Embed Size (px)
Citation preview
Egypt Rheumatol Rehab Vol. 30, No. 1, January 2003
51
SIGNIFICANCE OF RENAL STAGING IN LUPUS NEPHRITIS IN RELATION TO
CLINICAL MANIFESTATIONS, KIDNEY FUNCTION AND SERUM AUTOANTIBODIES
PROFILE MEDHAT AHMAD FOUAD SHALABY, TARIK A AL-AZRAQI *, GAMAL ABDUL-AT***, ABDUL RAHMAN AL-
SHEHRI***, MAHMOUD M RABEA **** & FAYZA M MUSTAFA***** Departments of Rheumatology & Rehabilitation, Al-Azhar
University Faculty of Medicine; Internal Medicine, King Khaled University Faculty of Medicine*; Histopathology, Suez Canal University Faculty of Medicine**; Internal Medicine *** and
Nephrology****, Assier Central Hospital; and Clinical Pathology, Abesseya Chest Hospital, Cairo*****
KEY WORDS: RENAL STAGING IN LUPUS NEPHRITIS, RELATION TO CLINICAL, CHEMICAL AND SEROLOGICAL MANIFESTATIONS.
ABSTRACT Objective: To assess the significance of renal staging
in lupus nephritis in relation to clinical manifestation, kidney function and serum auto antibodies profile in patients with systemic lupus erythematosus (SLE)
Methods: Thirty-eight patients with SLE nephritis subjected to renal biopsy were included in this study. The biopsies were classified according to WHO classification for renal staging.
The activities of the disease were recorded using BILAG scoring for activity. Immunological profile include anti-dsDNA,ANA,C3,C4,Immunoglobulin G,M,A, were assessed and the kidney function includes serum creatinine,urea, 24 hours urinary protein as well as total serum protein and serum albumin were measured.
Results: There was significance increase in creatinine, 24-hour urinary protein excretion and anti-ds DNA in lupus nephritis patients than those with extra-renal lupus (controls).
Significance of Renal Staging in Lupus Nephritis Medhat Shalaby et al.
52
In comparative study between different histological classes we found a significant elevation of serum creatinine in stage V glomerulonephritis (GN). Significant increased urinary protein per 24 hours excretion in stage III and IV GN. Significant increase anti-dsDNA in stage IV GN Significant increase the incidence of renal insufficiency with stage V GN (p<0.05)
Significant positive correlation between the histological stages of lupus nephritis and renal insufficiency & serum creatinine level with insignificant positive correlation with activity score, anti-dsDNA, C3,C4, immunoglobulin level IgG,M,and A.
Conclusion: Renal biopsy and histological staging has no significant relation to other parameters of clinical activity of systemic lupus erythematousus. Close monitoring of urine for protinurea, serum creatinine levels and anti-ds DNA especially in histological stages IV & V GN of renal biopsy may play a role in prediction of renal insufficiency in lupus nephritis.
INTRODUCTION Systemic lupus erythematosus (SLE) is a chronic inflammatory
disease of unknown cause that can affect the skin, joints, kidneys, lungs, nervous system, serous membranes and/or other organs of the body. Distinct immunologic abnormalities, especially the production of a number of antinuclear antibodies, are another prominent feature of the disease. The clinical course of SLE is characterized by periods of remissions and chronic or acute relapses. Women, especially in their 20s and 30s, are affected more frequently than men. Treatment is based on preventive measures, reversal of inflammation, and prevention of organ impairment and alleviation of symptoms (1-3).
The incidence of renal involvement in SLE varies widely between different series, ranging from 29 to 53 %. (4, 5). This is partly due to different definitions of abnormal renal function, but is also dependent on how extensively the patients is investigated (6).
The kidneys are frequently involved, presumably due to autoantibody deposition at the glomerular basement membrane (GBM), which results in complement activation and attraction and influx of inflammatory cells (7). Deposition of antibodies at the GBM can occur via trapping of circulating immune complexes within the glomerulus, via
Egypt Rheumatol Rehab Vol. 30, No. 1, January 2003
53
nucleosomes that bind to the GBM and act as a substrate for autoantibody binding, or through cross-reactivity of antinuclear antibodies with glomerular structures (7).
Antibodies most closely associated with lupus nephritis are anti-dsDNA antibodies (7). The specificity of the antibody required and the mechanisms involved in the induction of renal damage in SLE remain controversial. It is also not clear whether the DNA binding specificity of antibodies alone is sufficient for glomerulonephritis to occur (8).
An abnormal urinalysis with or without an elevated plasma creatinine concentration is present in approximately 50% of patients at the time of diagnosis and eventually develops in more than 75% of cases. The most frequently observed abnormality is protienuria (80%); while approximately 40% have hematuria and/or pyuria sometimes during the course of their illness (9).
According to some reports the prognosis of patients with lupus nephritis has improved during recent years, possibly because of early and selective use of immunosuppressive therapy (10).
The role of renal biopsy for the renal prognosis in patients with lupus nephritis has been studied by several workers; some of home have found an improvement of the prognostic models when adding renal biopsy data ( 11,12,13,14), whereas others have found that renal biopsies contain redundant prognostic information ( 15 ) and conservative use of renal biopsies has been advocated ( 16 )
.
Little has been written about the correlations of clinical parameters of systemic lupus with the histopathological classification, so, our work was designed to correlate the renal staging of lupus nephritis with the clinical activity as well as the kidney function and immunological profile.
PATIENTS & METHODS Thirty eight patients chosen from the rheumatology clinic, Assir
Central hospital, Abha, Saudi Arabia, diagnosed as SLE according the revised American Collage of Rheumatology (ACR) criteria (17) with clinical and laboratory evidence of renal disease which was defined as varying combinations of the following: urine protein >0.5 g/24 h, creatinine clearance < 60 ml/min, edema requiring diuretic therapy, diastolic blood pressure >90 mmhg and serum creatinine more than 124 mmol/l (1.5 mg/dl).
All patients diagnosed histologically by renal biopsy. These biopsies were performed during the course of assessment and management of the disease. Renal biopsy was done by percutaneous puncture ultrasound
Significance of Renal Staging in Lupus Nephritis Medhat Shalaby et al.
54
guided and all renal biopsies were assessed by a pathologist and classified according to the World Health Organization (WHO) criteria as: normal (type I), mesangial alterations (type II), focal, porliferative glomerulonephritis (type III), diffuse, proliferative glomerulonephritis (type IV), diffuse, membranous glomerulonephritis (type V), and advanced, sclerosing glomerulonephritis (type VI).
Thirteen patients suffering from SLE without clinical or laboratory evidence of nephritis and not subjected to renal biopsy were chosen as control group. All patients and controls were subjected to full clinical examination and the clinical disease activity was recorded using the BILAG index records at the time of renal biopsy. The BILAG index measures clinical disease activity according to the principle of the physician's intention to treat. The index assesses separately eight organs or systems: general, mucocutanous, central nervous system, musculoskeletal, cardiovascular/respiratory, vascular, and renal and hematological. Each system is allocated alphabetic scores (A-E) according to the presence or absence of variety of clinical features (mostly) in each organ system: A=disease that requires urgent disease-modifying therapy; B=disease that demands close attention and perhaps modification of minor therapy, e.g. antimalarial or non-steroidal anti-inflammatory drugs, or prednisolone < 20 mg/day; C=stable mild disease; D=system previously affected but currently inactive; E=system never involved. Global disease activity was calculated for each assessment, using the system A = 9, B = 3, C = 1, D = 0, and E = 0.Clinical active disease considered when global score more than six (>6).
The laboratory investigations in this study at the time of biopsy included the following; ESR, complete blood picture, serum urea and creatinine, 24 hours urinary protein excretion (gr/day), urine analysis for the presence of microscopic hematuria and sediment, total serum protein, serum albumin, serum complement 3and 4(C3 & C4) ,serum immunoglobulin G, M & A, anti-dsDNA and ANA. The subsequent therapy was also recorded.
Statistical Methods: Differences in the group means of the continuous variables were
tested by the non-parametric tests of Wilcoxon or Mann Whitney. Qualitative data were compared by the chi-square test. Correlations between the continuous and grouped data were performed by Spearman's rank correlation test. The test results were considered statistically significant when corresponding p value were <0.05. Data were analyzed using SPSS program, version 8.
Egypt Rheumatol Rehab Vol. 30, No. 1, January 2003
55
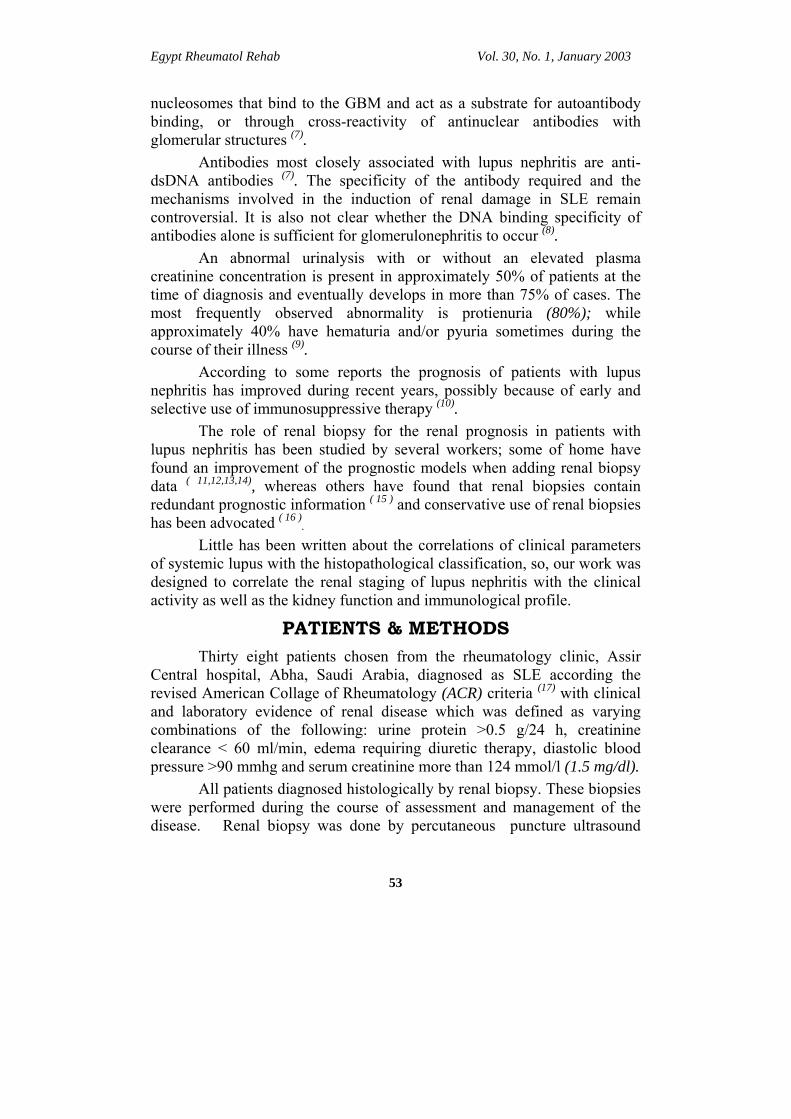
RESULTS Table (I): Patients and controls characteristics at the time of biopsy.
SLE with nephritis SLE without nephritis
Total number 38 13 Sex M/F 3/35 1/12 Age in years Mean + SD 26.5 +0.5 29.3 + 11.4 Duration of SLE (months). Mean + SD 43.5 (28.8) 44.7(31.7) Duration of Renal disease (months) Mean + SD 26.9(19) 0 24-h urinary protein (mg). Mean + SD 1785.9 (2003) 207.7 (173.6)* Total serum protein (umol/l) Mean + SD 6.8 (1.3) 7.2 (2.1) Serum albumin (umol/l) Mean + SD 3.1 (0.7) 3.3 (0.7) Serum creatinine (umol/l) Mean + SD 1.9 (1.2) 0.72 (0.29)* DNA Mean + SD 680 (1247.3) 393.3 (486.9)* ANA Mean + SD 2002.9 (1811.1) 1341 (1152.7) C3 Mean + SD 58.9 (36.2) 50.9 (14.5) C4 Mean + SD 19.1 (20.9) 12.6 (4.3) IgG Mean + SD 1891.4 (764.6) 1857.2 (435.7) IgM Mean + SD 245 (84.4) 225.7(46.9) IgA Mean + SD 318.9 (116.1) 330.7(57.1)
WHO Classification for Nephritis Class II, n (%) GN 11 (28.9) Class III, n (%) GN 11 (28.9) Class IV, n (%) GN 9 (23.9) Class V, n (%) GN 7 (18.4) Initial renal insufficiency n (%) 4 (10.5) 0(0%)
Medical treatment: Steroid use n (%) 38(100) 13(100) Steroid + cyclophosphamide n (%) 14(36.8) 4(30.8) Steroid + azathioprin n (%) 4(10.5) 2(15.4)
Steroid + Antimalarial use n (%) 21(55.3) 11(84.6)
* p<0.05
Thirty eight patients suffering from lupus nephritis subjected to renal biopsy were included in this study and 13 patients suffering from SLE without evidence of nephritis representing the control group. The features of the study and control group were summarized in table (1).
Statistically, the serum creatinine, anti-DsDNA as well as 24 hours urinary protein results were significantly higher in SLE patients with nephritis than the control group (SLE without nephritis).
Significance of Renal Staging in Lupus Nephritis Medhat Shalaby et al.
56
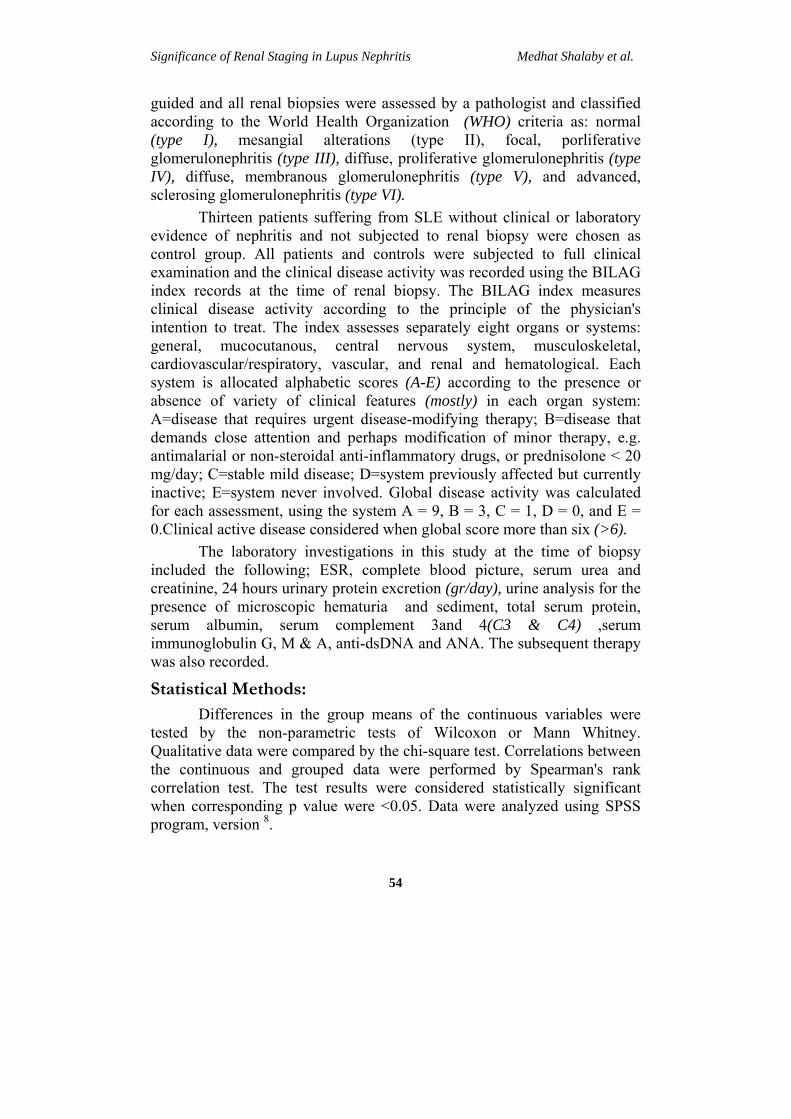
Table (2): Number of patients with active disease in organ/system assessed by BILAG score. Patients Controls No. % No. % General 33 86.9 11 84.6 Mucocutaneous 30 78.9 9 69.2 Central nervous system 6 15.8 4 30.8 Musculoskeletal 28 73.7 12 92.3 Cardiovascular/respiratory 11 28.9 6 46.2 Vasculitis 11 28.9 2 15.4 Renal 18 47.4 0 0 Hematological 26 68.4 4 30.8 Clinically active SLE 38 100 13 100 (Global score>6) BILAG score for activity 24.4+4.6 25+6.8
Correlation study results: In the study group, there was significant positive correlation
between renal staging and serum creatinine (p<0.05), 24/h urinary albumin (p<0.05) and treatment score (p<0.01) and significant negative correlation with total serum protein (p<0.05) and serum albumin (p<0.05).
There was a significant positive correlation between complement C3 and C4 (p<0.01). Significant positive correlation between anti-DsDNA and ANA (p<0.05).
In the control group: There was significant positive correlation between total serum protein and serum albumin (p<0.05). Statistical Results: Statistical results showed no significant differences between the study and control groups and correlation study found a significant positive correlation between the activity score and ESR and significant negative correlation with serum hemoglobin level (p<0.5)
Egypt Rheumatol Rehab Vol. 30, No. 1, January 2003
57
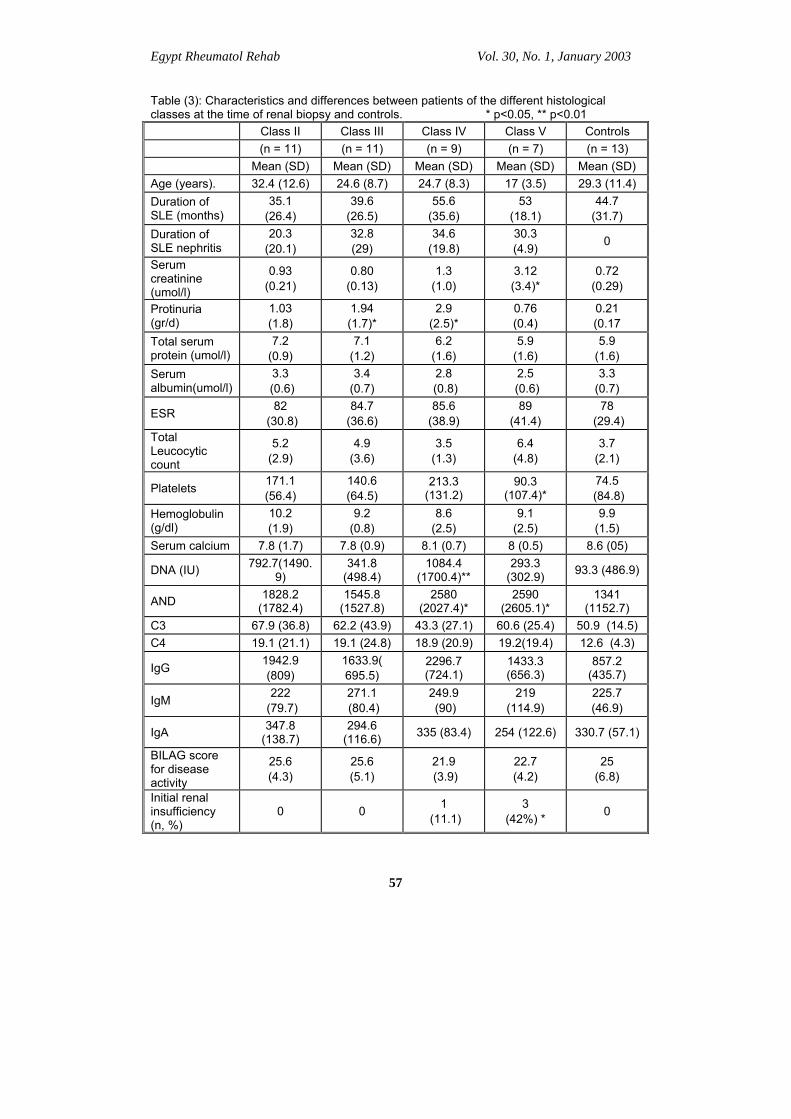
Table (3): Characteristics and differences between patients of the different histological classes at the time of renal biopsy and controls. * p<0.05, ** p<0.01 Class II Class III Class IV Class V Controls (n = 11) (n = 11) (n = 9) (n = 7) (n = 13) Mean (SD) Mean (SD) Mean (SD) Mean (SD) Mean (SD) Age (years). 32.4 (12.6) 24.6 (8.7) 24.7 (8.3) 17 (3.5) 29.3 (11.4) Duration of SLE (months)
35.1 (26.4)
39.6 (26.5)
55.6 (35.6)
53 (18.1)
44.7 (31.7)
Duration of SLE nephritis
20.3 (20.1)
32.8 (29)
34.6 (19.8)
30.3 (4.9) 0
Serum creatinine (umol/l)
0.93 (0.21)
0.80 (0.13)
1.3 (1.0)
3.12 (3.4)*
0.72 (0.29)
Protinuria (gr/d)
1.03 (1.8)
1.94 (1.7)*
2.9 (2.5)*
0.76 (0.4)
0.21 (0.17
Total serum protein (umol/l)
7.2 (0.9)
7.1 (1.2)
6.2 (1.6)
5.9 (1.6)
5.9 (1.6)
Serum albumin(umol/l)
3.3 (0.6)
3.4 (0.7)
2.8 (0.8)
2.5 (0.6)
3.3 (0.7)
ESR 82 (30.8)
84.7 (36.6)
85.6 (38.9)
89 (41.4)
78 (29.4)
Total Leucocytic count
5.2 (2.9)
4.9 (3.6)
3.5 (1.3)
6.4 (4.8)
3.7 (2.1)
Platelets 171.1 (56.4)
140.6 (64.5)
213.3 (131.2)
90.3 (107.4)*
74.5 (84.8)
Hemoglobulin (g/dl)
10.2 (1.9)
9.2 (0.8)
8.6 (2.5)
9.1 (2.5)
9.9 (1.5)
Serum calcium 7.8 (1.7) 7.8 (0.9) 8.1 (0.7) 8 (0.5) 8.6 (05)
DNA (IU) 792.7(1490.9)
341.8 (498.4)
1084.4 (1700.4)**
293.3 (302.9) 93.3 (486.9)
AND 1828.2 (1782.4)
1545.8 (1527.8)
2580 (2027.4)*
2590 (2605.1)*
1341 (1152.7)
C3 67.9 (36.8) 62.2 (43.9) 43.3 (27.1) 60.6 (25.4) 50.9 (14.5) C4 19.1 (21.1) 19.1 (24.8) 18.9 (20.9) 19.2(19.4) 12.6 (4.3)
IgG 1942.9 (809)
1633.9( 695.5)
2296.7 (724.1)
1433.3 (656.3)
857.2 (435.7)
IgM 222 (79.7)
271.1 (80.4)
249.9 (90)
219 (114.9)
225.7 (46.9)
IgA 347.8 (138.7)
294.6 (116.6) 335 (83.4) 254 (122.6) 330.7 (57.1)
BILAG score for disease activity
25.6 (4.3)
25.6 (5.1)
21.9 (3.9)
22.7 (4.2)
25 (6.8)
Initial renal insufficiency (n, %)
0 0 1 (11.1)
3 (42%) * 0
Significance of Renal Staging in Lupus Nephritis Medhat Shalaby et al.
58
Comparative study between the histological stages of SLE nephritis patients as well as the controls showed the following:
• Significant elevation of serum creatinine in stage V glomerulonephritis (GN) (p<0.05) • Significant increased urinary protein per 24 hours in stage III and IV GN (p<0.05) • Significant increase anti dsDNA in stage IV GN (p<0.01) • Significant increase ANA in stage VI & V GN (P<0.05) • Significant increase the incidence of renal insufficiency with stage V GN (p<0.05) • Significant positive correlation between the histological stages of lupus nephritis and renal insufficiency & serum creatinine level and insignificant positive correlation with activity score, anti ds DNA, C3,C4, immunoglobulin level IgG, M, and A,
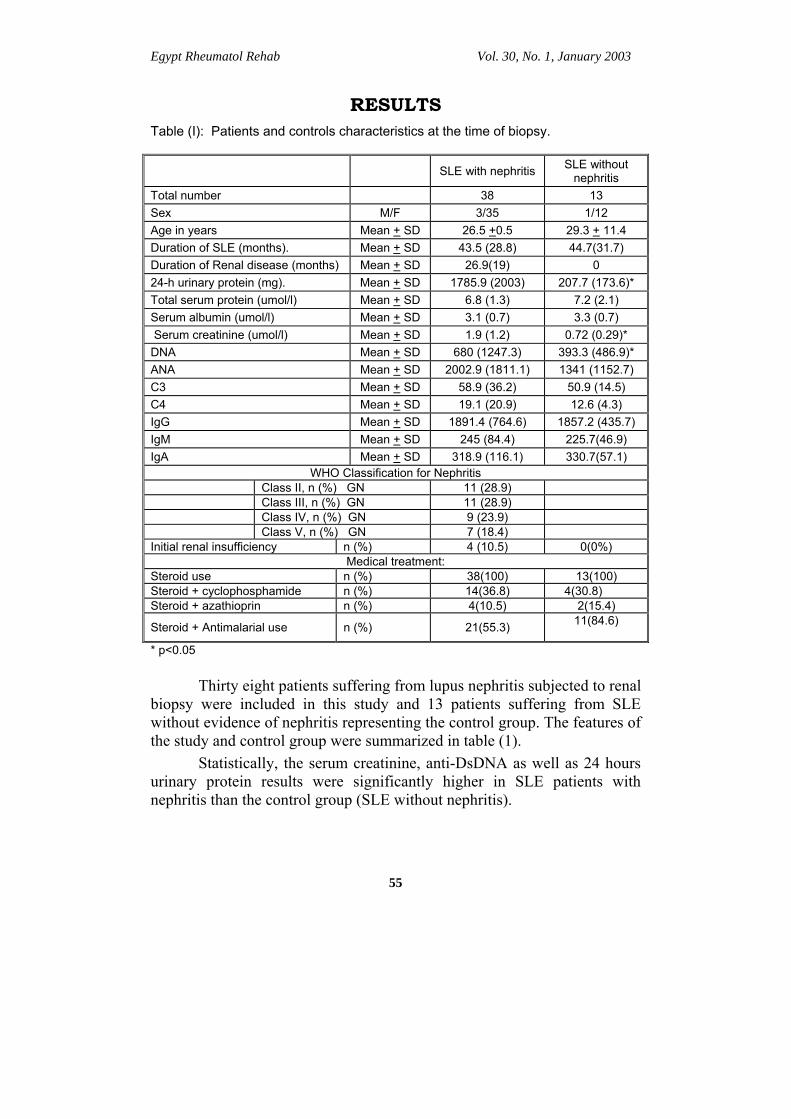
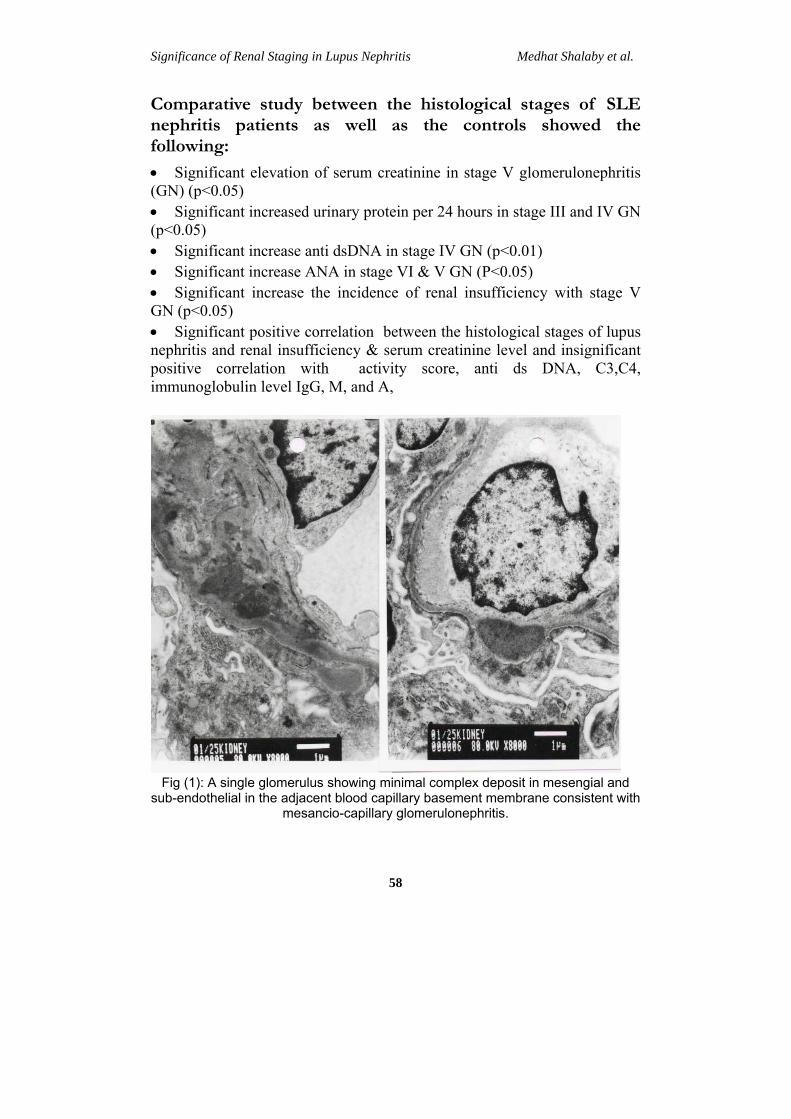
Fig (1): A single glomerulus showing minimal complex deposit in mesengial and
sub-endothelial in the adjacent blood capillary basement membrane consistent with mesancio-capillary glomerulonephritis.
Egypt Rheumatol Rehab Vol. 30, No. 1, January 2003
59
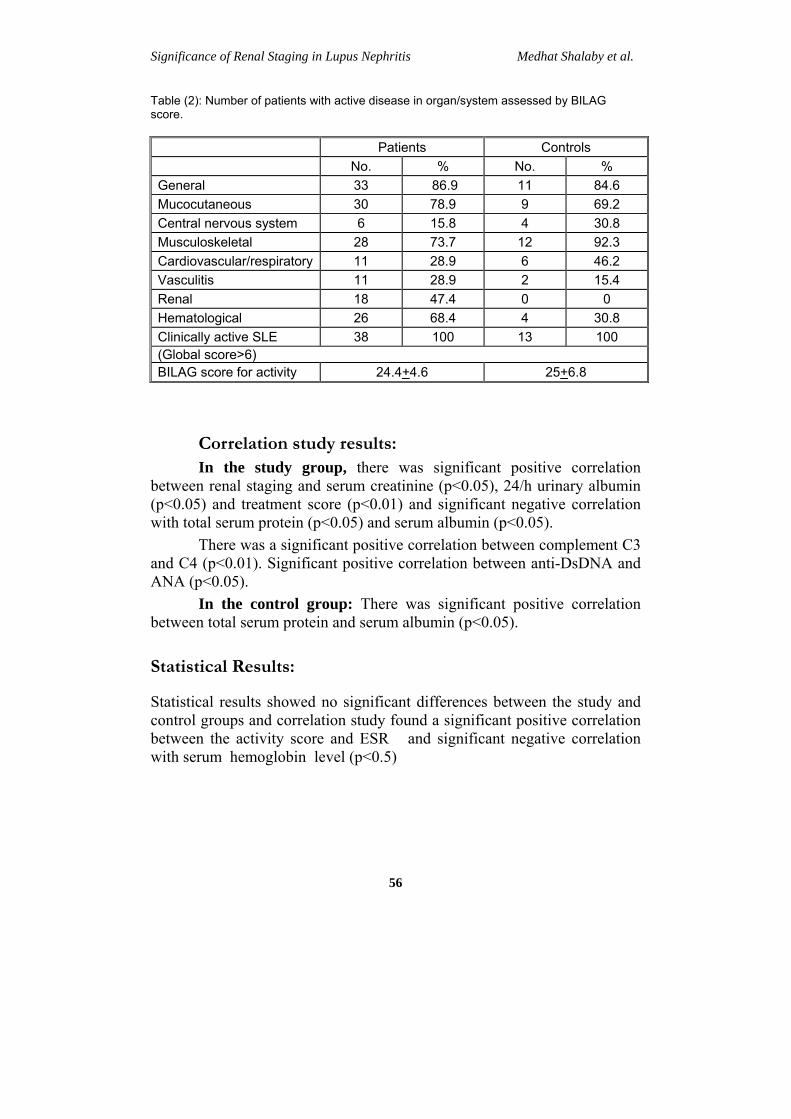
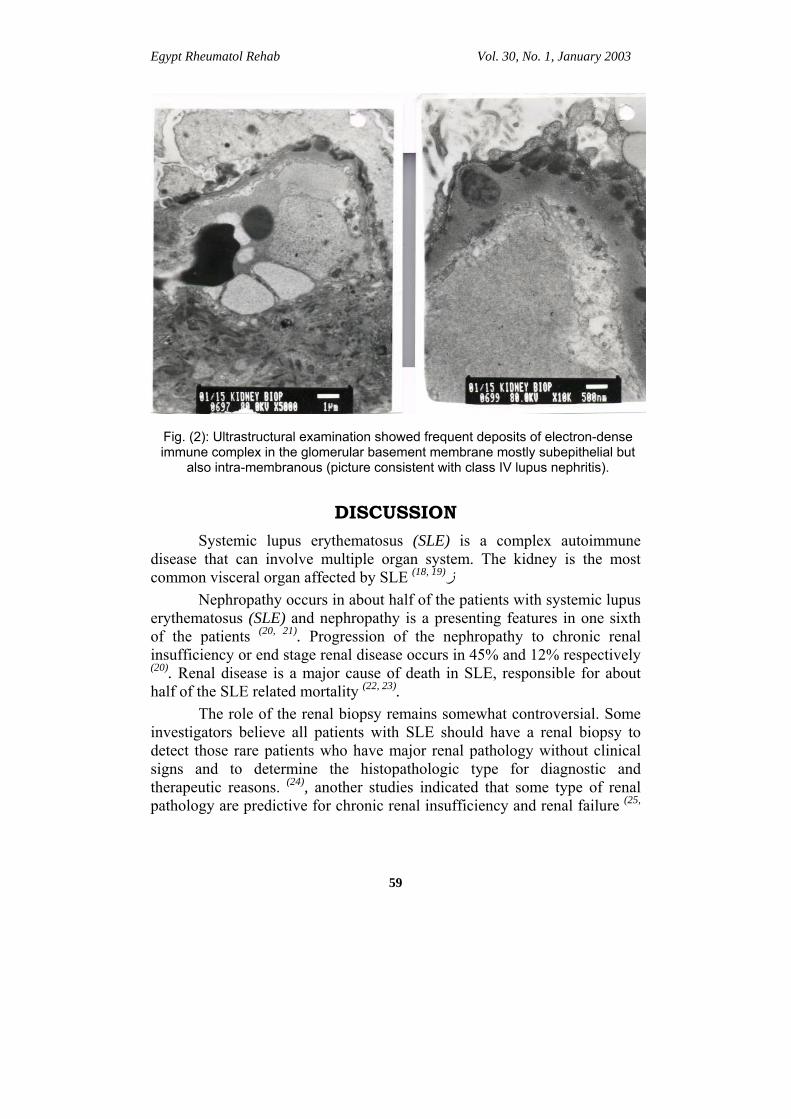
Fig. (2): Ultrastructural examination showed frequent deposits of electron-dense immune complex in the glomerular basement membrane mostly subepithelial but
also intra-membranous (picture consistent with class IV lupus nephritis).
DISCUSSION Systemic lupus erythematosus (SLE) is a complex autoimmune
disease that can involve multiple organ system. The kidney is the most common visceral organ affected by SLE (18, 19)ز
Nephropathy occurs in about half of the patients with systemic lupus erythematosus (SLE) and nephropathy is a presenting features in one sixth of the patients (20, 21). Progression of the nephropathy to chronic renal insufficiency or end stage renal disease occurs in 45% and 12% respectively (20). Renal disease is a major cause of death in SLE, responsible for about half of the SLE related mortality (22, 23).
The role of the renal biopsy remains somewhat controversial. Some investigators believe all patients with SLE should have a renal biopsy to detect those rare patients who have major renal pathology without clinical signs and to determine the histopathologic type for diagnostic and therapeutic reasons. (24), another studies indicated that some type of renal pathology are predictive for chronic renal insufficiency and renal failure (25,
Significance of Renal Staging in Lupus Nephritis Medhat Shalaby et al.
60
26). Others however showed that information about renal pathology did not improve the prognostic value of routine laboratory test (27).
However, our study was done on SLE nephritis patients to signify the importance of renal staging in correlation with the disease activity and autoimmune profile by analyzing the renal pathology and laboratory finding of those patients.
All our patients (SLE with nephritis) and the control group (SLE without nephritis) had clinically active lupus (i.e. global score > 6), comparative study between both groups showed significant elevation anti-ds DNA as well as serum creatinine and twenty four hours urinary protein excretion in the study group than the control group (p<0.05).
Bijl et al, 2002, stated that IgG2 anti-ds DNA were more frequently present in patients with renal disease compared with those with extra renal disease (28). Sasaki et al, 1991, suggested that anti-DNA circulating immune complex (CIC) preferentially occur in lupus patients with diffuse proliferative glomerulonephritis (DPGN). In our study we found a significant increase
In anti-ds DNA in those patients with nephritis than the control group and significantly increased in class IV GN (29).
Although we found in our study a significant increase in the serum creatinine level in class V GN, Mitjavila et al.,( 1997) in their study failed to find this association and he didn't found significance difference in creatinine between the different histological classes at the moment of the diagnosis although the WHO classification correlated well with protinuria and immunologic activity. Also he stated that high immunologic activity, mainly elevated anti-DNA titers and decreased level of CH100 (total hemolytic activity of complement) is highly suggestive of proliferative glomerulonephritis (30).
Different measures have been developed to assess the SLE disease activity, disease severity, and cumulative disease damage. The assessment of disease activity is important for the management of patients, both to direct necessary changes in medical treatment and to assess the impact of disease on the patients (31). For disease activity we used the British Isles Lupus Assessment Group index (BILAG) and we tried to correlate between the activity score and the different stages for SLE nephritis and the immunological profile (anti dsDNA, C3,C4) .Our results showed insignificant positive correlation.
The prognostic significant value of renal biopsy remains controversial. Bajaj et al, 2000 demonstrated the usefulness of renal biopsy
Egypt Rheumatol Rehab Vol. 30, No. 1, January 2003
61
in predicting mortality and endstage renal disease. They also accepted that renal biopsy had a role in the management of lupus nephritis (32), while others suggested that there is only marginal benefit from the biopsy (15, 33, and
34). Anyhow, the prognostic value of the 1982 WHO classification has
progressively declined probably due to transformation of nephritis patterns and better use of immunosuppressive therapy (35-37).
Austin et al, 1984 found in their study that patients with diffuse proliferative GN who manifested severe active or marked chronic parenchymal injury had a 40% probability of end stage kidney disease after five years of observation (38) and in another study done by Austin et al 1994, he found that renal insufficiency developed in 19 of 56 patients with diffuse proliferative GN, and in two of three patients with mixed membranous and proliferative nephropathy (39).
In this work, comparative study between the different stages of lupus nephritis found a significance increase incidence of renal insufficiency in class V GN (3 patients out of 9) and one patient with class IV, GN. We also found a significant positive correlation between the renal insufficiency and elevated serum creatinine.
Conclusion: Since nephritis may occur at any time of the course of SLE, close
monitoring of urine analysis for protinuria, serum creatinine level as well as anti-DsDNA remains warranted in the long term follow up of SLE patients. Renal biopsy, although we didn't found positive correlation with the disease activity will remain a good predictors for the occurrence of renal insufficiency especially class IV and Class V.
Acknowledgement: To Professor Ahmed Mahfouz Professor of Epidemiology,
Alexandria University, for his significant guidance and great effort in doing the statistical part of this study.
REFERENCES 1- Boumpas DT, Austin HA III, Fessler BJ, et al. (1995): Systemic lupus
erythematosus: Emerging concepts. Part1: renal, neuropsychiatric, cardiovascular, pulmonary, and hematologic disease. Ann Intern Med 122:940
2- Boumpas DT, Austin HA III, Fessler BJ, et al. (1995): Systemic lupus erythematosus Emerging concepts. Part 2: Dermatologic and joint disease,
Significance of Renal Staging in Lupus Nephritis Medhat Shalaby et al.
62
the antiphospholipid antibody syndrome, pregnancy and hormonal therapy, morbidity and mortality and pathogenesis. Ann Intern Med123:42.
3- Mills JA (1994): Systemic lupus erythematosus. N Engl J Med 330:1871. 4- Worrall JG, Snaith ML, and Batchelor JR, Isenberg DA (1990): SLE: a
rheumatological view. Analysis of the clinical features, serology and immunogenetics of 100 SLE patients during long-term follow-up Q J Med 74:319-30.
5- Estes D, Christian C (1971): The natural history of systemic lupus erythematosus. Medicine 50:85-95.
6- Moss KE, Isenberg DA (2001): Comparison of renal disease severity and outcome in patients with primary antiphospholipid syndrome, antiphospholipid syndrome secondary to systemic lupus erythematousus (SLE) and SLE alone. Rheumatology 40:863-867
7- Lefkowith JB, Gilkeson GS (1996): Nephritogenic autoantibodies in lupus: current concepts and continuing controversies. Arthritis Rheum 39:894-903.
8- Ravirrajan CT, Rahman MA, Papadaki L et al. (1998): Genetic, structural and functional properties of an IgG DNA-binding monoclonal antibody from a lupus patient with nephritis . Eur J Immunol 28:339-50.
9- Rothfield N (1981): Clinical features of SLE. In: Textbook of Rheumatology, Kelly, WN, et al (Eds), WB Saunders, Philadelphia.
10- Tan EM, Cohen AS, Fries JF (1982): The 1982 revised criteria for the classification of systemic lupus erythematosus (SLE) Arthritis Rheum 25:1271-1
11- Esdaile JM, Abrahamowicz M, Mackenize T, Hayslett JP, Kashgarian M (1994): The time-dependence of long term prediction in lupus nephritis Arthritis Rheum 37:359-68
12- Austin HA, Muenz LR, Joyce KM, Antonovych TT, Kullick ME, Klippel JH, et al. (1983): Prognostic factors in lupus nephritis.Contribution of renal histologic data Am J Med 75:382-91
13- Magil AB, Buterman ML, Ballon HS, Chan V, Lirenman DS, Rae A, et al. (1988): Prognostic factors in diffuse proliferative lupus glomerulonephritis. Kidney Int 34:511-517
14- Bakir AA, Levy PS, Dunea G (1994): The prognosis of lupus nephritis in African-Americans: a retrospective analysis. Am J Kidney Dis 24:159-71
15- Fries JF, Prota J, Liang MH (1978): Marginal benefit of renal biopsy in systemic lupus erythematousus. Arch Intern Med 138:1385-9
16- Salach RH, Cash JM (1996): Managing lupus nephritis: algorithms for conservative use of renal biopsy. Cleve Clin J Med 63:106-15
17-Tan EM, Cohen AS, Fries JF et al. (1982): The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 25:1271-7.
Egypt Rheumatol Rehab Vol. 30, No. 1, January 2003
63
18- Golbus J, McCune WJ (1994): Lupus nephritis: classification, prognosis, immunopathogenesis, and treatment. Rheum Dis Clin North Am 20:213-242
19- Boumpas DT, Austin HA, Fessler BJ, Balow JE, Klippel JH, Lockshin MD (1995): Systemic lupus erythematousus: emerging concepts. I. Renal, neurospychatric, cardiovascular, pulmonary, and hematologic disease. Ann Intern Med 122:940-950
20-Jacobsen S, Petersen J, Ullman S, Junker P, Voss A, Rasmussen JM, et al. (1998): A multicenter study of systemic lupus erythematosus in 513 Danish patients. I: Disease manifestations and analyses of clinical subsets. Clin Rheumatol 17:468-77.
21-Cervera R, Khamasthta MA, Font J, Sebastiani GD, Gil A, Lavilla P, et al. (1993): Systemic lupus erythematosus: clinical an immunological patterns of disease expression in a cohort of 1000 patients. Medicine 72:113-24
22 -Jacobsen S, Petersen J, Ullman S, Junker P, Voss A, Rasmussen JM, et al. (1998): A multicenter study of systemic lupus erythematousus in 513 Danish patients. II Mortality and factors of prognostic value Clin Rheumatol 17:478-84
23- Jacobsen S, Petersen J, Ullman S, Junker P, Voss A, Rasmussen JM, et al. (1999): Mortality and cause of death of 513 Danish patients with systemic lupus erythematousus. Scand. J Rheumatol 28:75-80
24-Golbus J & McCune J (1994): Lupus nephritis; classification,prognosis, immunopathogenesis and treatment. Rheum Disease clinics N America 20(1):213-242
25- Appel GB, Cohen DJ, Pirani CL, Meltzer JI, Estes D (1987): Long term follow-up of patients with lupus nephritis. A study based on the classification of the World Health Organization. Am J Med 83:877-85
26- Esdaile JM, Levinton C, Federgreen W, Hayslett JP, Kashgarian M (1989): The clinical and renal biopsy predictors of long-term outcome in lupus nephritis: a study of 87 patients and review of the literature. Q J Med 72:779-833
27- Donadio JV, Hart GM, Bergstralh EJ, Holley KE (1995): Prognostic determinants in lupus nephritis: a long term clinicopathologic study. Lupus4:109-15
28- Bijl M, Dijstebloem HM, Oast WW, Bootsma H, Derksen RH, WM, Aten J, Limburg PC, and Kallenberg CGM (2002): IgG subclass distribution of autoantibodies differ between renal and extrarenal relapses in patients with systemic lupus erythematosus.Rheumatology 42:62-67
29- Sasaki T, Muryoi T, Hatakeyam A, Suzuki M, Sato H, Seinio J, Saito T, Yoshinaga K (1991): Circulating Anti-DNA Immune complexes in active lupus nephritis.. Am J med91:355-62
Significance of Renal Staging in Lupus Nephritis Medhat Shalaby et al.
64
30- Mitjavila F, Pac V, Moga I, Poveda R, Vidaller A, Carrera M, Pujol R (1997): Clinicopathological correlations and prognostic factors in lupus nephritis. Cl Exp Rheum. 15:625-631
31- Brunner HI, Feldman BM, Bombrdier C, and Silverman ED (1999): Sensetivity of the Systemic Lupus Erythematousus Disease Activity Index, British Isles Assessment Group Index, and Systemic Lupus Activity Measure in the evaluation of clinical change in childhood-onset systemic lupus erythematousus. Arthritis & Rheumatism 42(7)1354-1360
32- Bajaj S, Albert L, Gladman DD, Urowitz MB, Hallett DC, and Ritchie S (2000): Serial renal biopsy in systemic lupus erythematousus. Rheumatology 27(12)2822-26
33- Whiting-O'Keefe Q, Riccardi PJ, Henke JE, Shearn MA, Hopper J, Epstein WW (1982): Recognition of information in renal biopsies of patients with lupus nephritis. Ann Intern Med 96:723-7
34- Wallacve DJ, Podell TE, Wiener JM, et al. (1982): Lupus nephritis: experience with 230 patients in private practice from 1950-1980. Am J Med 72:209-20
35- Cameron JS, Turner DR, Ogg C, Williams DG, Lessof MH, Chantler C, Leibowitz S (1979): Systemic lupus erythematousus with nephritis: A long term study.Q J Med 48:1-24
36- McLaughlin JR, Gladman DD, Urowitz MB, Bombardier C, Farewell VT, Cole E (1991): Kidney biopsy in systemic lupus erythematousus. II. Survival analysis according to biopsy results Arthritis Rheum 34:1266-73
37- Yang LY, Chen WP, Lin CY (1994): Lupus nephritis in children. A review of 167 patients Pediatrics 94:335-40
38- Austin HA, Muenz LR, Joyce KM, Antonovych TT, Balow JE (1984): Diffuse proliferative lupus nephritis: Identification of specific pathologic features affecting renal outcome. Kidney Int 25:689-695
39- Austin HA, Boumpas DT, Vaughan EM, and Balow JE (1994): Predicting renal outcomes in severe lupus nephritis:Contributions of clinical and histologic data. Kidney Int 45:544-550
أهمية التقسيم النسيجي في مرضى الذئبة الحمراء الكلوي وعالقتها ووظائف الكلى والتغيرات المناعية بالدمةآلينيكيإلباألعراض ا
وي راء الكل ة الحم انون من مرض الذئب أجرى هذا البحث على ثمانية وثالثون مريضا يعم عمل ذلك ت ا آ تم عمل تقسيم نسيجي لهم بعد اخذ عينة من الكلى ولقد تم مناظرة المرضى إآلينيكيائج اإلحصائية عدم وجود د أظهرت النت اعي ولق از المن ى والجه الفحوصات الخاصة بوظائف الكل
ن التقسيم النسيجي والنشاط المرضى و لكن وجدت عالقة ذات داللة إحصائية مع وظائف عالقة بي الكلى وآذلك التغيرات المناعية بالدم