Embed Size (px)
Citation preview

Sickle Cell Anemia and Epidural Extramedullaty Hematopoiesis
LAWRENCE M. LEWKOW, M.D. ILA. SHAH, M.D., F.A.C.P.
Detroit, Michigan
Acute flaccid paralysis due to epidural extramedullary hematopoi- esis developed in a 43-year-old man with sickle cell anemia. The patient showed no response to emergency decompressive lami- nectomy, radiotherapy, or exchange transfusion, and his neurologic deficit persisted unimproved. This is the first reported case of acute or irreversible spinal cord compression due to epidural extramed- ullary hematopolesis in a patient with sickle cell anemia.
Sickle cell anemia is a chronic hemolytic disease with protean sys- temic manifestations due to intravascular occlusion and infarction in virtually every organ system. Central nervous system involvement is a well recognized complication of this disease [ 11; however, spinal cord injury has only rarely been documented in the sickling disorders [2-41, We report herein the first case of acute spinal cord compres- sion with irreversible paraplegia due to epidural extramedullary he- matopoiesis in a patient with sickle cell anemia.
CASE REPORT
From Wayne State University School of Medicine, and the Department of Medicine, Hutzel Hospital, Detroit, Michigan. Requests for reprints should be addressed to Dr. Lawrence M. Lewkow, Section of Hematology. Department of Medicine, Hutzel Hospital, 4707 St. Antoine, Detroit, Michigan 4820 1. Manuscript accepted May 18, 1983.
A 43-year-old black man with known sickle cell anemia was admitted to Hutzel Hospital on December 5, 1982, complaining of lower back and ab- dominal pain of one day’s duration. The back pain was reported to be in the lower thoracic area and was sharp and constant without radiation. The patient was fully ambulatory at the time of admission and denied fever, chills, loss of bowel or bladder control, or any neurologic deficit. Abdominal pain was periumbilical and epigastric without nausea or vomiting.
At the age of 11, the patient had a lengthy hospitalization for fever with radiologic evidence of osteomyelitis of vertebrae T7 to T9. Radiography at that time revealed mid-dorsal kyphosis with marked compression deformity of these dorsal segments. A paravertebral abscess was aspirated, and re- peated cultures for bacteria, fungi, and acid-fast bacilli gave negative results from blood, sputum, abscess, gastric washings, and bone marrow. Treatment with sulfadiazine, penicillin, and streptomycin was given, and the patient wore a body jacket until the age of 15, when radiography revealed fusion of the mkl-dorsal vertebrae. Results of repeated tuberculin skin tests were negative over these four years. The patient was lost to follow-up until age 38 and has since had two or three admissioins per year for mild vaso-occlusive crisis and acute pancreatitis secondary to ethanol abuse. Serial radiography over the past four years reveals osteoporosis of cervical and dorsal spine, shoulders, elbows, hips, and femur. No progression of dorsal vertebral de- struction had been noted over the last four years. Initial examination showed vital signs to be normal, and the patient afebrile. A cataract was present in the lef-t eye, and a grade II/VI systolic murmur was heard at the left sternal border. Abdominal palpation revealed mild tenderness in both lower quadrants with diminished bowel sounds. The liver was 8 cm in total span and no spleen
748 April 1984 The American Journal of Medicine Volume 76

SICKLE CELL ANEMIA AND EXTRAMEDULLARY HEMATOPOIESIS-LEWKOW and SHAH
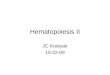
Figure 1. Left, Admission film demon- strating chronic gibbous deformity of vertebrae T7 to T9 with block vertebral deformity; right, initial myelogram per- formed in Trendelenberg position sho wjng block of contrast flow at the lower border of T8. Thoracic vertebral bodies are numbered.
was palpable or percussable. Initial neurologic examination revealed no deficits.
Initial laboratory values revealed a white blood count of 11,000 X lOgAiter with 51 percent polymorphonuclear leu- kocytes, 15 percent band forms, 17 percent lymphocytes, 12 percent monocytes, and 4 percent nucleated red blood cells. The hemoglobin level was 10.9 g/dl, hematocrit 31.5 percent, mean corpuscular volume 96.3, mean corpuscular hemoglobin content 34.6, and platelet count 55,000 X log/liter. Prothrombin time, partial thromboplastin time, thrombin time and fibrinogen level were all normal. Calcium, phosphorus, electrolyte, and blood urea nitrogen levels were also normal. Radiography of the thcracic spine (Figure 1, left) showed block vertebrae T7 to T9 with total obliteration of disk spaces and gibbous deformity with demineralization. These findings were unchanged over the past two years. Previous hemoglobin electrophoresis revealed hemoglobin S of 87 percent, A2 3 percent, and F 10 percent.
The patient was treated with fluids and intramuscular an- algesics on the night of admission and arose the next morning with complete paralysis of the right leg. Examination at that time revealed flaccid paralysis of the right leg, absent deep tendon reflexes, and bilaterally intact sensation, which evolved over the next six hours to complete lower extremity flaccid paralysis with a sensory level at T8. An indwelling urinary catheter drained 1,200 cc of urine. Myelography (Figure 1, right) revealed complete block of contrast at the lower border of T9. The cerebrospinal fluid was xantho- chromic, with a red blood cell count of 470 X log/liter, white blood cell count 0 X 10g/liter, glucose 88 mg/dl, and protein 298 mg/dl.
At emergency laminectomy, increased vascularity of the tissues of the paraspinous muscles was noted with thickened and hypertrophic bone. A thick epidural membrane was present and recent hemorrhage seen. After the epidural tissue was opened, the intradural contents showed free pulsation
after the tissue was removed. The surgical pathologist re- ported light and dark brown fibrous tissue that proved to be adipose tissue and blood vessels with extramedullary he- matopoiesis infiltrating the fibroadipose tissue (Figure 2). In one focus, the extramedullary hematopoiesis took the form of a well-encapsulated mass. The extramedullary hemato- poiesis was noted to be of distinct foci and did not extrude from the marrow space. Direct gram stains from the operative site showed some gram-positive cocci, and 10 days of treatment with nafcillin was given; however, all cultures, in- cluding those for fungi and mycobacteria, showed negative results. Dexamethasone was given postoperatively, and the patient showed some improvement in sensor level over the following 10 days; however, there was no improvement in motor ability below T9 level. Repeated myelography on De- cember 20, 1982, showed flow of contrast material into the cervical subarachnoid space with some tapering of the dye thought to be secondary to the gibbous deformity. Protein level in the cerebrospinal fluid had decreased to 163 mg/dl. Technetium bone scanning failed to reveal any other areas of extramedullary hematopoiesis.
Local radiotherapy of 1,000 rads was started on January 3, 1983, in 200~rad doses, and exchange transfusion lowered the hemoglobin S level to 30 percent. The patient was transferred to a rehabilitation institute and, eight months after the initial event, remains in flaccid paralysis with atonic bladder and without noticeable improvement in motor ability.
COMMENTS
Extramedullary hematopoiesis, or myeloid metaplasia,
is an unusual phenomenon usually seen in disease
states in which there is pathologic encroachment on, or abnormal activity of, intramedullary marrow-forming areas. The underlying disease may be unknown, as in
April 1984 The American Journal of Medicine Volume 78 749

SICKLE CELL ANEMIA AND EXTRAMEDULLARY HEMATOPOIESIS-LEWKOW and SHAH
agnogenic myeloid metaplasia, or secondary to other conditions of the medullary space, as outlined by Ward and Block [5]. Their category of reactive conditions includes the hemolytic anemias such as thalassemia and sickle cell disease. The precise mechanism causing the development of extramedullary hematopoiesis is not clear; however, a recent study in rabbits [6] has shown increased myeloid and erythroid progenitor cells in blood and spleen as these cells are depleted from the marrow. Thus, a possible mechanism of extramedullary hematopoiesis may be the colonization of extramed- ullary sites by bone marrow-derived stem cells.
Although extramedullary hematopoiesis may develop in any of numerous sites-most frequently liver, spleen, and lymph nodes-epidural extramedullary hemato- poiesis with cord involvement is a rare occurence. Only
TABLE I Previously Reported Cases of Epidural Extramedullary Hematopoiesis
Diagnosis Number Reported
Thalassemia major 6 Thalassemia intermedia 6 Myelosclerosis 6 Polycythemia rubra vera 2 Sickle cell anemia 1 Pyruvate kinase deficiency 1
Paget’s disease 1 Sideroblastic anemia 1 Chronic eosinophilic leukemia 1 Transposition of great vessels 1 Hemoglobin E 1 Pachydermoperiostosis 1
Figure 2. Photomicrograph of extra- medullary hematopoietic nodule removed at surgery. Note abundant megakaryo- cytes and myeloid elements (original magnification X 1,000, reduced by 30 percent).
28 cases [7-l I] of epidural extramedullary hemato- poiesis have been previously reported, many of these reviewed recently [7] and almost half seen in thalas- semic states (Table I). Only one previous case of epi- dural extramedullary hematopoiesis has been docu- mented in sickling disorders [ 121. In that patient, gradual weakness in the legs developed over a period of two months, but he was first seen by a physician 18 months after the onset of symptoms. He was noted to have complete spastic paraplegia with loss of sensation below the T7 dermatome and recovered completely within five months after decompressive laminec- tomy.
In our case, paralysis was extremely abrupt; in fact, the patient was fully ambulatory on the evening of ad- mission with no neurologic deficit at that time. The du- ration between his first symptom of right leg paralysis and decompressive laminectomy was less than 12 hours and evolution to complete flaccid paralysis oc- curred over only a six-hour period. As in most cases of epidural extramedullary hematopoiesis, decompressive laminectomy was the main modality of therapy due to the difficulty in making the diagnosis of extramedullary hematopoiesis noninvasively except in the unusual circumstance when extramedullary hematopoiesis is found previously at another site [ 131. The consulting neurosurgeon noted tumor involving the dura with small hematoma and a return of pulsatile state after tissue excision and laminectomy, giving credence to the idea that these tissues had caused vascular compromise locally. What role the hematoma played in the acute syndrome is not clear, however the hematopoietic tis- sue itself was noted to be a well-encapsulated mass.
750 April 1984 The American Journal of Medicine Volume 76

SICKLE CELL ANEMIA AND EXTRAMEDULLARY HEMATOPOIESIS-~ LEWKOW and SHAH
A trial of 1,000 rads of local radiotherapy was given
in view of several previous reports in which the com-
bination of surgery and 1,000 to 4,000 rads yielded
complete or partial recovery [7-l 11. In fact, four pa-
tients in whom the diagnosis of epidural extramedullary
hematopoiesis was made presumptively showed good
recovery with radiotherapy alone [7]. Technetium-99m
scanning was performed as reported by Bronn et al [ 141
in an attempt to delineate other areas of extramedullary
hematopoiesis for prophylactic treatment, although
other radionuclides such as gold-198, iron-52, and in-
dium [7] as well as computed tomography [ 151 have
been used successfully for this purpose.
It is unclear what role our patient’s long-standing
vertebral deformity played in the acute neurologic event.
A previous work-up for other causes of osteoporosis
revealed nothing, as did a thorough investigation for
infection at the time of surgery. The resemblance of the
vertebral deformity to tuberculous osteomyelitis led to
many fruitless searches for mycobacteria over the
course of 30 years, and there was no observable dif-
ference in spinal x-ray films for several years prior to
this admission. Ten of the previous cases of epidural
extramedullary hematopoiesis revealed radiologic
changes of osteoporosis or vertebral body collapse in
the involved areas; however, this is not an unusual
finding in sickling disorders. Karayalcin et al [ 161 re-
ported demineralization of the vertebral bodies to be the
most common x-ray finding of the spine in 127 patients
with sickle cell anemia, with a prevalence of 30 percent
in their report, although “wedge-shaped” compression
fracture was rare. There has been controversy in pre-
viously reported cases concerning the possibility that
the extramedullary hematopoiesis was simply extruded
from the diseased vertebrae, although this was clearly
not the finding in our case.
Exchange red cell transfusion was administered in
view of its apparent success in other central nervous
system disorders in sickle cell anemia [ 171, although
its efficacy in spinal cord injury is unclear.
Although this is only the second case of epidural
extramedullary hematopoiesis reported in sickle cell
anemia, our patient had much in common with previous
patients with this entity and diverse underlying diseases.
Eighty-four percent have been males with an average
age of 39 years. Patients with acute onset of neurologic deficits showed slow and incomplete recovery, and all
patients but one have had involvement of the thoracic
spine. Although most previous cases have been re-
ported in the surgical and radiologic literature, epidural
extramedullary hematopoiesis has always been seen
in conditions cared for by internists and generalists and,
even though rare, needs to be considered in the differ-
ential diagnosis of cord compression in the chronic
hemolytic anemias.
ACKNOWLEDGMENT
We would like to thank Doctors D. Austin, J. Kinzie, S.
Sheehan, and J. Warth for their help in the care of this
patient, and Mary Jackson for her assistance in prep-
aration of this manuscript.
6.
7.
8.
9.
Powars D, Wilson B, lmbus C, Pegelow C, Allen J: The natural historv of stroke in sickle cell disease. Am J Med 1978; 65: 461-471.
Greer M, Schotland D: Abnormal hemoglobin as a cause of neurological disease. Neurology (Minneapolis) 1962; 12: 114-123.
Guillozet N: Sickle cell SS genotype and paralysis in children. J Pediatr 1976; 89: 605-607.
Rothman SM, Nelson JS: Spinal cord infarction in a patient with sickle cell anemia. Neurology 1980; 30: 1072- 1076.
Ward HP, Block MH: The natural history of agnogenic myeloid metaplasia and a critical evaluation of its relationship with the myeloproliferative syndrome. Medicine (Baltimore) ; 1971; 50: 357-435.
Wang JC, Tobin MS: Mechanisms of extramedullary hema- topoiesis in rabbits with saponin induced myelofibrosis and myeloid metaplasia. Br J Haematol 1982; 51: 277-284.
Heffez DS, Sawaya R, Udvarhelyi GB, Mann R: Spinal epidural extramedullary hematopoiesis with cord compression in patient with refractory sideroblastic anemia. J Neurosurg 1982; 57: 399-406.
Ahmed F, Tobin M, Cohen D, Gomez Leon G: Beta thalas- semia. Spinal cord compression. NY State J Med 1981; 81: 1505-1508.
Wilson JJ, Hill ME, Crookston JH: Irradiation for progressive
REFERENCES
paraparesis in beta-thalassemia intermedia. Can Med Assoc J 1980; 123: 1133-1136.
10. Neiman HC, Gompels BM, Martel W: Pachydermoperiostosis with bone marrow failure and gross extramedullary he- matopoiesis. Radiology 1974; 110: 553-554.
11. Julien J, Broustet A, Trojani M, et al: Spinal cord compression by extramedullary hematopoiesis in chronic eosinophilic leukemia. Sem Hop Paris 1981; 57: 598-600.
12. Ammoumi AA,Sher JH, Schmelka D: Spinal cord compression by extramedullary hematopoietic tissue in sickle cell ane- mia. J Neurosurg 1975; 43: 483-485.
13. Sorsdahl OS, Taylor PE, Noyes WD: Extramedullary hemato- poiesis, mediastinal masses and spinal cord compression. JAMA 1964; 189: 89-93.
14. Bronn LJ, Paquelet JR, Tetalman MR: lntrathoracic extra- medullary hematopoiesis: appearance on 99m Tc sulphur colloid marrow scan. AJR 1980; 134: 1254-1255.
15. Case records of the Massachusetts General Hospital weekly clinicopathological exercises, case 23-1981. N Engl J Med 1981; 304: 1411-1421.
16. Karayalcin G, Dorfman J, Rosner F, Aballi AJ: Radiological changes in 127 patients with sickle cell anemia. Am J Med Sci 1976; 271: 132-144.
17. Lusher JM, Haghighat H, Khalifa AS: A prophylactic transfusion program for children with sickle cell anemia complicated by CNS infarction. Am J Hematol 1976; 1: 265-273.
April 1994 The American Journal of Medicine Volume 76 751