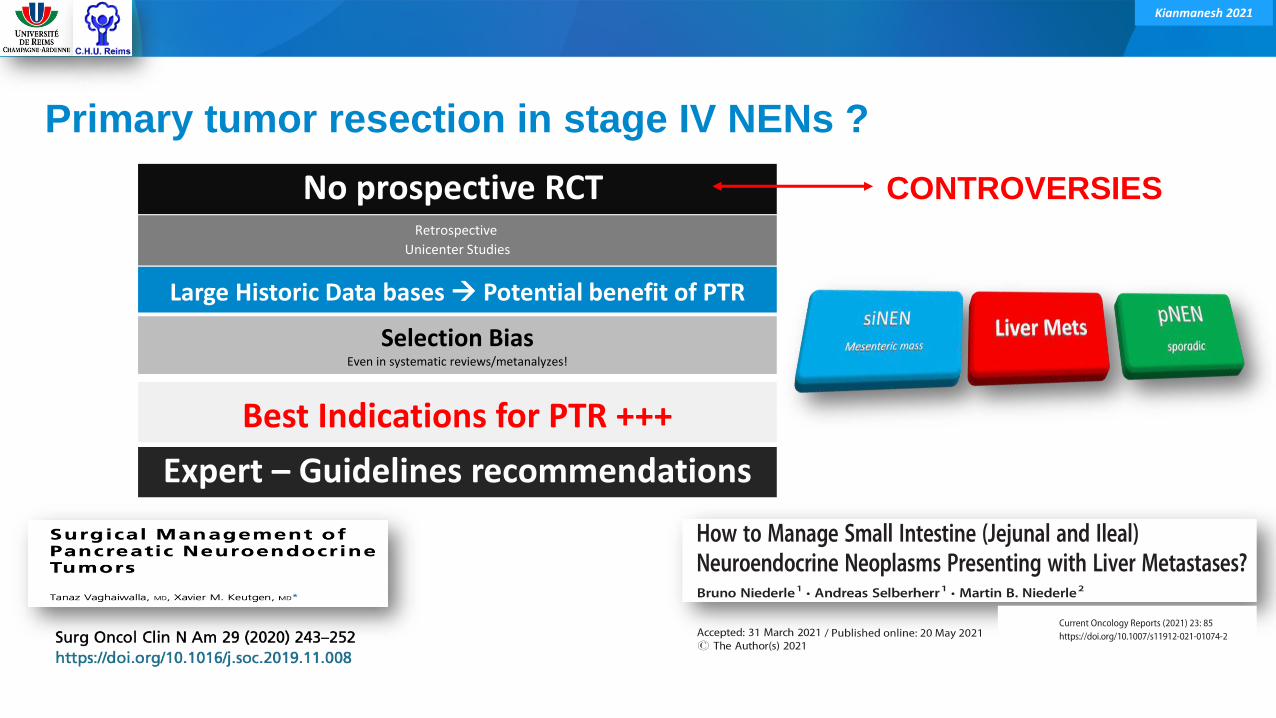
CONTROVERSIES
Primary tumor resection in stage IV NENs ?
No prospective RCT Retrospective
Unicenter Studies
Selection BiasEven in systematic reviews/metanalyzes!
Expert – Guidelines recommendations
Large Historic Data bases Potential benefit of PTR
Best Indications for PTR +++
Kianmanesh 2021
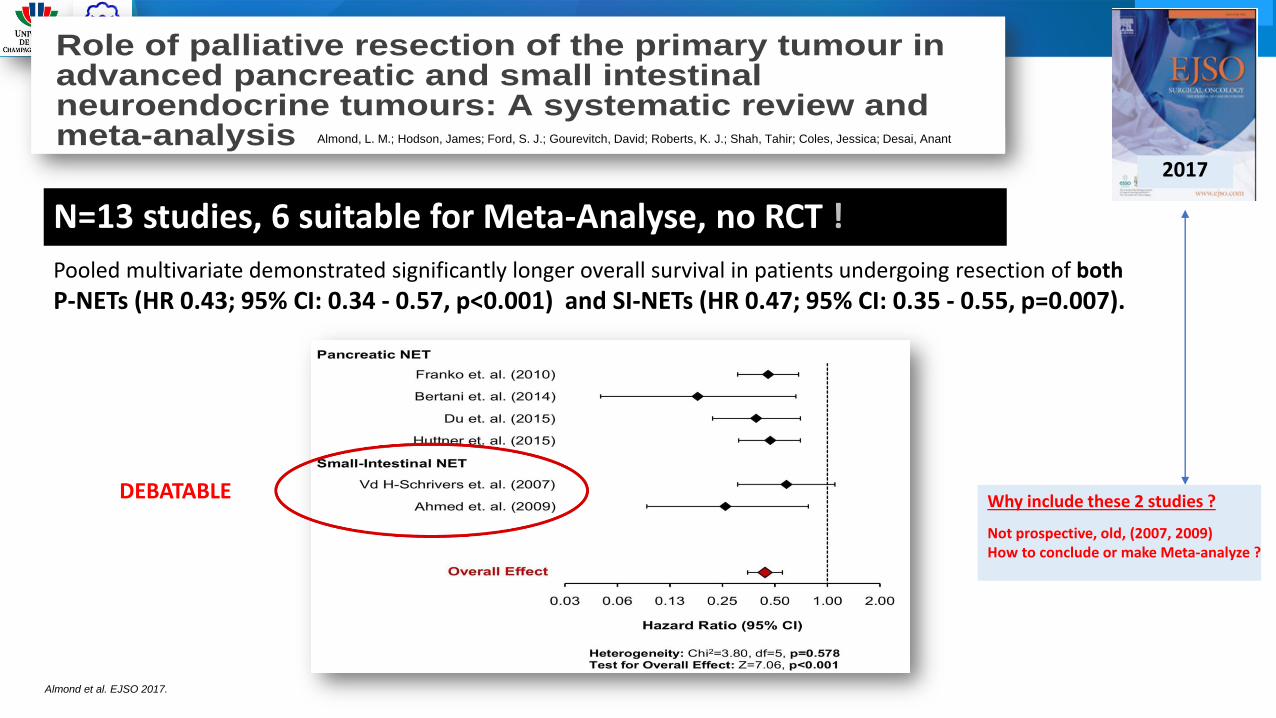
N=13 studies, 6 suitable for Meta-Analyse, no RCT !
Role of palliative resection of the primary tumour inadvanced pancreatic and small intestinalneuroendocrine tumours: A systematic review andmeta-analysisAlmond, L. M.; Hodson, James; Ford, S. J.; Gourevitch, David; Roberts, K. J.; Shah, Tahir;Coles, Jessica; Desai, Anant
DOI:10.1016/j.ejso.2017.05.016
License:Creative Commons: Attribution-NonCommercial-NoDerivs (CC BY-NC-ND)
Document VersionPeer reviewed version
Citation for published version (Harvard):Almond, LM, Hodson, J, Ford, SJ, Gourevitch, D, Roberts, KJ, Shah, T, Isaac, J & Desai, A 2017, 'Role ofpalliative resection of the primary tumour in advanced pancreatic and small intestinal neuroendocrine tumours: Asystematic review and meta-analysis', European Journal of Surgical Oncology (EJSO).https://doi.org/10.1016/j.ejso.2017.05.016
Link to publication on Research at Birmingham portal
General rightsUnless a licence is specified above, all rights (including copyright and moral rights) in this document are retained by the authors and/or thecopyright holders. The express permission of the copyright holder must be obtained for any use of this material other than for purposespermitted by law.
• Users may freely distribute the URL that is used to identify this publication.• Users may download and/or print one copy of the publication from the University of Birmingham research portal for the purpose of privatestudy or non-commercial research.• User may use extracts from the document in line with the concept of ‘fair dealing’ under the Copyright, Designs and Patents Act 1988 (?)• Users may not further distribute the material nor use it for the purposes of commercial gain.
Where a licence is displayed above, please note the terms and conditions of the licence govern your use of this document.
When citing, please reference the published version.
Take down policyWhile the University of Birmingham exercises care and attention in making items available there are rare occasions when an item has beenuploaded in error or has been deemed to be commercially or otherwise sensitive.
If you believe that this is the case for this document, please contact [email protected] providing details and we will remove access tothe work immediately and investigate.
Download date: 01. Feb. 2019
brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by University of Birmingham Research Portal
2017
Almond, L. M.; Hodson, James; Ford, S. J.; Gourevitch, David; Roberts, K. J.; Shah, Tahir; Coles, Jessica; Desai, Anant
Pooled multivariate demonstrated significantly longer overall survival in patients undergoing resection of both
P-NETs (HR 0.43; 95% CI: 0.34 - 0.57, p<0.001) and SI-NETs (HR 0.47; 95% CI: 0.35 - 0.55, p=0.007).
Almond et al. EJSO 2017.
Why include these 2 studies ?
Not prospective, old, (2007, 2009)How to conclude or make Meta-analyze ?
DEBATABLE
Kianmanesh 2021
SiNENs & pNENs are different diseases ?
Kianmanesh 2021
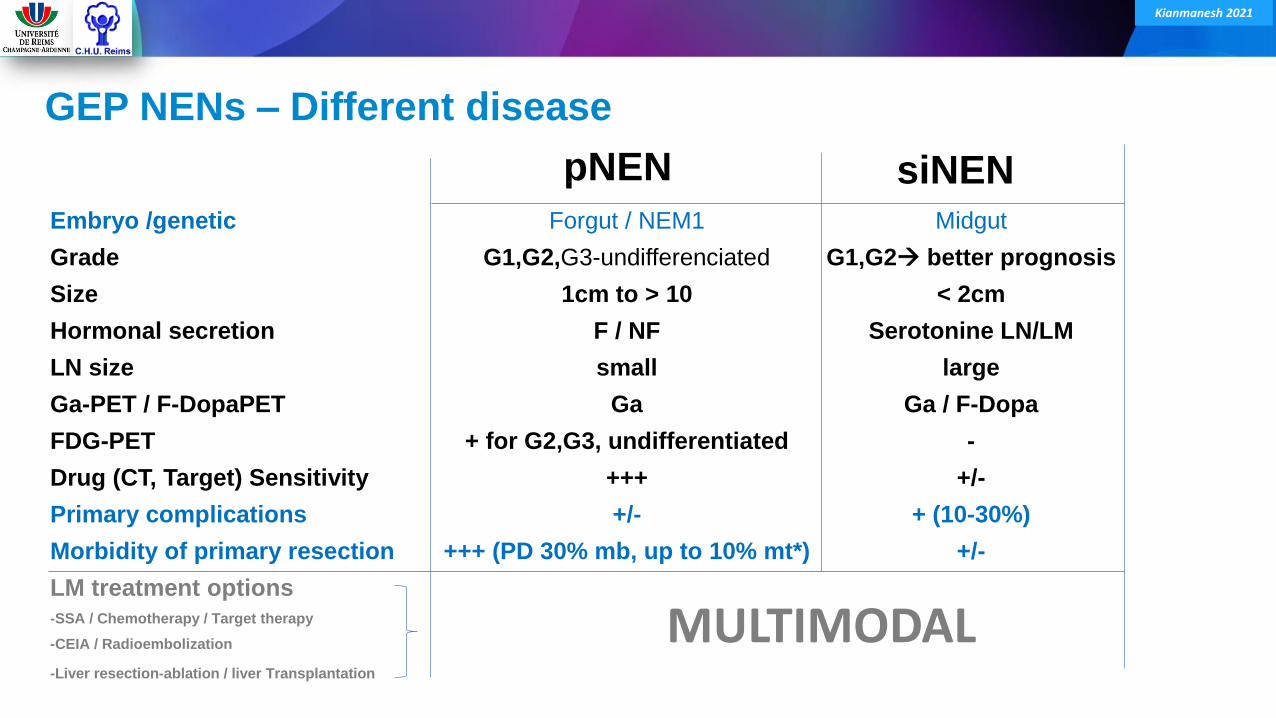
Embryo /genetic Forgut / NEM1 Midgut
Grade G1,G2,G3-undifferenciated G1,G2 better prognosis
Size 1cm to > 10 < 2cm
Hormonal secretion F / NF Serotonine LN/LM
LN size small large
Ga-PET / F-DopaPET Ga Ga / F-Dopa
FDG-PET + for G2,G3, undifferentiated -
Drug (CT, Target) Sensitivity +++ +/-
Primary complications +/- + (10-30%)
Morbidity of primary resection +++ (PD 30% mb, up to 10% mt*) +/-
LM treatment options-SSA / Chemotherapy / Target therapy
-CEIA / Radioembolization
-Liver resection-ablation / liver Transplantation
GEP NENs – Different disease
pNEN siNEN
MULTIMODAL
Kianmanesh 2021
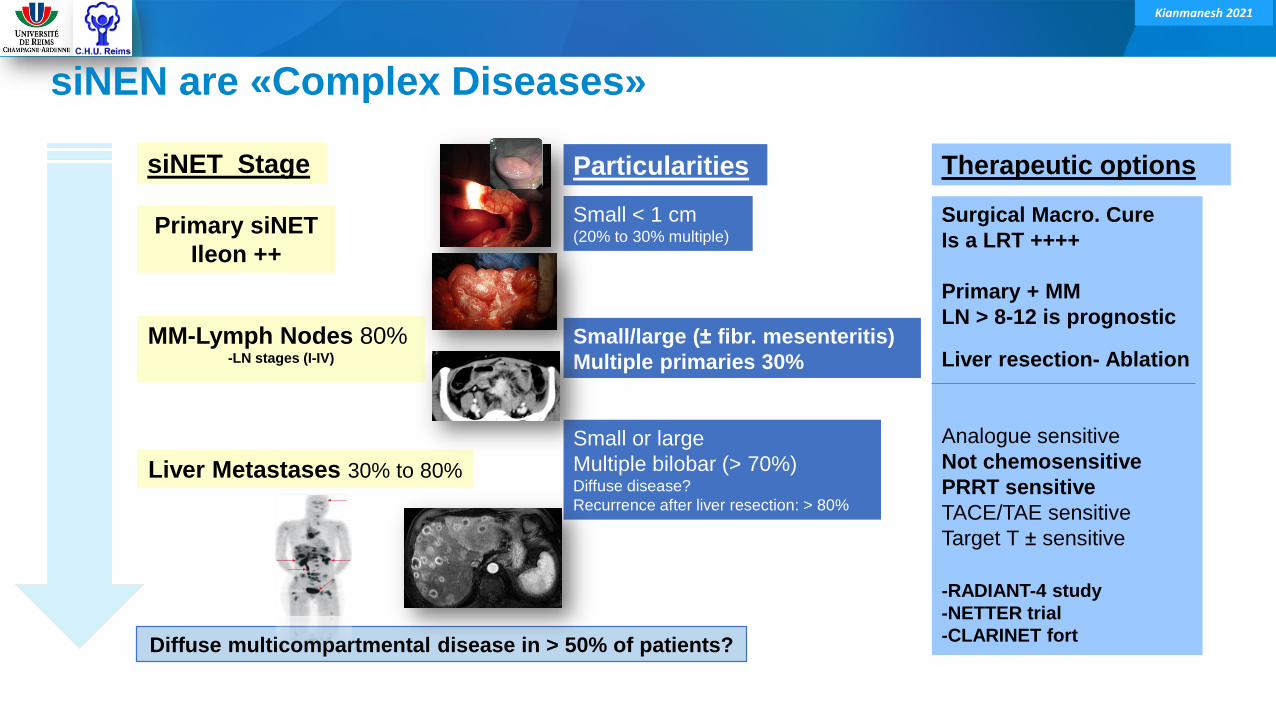
siNEN are «Complex Diseases»
Primary siNET
Ileon ++
MM-Lymph Nodes 80% -LN stages (I-IV)
Liver Metastases 30% to 80%
Small < 1 cm(20% to 30% multiple)
Small/large (± fibr. mesenteritis)
Multiple primaries 30%
Small or large
Multiple bilobar (> 70%)Diffuse disease?
Recurrence after liver resection: > 80%
Diffuse multicompartmental disease in > 50% of patients?
Surgical Macro. Cure
Is a LRT ++++
Primary + MM
LN > 8-12 is prognostic
Liver resection- Ablation
Analogue sensitive
Not chemosensitive
PRRT sensitive
TACE/TAE sensitive
Target T ± sensitive
-RADIANT-4 study
-NETTER trial
-CLARINET fort
siNET Stage Particularities Therapeutic options
Kianmanesh 2021
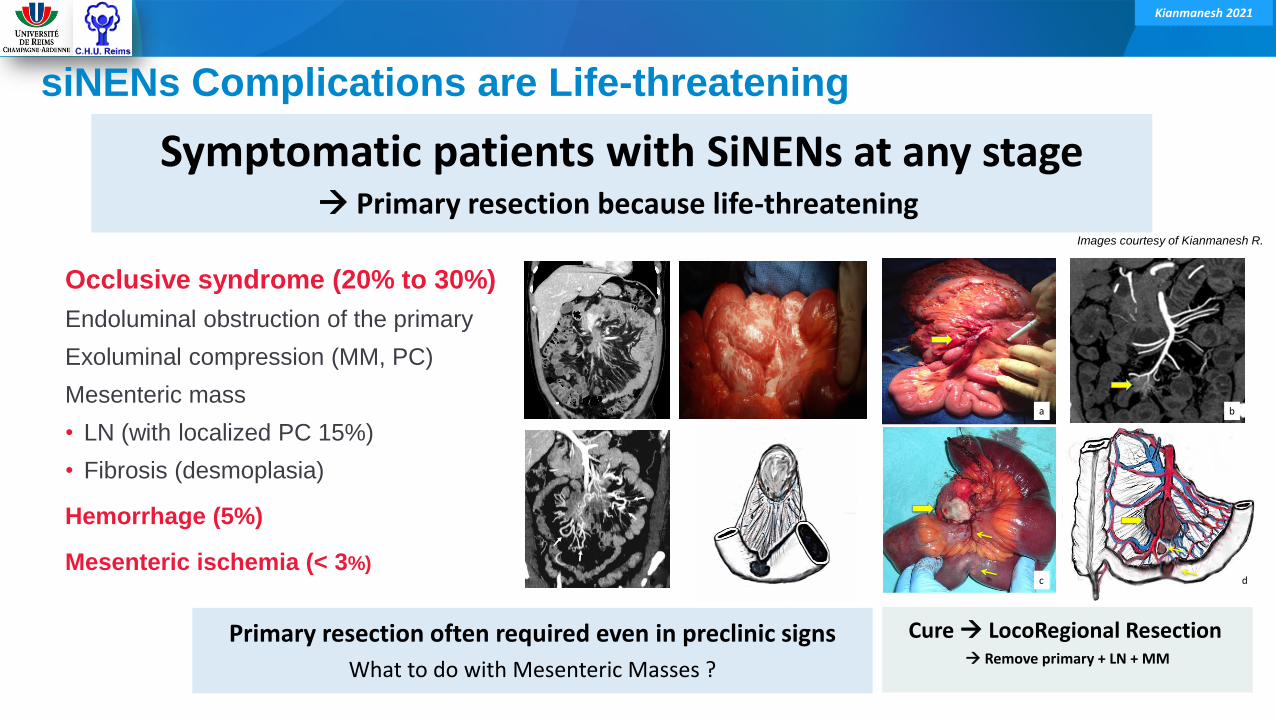
siNENs Complications are Life-threatening
Occlusive syndrome (20% to 30%)
Endoluminal obstruction of the primary
Exoluminal compression (MM, PC)
Mesenteric mass
• LN (with localized PC 15%)
• Fibrosis (desmoplasia)
Hemorrhage (5%)
Mesenteric ischemia (< 3%)
Images courtesy of Kianmanesh R.
a b
c d
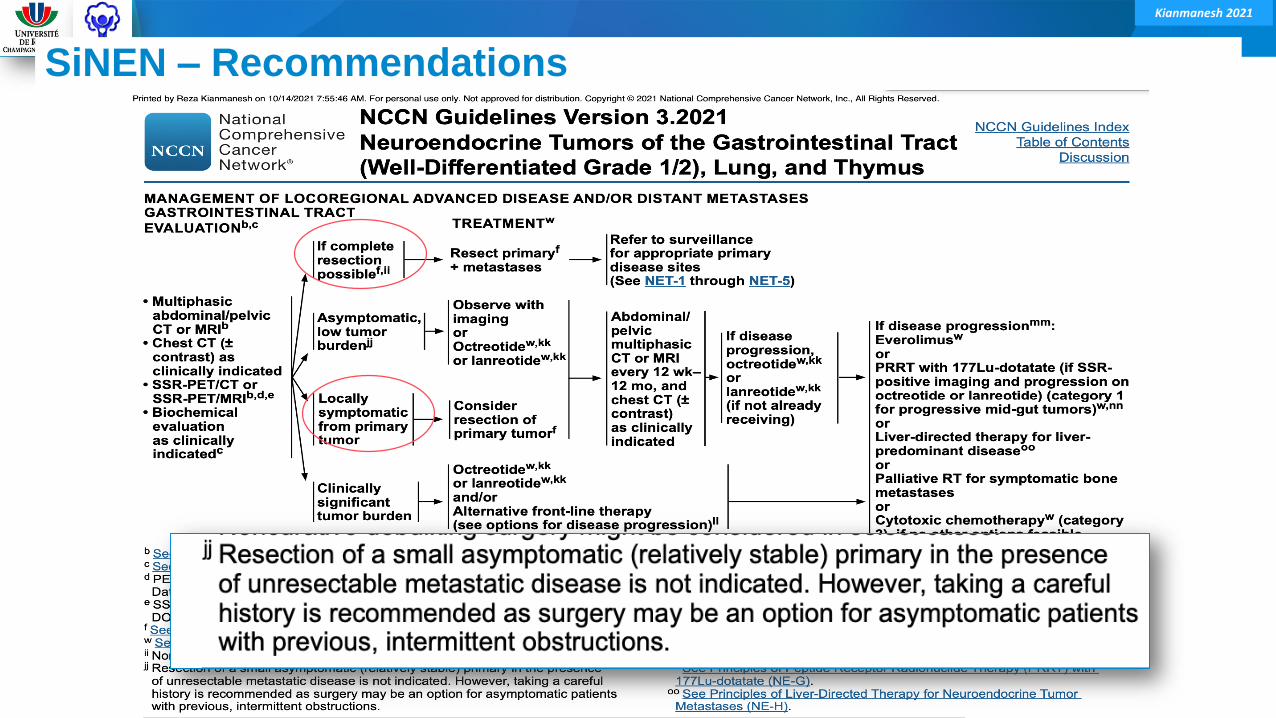
Symptomatic patients with SiNENs at any stage Primary resection because life-threatening
Primary resection often required even in preclinic signs
What to do with Mesenteric Masses ?
Cure LocoRegional Resection Remove primary + LN + MM
Kianmanesh 2021
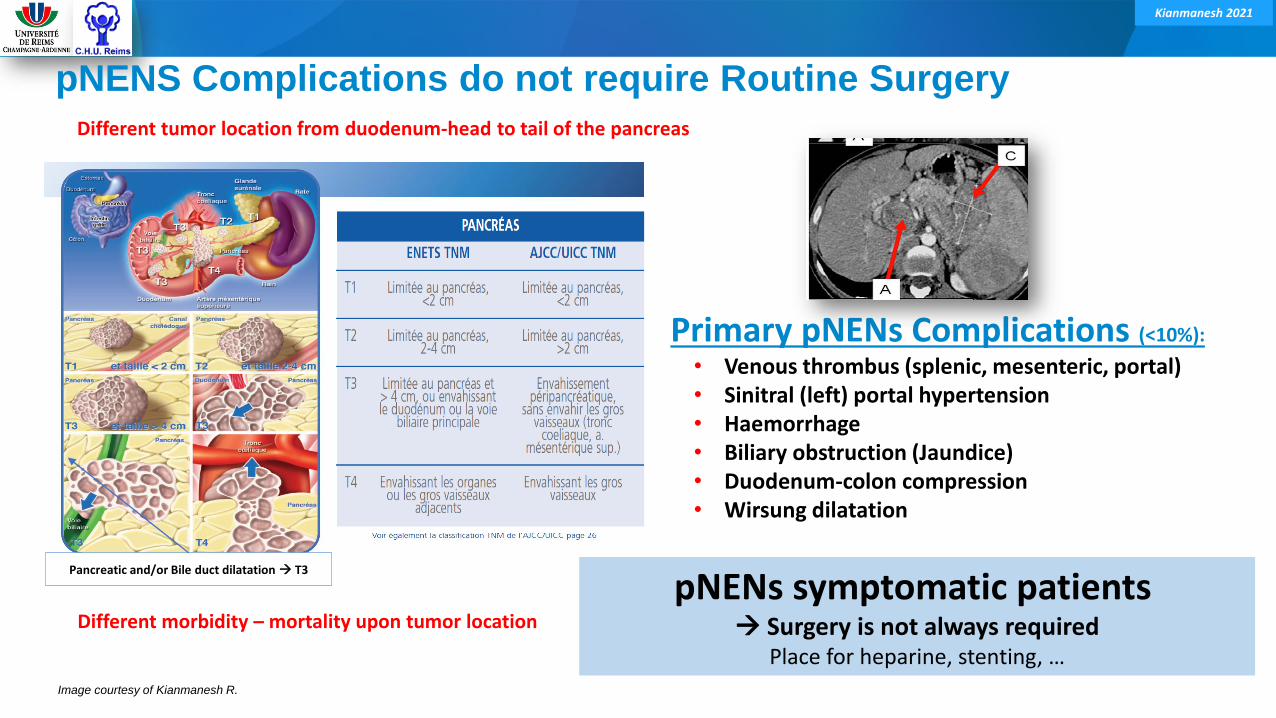
Pancreatic and/or Bile duct dilatation T3
pNENS Complications do not require Routine Surgery
Primary pNENs Complications (<10%):
• Venous thrombus (splenic, mesenteric, portal)• Sinitral (left) portal hypertension• Haemorrhage• Biliary obstruction (Jaundice)• Duodenum-colon compression• Wirsung dilatation
pNENs symptomatic patients Surgery is not always required
Place for heparine, stenting, …
Different tumor location from duodenum-head to tail of the pancreas
Different morbidity – mortality upon tumor location
Image courtesy of Kianmanesh R.
Kianmanesh 2021
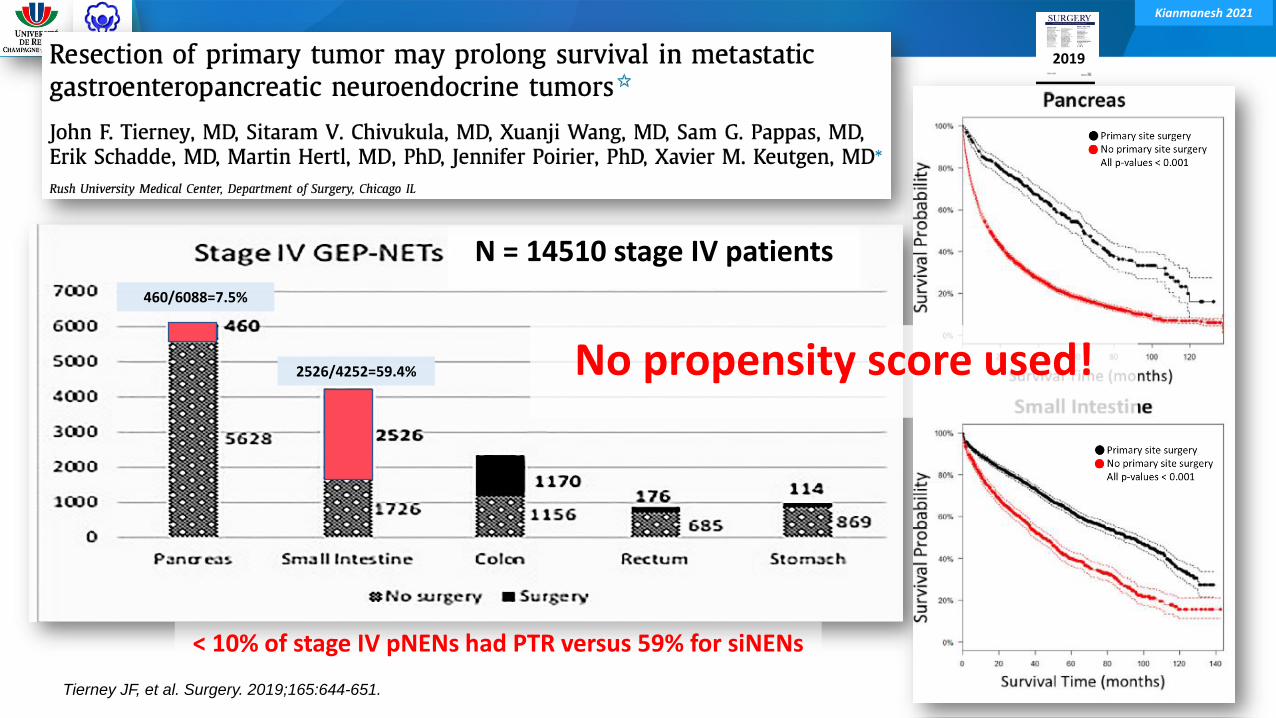
Tierney JF, et al. Surgery. 2019;165:644-651.
N = 14510 stage IV patients
2019
460/6088=7.5%
2526/4252=59.4%
< 10% of stage IV pNENs had PTR versus 59% for siNENs
No propensity score used!
Kianmanesh 2021
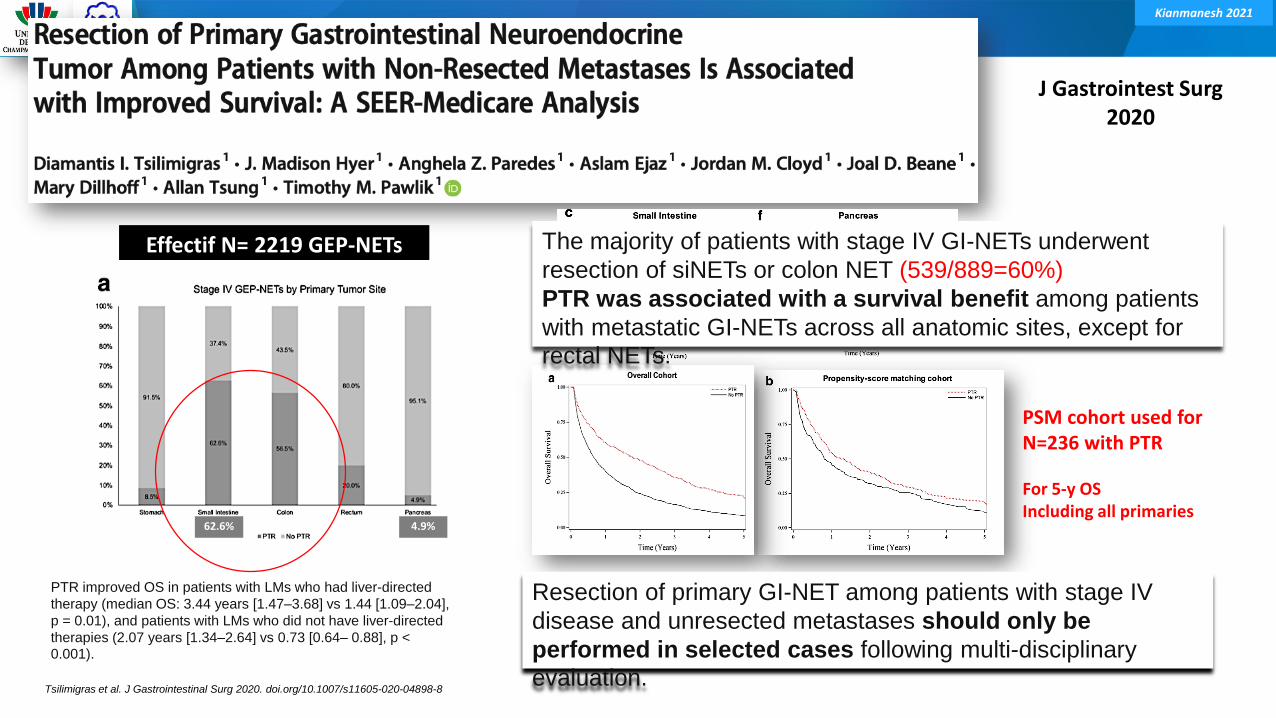
Tsilimigras et al. J Gastrointestinal Surg 2020. doi.org/10.1007/s11605-020-04898-8
J Gastrointest Surg2020
Effectif N= 2219 GEP-NETs
4.9%62.6%
Resection of primary GI-NET among patients with stage IV
disease and unresected metastases should only be
performed in selected cases following multi-disciplinary
evaluation.
PSM cohort used forN=236 with PTR
For 5-y OSIncluding all primaries
The majority of patients with stage IV GI-NETs underwent
resection of siNETs or colon NET (539/889=60%)
PTR was associated with a survival benefit among patients
with metastatic GI-NETs across all anatomic sites, except for
rectal NETs.
PTR improved OS in patients with LMs who had liver-directed
therapy (median OS: 3.44 years [1.47–3.68] vs 1.44 [1.09–2.04],
p = 0.01), and patients with LMs who did not have liver-directed
therapies (2.07 years [1.34–2.64] vs 0.73 [0.64– 0.88], p < 0.001).
Kianmanesh 2021
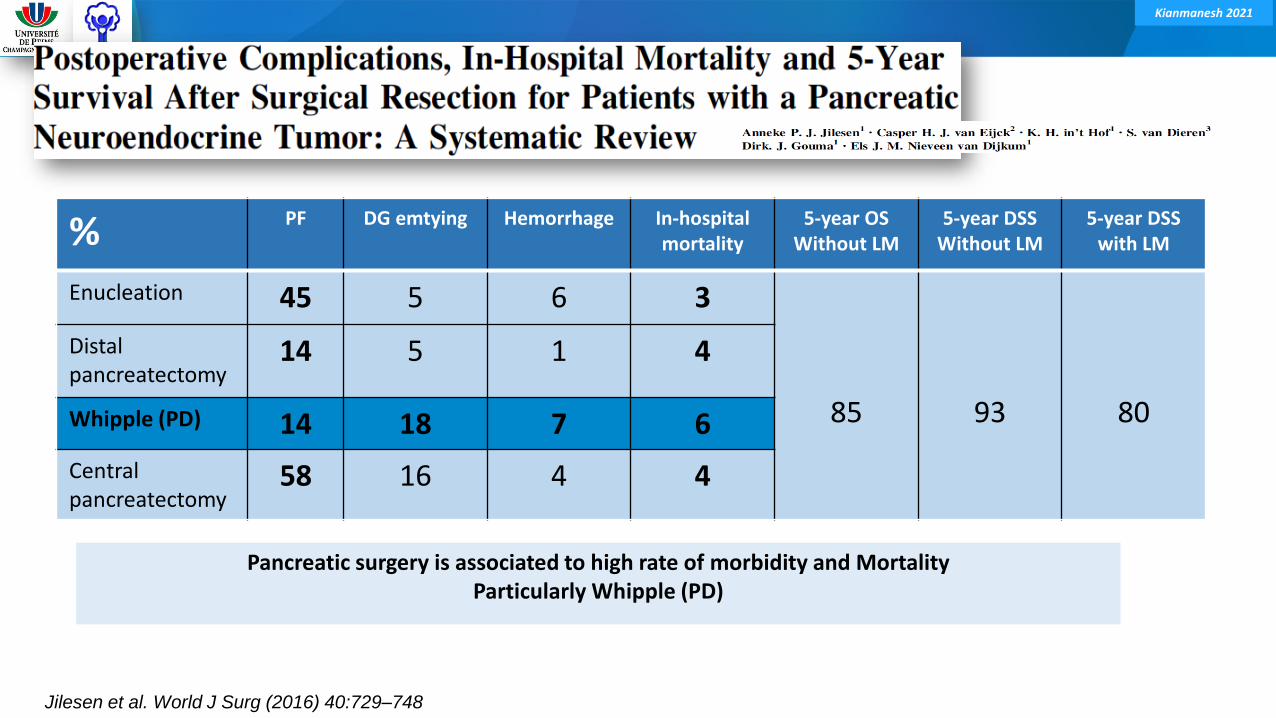
Complications of primary resection pNENs from siNENs
Kianmanesh 2021
% PF DG emtying Hemorrhage In-hospitalmortality
5-year OSWithout LM
5-year DSSWithout LM
5-year DSS with LM
Enucleation 45 5 6 3
85 93 80
Distal pancreatectomy
14 5 1 4
Whipple (PD) 14 18 7 6
Centralpancreatectomy
58 16 4 4
Jilesen et al. World J Surg (2016) 40:729–748
Pancreatic surgery is associated to high rate of morbidity and MortalityParticularly Whipple (PD)
Kianmanesh 2021
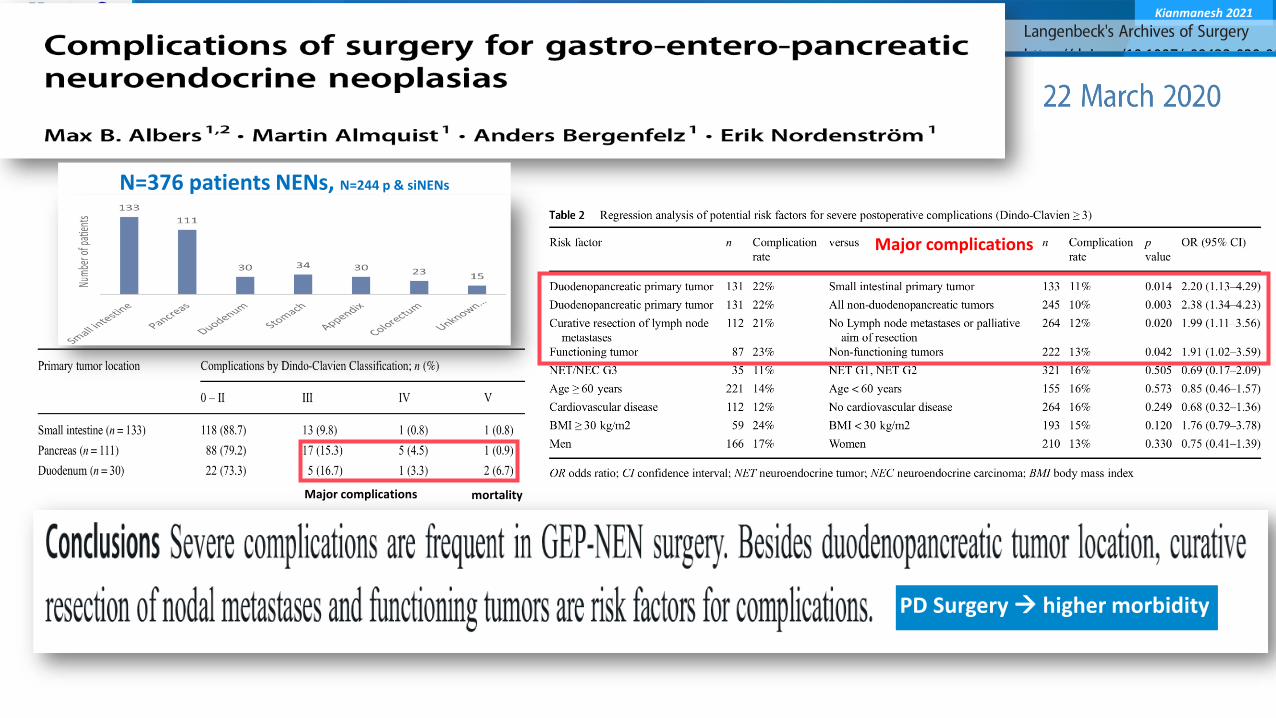
PD Surgery higher morbidity
mortalityMajor complications
N=376 patients NENs, N=244 p & siNENs
Major complications
Kianmanesh 2021
Stage IV – Resectable or unresectable LMs ?
Kianmanesh 2021
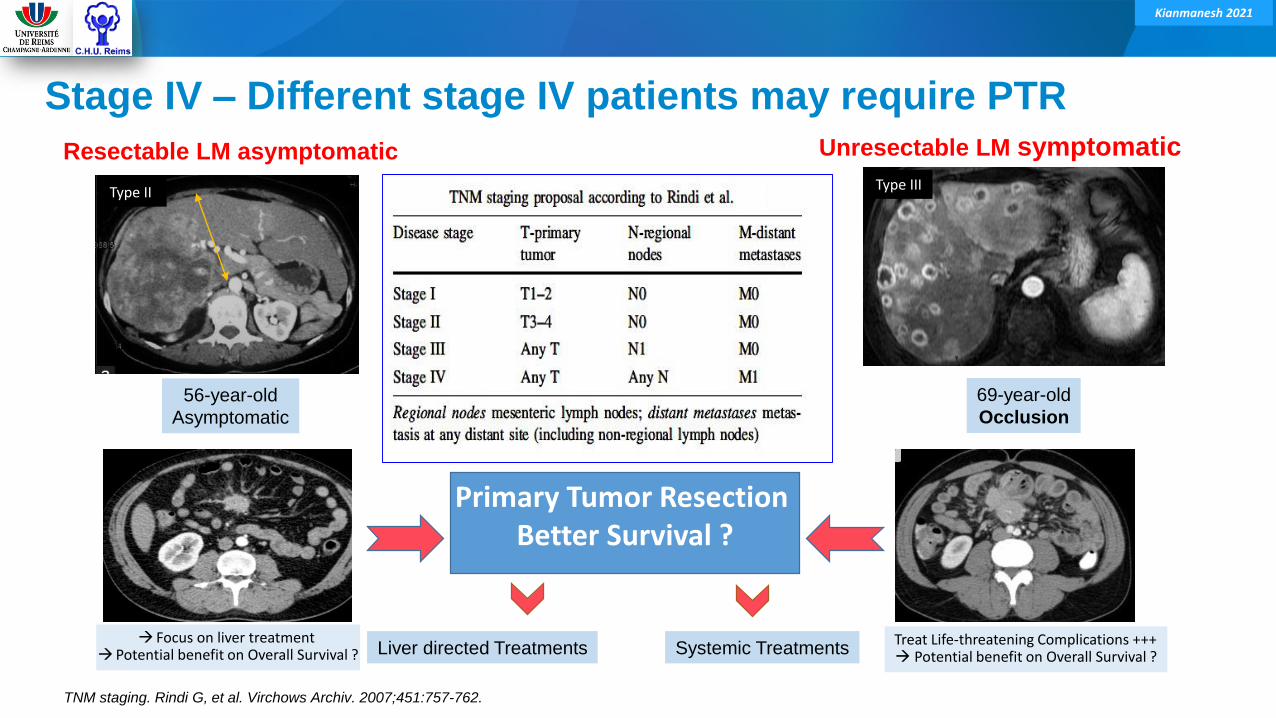
Stage IV – Different stage IV patients may require PTR
56-year-old
Asymptomatic
Resectable LM asymptomatic
TNM staging. Rindi G, et al. Virchows Archiv. 2007;451:757-762.
Focus on liver treatment Potential benefit on Overall Survival ?
Primary Tumor ResectionBetter Survival ?
Liver directed Treatments Systemic Treatments
Type II
69-year-old
Occlusion
Unresectable LM symptomatic
Treat Life-threatening Complications +++ Potential benefit on Overall Survival ?
Type III

Kianmanesh 2021
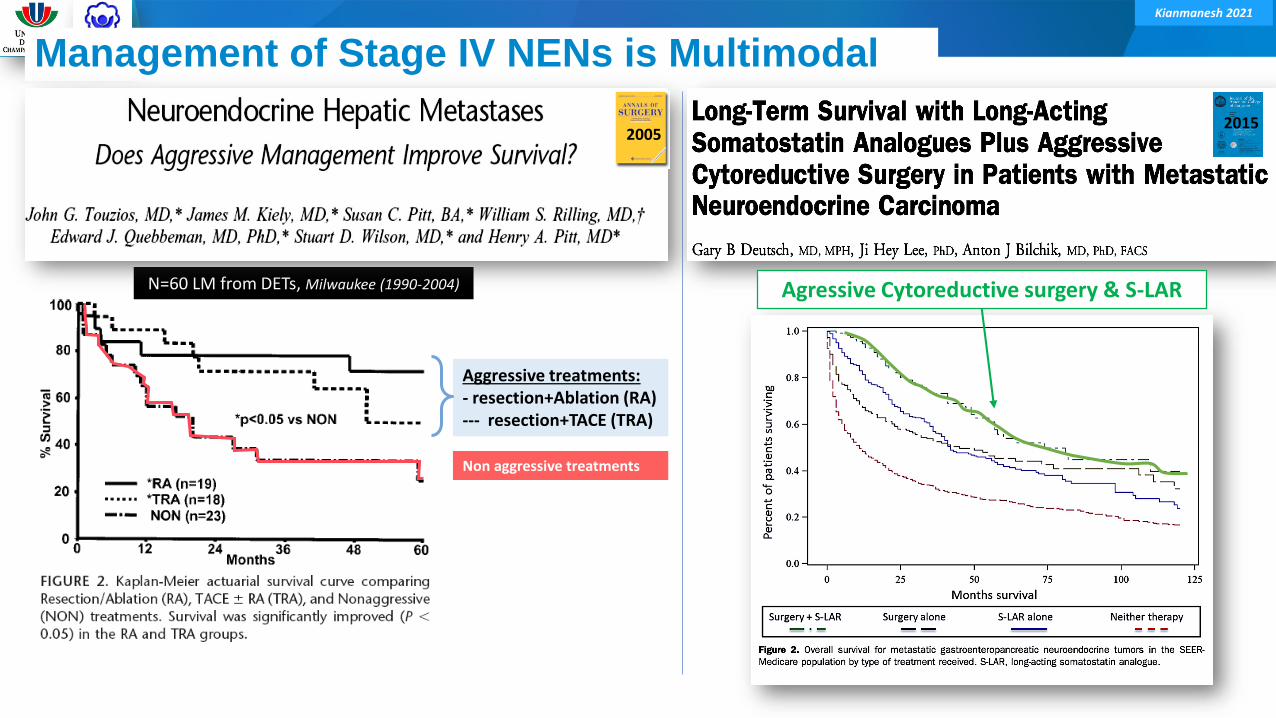
Agressive management of LMs,
Assicated S-Analogues & PRRT ?
Kianmanesh 2021
Aggressive treatments:- resection+Ablation (RA)--- resection+TACE (TRA)
Non aggressive treatments
2005
Management of Stage IV NENs is Multimodal
N=60 LM from DETs, Milwaukee (1990-2004)
2005
Agressive Cytoreductive surgery & S-LAR
2015
Kianmanesh 2021
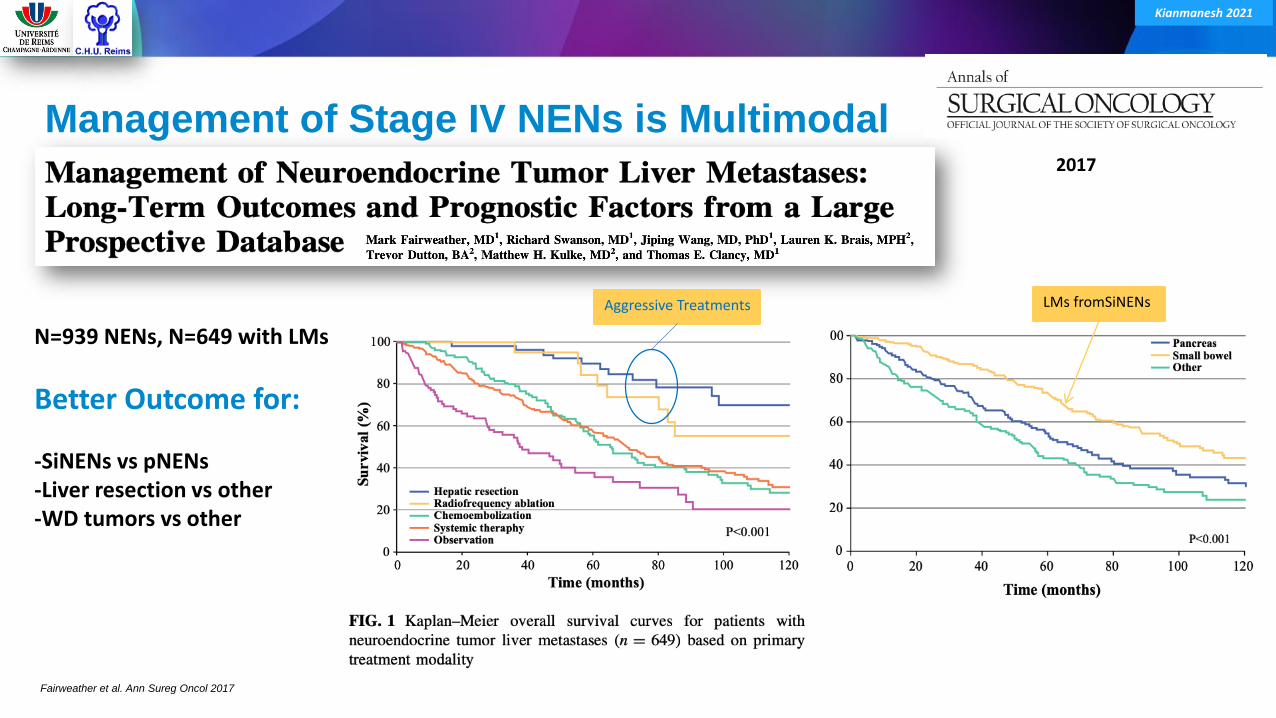
Management of Stage IV NENs is Multimodal
Fairweather et al. Ann Sureg Oncol 2017
N=939 NENs, N=649 with LMs
Better Outcome for:
-SiNENs vs pNENs-Liver resection vs other-WD tumors vs other
2017
Aggressive Treatments LMs fromSiNENs
Kianmanesh 2021
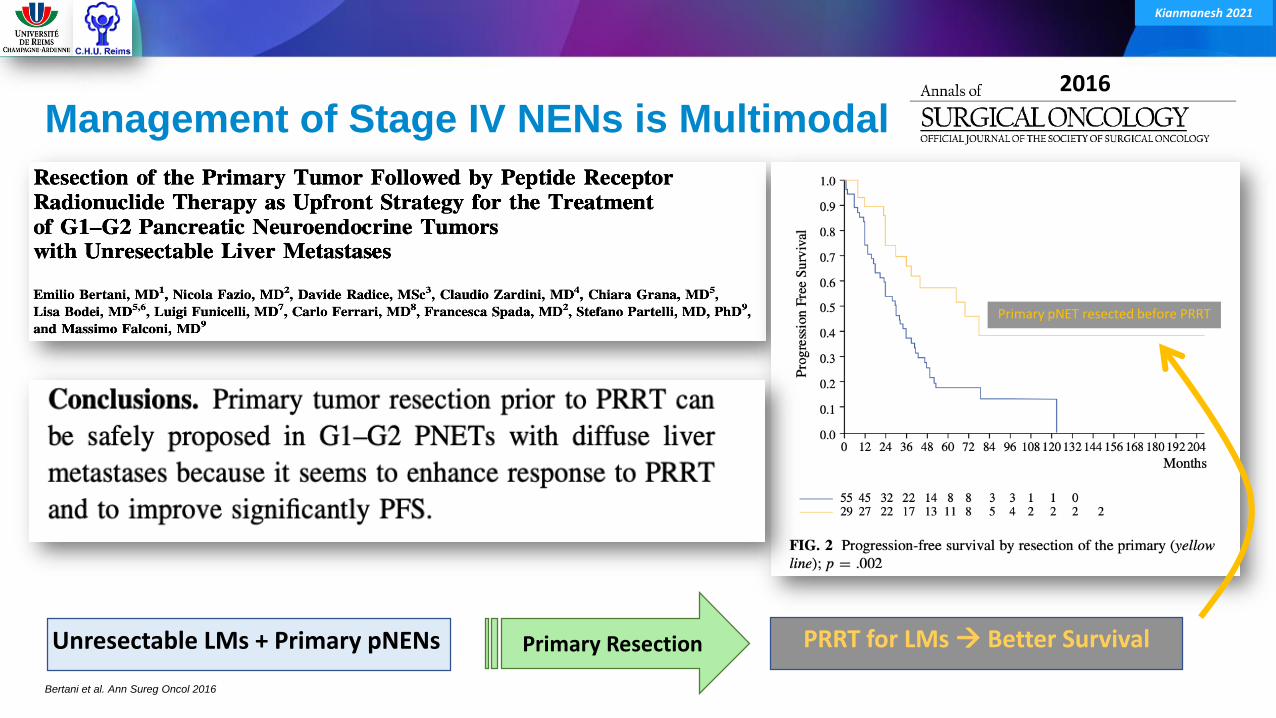
Management of Stage IV NENs is Multimodal
Bertani et al. Ann Sureg Oncol 2016
Unresectable LMs + Primary pNENs Primary Resection
2016
Primary pNET resected before PRRT
PRRT for LMs Better Survival
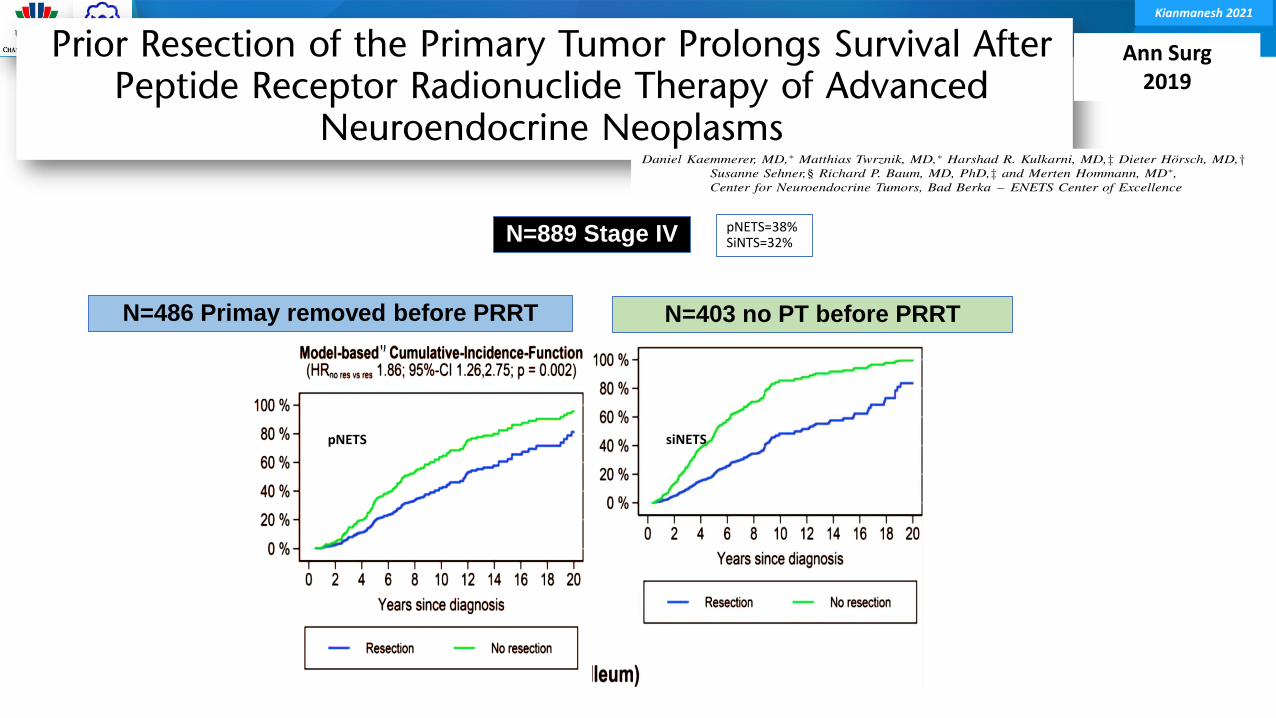
Kianmanesh 2021
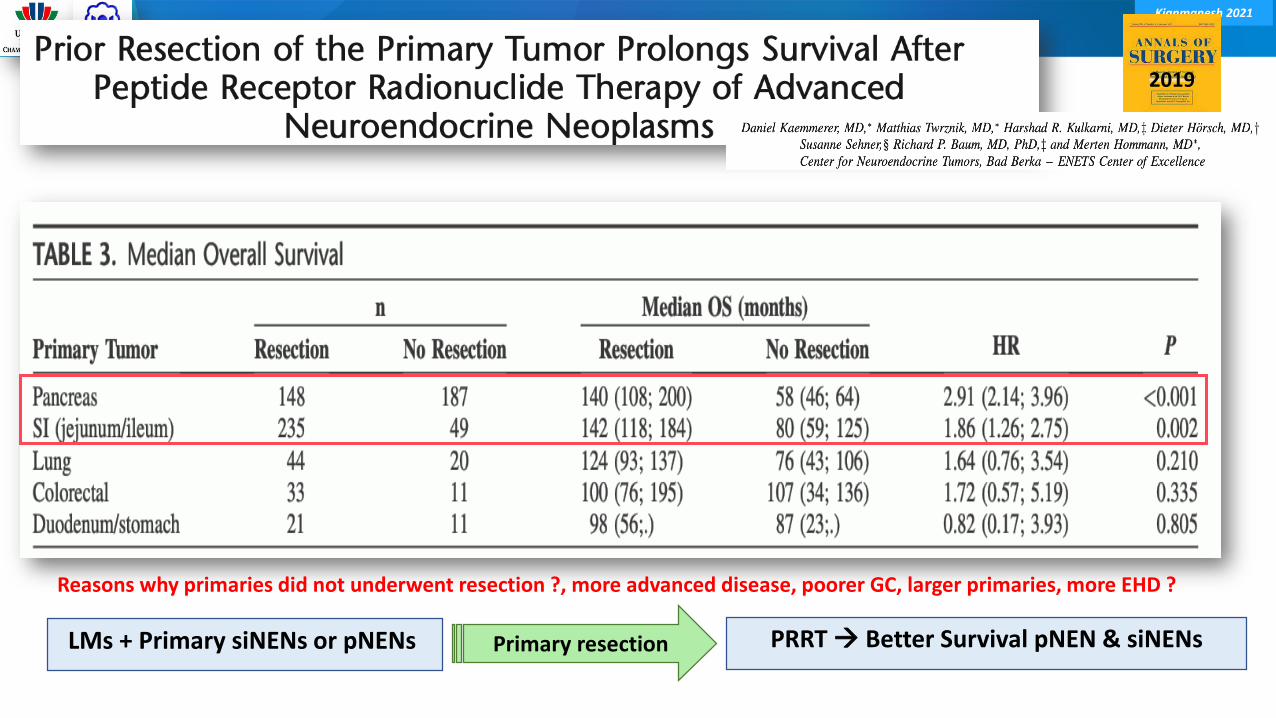
N=889 Stage IV
Ann Surg2019
N=403 no PT before PRRTN=486 Primay removed before PRRT
pNETS=38%SiNTS=32%
pNETS siNETS
Kianmanesh 2021
2019
LMs + Primary siNENs or pNENs Primary resection PRRT Better Survival pNEN & siNENs
Reasons why primaries did not underwent resection ?, more advanced disease, poorer GC, larger primaries, more EHD ?
Kianmanesh 2021
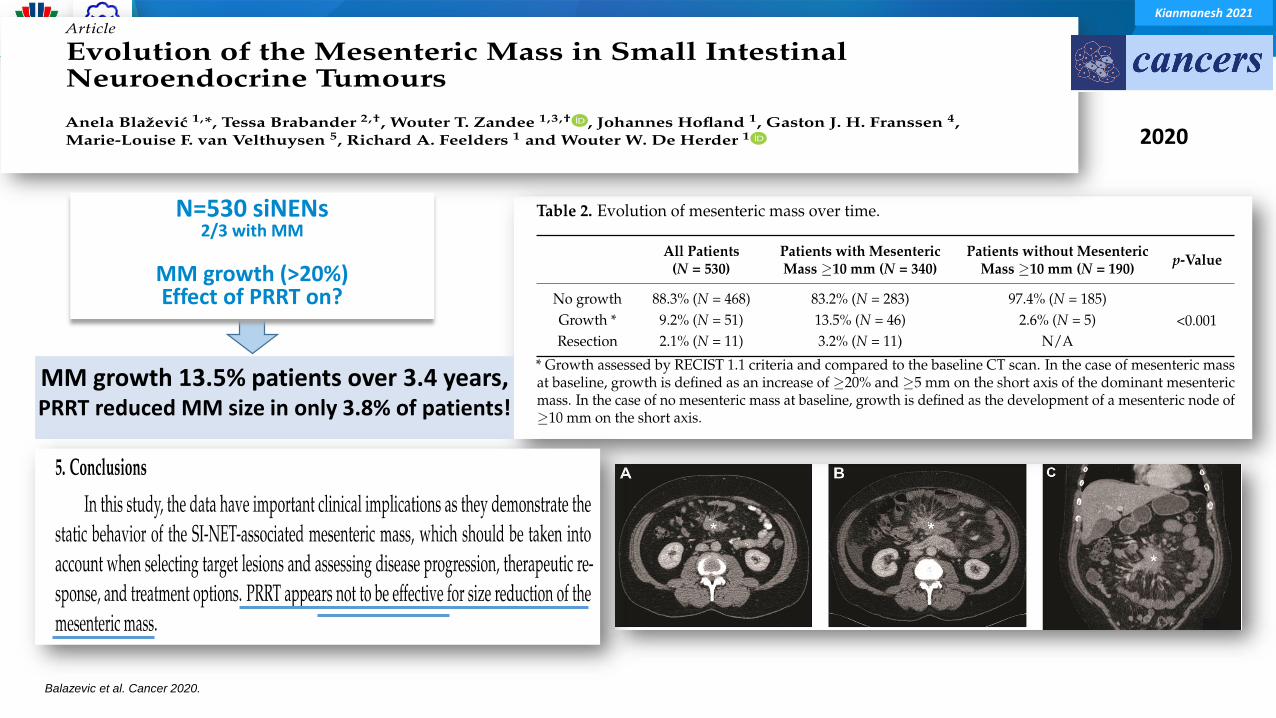
Balazevic et al. Cancer 2020.
MM growth 13.5% patients over 3.4 years,PRRT reduced MM size in only 3.8% of patients!
2020
N=530 siNENs2/3 with MM
MM growth (>20%)Effect of PRRT on?
Kianmanesh 2021
Stage IV with extrahepatic disease (EHD)

Kianmanesh 2021
International Journal of Surgery2015
2 main prognostic factors:-Tumor burden-ExtraH disease
Bertani et al. International Journal of Surg 2015.
PTR of siNENs with LMs is less effective in patients with extahepatic disease
--- LMs & Extahepatic
Kianmanesh 2021
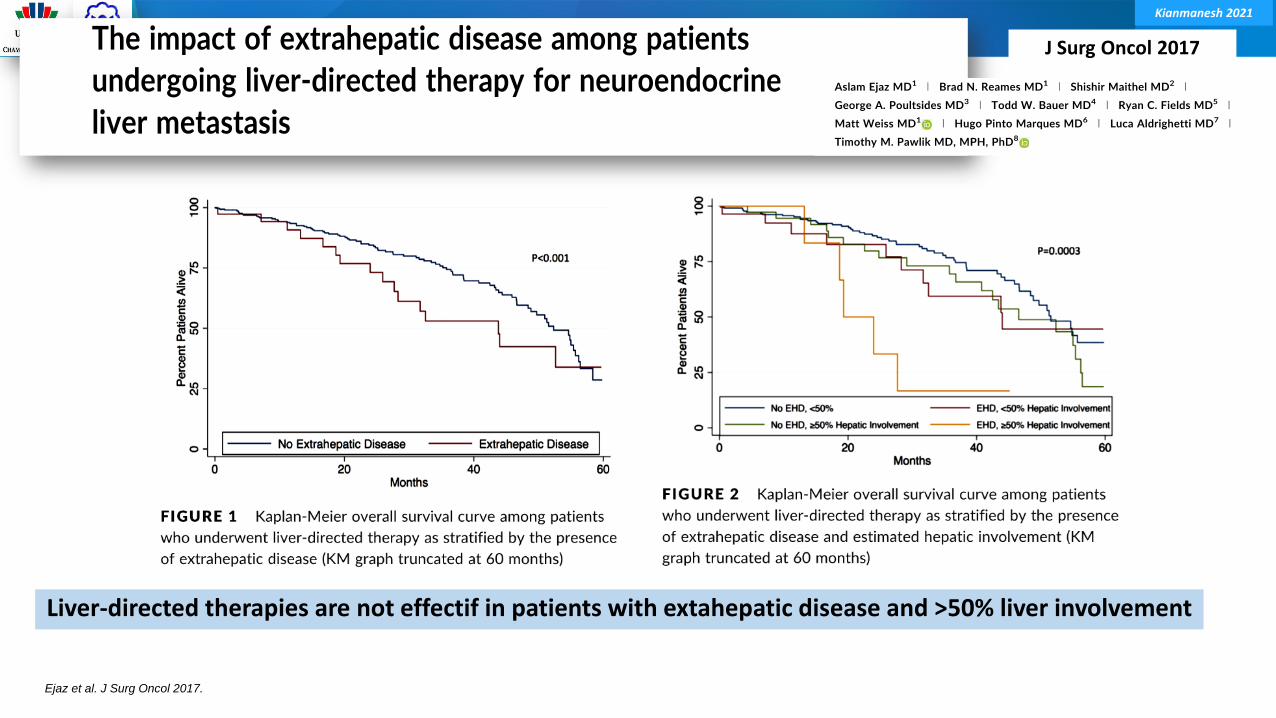
Ejaz et al. J Surg Oncol 2017.
J Surg Oncol 2017
Liver-directed therapies are not effectif in patients with extahepatic disease and >50% liver involvement
Kianmanesh 2021
Actual controversies – Recommendations
Scientific data
Kianmanesh 2021
SiNEN – Recommendations
Kianmanesh 2021
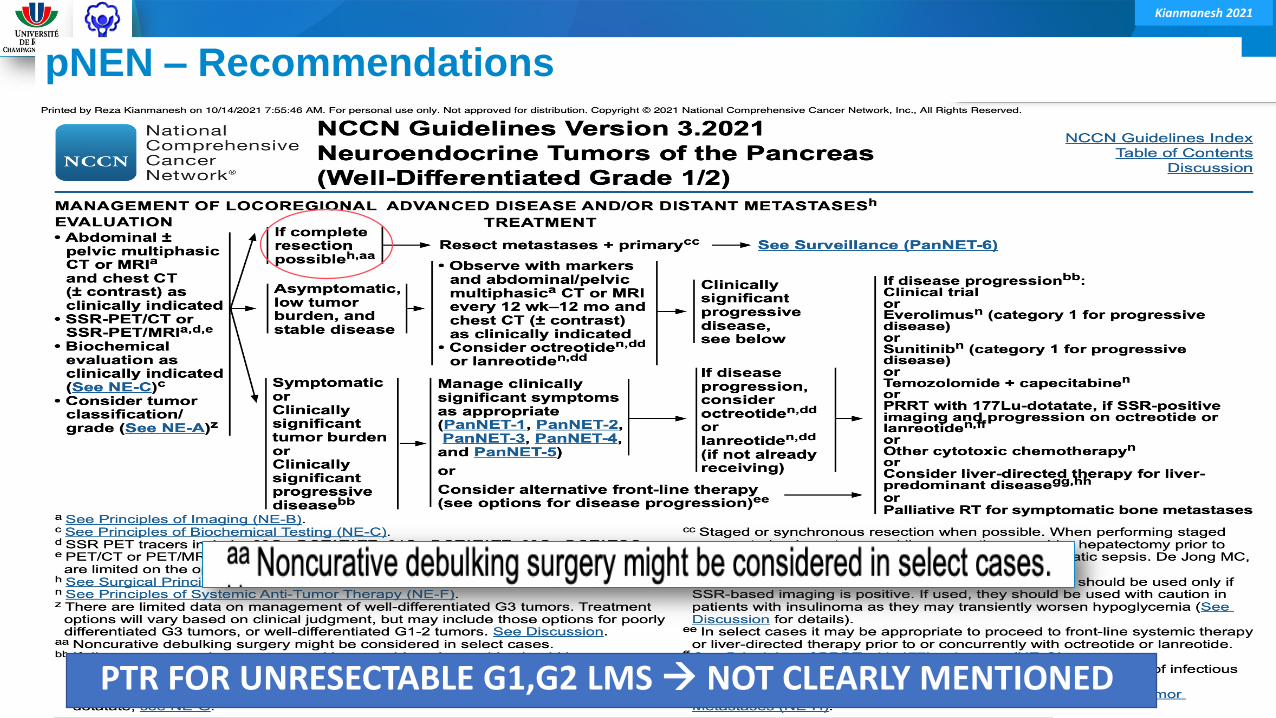
pNEN – Recommendations
PTR FOR UNRESECTABLE G1,G2 LMS NOT CLEARLY MENTIONED
Kianmanesh 2021
Recent Reviews and Larges Series
Kianmanesh 2021
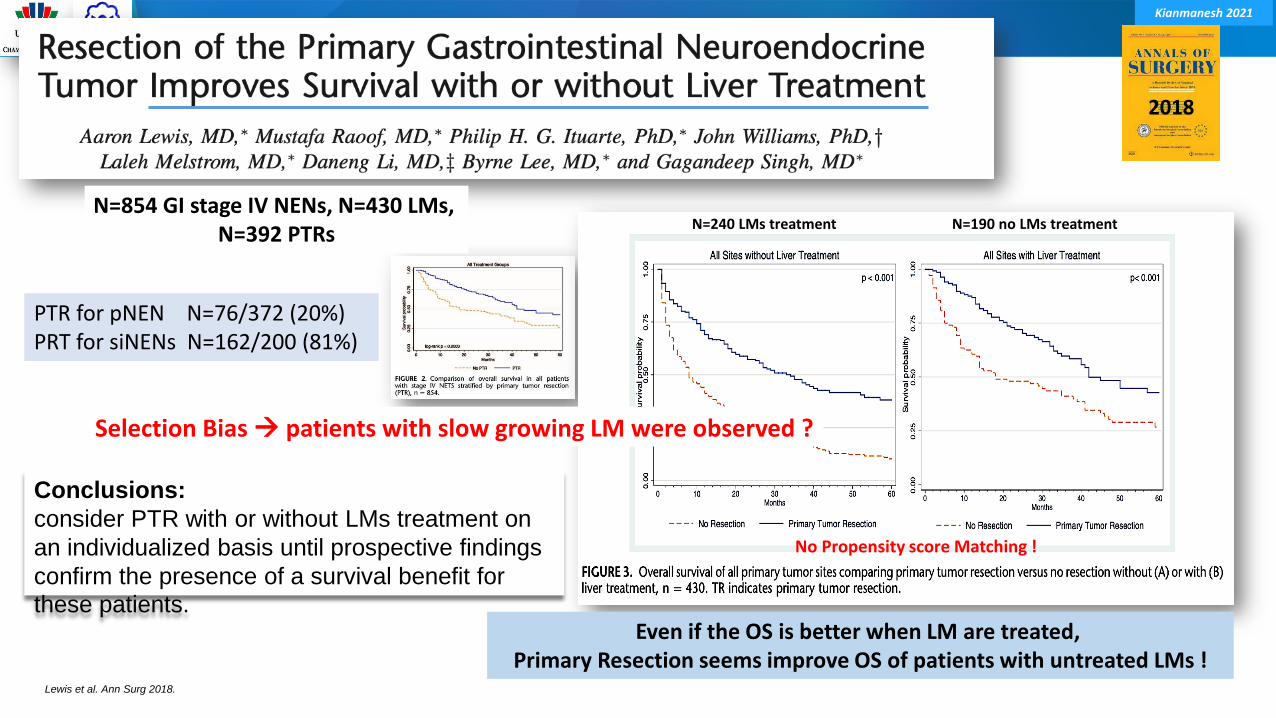
Lewis et al. Ann Surg 2018.
2018
Even if the OS is better when LM are treated, Primary Resection seems improve OS of patients with untreated LMs !
N=854 GI stage IV NENs, N=430 LMs, N=392 PTRs
N=240 LMs treatment N=190 no LMs treatment
PTR for pNEN N=76/372 (20%)PRT for siNENs N=162/200 (81%)
No Propensity score Matching !
Conclusions:
consider PTR with or without LMs treatment on
an individualized basis until prospective findings
confirm the presence of a survival benefit for
these patients.
Selection Bias patients with slow growing LM were observed ?
Kianmanesh 2021
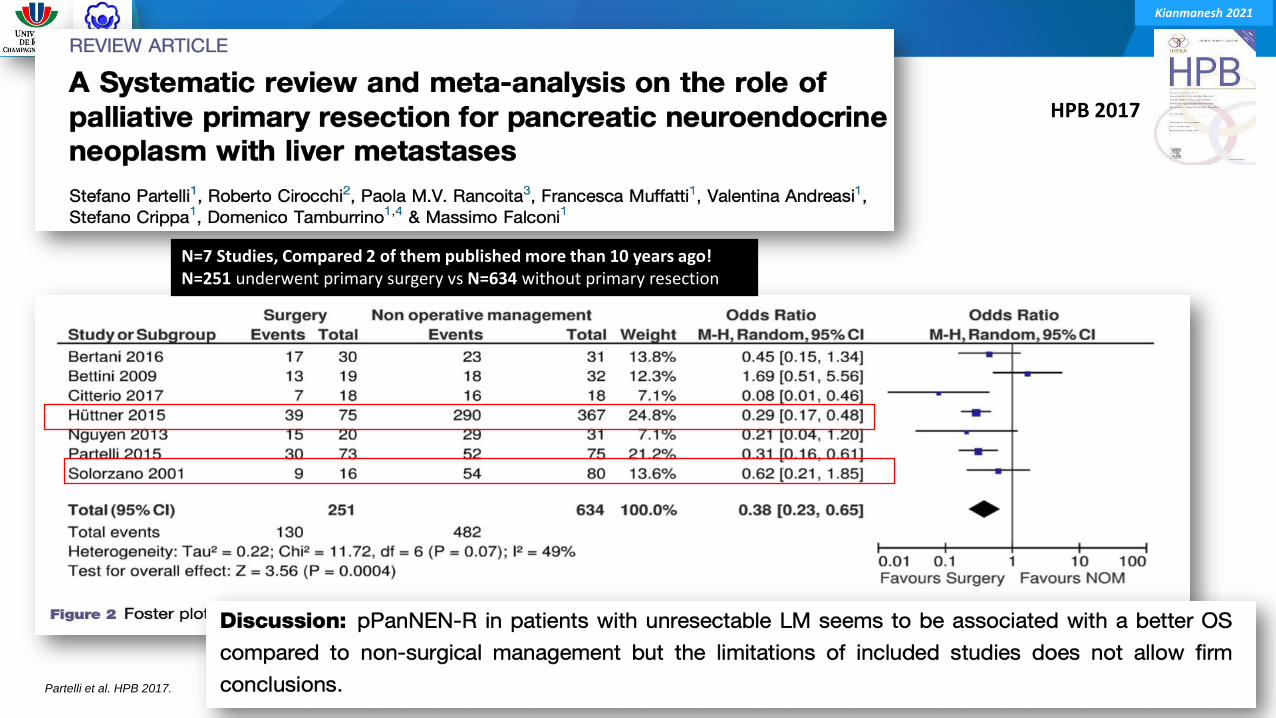
Partelli et al. HPB 2017.
HPB 2017
N=7 Studies, Compared 2 of them published more than 10 years ago!N=251 underwent primary surgery vs N=634 without primary resection
Kianmanesh 2021
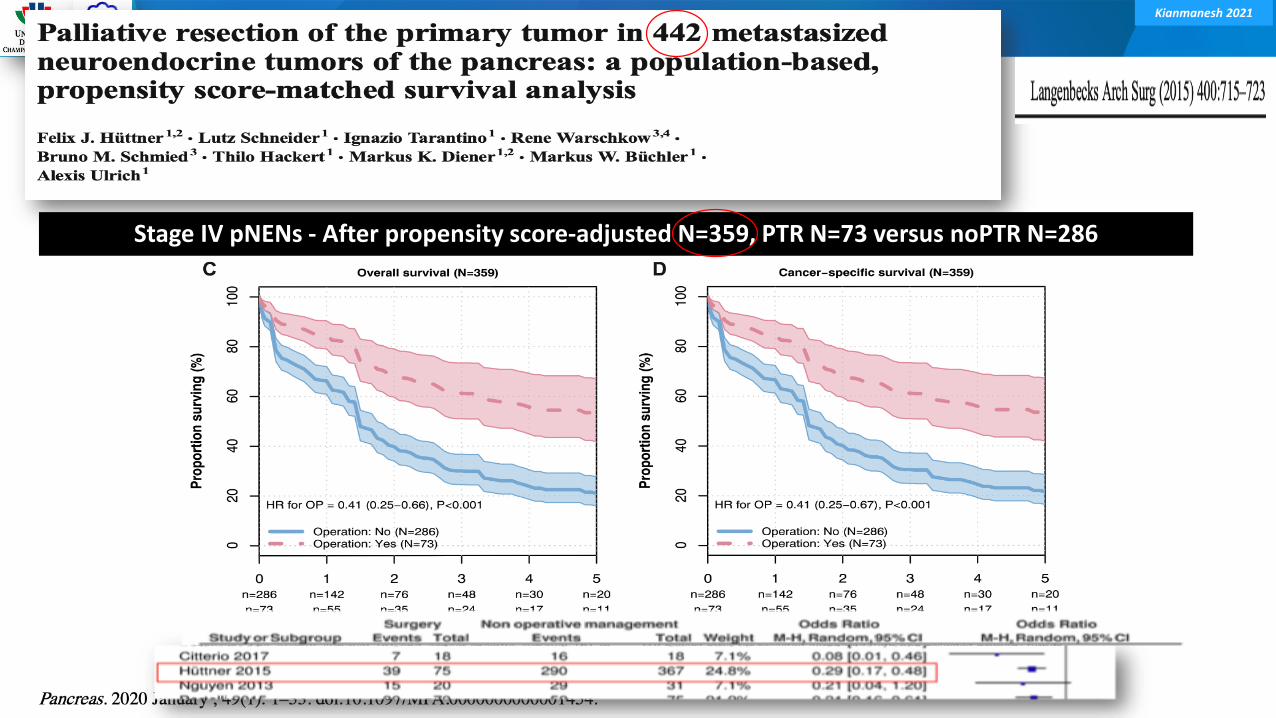
Stage IV pNENs - After propensity score-adjusted N=359, PTR N=73 versus noPTR N=286
Kianmanesh 2021
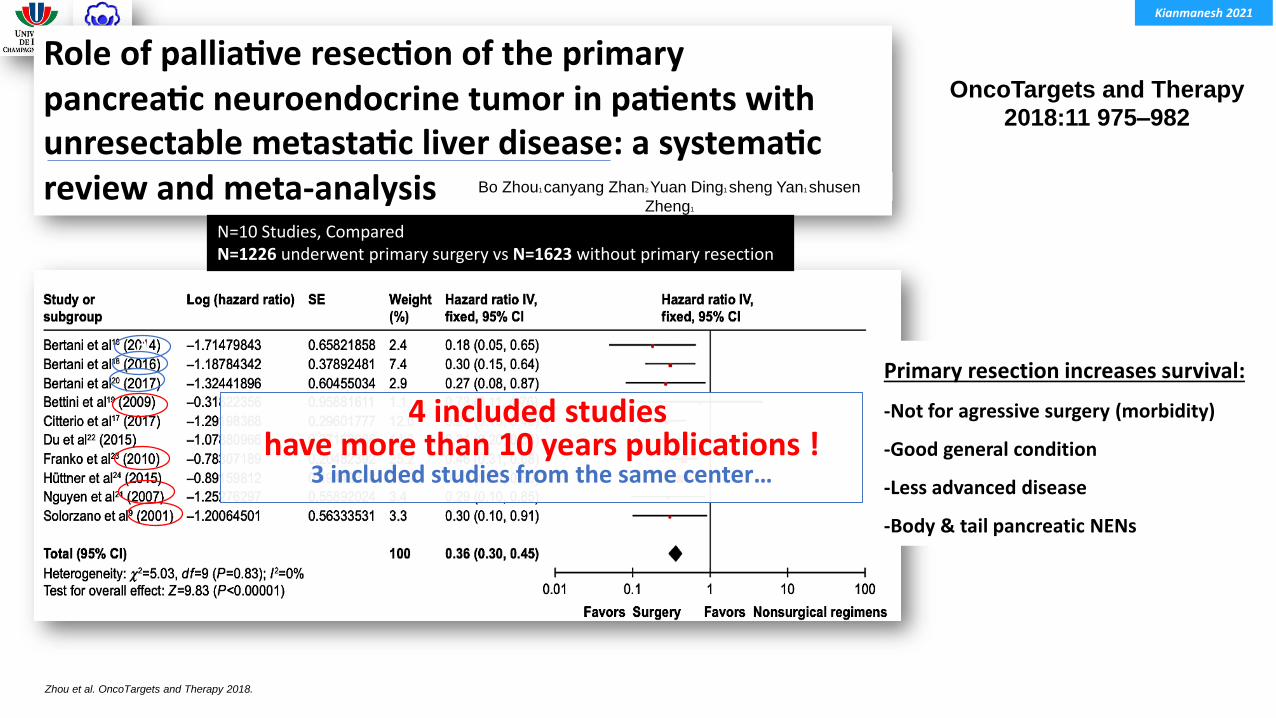
Zhou et al. OncoTargets and Therapy 2018.
OncoTargets and Therapy
2018:11 975–982
Primary resection increases survival:
-Not for agressive surgery (morbidity)
-Good general condition
-Less advanced disease
-Body & tail pancreatic NENs
N=10 Studies, ComparedN=1226 underwent primary surgery vs N=1623 without primary resection
Bo Zhou1 canyang Zhan2 Yuan Ding1 sheng Yan1 shusen
Zheng1
4 included studies have more than 10 years publications !
3 included studies from the same center…
∂
Kianmanesh 2021
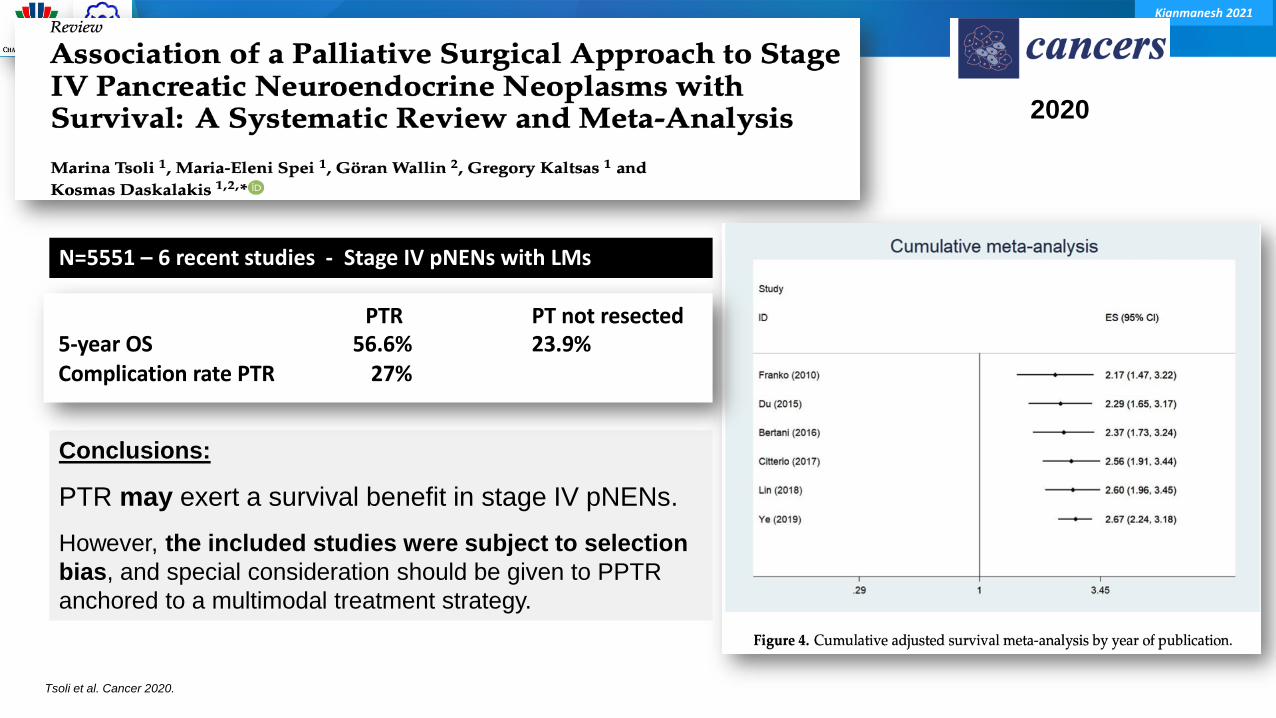
Tsoli et al. Cancer 2020.
2020
Conclusions:
PTR may exert a survival benefit in stage IV pNENs.
However, the included studies were subject to selection
bias, and special consideration should be given to PPTR
anchored to a multimodal treatment strategy.
N=5551 – 6 recent studies - Stage IV pNENs with LMs
PTR PT not resected5-year OS 56.6% 23.9%Complication rate PTR 27%
Kianmanesh 2021
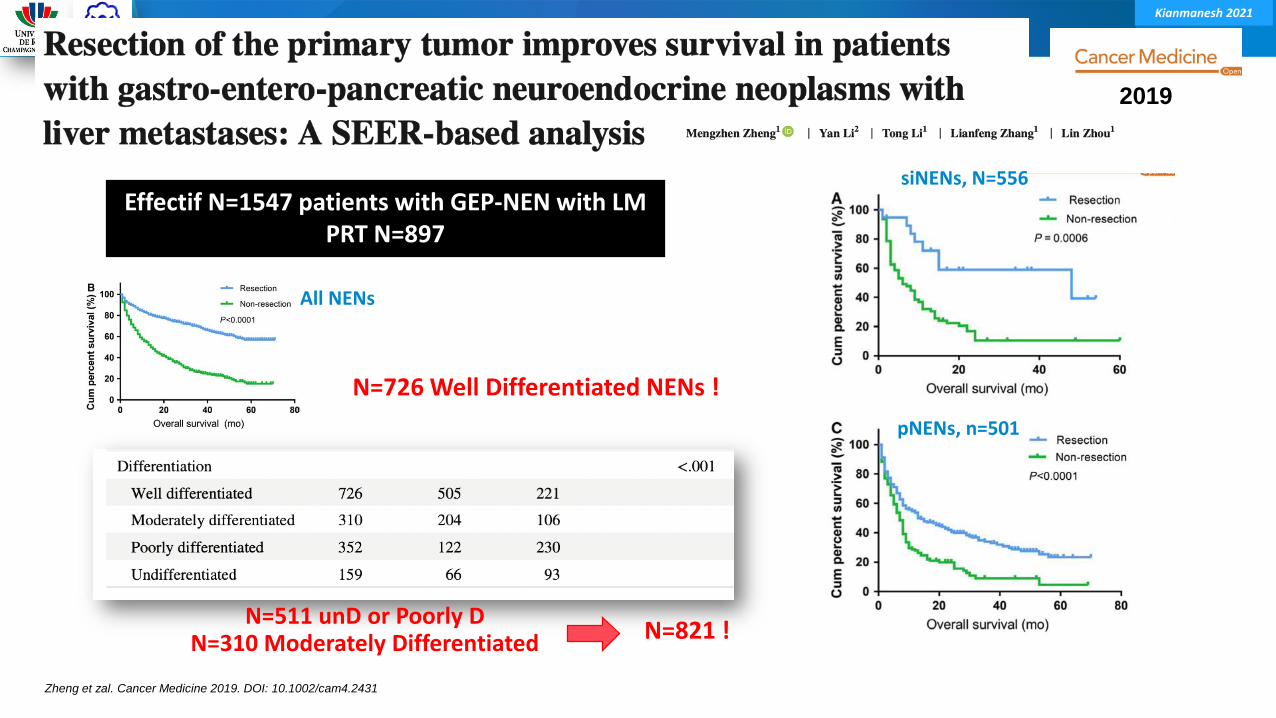
Zheng et zal. Cancer Medicine 2019. DOI: 10.1002/cam4.2431
2019
Effectif N=1547 patients with GEP-NEN with LMPRT N=897
siNENs, N=556
pNENs, n=501
All NENs
N=511 unD or Poorly DN=310 Moderately Differentiated
N=726 Well Differentiated NENs !
N=821 !
Kianmanesh 2021
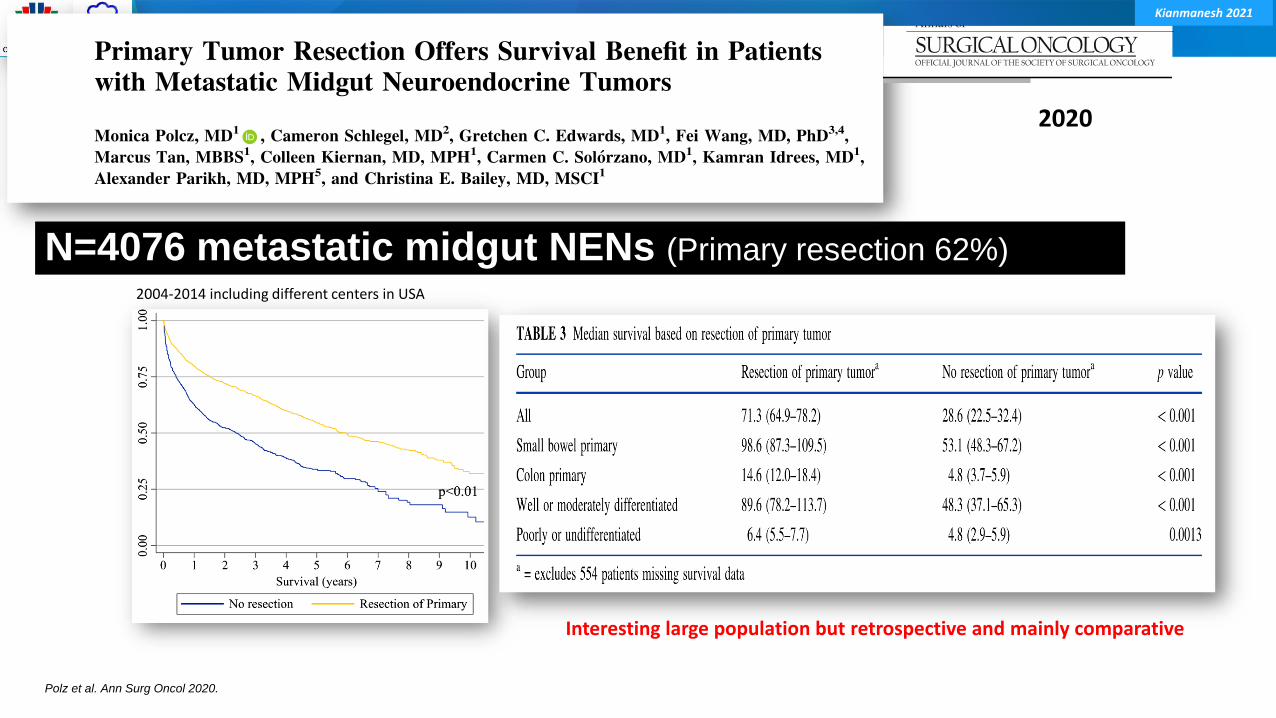
N=4076 metastatic midgut NENs (Primary resection 62%)
2020
Polz et al. Ann Surg Oncol 2020.
2004-2014 including different centers in USA
Interesting large population but retrospective and mainly comparative

Kianmanesh 2021
Daskalakis et al. JAMA Oncol. doi:10.1001/jamaoncol.2017.3326
Uppsala, Sweden, 1985-2015. N=363 Stage IV - SiNETs
No abdominal symptom within 6 months +++Emergency Surgery excluded.
Compared 2 groups:
N=161 prophylactic up-front LRSN=202 nonsurgical or delayed LRS
N=820 eligible N=363 included
2017
-Prophylactic up-front LRS conferred no survival
advantage in asymptomatic patients with stage IV
SI-NETs.
-Delayed surgery as needed was comparable in all examined
outcomes and was associated with fewer reoperations for
intestinal obstruction.
-The value of a priori LRS in the presence of distant
metastases is challenged and needs to be elucidatedin a randomized clinical study.
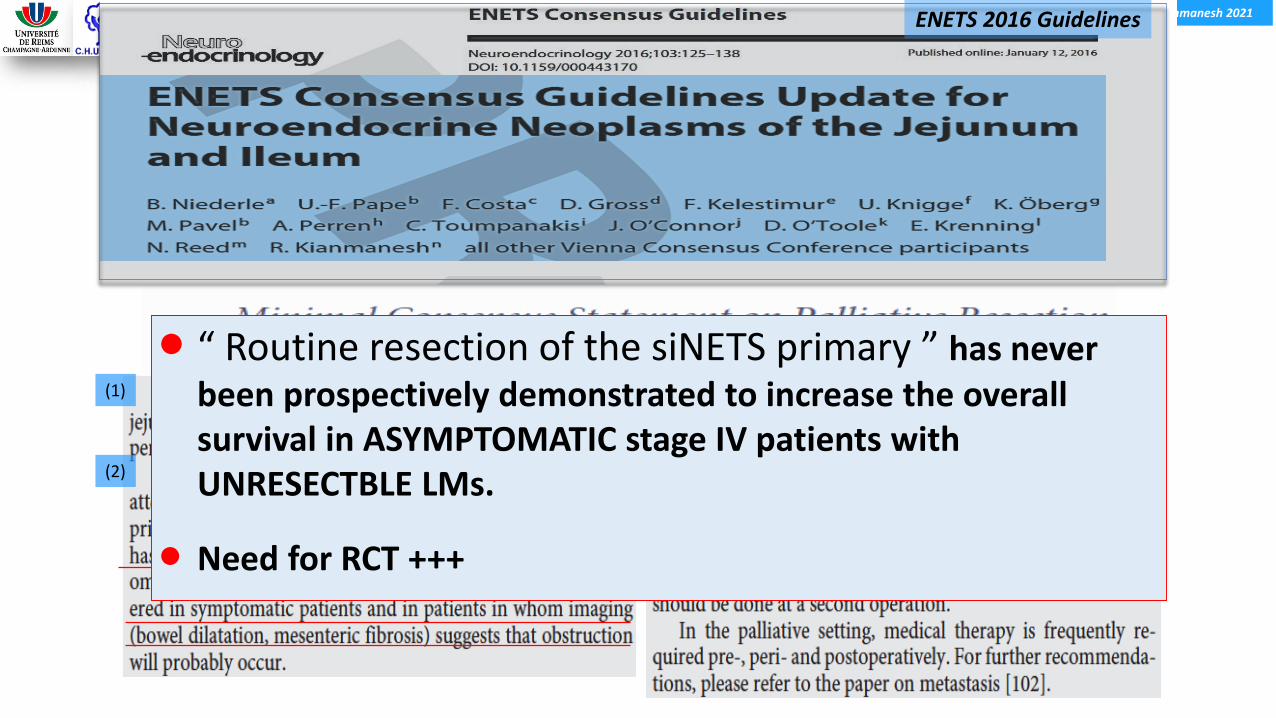
Kianmanesh 2021ENETS 2016 Guidelines
(1)
(2)
(3)
“ Routine resection of the siNETS primary ” has never been prospectively demonstrated to increase the overall survival in ASYMPTOMATIC stage IV patients with UNRESECTBLE LMs.
Need for RCT +++

Kianmanesh 2021
Take Home Messages and Conclusions
Kianmanesh 2021
Take Home Message “Primary resection in metastatic disease stage IV”
Andreasi et al. Curr Treat Options in Oncol 2020. Bertani et al. Surgery 2014. Neiderle et al. Current Oncology Reports 2021, 23, 85. Howe et al. Pancreas 2017. Howe et al. Pancreas 2020.
No Randomized Trial – Multiple selection bias in systematic reiews, meta-analyzes without RCT, retrospective data ?
● No survival benefit in case of G3 & poorly differentiated lesions (should be excluded from analyzes)
● PTR is recommended in all symptomatic siNET patients
● PTR may improve survival in selected patients with low-grade burden tumors, low risk resectableprimaries and in some patients with LMs in both pNENs and siNENs especially prior to PRRT.
● Patient selection in MDT remains mandatory in a multimodal long-term therapeutic strategy upon:
⁃ Patient’s general condition
⁃ Tumor grade/differentiation
⁃ Presence of extrahepatic disease / degree of liver involvement and resectability
⁃ Risks of PTR upon tumor nature and location, functionality, difficulties of lymphadenectomy (MM)
• for pNENs, body and tail pNENs rather than head of the pancreas (High morbidity)
• for SiNENs, remove the primary and LN and the MM (if possible, LN-stages I,II,IIIdown)
• Possibility of effective treatments including PPRT, LD-therapies, hepatectomy, TA and/or liver transplantation.





























