Embed Size (px)
Citation preview

Open AccessTechnical ReportPublished 09/30/2014DOI: 10.7759/cureus.213
Copyright © 2014 Renouf et al.
Distributed under Creative Commons CC-BY 3.0
Body Packing with Cocaine: ASimulation Exercise
Tia Renouf, Holly Black, Sabrina Alani, Adam Dubrowski
Corresponding author: Adam Dubrowski
1. Emergency Medicine, Memorial Univers ity 2. Medicine, Memorial Univers ity ofNewfoundland 3. Emergency Medicine, Oncology, Memorial Univers ity ofNewfoundland 4. Emergency Medicine, Pediatrics, Memorial Univers ity ofNewfoundland
Categories: Emergency Medicine, Medical Education, Medical SimulationKeywords: emergency medicine, medical education, s imulation based medicaleducation, toxicology, body packing, cocaine, hypertensive emergency, arrythmias,seizures
How to cite this articleRenouf T, Black H, Alani S, et al. (2014-09-30 11:22:16 UTC) Body Packing withCocaine: A Simulation Exercise. Cureus 6(9): e213. doi:10.7759/cureus.213
AbstractPedagogically sound simulation-based medical education (SBME)produces effective learning [1]. We present a simulation scenario for"body packing", which is the concealment of an illicit drug inpackets (usually condoms) inside the body by swallowing or recto-vaginal insertion, usually for transportation across borders. Thisscenario will train Emergency Medicine residents to suspect bodypacking under appropriate circumstances, and to treat the potentialalimentary pathologies and drug toxicities which body packing withcocaine can cause.

IntroductionAlso known as “muling”, body packing involves filling a body cavitywith wrapped packets of an illegal drug. It is sometimes confusedwith “body stuffing”, an evasive tactic by a person carrying generallysmall amounts of illicit drugs, should they feel they are about to beapprehended by police. In contrast, body packing is typicallysuspected at international airports, where security personnel ordrug dogs are trained to find contraband. Drug packets concealed ina body cavity can leak or burst, causing a massive overdose, usuallyof cocaine and heroin. The packets themselves can also cause bowelor esophageal obstruction, perforation, and peritonitis. The leakageof packets containing cocaine is a medical emergency and anindication for prompt surgical removal.
For medical learners in smaller residential and urban areas, whereinternational traffic is limited or absent, the diagnosis of bodypacking may be challenging. For example, trainees at MemorialUniversity of Newfoundland (MUN) located in St. John'sNewfoundland (population 208,372 as of 2013) serve a relatively smallpopulation, in which the drug trade has recently taken hold wherethere was once mostly petty crime. It has been projected that recentoffshore gas discovery and attendant international travel may bringmore cases of body packing to this province’s emergencydepartments.
We describe a simulation exercise designed to teach trainees at MUNan approach to cocaine toxicity in the setting of body packing.
Technical ReportThis simulation session uses the Gaumard Noelle S575 human patientsimulator, programmed to produce a cocaine intoxication. Ifrequested by the learner, a plain abdominal x-ray image showspackets of drug within the bowel of a patient who is in handcuffs.Two confederates are employed as prison personnel. The detailedstepwise scenario is written and given to technical staff, who thenprograms the computer to control the simulation.
Pre-briefingBefore the simulation begins, students are introduced to the“fictional contract”, in which they acknowledge that although thecase is an invention, participants will behave as though it is real. Thiscreates a safe place where trainees can make mistakes. It is
2014 Renouf et al. Cureus 6(9): e213. DOI 10.7759/cureus.213 Page 2 of 14

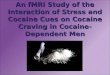
acknowledged to be a strictly formative exercise. In this case, theabdominal x-ray image used is also a simulation. One image, obtainedonline, shows evidence of body packing (Figure 1), while the other,because of an error in positioning a patient in our x-ray department,shows an inmate/patient's handcuffs and shackles in an otherwiseunremarkable film (Figure 2). To help tell the story, two real x-rayimages were superimposed (Figure 3). The students are told, “thishybrid image is obviously not real, but we would like you to suspendyour disbelief for the purposes of learning”.
2014 Renouf et al. Cureus 6(9): e213. DOI 10.7759/cureus.213 Page 3 of 14

Figure 1:Abdominal x-ray image showing packets of cocaine
Figure 2:Normal abdominal x-ray image in hand-cuffed patient brought to Emergency from jail
2014 Renouf et al. Cureus 6(9): e213. DOI 10.7759/cureus.213 Page 4 of 14

Figure 3:Synthesis of FIgures 1 and 2, showing shackles as well as cocaine-filled packets in bowel
CaseThe learning objectives for this simulation scenario are:
1. ABCs of resuscitation and forming an initial impression,
2. Recognition of the sympathomimetic toxidrome,
2014 Renouf et al. Cureus 6(9): e213. DOI 10.7759/cureus.213 Page 5 of 14

3. Recognition and treatment of cocaine toxicity while prioritizing itsthree most lethal complications: hyperthermia, hypertensiveemergency, and cardiac arrhythmias,
4. Recognition of body packing.
In this simulation, the learners are informed that a young male, inthis case, a Gaumard Noelle S575 human patient simulator, is broughtin handcuffs to a tertiary care emergency room (ER), accompanied bytwo prison personnel. Trained Standardized Patients (SPs) act as thetwo prison personnel, who are present throughout the scenario toanswer any questions (if relevant) but who are instructed not toprovide any voluntary information. The learners are informed thatthe immigration authorities apprehended him from hisColumbian flight when it landed unexpectedly in St. John’s. Theysuspected drug trafficking because he paid cash for his one-wayticket, was wearing sunglasses at night, and seemed nervous. Thepatient is alert and well at the airport. His nose is running.
Table 1 describes the simulation algorithm used in progressivelydeteriorating the patient (Gaumard Noelle S575 human patientsimulator) by the educator using the computer.
ScenarioYou are an emergency room physician at a tertiary care center and have just begunyour shift. A 26-year-old patient who is accompanied by law enforcement, is yourfirst patient. On return from Columbia he was arrested at the airport on drugrelated charges. He is currently being triaged.Begin Scenario- Learner enters the patient's roomObjective 1: Airway, breathing, and circulation/Initial impressionAdditional Scenario Data/Physical Exam Findings Vital Signs Appropriate Learner Action
Patient is in handcuffs andshackles. Patient is deliriousand diaphoretic. He issniffing and his nose isrunning.
Vital signs:BP180/110,HR 160, T38.8, RR 24GCS 15
Immediately brings to resuscitation bay.While taking history andphysical, initiates 2 large bore iv's,cardiac monitor,ekg,finger stick glucose,thiamine 100 mg iv, dextrose.
Objective 2: Recognition of sympathomimetic toxidromeAdditional Scenario Data/Physical Exam Findings Vital Signs Appropriate Learner Action
Teacher as penetentiaryattendent: "We got this guy
2014 Renouf et al. Cureus 6(9): e213. DOI 10.7759/cureus.213 Page 6 of 14

off a flight. Took him to thePen 'cos he lookedsuspicious. Started to actstrange in the jail so webrought him to you, Doc." If examined: The patient isvery diaphoretic andagitated. Mydriasis andhyperreflexia are noted,abdomen is nontender, bowelsounds are decreased, lungsounds clear, equal air entrybilaterally, normal S1S2
Vital signs:BP180/110,HR 160, T38.8, RR 24GCS 15
Orders: Complete blood count (CBC),electrolytes, BUN, creatinine, creatinekinase (CK), alcohol level, venous bloodgas, serum osmolality, liver functionpanel(LFTs),troponin,INR,urinalysis/urinedrug screen, blood cultures, ECG
Laboratory/ECG/Diagnostic imaging results:If Ordered:Bedside glucose: 6 mmol/LECG: Sinus tachycardia and diffuse ischemia: See Figure 4Abdominal xray: pendingObjective 3: Recognition and treatment of cocaine toxicity, and priorizing its 3most lethal complications: hyperthermia, hypertensive emergency and cardiacarrythmiasTeacher as nurse: “Doctor,the blood work is drawn, butyour patient is more agitatedand is yelling. He is reallydiaphoretic now and he isgrinding his teeth. He ismuttering somethingabout chest pain."
Vital Signs:BP150/110,HR 135, T39, RR 24GCS15
Learner reassesses the patient. Ordersrepeated doses of benzodiazepines.Simultaneously prepares for RapidSequence Intubation if airway not secureor patient's predicted clinicalcourse mandates pre-emptive airwaycontrol. Initiates intensive coolingmeasures such as cool wet sheets, fans,ice packs to axillae and groins, or iceimmersion in refractory hyperthermia. Aggressive hydration with crystalloid Nitroglycerine, benzodiazepines for chestpain
If no benzodiazapinesordered
Vital signsdeteriorate
If no cooling measuresinitiated
Vital signsdeteriorate
Patient says the chest pain isnot so bad Learner continues to assess patient.
Orders repeat ECGLaboratory/ECG/Diagnostic imaging resultsECG: Na Blockade See Figure 5 Manages arrhythmia by reversing
sodium blockade with sodiumIf no management of Vital signs
2014 Renouf et al. Cureus 6(9): e213. DOI 10.7759/cureus.213 Page 7 of 14

arrhythmia deteriorate bicarbonate 1-2 meq/kgAbsominal xray not yet available
Teacher as nurse: “Doctorthe blood work is back”
Vital signs:BP 140/85,HR 115, T379, RR 22GCS 15
Manages lab abnormalities. Continuesaggressive hydration. 1 salbutamolneb,10 units regular insulin IV and 50ccof 50% dextrose IV.Consider iv calcium gluconate
Laboratory/ECG/Diagnostic imagingresults:Lab results as ordered by learner:Electrolytes: K- 6.8 mmol/L, Na 140mmol/L,CBC: NormalLFT’s: NormalPT/PTT: NormalSerum osmolality: 290 mmol/kgCreatinine: 140 umol/LCK: 5553 U/LAlcohol: negativepH: 7.29Urine: hemoglobin positive/ microscopynegative for red blood cells ORmyoglobin positive. Cocaine positive (mayoccur if small amounts drug ingestedduring ingestion of packets, or if packetruptures)
Teacher as nurse: “Doctorthe patients blood pressureis 190/130”
Vital signs:BP190/130,HR 120, T379, RR 24
Manages hypertension with increaseddoses benzodiazepines
No change Orders high-dose nitroglycerine forafterload reduction, nitroprusside orphentolamine when benzodiazepinesineffective. An advanced learner maysuggest labetalol if they can explain thechoice (alpha and beta blockade).
If learner gives beta blockers Patientdeteriorates
Teacher as nurse: “Help, heis having a seizure”
Vital signs:BP170/100,
Manages withbenzodiazepines endotracheal intubationif airway compromised, or if indicated by
2014 Renouf et al. Cureus 6(9): e213. DOI 10.7759/cureus.213 Page 8 of 14

is having a seizure” HR 120, T39, RR 24
if airway compromised, or if indicated bypredicted course of the patient
Objective 4: Recognition and treatment of body packingUpon recognition of thesympathomimetic toxidromeand the appropriatemanagement of the mostcritical problems, thelearner is informed that thepatient continues to haveunusually prolongedsymptoms as if he continuesto be exposed to thesubstance
Vital signs:BP 160/92HR 125, T379, RR 26GCS 15
Learner considers the possibility of drugconcealment/body packing. Abdominalxray now available.
. Laboratory/ECG/Diagnostic imaging results:X-ray: See Figure 3 If airway secure, learner consults
surgery immediately for packetremoval,considers oral charcoal, initiateswhole bowel irrigation if timepermits. Strongly considers endotrachealintubation to facilitate all of the above
If no whole bowelirrigation ordered: Teacheras Police: “You know Doc, wewere kind of concerned hemight be a drug mule”
Vital signsdeteriorate
Appropriate treatment results in the simulated patient stabilizingEnd Scenario
Table 1: Simulation TemplateBlood Pressure (BP) Heart Rate (HR) Temperature (T) Respiratory Rate (RR) Glasgow ComaScale (GCS)
DebriefingDebriefing has been described as a critical component of thesimulation exercise [2]. Initially, students are encouraged to discusstheir feelings about the case. To encourage candor, we allow amaximum of one teacher per learner. We use the advocacy-inquirytechnique [3], which allows us to frame the trainee’s thoughtprocesses non-judgmentally, and to neutrally suggest otherapproaches which might be more fruitful.
Post-scenario didacticsA brief didactic session, which addresses the learning objectives, isheld after the debrief. This allows consolidation of the knowledgeacquired during the simulation and closes any knowledge gaps.
2014 Renouf et al. Cureus 6(9): e213. DOI 10.7759/cureus.213 Page 9 of 14

DiscussionDrug muling was first described in Canada in 1973 [4], when a singlecondom filled with hashish caused a small bowel obstruction and wasuneventfully removed.
Body packing with sympathomimetic illicit drugs is globallyincreasing in frequency [5], partly due to increased airport securitypost-September 11th [6], but it remains an uncommon problem inmany small centres. Failure to recognize the presence of bodypacking can lead to potentially fatal medical errors. For example, thepatient in our scenario was taken to jail from the airport when it mayhave been more appropriate to bring him to the ER.
Several kinds of drugs can be carried in the alimentary tract orvagina, including cocaine, heroin, ecstasy, and cannabis products.Typically, only one kind of drug is transported at a time. The amountof drug carried is variable; 50-200 packets, each containing up to 10gm of a drug, has been described. A single ruptured packet maycause death as more than 10 times the lethal dose of cocaine may bereleased [7]. Drug packets, once primitively constructed, are nowprecisely crafted with well-compacted contraband covered in latexand sometimes wax. They are uniform in appearance andoccasionally wrapped in foil to alter their radiographic appearance[8]. Body packers usually know exactly how many packets they arecarrying, but may deny carrying any. Luggage contents mayinclude large numbers of condoms, latex fingers and gloves,petroleum jelly, coconut oil for swallowing packets, toilet paper, roomdeodorants, and coal packets, as well as medicines to controlabdominal cramping and diarrhea. If body packers elude arrest,laxatives are taken to encourage packet expulsion; if they come tothe hospital and remain asymptomatic, packets are counted whenexpelled, then given to police. Two consecutive normal stools indicatethat the drug has passed [7].
Body packing with cocaine can be lethal. The condoms, balloons, orcellophane enclosing the drug can leak or rupture, causing apotentially fatal overdose. The packets themselves can cause a bowelobstruction, perforation, and/or peritonitis. Esophageal rupture canoccur. As one leaking packet of drug can release a fatal amount ofcocaine, it is important for emergency medicine trainees torecognize the sympathomimetic toxidrome, the othertoxicities caused by cocaine, and the presence of body packing,which implies that many more packets of drug are concealed inside
2014 Renouf et al. Cureus 6(9): e213. DOI 10.7759/cureus.213 Page 10 of 14

the body where they can leak and worsen the toxicity. In a stablepatient, any free drug will be absorbed somewhat by oral charcoal,while the packets are expelled over time with whole bowel irrigation.Should symptoms and signs of cocaine toxicity develop, surgery mustbe consulted while resuscitation is underway for packet removal vialaparotomy. Laparoscopic removal risks tearing thecondoms. Conservative management is usually successful when thepackets are not leaking [9-10].
This simulation scenario uses a computerized human mannequin toteach emergency medicine trainees an approach to the sympathetictoxidrome, cocaine toxicity, and body packing. It also uses a “fictionwithin a fiction”: two real abdominal x-ray images are superimposedto create a third entity which helps tell the story. Because of thereports of controversy about the ethical difference betweenimproving an image, and frankly altering it [11], we have decided toacknowledge this fact and admit to the factitious nature of the imagewhile discussing our contract with the learner. In order to avoiddisclosing details prematurely, the images themselves are not shownuntil later in the simulation. The x-ray depicting shackles andhandcuffs in an otherwise unremarkable film came from an actualpatient from a local jail. Usually shackles and cuffs are not imagedbecause the patient raises their hands above their head; on thisoccasion, an error in our x-ray department led to the inclusion of thehardware. We felt that such a striking and unusual image could formthe basis for our body packing scenario. Since we rarely see bodypacking, and have no actual images of it from our own population, weacquired the x-ray showing packets within the bowel online andsuperimposed the two. The resulting image showing shackles andhandcuffs as well as packets in the bowel, may be "larger than life",but it serves to illustrate the diagnosis in our setting, where bodypacking is rare now, but potentially will become more frequent.
As mentioned earlier, the learning objectives for this simulationscenario were:
1. ABCs of resuscitation and forming an initial impression,
2. Recognition of the sympathomimetic toxidrome,
3. Recognition and treatment of cocaine toxicity while priorizing itsthree most lethal complications: hyperthermia, hypertensiveemergency, and cardiac arrythmias,
2014 Renouf et al. Cureus 6(9): e213. DOI 10.7759/cureus.213 Page 11 of 14

4. Recognition of body packing.
These objectives were developed because cocaine toxicity produces amulti-system assault. Hyperthermia must be promptly andaggressively managed with cooling techniques andbenzodiazepines in order to reduce mortality. It is associated withrhabdomyolysis, hyperkalemia (which may worsen cardiacarrhythmias), renal failure, and myocardial ischemia (Figure 4).Hypertensive emergencies associated with cocaine overdose aretreated with benzodiazepines and phentolamine (a pure alpha-blocker), and high-dose nitroglycerine or nitroprusside. Beta-blockade will worsen the situation. Cardiac arrhythmias seen aremost commonly sinus tachycardia, but excess adrenalization mayproduce atrial fibrillation (AF) or supraventricular tachycardia (SVT).Wide-complex ventricular tachycardia may happen in association withfast sodium channel blockade (Figure 5) and is treated with sodiumbicarbonate. It may be preceded by the RSR' pattern in AVR, as inother sodium channel blockers overdoses, such as tricyclicantidepressants. Lidocaine and other 1A anti-arrhythmics must beavoided because they block sodium channels. The presence of bodypacking raises the possibility of worsening toxicity as well asmechanical bowel obstruction, perforation, and peritonitis.
Figure 4: Diffuse ischemic changeCommonly seen with chest pain in cocaine intoxication [12]
2014 Renouf et al. Cureus 6(9): e213. DOI 10.7759/cureus.213 Page 12 of 14

Figure 5:RSR' pattern and wide QRS typical of sodium channel blockade, seen in cocaine and othertoxicities like tricyclic anti-depressants [13].
Patients with cocaine toxicity often present with toxic delirium, inwhich it is important to consider other causes, such asinfection, Wernieke's encephalopathy, or trauma. It is prudent toorder blood cultures, if indicated, and administer thiamine anddextrose at the outset.
ConclusionsSimulation is a valuable tool for teaching emergency medicinetrainees the effects of cocaine toxicity in the context of bodypacking. Simulation includes a fictional contract in which teachersand learners acknowledge that the case in question is not real, butagree to suspend their disbelief and proceed as though it is. Wedescribe a simulation exercise in which the transposition of two realx-ray images produces a third image, which helps tell the story.
Additional InformationDisclosuresNo disclosures were made. No human/animal subjects were involvedin this study.
AcknowledgementsThis project was supported by Tuckamore Simulation ResearchCollaborative and Emergency Medicine Education Committee,Memorial University of Newfoundland. Two original x-ray images
2014 Renouf et al. Cureus 6(9): e213. DOI 10.7759/cureus.213 Page 13 of 14

were combined digitally to create a third image. Thanks to LukeMerdsoy for this work.
References1. Issenberg SB, Scalese RJ: Simulation in health care education.
Perspect Biol Med 2008, 51:31-46. doi: 10.1353/pbm.2008.00042. Rudolph JW, Simon R, Rivard P, Dufresne RL, Raemer DB: Debriefin
g with good judgment: Combining rigorous feedback with genuine inquiry. Anesthesiol Clin 2007, 25:361-76.
3. Helminski L, Koberna S: Total quality in instruction: A systems approach. In Academic initiatives in total quality for higher education.Edited by Roberts HV. Milwaukee, WI: ASQC Quality Press;1995:309–362.
4. Deitel M, Syed AK: Intestinal obstruction by an unusual foreign body. Can Med Assoc J 1973, 109:211-2.
5. Hergan K, Kofler K, Oser W: Drug smuggling by body packing: What radiologists should know about it. Eur Radiol 2004, 14:736-42.
6. Stampede of drug mules at Kennedy: after 9/11 lull, heroin & ecstasy busts soar. 2002, Accessed: September 17, 2014. http://www.nydailynews.com/archives/news/stampede-drug-mules-kennedy-9-11-lull-heroin-ecstasy-busts-soar-article-1.484075.
7. Rao RB, Hoffman RS: Cocaine, amphetamines, and other sympathomimetics. In Rosen’s emergency medicine: concepts and clinicalpractice. 5th edition. St. Louis, MO: Mosby; 2002:1994-2000.
8. Traub SJ, Hoffman RS, Nelson LS: Body packing--the internal concealment of illicit drugs. NEJM 2003, 349:2519-26.
9. Beckley I, Ansari NA, Khwaja HA, Mohsen Y: Clinical management of cocaine body packers: the Hillingdon experience. Can J Surg2009, 52:417-21.
10. Bulstrode N, Banks F, Shrotria S: The outcome of drug smuggling by 'body packers'--the British experience. Ann R Coll Surg Engl2002, 84:35-8.
11. Bourne PE, Barbour V: Ten simple rules for building and maintaining a scientific reputation. PLoS Comput Biol 2011, 7:e1002108. doi:10.1371/journal.pcbi.1002108
12. Tricyclic overdose (Sodium-Channel Blocker Toxicity). 2014,Accessed: September 17, 2014. http://lifeinthefastlane.com/ecg-library/basics/tca-overdose.
13. Myocardial Ischaemia. 2014, Accessed: September 17, 2014. http://lifeinthefastlane.com/ecg-library/myocardial-ischaemia/.
2014 Renouf et al. Cureus 6(9): e213. DOI 10.7759/cureus.213 Page 14 of 14