Embed Size (px)
Citation preview
J Clitn Pathol 1981 ;34:884-891
Signet ring cell lymphoma: a rare variant offollicular lymphomaM HARRIS, B EYDEN, G READ*
From the Department of Pathology, and *Department of Radiotherapy, Christie Hospital andHolt Radium Institute, Manchester M20 9BX
SUMMARY A case of signet ring cell lymphoma, the eighth in published reports is recorded. This raretumour is a variant of follicular lymphoma which may be mistaken for metastatic carcinoma. Thecase has been studied by light microscopy, immunohistochemistry and electron microscopy andconfirms that this sub-group has rather uniform characteristics. Observations on the possible originsof the vacuoles are presented.
Since 1978, six cases of malignant lymphoma inwhich signet ring cells were a prominent histologicalfeature have been recorded in published reports inthe USA' 2 3 and one further case with a few suchcells has also been recorded.2 One case has beenrecorded in Australia.4 This is a little known and raremorphological variant of lymphoma whose histo-logical appearances may be misinterpreted if thepathologist is unaware of its existence. For thisreason we wish to record the first case to appear in aBritish publication.
Case report
A 57-year-old man presented at another hospitalwith a three month history of a swelling in the leftgroin. His general health was excellent and he wasotherwise asymptomatic. A right-sided hydrocelehad been drained 18 months earlier but there was noother previous medical history. A biopsy of theswelling was done and he was referred to thishospital for treatment.On examination he was a fit man. There was a
recent biopsy scar in the left groin with a mass ofresidual lymph nodes deep to it, but no otherperipheral lymphadenopathy was detected. The liverand spleen were not enlarged. There was a right-sidedhydrocele but both testes were normal to palpation.A small basal cell carcinoma, proven by biopsy, waspresent on the left outer canthus.
Investigations were as follows: haemoglobin16-8 g/dl, white cell count 6-9 x 109/l (6900/mm3),platelet count 254 x 109/l (254 000/mm3). Bio-chemical profile normal. Serum protein electro-
Accepted for publication 7 January 1981
phoresis normal. Serum immunoglobulin con-centrations: IgG 12 g/l (normal 8 0-16 0), IgA1 9 g/l (normal 1-2-4 0), IgM 1 3 g/l (normal 0-5-1-6).Twenty-four hour urine immunoassay: 1 2 1 ofurine contained 6-3 mg of kappa light chains and0 9 mg of lambda light chains (normal < 200 mg/l).Bone marrow aspirate and trephine-normal. Chestx-ray examination showed some cardiac enlarge-ment but was otherwise normal. Intravenousurogram-normal. Computer-assisted tomographyof lower chest and abdomen did not show evidence oflymphadenopathy. In view of the difficulty ininterpreting the first biopsy a further biopsy of theinguinal mass was done.
After diagnosis a radical course of radiotherapywas given, the field encompassing the para-aortic,iliac and inguinal node areas. A central mid-planedose of 3500 cGy was given in 20 fractions over28 days. By the conclusion of the radiotherapy therehad been almost complete clinical resolution of theaffected inguinal nodes. The basal cell carcinomaalso received radiotherapy.
Material and methods
LIGHT MICROSCOPYTissue was fixed in 10% buffered formalin, processedand embedded in paraffin wax by conventionaltechniques. Sections (5 ,um) were then stained byhaematoxylin and eosin (H and E), Gordon andSweet's method for reticulin fibres, PAS, diastase-PAS and Alcian blue. Stains for acid phosphatasewere done using a modification of the method ofYam, Li and Lam.5Wax sections were also stained by the peroxidase-
antiperoxidase technique for IgG, IgM, IgA, lambda884
copyright. on 7 S
eptember 2018 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.8.884 on 1 August 1981. D
ownloaded from
Signet ring cell lymphoma: a rare variant offollicular lymphoma
and kappa light chains, and for muramidase.Frozen sections of the formalin-fixed tissue werestained for lipids by oil red 0, Sudan black and Nileblue sulphate.Touch preparations from the cut surface of the
fresh lymph node were air-dried, fixed in 10%formalin and stained by H and E and Giemsa. Smallblocks were also embedded in Spurr resin, sectionedat 2 ,um and stained by H and E.
ELECTRON MICROSCOPYFresh tissue from the second lymph node biopsy wasminced into 1 mm cubes and fixed in chilled 40%glutaraldehyde in Millonig's buffer. After rinsing inbuffer and secondary fixation in 1% osmium tetroxide,the specimens were dehydrated in acetone and 1,2-epoxypropane and embedded in TAAB 812. AnLKB Ultrotome III was used to cut 1 tm surveysections which were stained with toluidine blue inaqueous 1% borax; ultra-thin sections were stainedin aqueous uranyl acetate, then lead citrate andexamined in a Kratos ex-clinical 275 electronmicroscope.
Results
LIGHT MICROSCOPY
Original biopsy offemoral lymph node This node wasextensively necrotic and, beyond suggesting thatit might well be the site of lymphoma, no firmdiagnosis was made.
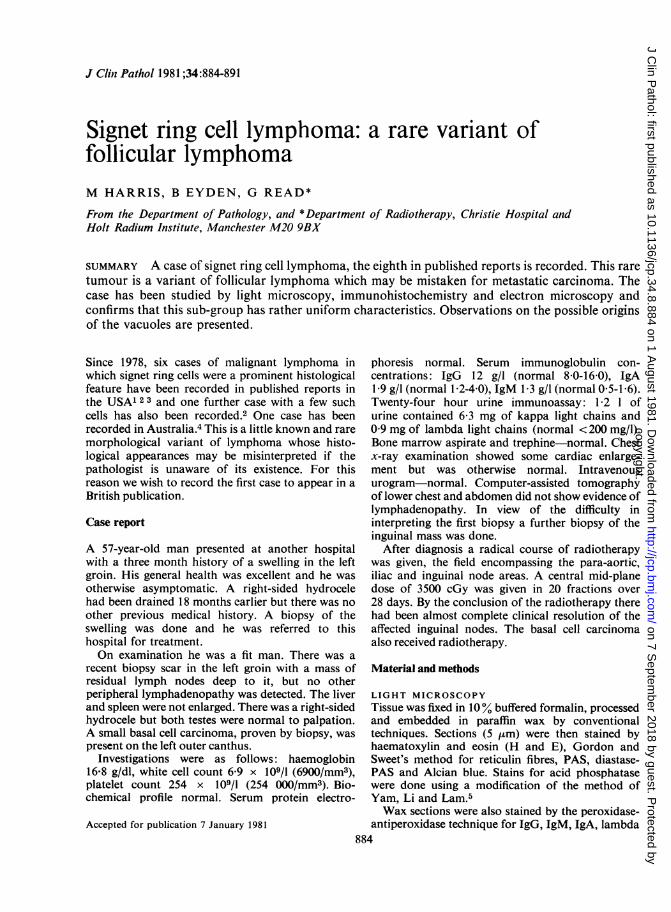
Second biopsy of femoral lymph node The normalnodal architecture was destroyed. Approximately80% of the node was replaced by lymphomaof diffuse pattern but at the periphery a rimof neoplastic follicles was apparent (Fig. 1).Slight extension of lymphoma cells into perinodaltissues was present. In the areas of diffuse pattern,a high proportion of the cells were of signet ringmorphology. They contained cytoplasmic vacuoles ofvariable size, the largest compressing the nucleus to aperipheral crescent (Figs. 2 and 3). The other cells inthis area were mainly small centrocytes (smallcleaved cells) having characteristic irregular nucleiwith absent or inconspicuous nucleoli and sparse
a Fig. 1 iVeoplastic follicles areseen to the left with lymphoma ofdiffuse pattern to the right.Haematoxylin and eosin x 58
885
copyright. on 7 S
eptember 2018 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.8.884 on 1 August 1981. D
ownloaded from
Harris, Eyden, Read
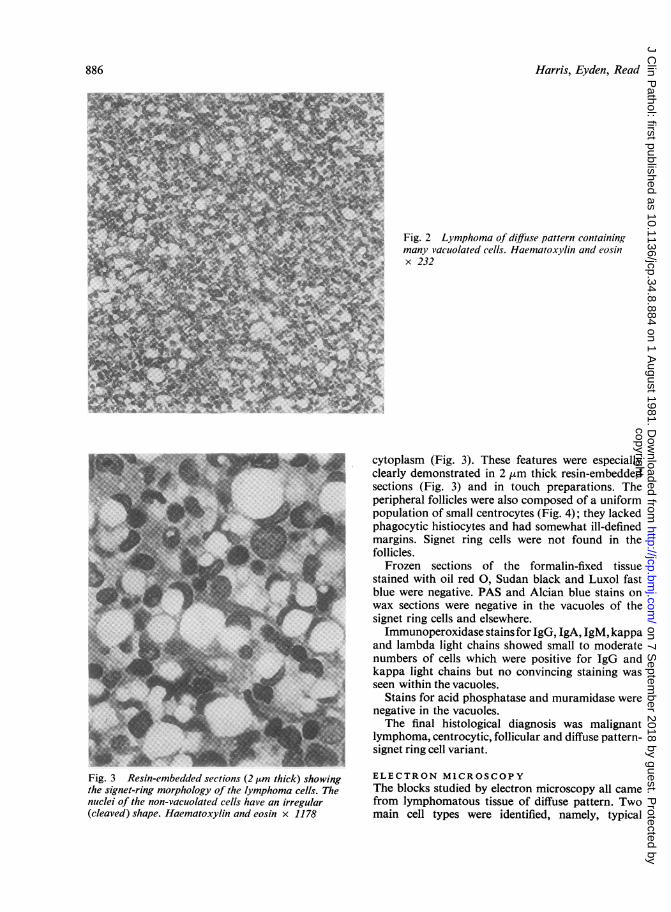
Fig. 3 Resin-embedded sections (2 ttm thick) showingthe signet-ring morphology of the lymphoma cells. Thenuclei of the non-vacuolated cells have an irregular(cleaved) shape. Haematoxylin and eosin x 1178
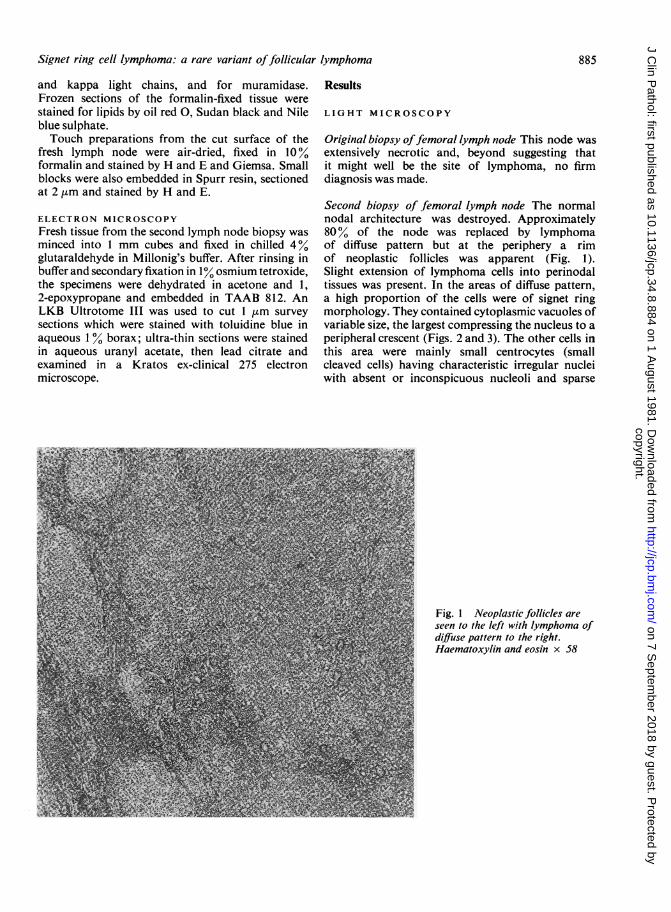
Fig. 2 Lymphoma of diffiuse pattern containing; many vacuolated cells. Haematoxylin and eosin
| j x 232
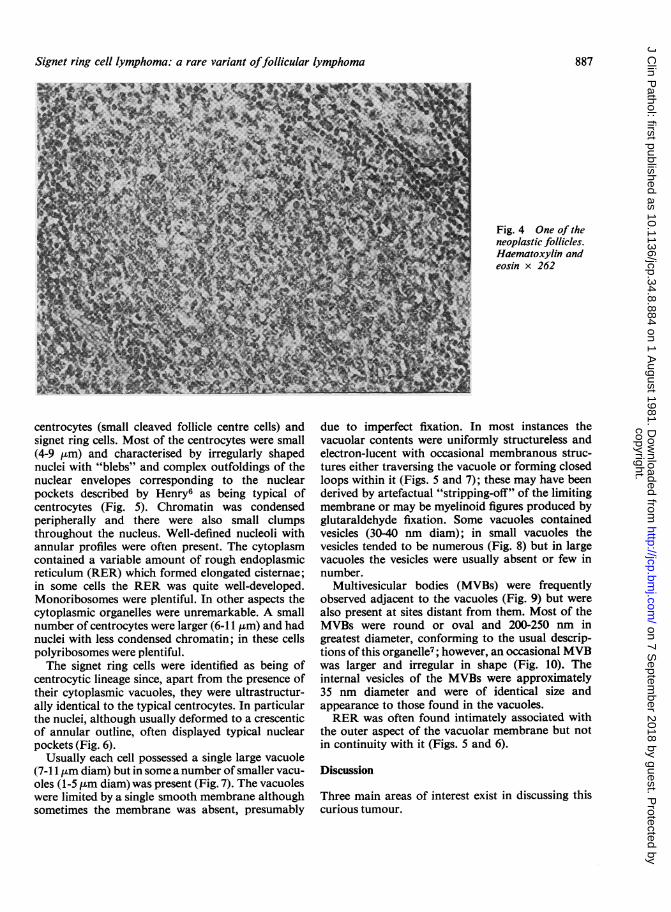
cytoplasm (Fig. 3). These features were especiallyclearly demonstrated in 2 tsm thick resin-embeddedsections (Fig. 3) and in touch preparations. Theperipheral follicles were also composed of a uniformpopulation of small centrocytes (Fig. 4); they lackedphagocytic histiocytes and had somewhat ill-definedmargins. Signet ring cells were not found in thefollicles.
Frozen sections of the formalin-fixed tissuestained with oil red 0, Sudan black and Luxol fastblue were negative. PAS and Alcian blue stains onwax sections were negative in the vacuoles of thesignet ring cells and elsewhere.Immunoperoxidase stains for IgG, IgA, 1gM, kappa
and lambda light chains showed small to moderatenumbers of cells which were positive for IgG andkappa light chains but no convincing staining wasseen within the vacuoles.
Stains for acid phosphatase and muramidase werenegative in the vacuoles.The final histological diagnosis was malignant
lymphoma, centrocytic, follicular and diffuse pattern-signet ring cell variant.
ELECTRON MICROSCOPYThe blocks studied by electron microscopy all camefrom lymphomatous tissue of diffuse pattern. Twomain cell types were identified, namely, typical
886
copyright. on 7 S
eptember 2018 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.8.884 on 1 August 1981. D
ownloaded from
Signet ring cell lymphoma: a rare variant offollicular lymphoma
Fig. 4 One of theneoplastic follicles.Haematoxylin andeosin x 262
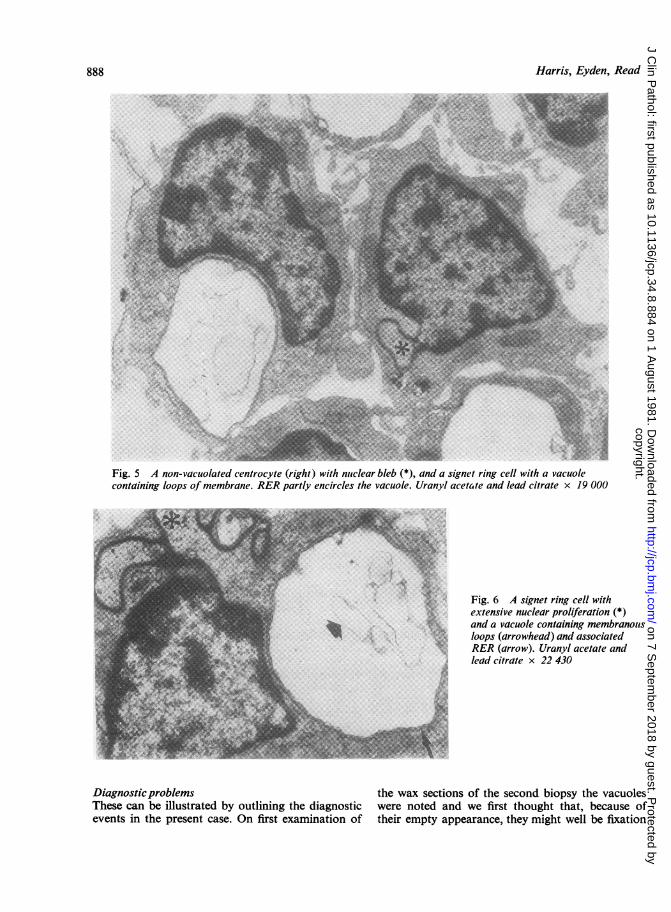
centrocytes (small cleaved follicle centre cells) andsignet ring cells. Most of the centrocytes were small(4-9 Km) and characterised by irregularly shapednuclei with "blebs" and complex outfoldings of thenuclear envelopes corresponding to the nuclearpockets described by Henry6 as being typical ofcentrocytes (Fig. 5). Chromatin was condensedperipherally and there were also small clumpsthroughout the nucleus. Well-defined nucleoli withannular profiles were often present. The cytoplasmcontained a variable amount of rough endoplasmicreticulum (RER) which formed elongated cisternae;in some cells the RER was quite well-developed.Monoribosomes were plentiful. In other aspects thecytoplasmic organelles were unremarkable. A smallnumber of centrocytes were larger (6-11 ,um) and hadnuclei with less condensed chromatin; in these cellspolyribosomes were plentiful.The signet ring cells were identified as being of
centrocytic lineage since, apart from the presence oftheir cytoplasmic vacuoles, they were ultrastructur-ally identical to the typical centrocytes. In particularthe nuclei, although usually deformed to a crescenticof annular outline, often displayed typical nuclearpockets (Fig. 6).
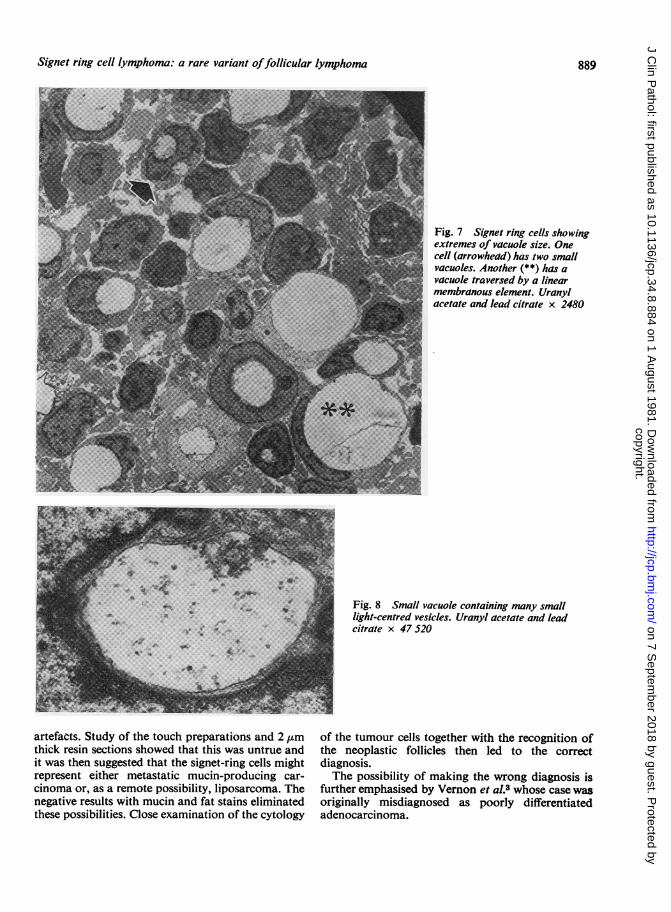
Usually each cell possessed a single large vacuole(7-11 ILm diam) but in some a number of smaller vacu-oles (1-5 ,um diam) was present (Fig. 7). The vacuoleswere limited by a single smooth membrane althoughsometimes the membrane was absent, presumably
due to imperfect fixation. In most instances thevacuolar contents were uniformly structureless andelectron-lucent with occasional membranous struc-tures either traversing the vacuole or forming closedloops within it (Figs. 5 and 7); these may have beenderived by artefactual "stripping-off" of the limitingmembrane or may be myelinoid figures produced byglutaraldehyde fixation. Some vacuoles containedvesicles (30-40 nm diam); in small vacuoles thevesicles tended to be numerous (Fig. 8) but in largevacuoles the vesicles were usually absent or few innumber.
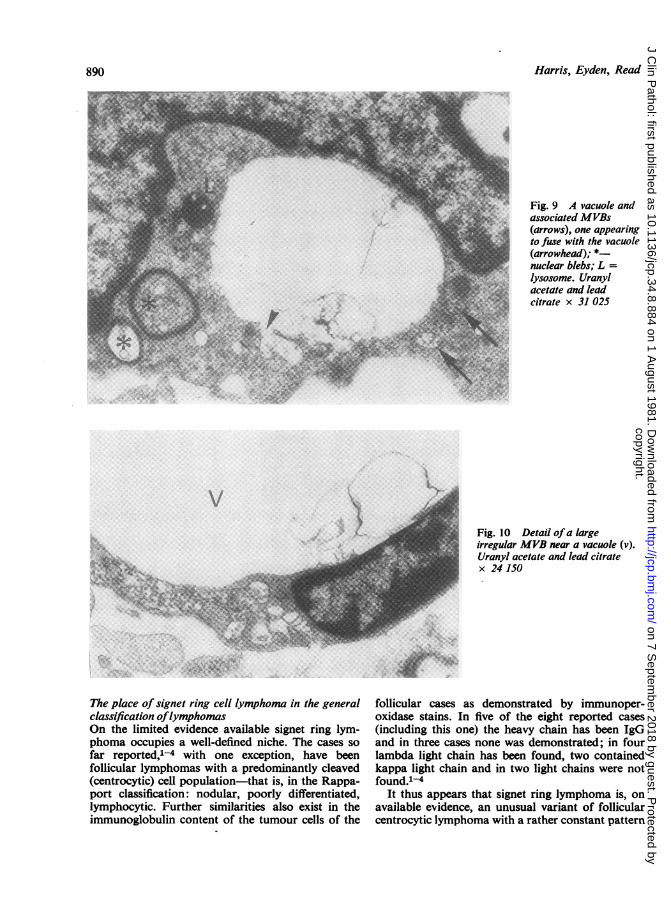
Multivesicular bodies (MVBs) were frequentlyobserved adjacent to the vacuoles (Fig. 9) but werealso present at sites distant from them. Most of theMVBs were round or oval and 200-250 nm ingreatest diameter, conforming to the usual descrip-tions of this organelle7; however, an occasional MVBwas larger and irregular in shape (Fig. 10). Theinternal vesicles of the MVBs were approximately35 nm diameter and were of identical size andappearance to those found in the vacuoles.RER was often found intimately associated with
the outer aspect of the vacuolar membrane but notin continuity with it (Figs. 5 and 6).
Discussion
Three main areas of interest exist in discussing thiscurious tumour.
887
copyright. on 7 S
eptember 2018 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.8.884 on 1 August 1981. D
ownloaded from
Harris, Eyden, Read
t.
Fig. 5 A non-vacuolated centrocyte (right) with nuclear bleb (*), and a signet ring cell with a vacuolecontaining loops of membrane. RER partly encircles the vacuole. Uranyl acetaite and lead citrate x 19 000
Fig. 6 A signet ring cell withextensive nuclear proliferation (*)and a vacuole containing membranouisloops (arrowhead) and associatedRER (arrow). Uranyl acetate andlead citrate x 22 430
DiagnosticproblemsThese can be illustrated by outlining the diagnosticevents in the present case. On first examination of
the wax sections of the second biopsy the vacuoleswere noted and we first thought that, because oftheir empty appearance, they might well be fixation
888
copyright. on 7 S
eptember 2018 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.8.884 on 1 August 1981. D
ownloaded from
Signet ring cell lymphoma: a rare variant offollicular lymphoma
Fig. 7 Signet ring cells showingextremes of vacuole size. Onecell (arrowhead) has two smallvacuoles. Another (**) has avacuole traversed by a linearmembranous element. Uranylacetate and lead citrate x 2480
:....:....F...'... '...... ....
.... ... ..... ..
......
*.
Fig. 8 Small vacuole containing many smalllight-centred vesicles. Uranyl acetate and leadcitrate x 47 520
artefacts. Study of the touch preparations and 2 ,mthick resin sections showed that this was untrue andit was then suggested that the signet-ring cells mightrepresent either metastatic mucin-producing car-cinoma or, as a remote possibility, liposarcoma. Thenegative results with mucin and fat stains eliminatedthese possibilities. Close examination of the cytology
of the tumour cells together with the recognition ofthe neoplastic follicles then led to the correctdiagnosis.The possibility of making the wrong diagnosis is
further emphasised by Vernon et al.3 whose case wasoriginally misdiagnosed as poorly differentiatedadenocarcinoma.
889
copyright. on 7 S
eptember 2018 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.8.884 on 1 August 1981. D
ownloaded from
Harris, Eyden, Read
Fig. 9 A vacuole andassociated MVBs(arrows), one appearingto fuse with the vacuole(arrowhead); *nuclear blebs; L =
lysosome. Uranylacetate and leadcitrate x 31 025
X-2..~ ~ ..... -
The place of signet ring cell lymphoma in the generalclassification oflymphomasOn the limited evidence available signet ring lym-phoma occupies a well-defined niche. The cases sofar reported,'4 with one exception, have beenfollicular lymphomas with a predominantly cleaved(centrocytic) cell population-that is, in the Rappa-port classification: nodular, poorly differentiated,lymphocytic. Further similarities also exist in theimmunoglobulin content of the tumour cells of the
Fig. 10 Detail of a largeirregular MVB near a vacuole (v).Uranyl acetate and lead citratex 24 150
follicular cases as demonstrated by immunoper-oxidase stains. In five of the eight reported cases(including this one) the heavy chain has been IgGand in three cases none was demonstrated; in fourlambda light chain has been found, two containedkappa light chain and in two light chains were notfound.14
It thus appears that signet ring lymphoma is, onavailable evidence, an unusual variant of follicularcentrocytic lymphoma with a rather constant pattern
890
copyright. on 7 S
eptember 2018 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.8.884 on 1 August 1981. D
ownloaded from

Signet ring cell lymphoma: a rare variant offollicular lymphoma
of cytoplasmic immunoglobulin production.The possible exception to this generalisation is
represented by case 2 of Van den Tweel et al.2 Thiscase was diagnosed as immunoblastic sarcoma andalthough signet ring cells were present they were veryfew in number and a more prominent feature was thepresence of many Russell's bodies.
The origin and nature ofthe vacuolesSix cases from the previous reports have been studiedby electron microscopy. In five the vacuoles havebeen observed to be membrane-bound and all sixhave contained variable numbers of intravacuolarmicrovesicles. Vernon et al.3 state that the limitingmembrane of the vacuoles is continuous withadjacent smooth endoplasmic reticulum, althoughthis feature is not illustrated. We have not been ableto confirm this observation but we have noted arelation with the RER, although continuity betweenvacuole membrane and RER was not found. Thisultrastructural pattern does not, however, resemblethe accumulations of RER which formed thecytoplasmic inclusions in cases IP, RW and MS ofKim et al.1
Previous workersl-3 with the exception of Moir4also agree that immunoperoxidase stains demon-strate the presence of immunoglobulin within thesignet-ring cells although they comment thatstaining is usually confined to a narrow peripheralrim of the vacuoles. The consensus thus appears tobe that the vacuoles are accumulations of intra-cellular immunoglobulin, and Vernon et al.3 suggestthat it is stored within the microvesicles. Previousauthors12 have thus tended to consider the signetring lymphomas as being in some way analogouswith lymphomas in which Russell's bodies areprominent and have implied that the two types ofinclusion are related phenomena, although ultra-structurally they are quite different.Our own findings differ somewhat from most
previously reported observations.'-3 The immuno-peroxidase technique did not convincingly demon-strate intravesicular immunoglobulin agreeing withthe results of Moir.4 The suggestion that the intra-vacuolar vesicles contain immunoglobulin3 might becompatible with these findings, since in our casethese vesicles were sparse, many vacuoles appearingentirely empty. The small vacuoles containing manyvesicles would be expected to stain for immuno-globulin and such vacuoles may perhaps have beenpresent, but not recognisable by light microscopy, inthose cells staining positively for immunoglobulin.However, we are not convinced that the intra-
vacuolar vesicles are, in fact, stored immunoglobulinand our ultrastructural observations suggest thatthey may be derived from MVBs. The evidence forthis lies in the frequent proximity of MVBs to thevacuoles and the identical size and structure of thevesicles in the MVBs and the vacuoles although onlyone example where an MVB appeared to be incontinuity with a vacuole could be found (Fig. 9).MVBs are a form of lysosome7 and structuresinterpreted as giant MVBs by Ghadially7 werereported in multiple myeloma cells by Sorenson(1961)8 and in reticulosarcoma cells by Vasquez,Pavlovsky and Bernhard.9 Thus, it might be that thevacuoles in signet ring cell lymphomas are alsogiant MVBs, although our negative results withstains for lysosomal enzymes are against thishypothesis.
Addendum
Since this paper was accepted for publication afurther case of signet ring cell lymphoma has beenreported from Italy. However, in this case the cell-ular inclusions were of the "Russell's body" type.'0
References
' Kim H, Dorfman RF, Rappaport H. Signet ring celllymphoma. A rare morphologic and functional expressionof nodular (follicular) lymphoma. Am J Surg Pathol 1978;2:119-32.
2 Van den Tweel JG, Taylor CR, Parker JW, et al. Immuno-globulin inclusions in non-Hodgkin's lymphomas. Am JClinPathol 1978;69:306-13.
Vernon S, Voet RL, Naeim F, et al. Nodular lymphomawith intracellular immunoglobulin. Cancer 1979;44:1273-9.
4 Moir DH. Signet ring cell lymphoma: a case report.Pathology 1980;12:1 19-22.
6Yam LT, Li CY, Lam KW. Tartrate resistant acid phospha-tase isoenzyme in the reticulum cells of leukemic reticulo-endotheliosis. N Engi J Med 1971;284:357-60.
6 Henry K. Electron microscopy in the non-Hodgkin'slymphomata. Br J Cancer 1976;31, suppl II:73-93.
7 Ghadially FN. Ultrastructural pathology of the cell. Londonand Boston: Butterworths, 1975.
8Sorenson GD. Electron microscopic observations of viralparticles within myeloma cells of man. Exp Cell Res 1961;25:219-21.
Vasquez C, Pavlovsky A, Bernhard W. Lesions nucleaireset inclusions cytoplasmiques particulieres dans deux casde lymphoreticulo-sarcomes humains. CR Acad Sci(Paris) 1963 ;256:2261-4.
10 Pileri S, Serra L, Govoni E, at al. Signet ring cell lym-phoma: a case report. Histopathology 1981 ;5:165-73.
Requests for reprints to: Dr M Harris, Department ofPathology, Christie Hospital and Holt Radium Institute,Manchester M20 9BX, England.
891
copyright. on 7 S
eptember 2018 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.8.884 on 1 August 1981. D
ownloaded from