Embed Size (px)
Citation preview

Il trattamento delle aritmie in età geriatrica
Stefano Fumagalli Cardiologia e Medicina Geriatrica, AOU Careggi e Università di Firenze
Simposio
NUOVE TECNOLOGIE IN TEMA DI
CARDIOPATIE DELL’ANZIANO PER IL
TRATTAMENTO DELLE ARITMIE E DELLE
VALVULOPATIE
Il trattamento delle aritmie in età geriatrica
Simposio
NUOVE TECNOLOGIE IN TEMA DI CARDIOPATIE DELL’ANZIANO
PER IL TRATTAMENTO DELLE ARITMIE E DELLE VALVULOPATIE
Premesse

QRS di normale morfologia
ECG in assenza di terapia in una paziente di 83 anni
Presenza di fibrillazione atriale ad elevata risposta ventricolare media (FC: 95-120
b/min); PA 160/100 mmHg

PA 150/70 mmHg; FC 72 b/min. ECG – ritmo sinusale, BAV I grado
(PR: 250 ms); comparsa di BBS (QRS: 240 ms)
ECG dopo assunzione di propafenone 600 mg “pill-in-the-
pocket” La paziente ha preso due volte la terapia, emozionata per l’arrivo dei familiari.
Comparsa di astenia, senso di vertigine e quindi presincope, giunge in DEA …

Pro
ba
bilit
y o
f d
ea
th
Years
55% -
AAD >75 y
33% -
AAD 65-75 y
.....................................................................................................................................................................................
.....................................................................................................................................................................................
CLIN ICAL RESEARCHAtrial fibrillation
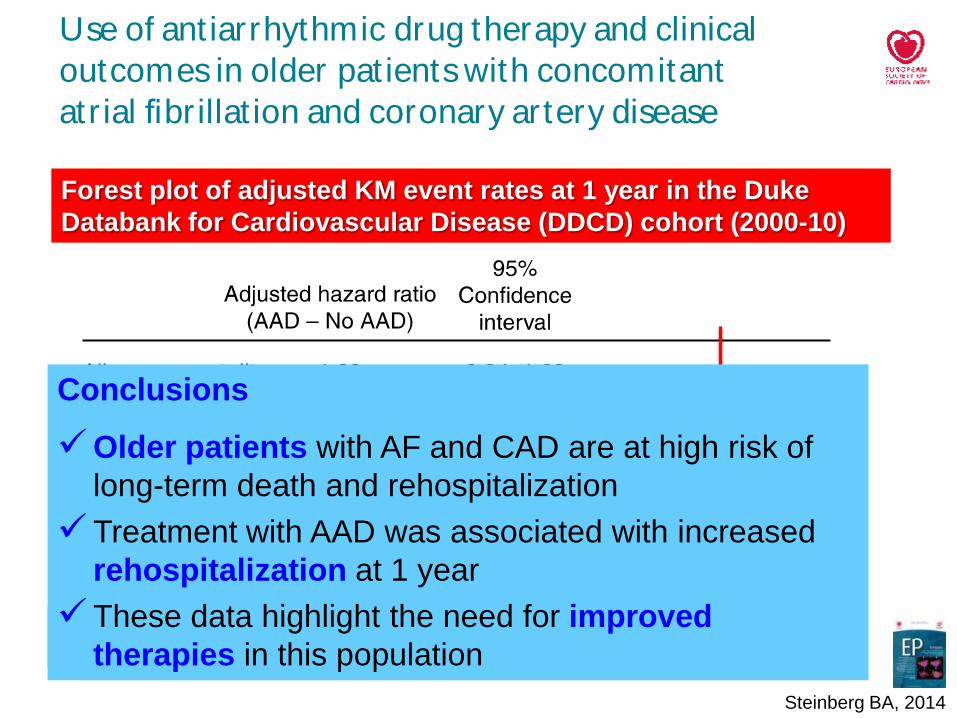
Use of ant iarrhythmic drug therapy and clinical
outcomes in older pat ientswith concomitant
atr ial fibrillat ion and coronary artery disease
Benjamin A. Steinberg1,2,3*, Samuel H. Broder ick3, Renato D. Lopes2,3, Linda K. Shaw3,
Kevin L. Thomas1,2,3, Tracy A. DeW ald2, James P. Daubert 1,2,3, Er ic D. Peterson2,3,
Chr istopher B. Granger 2,3, and Jonathan P. Piccini1,2,3
1Duke Center for Atrial Fibrillation, Durham, NC, USA; 2Department of Medicine, Duke University Medical Center, Durham, NC, USA; and 3Duke Clinical Research Institute,
Duke University Medical Center, PO Box 17969, Durham, NC 27715, USA
Received 12 December 2013;accepted after revision 17 March 2014;online publish-ahead-of-print 21 April 2014
A im s Atrial fibrillation(AF) andcoronaryarterydisease(CAD) arecommoninolder patients.Weaimedto describetheuseof
antiarrhythmic drug(AAD) therapy and clinical outcomes in these patients.
Met hods
and r esult s
Weanalysed AAD therapyand outcomesin1738 older patients(age ≥ 65) with AFand CAD in theDukeDatabank for
cardiovascular disease. The primary outcomes were mortality and rehospitalization at 1 and 5 years. Overall, 35%of
patients received an AAD at baseline, 43%were female and 85%were white. Prior myocardial infarction (MI, 31%)
and heart failure (41%) were common. Amiodarone was the most common AAD (21%), followed by pure Class III
agents(sotalol 6.3%, dofetilide 2.2%). Persistence of AAD waslow (35%at 1 year). After adjustment, baseline AAD use
wasnot associatedwith1-year mortality [adjustedhazardratio (HR) 1.23,95%confidenceinterval (CI) 0.94–1.60] or car-
diovascular mortality (adjusted HR1.27,95%CI 0.90–1.80). However, AAD usewasassociated with increased all-cause
rehospitalization (adjusted HR1.20, 95%CI 1.03–1.39) and cardiovascular rehospitalization (adjusted HR1.20, 95%CI
1.01–1.43) at 1 year. Thisassociation did not persist at 5 years; however, these patientswere at very high risk of death
(55%for those . 75 and on AAD) and all-cause rehospitalization (87%for those . 75 and on AAD) at 5 years.
Conclusions In older patients with AFand CAD, antiarrhythmic therapy was associated with increased rehospitalization at 1 year.
Overall,thesepatientsareat highriskof longer-termhospitalizationanddeath.Safer,better-tolerated,andmoreeffective
therapies for symptom control in thishigh-risk population arewarranted.- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywor ds Atrial fibrillation † Ischaemic heart disease † Antiarrhythmic drug † Elderly † Outcomesresearch
Atrial fibrillation (AF) isthe most common dysrhythmia in adults,
and its incidence increases significantly with age. Ultimately, more
than one in four persons over the age of 40 will be diagnosed with
AF and 10% of octogenarians carry a diagnosis of AF.1,2 Atrial
fibrillation has a negative impact on the quality of life comparable
with that observed in patients with ischaemic heart disease, and
the effect is largely attributable to significant symptoms including
palpitations, fatigue, and exertional limitations.3,4 Randomized
data have suggested that maintenance of sinus rhythm (‘rhythm
control’) isassociated with improved symptoms.5,6
However,antiarrhythmic drug(AAD) therapyinpatientswithcor-
onary artery disease (CAD) raisesseveral safety concerns, including
toxic side effects and the potential for fatal proarrhythmia.7–9 Yet
most of the evidence in the literature is derived from selected
populationsand few dataare available in older patients. In an effort
to assess the effects of AAD on clinical outcomes in older patients
with AF and CAD, we performed an analysis of patients in the
Duke Databank for Cardiovascular Disease. The objectives of this
study were (i) to describe the use of AADs in older patients
with AF and CAD, (ii) to assess clinical outcomes in these
* Correspondingauthor. Tel: + 1 919 668 8686; fax: + 1 877 991 8498. E-mail address: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2014. For permissionsplease email: [email protected].
Europace (2014) 16, 1284–1290
doi:10.1093/europace/euu077
at Un
iversitÃ
deg
li Stu
di d
i Firen
ze on S
eptem
ber 2
5, 2
014
http
://euro
pace.o
xfo
rdjo
urn
als.org
/D
ow
nlo
aded
from
Steinberg BA, 2014
Unadjusted KM event rates for all-cause mortality in the Duke
Databank for Cardiovascular Disease (DDCD) cohort (2000-10)
N=1738, Age: 74 years 65-75 y: 55%; >75y: 45%
AAD - 65-75 y: 33%; >75y: 55%
Amiodarone: ≈60%
P-value <0.001
.....................................................................................................................................................................................
.....................................................................................................................................................................................
CLIN ICAL RESEARCHAtrial fibrillation
Use of ant iarrhythmic drug therapy and clinical
outcomes in older pat ientswith concomitant
atr ial fibrillat ion and coronary artery disease
Benjamin A. Steinberg1,2,3*, Samuel H. Broder ick3, Renato D. Lopes2,3, Linda K. Shaw3,
Kevin L. Thomas1,2,3, Tracy A. DeW ald2, James P. Daubert 1,2,3, Er ic D. Peterson2,3,
Chr istopher B. Granger 2,3, and Jonathan P. Piccini1,2,3
1Duke Center for Atrial Fibrillation, Durham, NC, USA; 2Department of Medicine, Duke University Medical Center, Durham, NC, USA; and 3Duke Clinical Research Institute,
Duke University Medical Center, PO Box 17969, Durham, NC 27715, USA
Received 12 December 2013;accepted after revision 17 March 2014;online publish-ahead-of-print 21 April 2014
A im s Atrial fibrillation(AF) andcoronaryarterydisease(CAD) arecommoninolder patients.Weaimedto describetheuseof
antiarrhythmic drug(AAD) therapy and clinical outcomes in these patients.
Met hods
and r esult s
Weanalysed AAD therapyand outcomesin1738 older patients(age ≥ 65) with AFand CAD in theDukeDatabank for
cardiovascular disease. The primary outcomes were mortality and rehospitalization at 1 and 5 years. Overall, 35%of
patients received an AAD at baseline, 43%were female and 85%were white. Prior myocardial infarction (MI, 31%)
and heart failure (41%) were common. Amiodarone was the most common AAD (21%), followed by pure Class III
agents(sotalol 6.3%, dofetilide 2.2%). Persistence of AAD waslow (35%at 1 year). After adjustment, baseline AAD use
wasnot associatedwith1-year mortality [adjustedhazardratio (HR) 1.23,95%confidenceinterval (CI) 0.94–1.60] or car-
diovascular mortality (adjusted HR1.27,95%CI 0.90–1.80). However, AAD usewasassociated with increased all-cause
rehospitalization (adjusted HR1.20, 95%CI 1.03–1.39) and cardiovascular rehospitalization (adjusted HR1.20, 95%CI
1.01–1.43) at 1 year. Thisassociation did not persist at 5 years; however, these patientswere at very high risk of death
(55%for those . 75 and on AAD) and all-cause rehospitalization (87%for those . 75 and on AAD) at 5 years.
Conclusions In older patients with AFand CAD, antiarrhythmic therapy was associated with increased rehospitalization at 1 year.
Overall,thesepatientsareat highriskof longer-termhospitalizationanddeath.Safer,better-tolerated,andmoreeffective
therapies for symptom control in thishigh-risk population arewarranted.- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywor ds Atrial fibrillation † Ischaemic heart disease † Antiarrhythmic drug † Elderly † Outcomesresearch
Atrial fibrillation (AF) isthe most common dysrhythmia in adults,
and its incidence increases significantly with age. Ultimately, more
than one in four persons over the age of 40 will be diagnosed with
AF and 10% of octogenarians carry a diagnosis of AF.1,2 Atrial
fibrillation has a negative impact on the quality of life comparable
with that observed in patients with ischaemic heart disease, and
the effect is largely attributable to significant symptoms including
palpitations, fatigue, and exertional limitations.3,4 Randomized
data have suggested that maintenance of sinus rhythm (‘rhythm
control’) isassociated with improved symptoms.5,6
However,antiarrhythmic drug(AAD) therapyinpatientswithcor-
onary artery disease (CAD) raisesseveral safety concerns, including
toxic side effects and the potential for fatal proarrhythmia.7–9 Yet
most of the evidence in the literature is derived from selected
populationsand few dataare available in older patients. In an effort
to assess the effects of AAD on clinical outcomes in older patients
with AF and CAD, we performed an analysis of patients in the
Duke Databank for Cardiovascular Disease. The objectives of this
study were (i) to describe the use of AADs in older patients
with AF and CAD, (ii) to assess clinical outcomes in these
* Correspondingauthor. Tel: + 1 919 668 8686; fax: + 1 877 991 8498. E-mail address: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2014. For permissionsplease email: [email protected].
Europace (2014) 16, 1284–1290
doi:10.1093/europace/euu077
at Un
iversitÃ
deg
li Stu
di d
i Firen
ze on S
eptem
ber 2
5, 2
014
http
://euro
pace.o
xfo
rdjo
urn
als.org
/D
ow
nlo
aded
from
Steinberg BA, 2014
Forest plot of adjusted KM event rates at 1 year in the Duke
Databank for Cardiovascular Disease (DDCD) cohort (2000-10)
All cause 5-year re-hospitalization
65-75 non-AAD: 79%; >75y AAD: 87%
Conclusions
Older patients with AF and CAD are at high risk of
long-term death and rehospitalization
Treatment with AAD was associated with increased
rehospitalization at 1 year
These data highlight the need for improved
therapies in this population

Surv
ivors
(%
)
Time (years)
HR 0.73 (95%CI 0.67-0.80)
p<0.001
HR 0.97 (95%CI 0.83-1.14)
p=0.73
Placebo
b-blocker
Sinus Rhythm (N=13946, Age: 64 y, EF: 27%)
Atrial Fibrillation (N=3066, Age: 69 y, EF: 27%)
Kaplan-Meier survival curve for patients with sinus rhythm and
atrial fibrillation in the β-blocker and placebo groups (FU: 3.3 years)
Kotecha D, 2014
Mortality: 16%
Mortality: 21%

Event-
free (
%)
Time (years)
HR 0.78 (95%CI 0.73-0.83)
p<0.001
HR 0.91 (95%CI 0.79-1.04)
p=0.15
Placebo
b-blocker
Sinus Rhythm (N=13946, Age: 64 y, EF: 27%)
Atrial Fibrillation (N=3066, Age: 69 y, EF: 27%)
Cardiovascular hospital admission in patients with sinus rhythm and
atrial fibrillation in the β-blocker and placebo groups (FU: 3.3 years)
Kotecha D, 2014
Events: 26%
Events: 29%

Esti
mate
d S
urv
ival
Time (years)
0.0
0.2
0.4
0.6
0.8
1.0
0 2 4 6 8 0 2 4 6 8
AF with Heart Failure (Age: 80 years, FU: 3.1 & 3.0 years)
AF without Heart Failure (Age: 79 years, FU: 4.2 & 3.9 years)
No-Digoxin N=24331, Events: 62.1%
Digoxin N=15181, Events: 73%
No-Digoxin N=77399, Events: 49.8%
Digoxin N=23200, Events: 63%
HR=1.14
HR=1.17
Kaplan-Meier curves for digoxin use and all-cause mortality in AF
patients with and without heart failure (Quebec, Canada; 1998-2012)
Shah M,
2014

Il trattamento delle aritmie in età geriatrica
Simposio
NUOVE TECNOLOGIE IN TEMA DI CARDIOPATIE DELL’ANZIANO
PER IL TRATTAMENTO DELLE ARITMIE E DELLE VALVULOPATIE
Verso un nuovo approccio …

Days
Wit
ho
ut A
F r
ec
urr
en
ce
Late (>14 days)
recurrences
RR=0.51, 95%CI
(0.25-1.00), p=0.03
N=118
N=120
De Ferrari G, Camm
JA, Marchionni N,
Fumagalli S, 2014
Late sodium current blockers, by reducing the triggers, may
represent a novel approach against AF

Atr
ial
Fib
rill
ati
on
(H
R,
95%
CI)
Relative Weight Change (%)
Po
po
rtio
n o
f P
op
ula
tio
n (
%)
Loss
>5%
Gain
>10% +61%
+52%
Association of relative weight change with incidence of AF in
men after adjustment for age and race
Huxley RR, 2014

2,8
1
3,6
2
0
1
2
3
4
Admission Patient
SAFETY
Standard
11
18
0
5
10
15
20
25
(Days
)
Pati
en
ts (
%)
SAFETY (N=168) – Age: 72 y
Standard (N=167) – Age: 71 y
Length of Stay in Hospital per
HR=0.62 (0.35-1.10)
P=0.099 P=0.035
P=0.018
Mortality and length of stay in hospital for recurrent admissions
by type of management
FU time: 24 months
Mortality
Unplanned
admission
CV admission
Stewart S, 2014
Standard management consisted of routine primary care & hospital follow-up.
The SAFETY intervention comprised a home visit and Holter monitoring after
discharge by a cardiac nurse with prolonged FU and multidisciplinary support
Intensive educative sessions – N=144 (93%)
Regular telephone support – N=77 (50%); telephone calls – N: 12.6 (3’ 26”)
Repeat home visits – N=40 (26%)

Imaging Characteristics Stratified by Sleep Apnea (N=720; Age: 56+11 years; sleep apnea – N=142, 20%)
Neilan TG, 2013
56
51
55
53
40
45
50
55
60
LVEF RVEF
SA positive
SA negative P=NS
P<0.0001
(%)
31
28
20
25
30
35
PASP
P=0.0002
(mm
Hg
)
44
40
30
35
40
45
50
LAD
P<0.0001
(mm
)
LVEF: LV ejection fraction
RVEF: RV ejection fraction PASP: pulmonary artery systolic pressure
LAD: left atrium dimensions

N=578,
RR: 30%
N=142,
RR: 51%
N=71,
RR: 68%
N=71,
RR: 35%
P<0.0001
P<0.0001
P=NS
AF recurrence according to presence and treatment of sleep apnea
Neilan TG, 2013
RR: recurrence rate
Treated / Untreated:
CPAP therapy >/< 4 h
FU: 42 months after pulmonary vein isolation

Atr
ial
Fib
rill
ati
on
Bu
rden
(h
/day)
Months
Success
rate: 24% Success
rate: 74%
Ablation (N=261)
Age: 79 y; EF: 51%;
AF duration: 48 m
Control (N=63)
Age: 79 y; EF: 49%;
AF duration: 43 m
Nademanee K, 2014
Comparison of 4-year atrial tachycardia/atrial fibrillation burden
between group 1 and group 2 patients with an implantable device

Nademanee K, 2014
Kaplan–Meier curves demonstrating improved survival from all-
cause mortality in patients who remained in SR after AF ablation
Ablation - NSR
Ablation - AF
No Ablation
1 5
98%
97%
86%
42%
87%
52%

Acute complications (24-h)
Ischemic stroke 2 (0.8%)
Hemopericardium 4 (1.5%)
Major bleeding (groin sites) 10 (4%)
Pulmonary edema 3 (1%)
30-day major events
Death for intracerebral hemorrhage 1 (0.4%)
Pseudoaneurysms 4 (1.5%)
Severe bleeding (groin sites) 3 (1%)
Atrial tachycardia 7 (2.5%)
Urinary tract infections 3 (1%)
High fever 2 (0.8%)
Nademanee K, 2014
Procedure time: 136+40’; 1/2/3/4 sessions = 56/34/7/3% of patients

38.9 37.5
8.1 7.1
1.7
14.
3 8.3 7.4 6.8 1.9
8.9 5.6
4.3
Summary of studies reporting on rates on asymptomatic cerebral
emboli in the immediate AF post-ablation period (<24–48 h)
Inc
ide
nc
e (
%) 50
40
30
20
10
0
70
60
Multi-electrode RF Irrigated RF CryoBalloon
Without With
procedural techniques
to reduce sources of
microemboli
Verma A, 2013

25.7%
29.8%
68.6%
72.8%
D=-4.1%
D=-4.2%
8.3%
10.0%
42.3%
47.4%
ICD (N=3545) – Age: 74.9 y, >80 y: 23.9%, EF: 25%
CRT-D (N=3545) - Age: 74.6 y, >80 y: 22.9%, EF: 25%
Events in the National Cardiovascular Data Registry’s ICD Registry (propensity-matched cohort; eligible - N=29777; 2006-9)
Masoudi FA, 2014

Time (days)
Pro
bab
ilit
y o
f su
rviv
al
Telemonitoring
N=10/333 (3.0%)
Control
N=27/331 (8.2%)
Hindricks G, 2014
Kaplan-Meier curves of patient survival in the IN-TIME trial (2007-2010; age: 65.5 years, LVEF: 26%, CRT-D: ≈58%, FU: ≈330 days)c
Telemonitoring contacts: N=641 in 71% of pts
Contacts due to: Worsened HF: 12% / Deviation Tx: 15%
Additional visits: 63 pts (19%); IS Visits – T: 3.1 vs C: 2.9 pt.y
HR = 0.36 (95%CI = 0.17-0.74)
P = 0.004

N=52 intervallo
Età (anni) 68+10 41-82
Età >75 anni (%) 26.6%
FC (b/min) 73+12 50-100
PAS (mmHg) 117+15 85-145
PAD (mmHg) 70+10 45-90
FE VS (%) 28+5 18-38
Cardiopatia ischemica (%) 44
Charlson Comorbidity Index 4.4+2.0 1-9
Farmaci (N) 7+2 1-13
ACE-I / ARB (%) 65 / 24
b-bloccanti (%) 83
Digitale (%) 9
Diuretici (%) 86
Effetti della terapia di resincronizzazione cardiaca (CRT).
Risultati preliminari di uno studio policentrico italiano

67 64
56
48
35
45
55
65
75
85
Base 6 m
LVEDD
LVESD
28
35
20
25
30
35
40
45
Base 6 m
P<0.001
Dia
metr
i d
el V
S (
mm
)
Fra
zio
ne d
i eie
zio
ne V
S (
%)
P=0.010
Effetti della terapia di resincronizzazione cardiaca (CRT)
sulla performance e sul “reverse remodeling” del VS
6 m: 6 mesi
P<0.001
LVEDD: diametro telediastolico
LVESD: diametro telesistolico
N=52; età media: 68+10 anni; Classe NYHA III: 65%; FA: 21% -
Risultati preliminari (Centri partecipanti: Firenze, Bergamo, Caserta)

2,5
1,8
0,5
1
1,5
2
2,5
3
3,5
Base 6 m
P<0.001 Cla
sse N
YH
A
Effetti della CRT su stato funzionale e neuro-cognitivo di
pazienti con grave scompenso cardiaco
6 m: 6 mesi
N=52; età media: 68+10 anni; Classe NYHA III: 65%; FA: 21% -
Risultati preliminari (Centri partecipanti: Firenze, Bergamo, Caserta)
26
27
18
22
26
30
Base 6 m
P=0.009 MM
SE
(p
un
teg
gio
)
9,1
10,2
4
6
8
10
12
Base 6 m
P=0.012 SP
PB
(p
un
teg
gio
)
SPPB: Short Physical Performance Battery
Balance Test (p=0.253); Gait Speed (p=0.005);
Chair Standing (p=0.015)

La terapia antiaritmica in pazienti di età avanzata è estremamente
complessa e, molto spesso, inefficace o pericolosa, se attuata con
trattamenti tradizionali
L’utilizzo di trattamenti innovativi, non necessariamente ad elevata
tecnologia, indirizzati ad un maggior contatto con il paziente è
risultato efficace nel ridurre le ospedalizzazioni e, talvolta, la
mortalità
Sono necessari studi clinici specifici per valutare quali pazienti
anziani possano effettivamente trarre vantaggio da interventi ad
elevata invasività
La terapia di resincronizzazione cardiaca, grazie ad una azione
significativa sul ventricolo sinistro, migliora non soltanto la prognosi
del paziente, ma anche il profilo funzionale e neuro-cognitivo
Conclusioni

1 1 1 1,03 1,12
1,23
1
1,61 1,59
0
0,5
1
1,5
2
Ideal Intermediate Poor
<25
25-29.9
>29.9
Physical Activity
Atr
ial F
ibri
lla
tio
n (
HR
, 9
5%
CI)
Risk of Incident AF by the Impact of Level of Physical Activity and Overweight &
Obesity, in Men, in the ARIC (1987-2009, N=1775/14219, 6.9 per 1000 person-years)
Huxley RR, 2014
P interaction= 0.05 BMI

OR 95%CI p
Age / / NS
Female / / NS
Lives alone / / NS
Education Years / / NS
Depressive Symptoms 5.14 1.84-14.34 <0.05
Cognitive impairment 6.27 2.54-15.36 0.001
CHA2DS2VASc score / / NS
HAS-BLED score 2.52 1.03-6.16 <0.05
Multivariate Predictors of the Absence of Oral Anticoagulation Therapy (N=137; Age: 82 years; Permanent AF: 70%; Not anticoagulated: 51%; High
risk – CHA2DS2VASc: 99%; HAS-BLED: 39%)
Depressive Symptoms: Geriatric Depression Scale >5; Cognitive impairment: Mini-Mental State
Examination ≤ 23
Sanchez-Barba B, 2013
ARE GERIATRIC SYNDROMES ASSOCIATED WITH RELUCTANCE
TO INITIATE ORAL ANTICOAGULATION THERAPY IN ELDERLY
ADULTS WITH NONVALVULAR ATRIAL FIBRILLATION?








![Le cardiopatie Congenite 2007 [modalità compatibilità]lnx.mednemo.it/wp-content/uploads/2008/01/le-cardiopatie-congenite... · Principali fattori eziologici alla base delle cardiopatie](https://img.pdfslide.net/doc/110x75/5c6d95b009d3f2f4358bf0d0/le-cardiopatie-congenite-2007-modalita-compatibilitalnx-principali-fattori.jpg)