Embed Size (px)
Citation preview

S I N G L E G A S T R I C P O L Y P * REPORT OF AN INSTANCE
By M A R T I N G. VORHAUS, M.D.
and
A R T H U R E. T. ROGERS, M.D. NEW YORK CITY, N. Y.
I N 1888, Menetrier 1 published a description of gastric polyp which stands as a classic in the interpretation of this
condition. Since then, many reports have appeared so that, today, the subject is fairly well covered. An excellent review of the previous literature is incorporated in the thesis of Kirklin and Broders 2 of the Mayo Clinic. In addition to their review, four instances of solitary lesions of the stomach are cited in a group of nineteen cases of gastric polyposis.
Unquestionably, the most effective method of diagnosing polyp of the stomach is the roentgen study, provided proper technique is exhibited. All observers have emphasized the possibilities for error at roentgen observation dependent upon food residues in the stomach itself, pressure from the adjacent gas-laden colon, foreign bodies in the stomach, notably hair- balls, and gastric carcinoma of the polypoid type.
The following case report is published to emphasize, again, the necessity for accurate gastro-intestinal roentgen-studies in a patient where, clinically, the digestive disturbance was productive only of vague symptomatology.
CASE R E P O R T
R. C., female, age 50, admitted to the Medical Clinic complaining of generalized abdominal pains, occurring five to ten minutes after meals, radiating to the back and right shoulder and relieved by alkalis, accom- pained by distension, heart burn, belching, anorexia, loss of fourteen pounds in the past three months, and severe constipation.
Two years previously, a cholecystectomy had been performed at another institution for the above symptoms without relief. Additional facts in the past history include typhoid fever many years ago and a previous hysterectomy.
The physical examination revealed no pertinent iindings except evi- dence of loss in weight. The laboratory study revealed normal findings for the urine and the blood; there was a low, normal gaslric acidity value following food test meals.
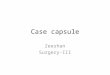
Routine gaslro-intestinal X-ray studies were made in this department. Stomach fluoroscopy and subsequent tihns disclosed a regular, con- stant, punched-out, filling-defect on the greater curvature of the pyloric antrum. On the opposite curvature, there was a fairly constant in- cisura. There, was a considerable gastric residue seen by inspection of both the three- and six-hour progress fdms, each film exhibiting the greater curvature filling-defect. A diagnosis of single gastric polyp was made, dependent upon the character and persistence of the anomaly (Figs. 1 & 2 and 3 & 4).
Pathological examination, by Dr. Henry L. Jaffe, proved the specimen to be an inflammatory polyp of the gastric mucosa (Fig. 5).
Follow-up of the patient showed disappearance of symptoms pre- viously noted, pre-operatively.
DISCUSSION
Special interest in this case centers upon the vagueness of the symptoms which were associated with such relatively extensive pathology. Existence of upper abdominal pain, radiating to the back and right shoulder and accompanied by dyspeptic symptoms, had led to the incorrect diagnosis of
Fig. 2--Stomach immediately after ingestion of barium meal.
gall bladder-disease at another institution, on the basis of which cholecystectomy had been performed. No gastro-in- testinal roentgenogram had been made at the first hospital experience and no report of the gall bladder studies which were made, is available. Unquestionably, prior to the first operation, gastro-intestinal roentgen films would have re- vealed the true nature of the pathological process in the stomach at that time as they did at our hands two years sub- sequently.
In gastric polyposis, occurrence of pain soon after meals is a frequent observation. The descriptions of the pain asso-
Fig. 1--Stomach immediately after ingestion of barium meal.
At operation, by Dr. Philip M. Grausman, a hard mass was felt about four inches from the pyloric end of the stomach. The stomach was opened and this mass was removed. The patient made an uneventful recovery.
*From the Department of Gastro-Intestinal Radiography, llospital for Joint Dis- eases, New York City.
Received for publication, April 8, 1934.
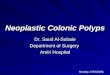
Fig. 3--Stomach, three hours following barium meal.
ciated with gastric polyp vary as to its degree and location. Pain simulating biliary colic is, perhaps, one of the most in- frequent types of all pain according to the various writers upon stomach polyposis.
The mechanism of pain production in our case is one which is open to conjecture. The roentgenograms demon-
169

170 A M E R I C A N J O U R N A L OF D I G E S T I V E D I S E A S E S AND ~NTUTRITION
Fig. 4---Stomach, six hours following barium meal. Single gastric pol)~p--A.
strate clearly that the polyp was a considerable distance from the pyloric sphincter; its pedicle was so short that it could not have been displaced downwards sufficiently to produce pyloric obstruction. There may have been, of course, an as- sociated pylor6spasm but our films demonstrate no roentgen evidence that spasm existed. Antral spasm might have been associated with the lesion and is 'a possible cause for the pain, even though the pain's radiation and location are atypical.
At all events, these unusual types and locations of pain serve to emphasize the fact that pain resembling that of biliary colic in intensity, location and radiation may be due at times, to organic disease entirely extraneous to the biliary tract. The gastric polyp present in this patient was in a location and of a size readily demonstrable by routine gastro- intestinal X-ray examination. Even in the presence of clear- cut roentgen evidence of gall bladder pathology, it is some- times advisable to study the gastro-intestinal tract; certainly, in those patients where, following cholecystectomy, the previous symptoms continue unabated, it becomes an ab- solute necessity that one rule out organic disease of the
F i g . 5 - - P h o t o m i c r o g r a m o f g a s t r i c p o l y p r e m o v e d a t o p e r a t i o n .
stomach as a cause. This case serves as an example: here one has a patient who was subjected to a totally unnecessary cholecystectomy and two years of additional post-operative suffering--a course which classified her as one of those patients unimproved by cholecystectomy--simply' because no stomach roentgenograms had been made when distressing dyspepsia first arose.
SUMMARY Report is made of an instance of single gastric polyp,
accompanied by a clinical symptomology resembling biliary colic; of cholecystectomy followed by no benefit; the dem- onstration of the polyp, roentgenographically; complete dis- appearance of all digestive symptoms after surgical removal of the anomaly. Pathologically, ;the lesion was of inflamma- tory character.
BIBLIOGRAPHY 1. P. Menetrier. Des polyadenomes gastriques et leurs rapports avec le cancer de
restoinac. Arch. de physiol, norm. e! path. 1:32,236, 1888.
2. B . B . Kirklin and A. C. Broders. Boentgenologic and Pathologic Aspects of Gas- tric Polyposis. J . A . M . A . 98:95, January 9, 1932.
R E C U R R E N T "HIATUS HERNIA" SYNDROME OF VON B E R G M A N N B y
FELIX CUNHA, M.D.* SAN FRANCISCO, CALIFORNIA
R ECENTLY, Hurst ~ described, under the title of this contribution, a peculiar type or variety of diaphra$-
matic hernia. He so named the anomaly because it had been brought to his aftention at Von Bergmann's Clinic at the Charite in Berlin in 1931. Yon Bergmann 2 stated that he regarded the disturbance of greater frequency than com- monly was supposed and that it accounted for a large variety of sub-sternal symptoms for which no other adequate etiology could be designated.
Friedenwald 3 and his associates, in 1925, described this particular variety of hernia and first called attention to the fact that 'it was necess.ary to fluoroscope patients so affected in the recumbent position in order to demonstrate the lesion, since, in the upright position, i t could not be seen. At the same time, these observers noted that forcible, deep inspira- tion during the examination, caused the hernia to become more prominent.
Hurst I believes that this particular variety of hernia should be separated from the more usual forms of hernia of the *Instructor in Medicine, University of California Medical School, San Francisco.
Visiting Physician, Gastro-Enterological Clinic, San Francisco Polyclinic and Post-Graduate Hospital.
Received for publication, April 5, 1934.
diaphragm commonly occtirring through the oesophageal hiatus. He calls attention to its incidence being mainly in elderly persons and that the tissues immediately adjacent to the oesophagus as it passes through the diaphragm, are abnormally lax. This laxity Hurst attributes to senile atro- phic changes with the consequent loss of tone. In the pres- ence of such a point of lowered resistance, it is only necessary to add one other factor, namely, increased intra-gastric pressure, either intermittent or constant; then the same mechanical factors are 15resent which produce herniae in other parts of the body.
Akerlund 4 described three types of hiatus herniae: a. Congenital--that associated with congenitally shortened
oesophagus. b. Para-oesophageal--where a portion of the lower oesopha-
gus is in the abdomen and some portion of the cardiac end of the stomach bulges around that low-lying terminus
1. Hurst , A. F. Joarnal A .M.A.A. 102:585-587, February 24, 1934. 2. " Von Bergmann, Gustav, und Goldner, Martin. Fanctionelle Pathologie, Berlin,
Julius Springer, 1932. 3. Friedenwald, Julius, and Feldman, Manrice. Am. J. M. Sc. 170:263, August, 1925. 4. Akerlund, A. Oehnell, und E. Kay. Acta Radiologica (Stockholm) VI, 3 (1926). 5. Schatski, R. Fort a. d. Geb. d. Roentgen Strahlcn. 45:177-187, February, 1932.