Embed Size (px)
Citation preview
SLIDE 1 of 34
IS THERE A CAUSAL RELATIONSHIP BETWEEN SUBSTANCE ABUSE AND PSYCHIATRIC
ILLNESS?
Dr Martin Frisher Department of Medicines Management
Keele University, Staffordshire, UK
Manchester, Tuesday 24th November 2005
SLIDE 2 of 34
UK Department of HealthUK Department of HealthComorbidity in Primary CareComorbidity in Primary Care
Study 1: Estimate the occurrence of Study 1: Estimate the occurrence of comorbidity in comorbidity in primary care in England and primary care in England and Wales.Wales.
Study 2: Analyse the time sequence between Study 2: Analyse the time sequence between mono mono and dual diagnosis. and dual diagnosis.
Study 3: Compare health care utilisation by Study 3: Compare health care utilisation by mono, mono, comorbid and control comorbid and control patients.patients.
Study 4: Confirm whether secondary care Study 4: Confirm whether secondary care diagnoses diagnoses are recorded in primary are recorded in primary care.care.
SLIDE 3 of 34
Frisher M, Collins C, Millson D, Crome I, Croft P. Prevalence of comorbid psychiatric illness and substance misuse in primary care in England and Wales Journal of Epidemiology and Community Health 2004; 58:1036-1041
Frisher M, Crome I, Macleod J, Millson D, Croft P. Substance misuse and psychiatric illness: prospective observational study using the general practice research database. Journal of Epidemiology and Community Health 2005; 59:847–850
Papers from the study
SLIDE 4 of 34
First presentation to health First presentation to health serviceservice
Addicts’ mental illness being being ignored?Addicts’ mental illness being being ignored?
George Harrison’s attacker Michael Abram’s George Harrison’s attacker Michael Abram’s schizophrenia was not diagnosed - because of schizophrenia was not diagnosed - because of heroin abuse?heroin abuse?
On the other hand, among psychiatric On the other hand, among psychiatric patients…..“addiction being ignored”patients…..“addiction being ignored”
““Urgent action is needed to help mentally-ill people Urgent action is needed to help mentally-ill people who are addicted to drink or drugs, an influential who are addicted to drink or drugs, an influential group of MPs has warned”. (group of MPs has warned”. (All-Party All-Party Parliamentary Drugs Misuse Group, 2000)Parliamentary Drugs Misuse Group, 2000)
SLIDE 5 of 34
Comorbidity: US ResearchComorbidity: US Research
50% of schizophrenic patients have 50% of schizophrenic patients have substance misuse disordersubstance misuse disorder
Such co-morbidity is associated with:Such co-morbidity is associated with: heavy use of psychiatric inpatient care, poor heavy use of psychiatric inpatient care, poor
treatment compliance, poor prognosis and treatment compliance, poor prognosis and high offending rateshigh offending rates
Services Services combiningcombining psychiatric and psychiatric and substance misuse treatments may be substance misuse treatments may be more effective than management by more effective than management by separate servicesseparate services
SLIDE 6 of 34
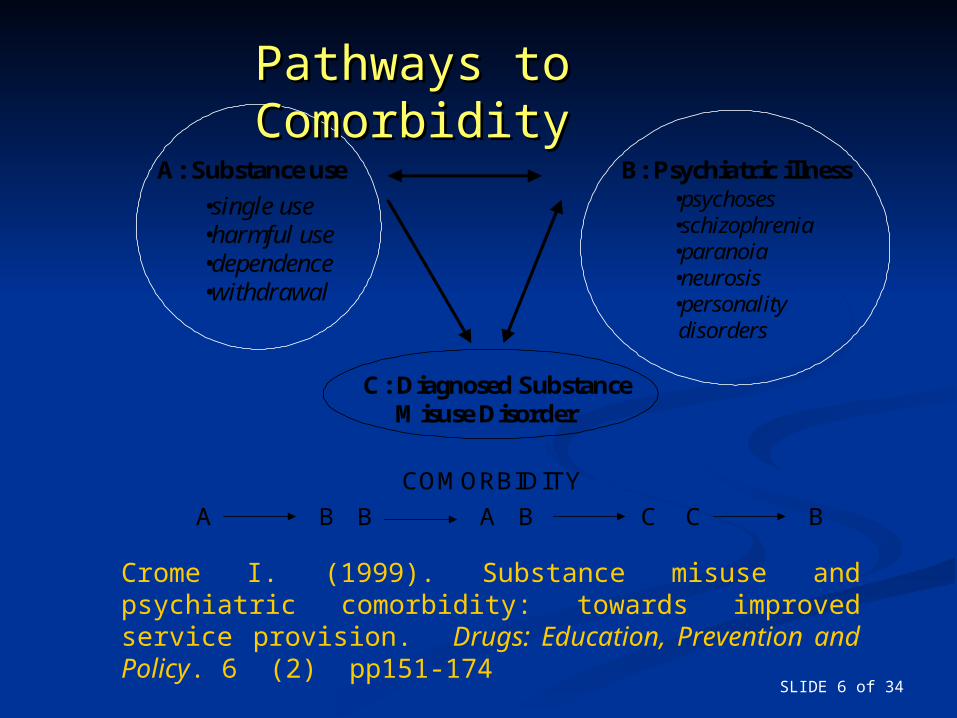
C: Diagnosed Substance Misuse Disorder
A: Substance use B: Psychiatric illness
•single use•harmful use•dependence•withdrawal
•psychoses•schizophrenia•paranoia•neurosis•personality disorders
COMORBIDITY
A B B C C BB A
Pathways to Pathways to ComorbidityComorbidity
Crome I. (1999). Substance misuse and psychiatric comorbidity: towards improved service provision. Drugs: Education, Prevention and Policy. 6 (2) pp151-174
SLIDE 7 of 34
Type of Comorbidity StudyType of Comorbidity Study
PrevalencePrevalence General population, primary General population, primary
care, specialist servicescare, specialist services Development of comorbidityDevelopment of comorbidity
Clinical, epidemiologicalClinical, epidemiological TreatmentTreatment
Standard or specialisedStandard or specialised
SLIDE 8 of 34
Studying Co-morbidity using Studying Co-morbidity using the GPRDthe GPRD
Data collected from about 1.8 Data collected from about 1.8 million patients (230/370 practices)million patients (230/370 practices)
258 substance misuse diagnoses 258 substance misuse diagnoses and 1,693 psychiatric diagnoses and 1,693 psychiatric diagnoses (based on ICD 9 and Read Codes)(based on ICD 9 and Read Codes)
SLIDE 9 of 34
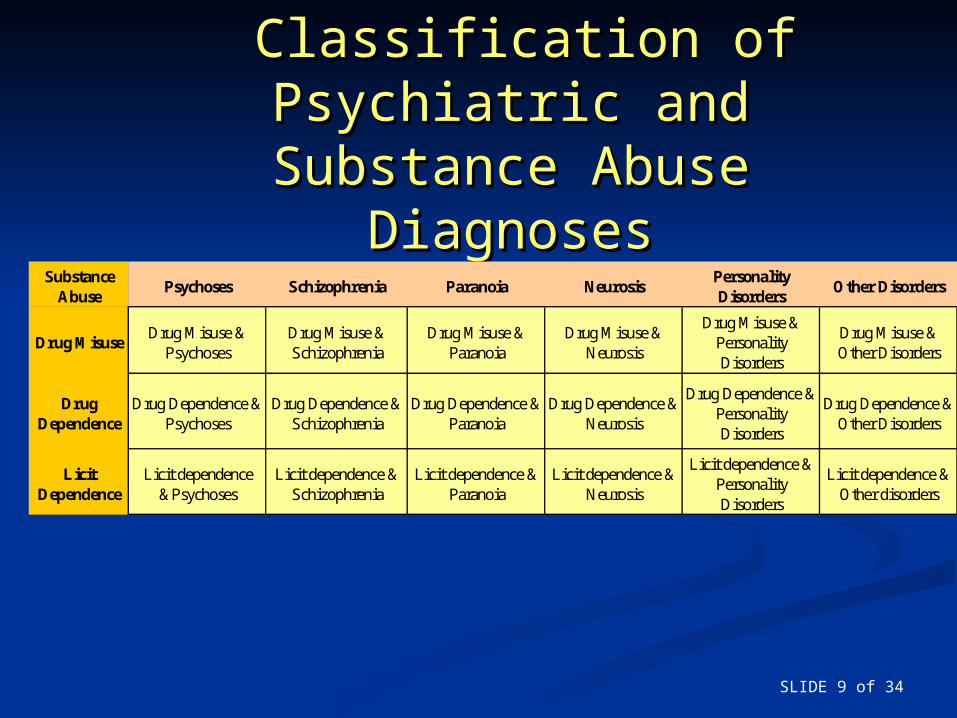
Classification of Psychiatric Classification of Psychiatric and Substance Abuse and Substance Abuse
DiagnosesDiagnosesSubstance
AbusePsychoses Schizophrenia Paranoia Neurosis
Personality Disorders
Other Disorders
Drug MisuseDrug Misuse &
PsychosesDrug Misuse & Schizophrenia
Drug Misuse & Paranoia
Drug Misuse & Neurosis
Drug Misuse & Personality Disorders
Drug Misuse & Other Disorders
Drug Dependence
Drug Dependence & Psychoses
Drug Dependence & Schizophrenia
Drug Dependence & Paranoia
Drug Dependence & Neurosis
Drug Dependence & Personality Disorders
Drug Dependence & Other Disorders
Licit Dependence
Licit dependence &Psychoses
Licit dependence & Schizophrenia
Licit dependence & Paranoia
Licit dependence & Neurosis
Licit dependence & Personality Disorders
Licit dependence & Other disorders
SLIDE 10 of 34
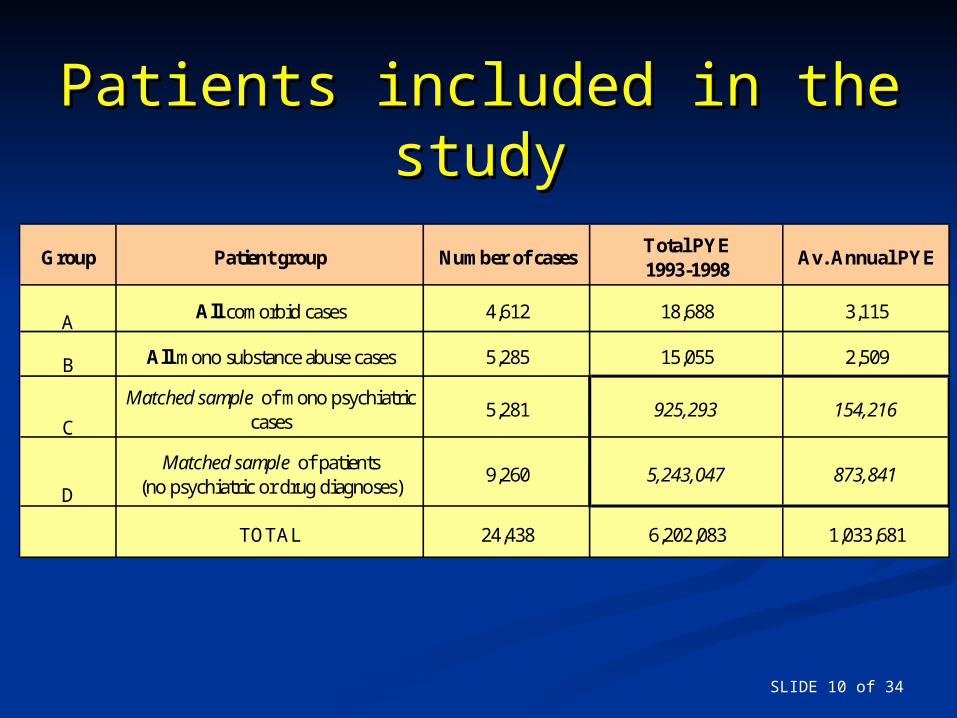
Patients included in the Patients included in the studystudy
Group Patient group Number of casesTotal PYE 1993-1998
Av. Annual PYE
AAll comorbid cases 4,612 18,688 3,115
B All mono substance abuse cases 5,285 15,055 2,509
C
Matched sample of mono psychiatric cases
5,281 925,293 154,216
D
Matched sample of patients (no psychiatric or drug diagnoses)
9,260 5,243,047 873,841
TOTAL 24,438 6,202,083 1,033,681
SLIDE 11 of 34
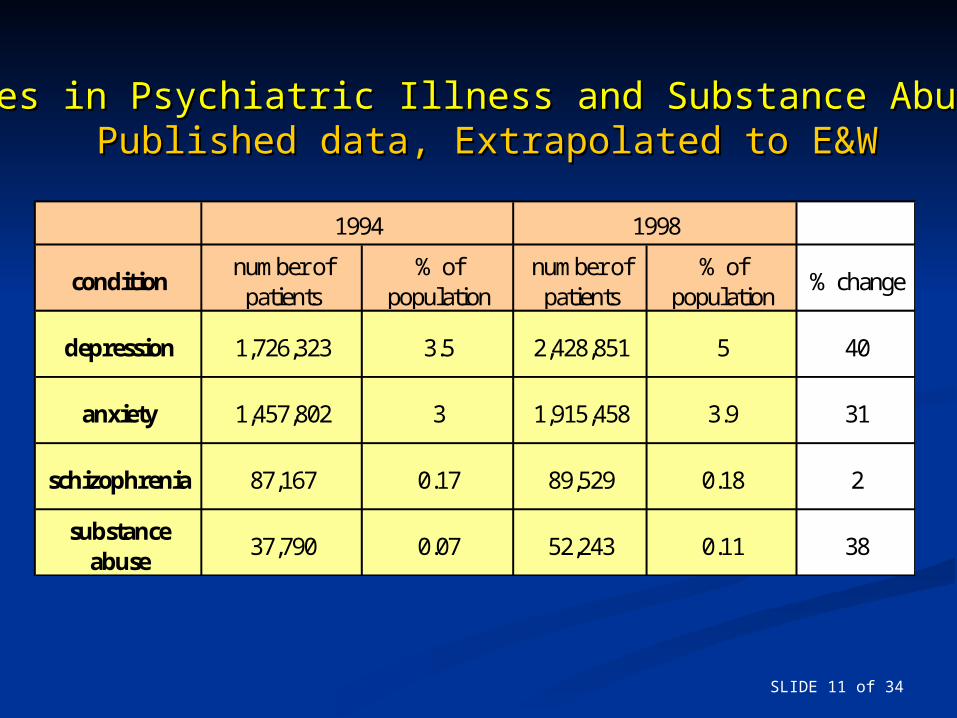
Changes in Psychiatric Illness and Substance Abuse UseChanges in Psychiatric Illness and Substance Abuse UsePublished data, Extrapolated to E&WPublished data, Extrapolated to E&W
conditionnumber of
patients% of
populationnumber of
patients% of
population% change
depression 1,726,323 3.5 2,428,851 5 40
anxiety 1,457,802 3 1,915,458 3.9 31
schizophrenia 87,167 0.17 89,529 0.18 2
substance abuse
37,790 0.07 52,243 0.11 38
1994 1998
SLIDE 12 of 34
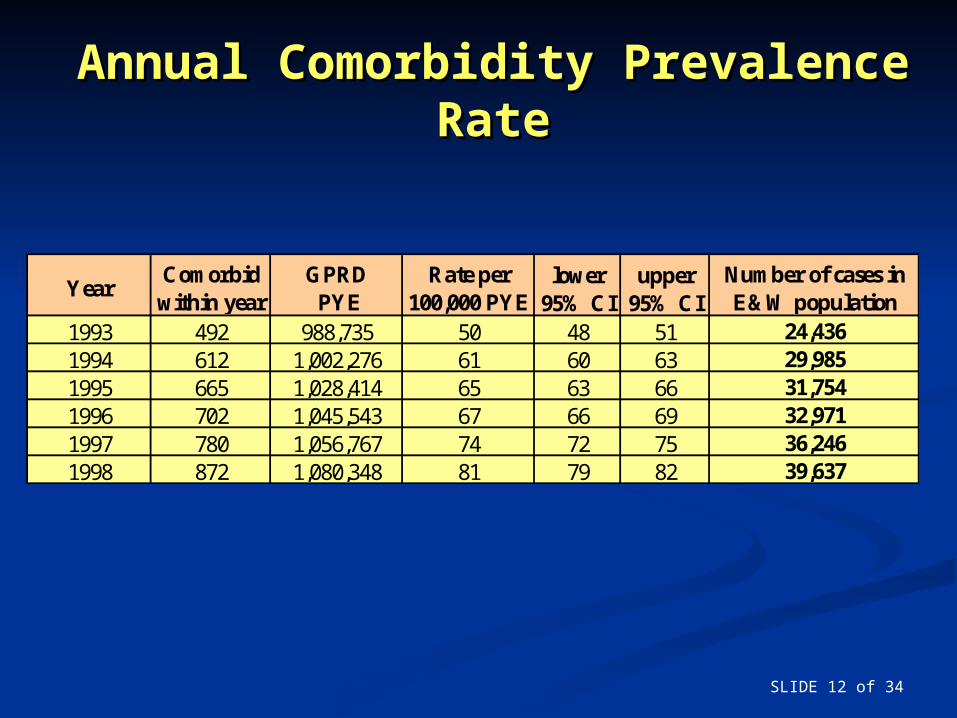
Annual Comorbidity Prevalence Annual Comorbidity Prevalence RateRate
YearComorbid
within yearGPRD PYE
Rate per 100,000 PYE
lower 95% CI
upper 95% CI
Number of cases in E&W population
1993 492 988,735 50 48 51 24,4361994 612 1,002,276 61 60 63 29,9851995 665 1,028,414 65 63 66 31,7541996 702 1,045,543 67 66 69 32,9711997 780 1,056,767 74 72 75 36,2461998 872 1,080,348 81 79 82 39,637
SLIDE 13 of 34
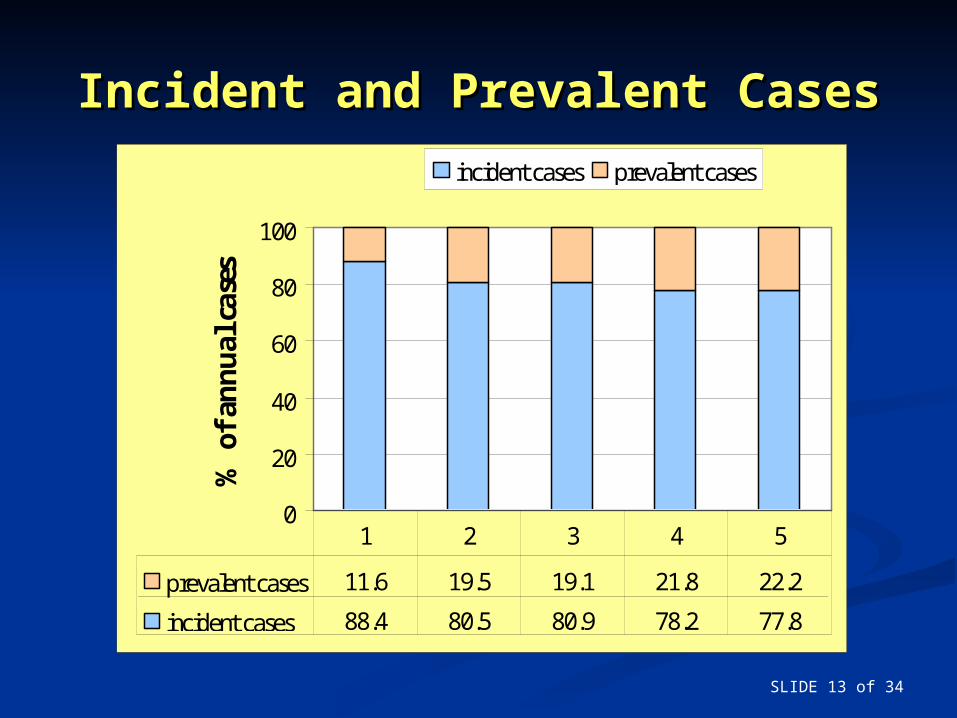
Incident and Prevalent CasesIncident and Prevalent Cases
0
20
40
60
80
100%
of
ann
ual
cas
es .
incident cases prevalent cases
prevalent cases 11.6 19.5 19.1 21.8 22.2
incident cases 88.4 80.5 80.9 78.2 77.8
1 2 3 4 5
SLIDE 14 of 34
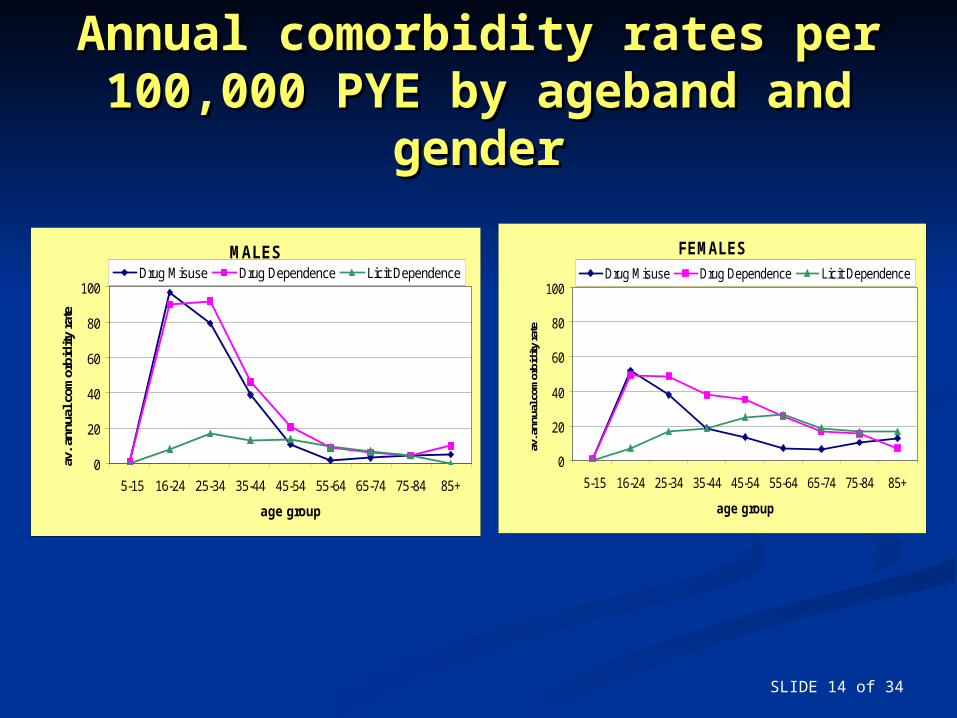
Annual comorbidity rates per Annual comorbidity rates per 100,000 PYE by ageband and 100,000 PYE by ageband and
gendergender
MALES
0
20
40
60
80
100
5-15 16-24 25-34 35-44 45-54 55-64 65-74 75-84 85+
age group
av. a
nnua
l com
orbi
dity
rat
e
Drug Misuse Drug Dependence Licit Dependence
FEMALES
0
20
40
60
80
100
5-15 16-24 25-34 35-44 45-54 55-64 65-74 75-84 85+
age group
av. a
nnua
l com
orbi
dity
rate
Drug Misuse Drug Dependence Licit Dependence
SLIDE 15 of 34
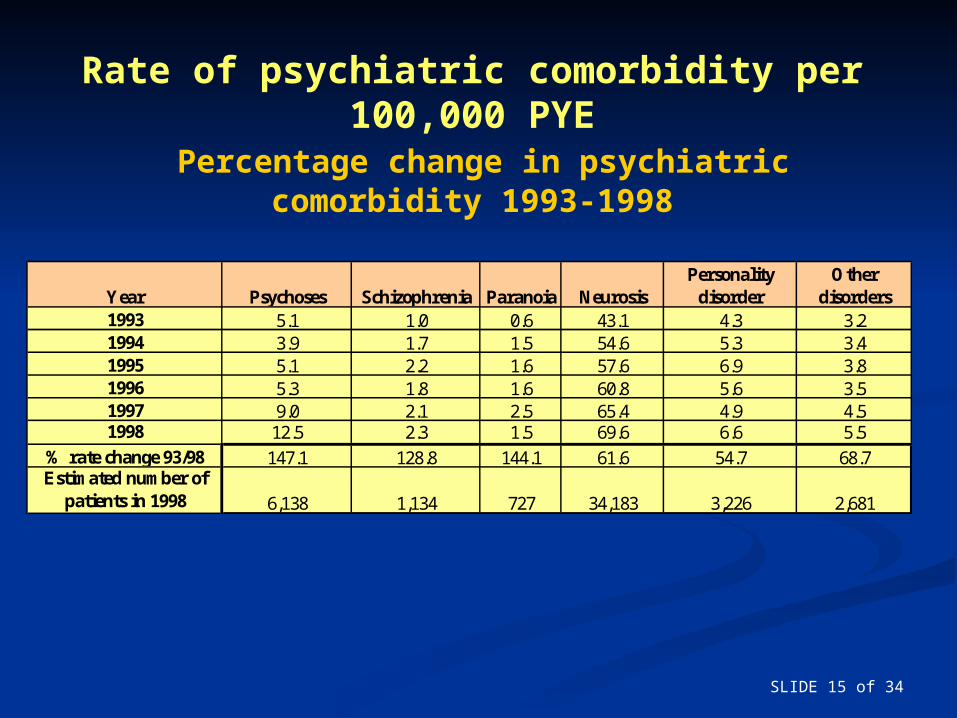
Rate of psychiatric comorbidity per 100,000 PYE
Percentage change in psychiatric comorbidity 1993-1998
Year Psychoses Schizophrenia Paranoia NeurosisPersonality
disorderOther
disorders1993 5.1 1.0 0.6 43.1 4.3 3.21994 3.9 1.7 1.5 54.6 5.3 3.41995 5.1 2.2 1.6 57.6 6.9 3.81996 5.3 1.8 1.6 60.8 5.6 3.51997 9.0 2.1 2.5 65.4 4.9 4.51998 12.5 2.3 1.5 69.6 6.6 5.5
% rate change 93/98 147.1 128.8 144.1 61.6 54.7 68.7Estimated number of
patients in 1998 6,138 1,134 727 34,183 3,226 2,681
SLIDE 16 of 34
Illicit Drug Use and Mental HealthIllicit Drug Use and Mental Health
‘‘Evidence establishes Evidence establishes clear link between clear link between use of cannabis and use of cannabis and mental health’mental health’
BMJ Editorial 2002BMJ Editorial 2002
SLIDE 17 of 34
Cannabis and Mental HealthCannabis and Mental Health
‘‘Cannabis use does not appear to be Cannabis use does not appear to be causally related to the causally related to the incidenceincidence of of schizophrenia’schizophrenia’
‘‘It may precipitate disorders in persons It may precipitate disorders in persons who are who are vulnerablevulnerable to developing to developing psychosis’psychosis’
Degenhardt et al Drug and Alcohol Dependence 2003Degenhardt et al Drug and Alcohol Dependence 2003
SLIDE 18 of 34
The move to causalityThe move to causality
Use of cannabis increases the risk of schizophrenia Use of cannabis increases the risk of schizophrenia and depression and depression but baseline psychiatric illness is not but baseline psychiatric illness is not associated with an elevated risk of substance useassociated with an elevated risk of substance use (Rey J and Tennant C. Cannabis and Mental Health. (Rey J and Tennant C. Cannabis and Mental Health. BMJ 2002; 325: 1183-4 2002).BMJ 2002; 325: 1183-4 2002).
““Use of cannabis will contribute to more Use of cannabis will contribute to more episodes or new cases of (psychiatric) illness”episodes or new cases of (psychiatric) illness” (assumes that cannabis use is increasing and/or) the (assumes that cannabis use is increasing and/or) the level of cannabis use among users is increasing).level of cannabis use among users is increasing).
““Surprising that, given this association, there Surprising that, given this association, there does not appear to increasing incidence of does not appear to increasing incidence of schizophrenia in the population”.schizophrenia in the population”.
SLIDE 19 of 34
Substance misuse can have a negative impact Substance misuse can have a negative impact upon the course of psychotic disorders and can upon the course of psychotic disorders and can exacerbate symptomsexacerbate symptoms
Some substances, particularly alcohol, Some substances, particularly alcohol, cannabinoids, hallucinogens and stimulants can cannabinoids, hallucinogens and stimulants can produce psychotic symptoms directly without produce psychotic symptoms directly without coincidental mental illness.coincidental mental illness.
Although these substances may trigger Although these substances may trigger psychotic disorders amongst people with a psychotic disorders amongst people with a predisposition, the existence of any stronger predisposition, the existence of any stronger causal relationship remains controversialcausal relationship remains controversial..
Does Substance Misuse Cause Mental Illness?Consensus Pre BMJ

SLIDE 20 of 34
Some reports suggest cannabis Some reports suggest cannabis exacerbates symptoms of schizophrenia, exacerbates symptoms of schizophrenia, but two clinical studies suggest but two clinical studies suggest cannabis use alleviates symptoms.cannabis use alleviates symptoms.
Cannabis use is not associated with the Cannabis use is not associated with the development of psychosis in an 'ultra' development of psychosis in an 'ultra' high-risk group high-risk group Aust N Z J PsychiatryAust N Z J Psychiatry 2002 2002
Is the evidence clear?
SLIDE 21 of 34
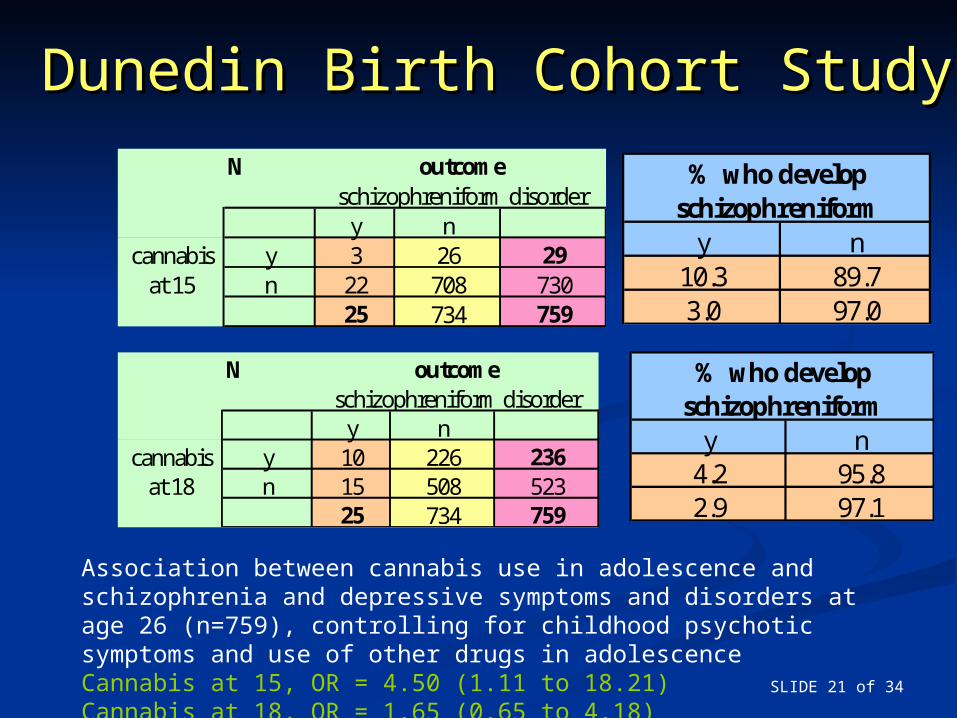
Dunedin Birth Cohort StudyDunedin Birth Cohort Study
Association between cannabis use in adolescence and schizophrenia and depressive symptoms and disorders at age 26 (n=759), controlling for childhood psychotic symptoms and use of other drugs in adolescenceCannabis at 15, OR = 4.50 (1.11 to 18.21)Cannabis at 18, OR = 1.65 (0.65 to 4.18)
N
y ncannabis y 3 26 29
at 15 n 22 708 73025 734 759
outcomeschizophreniform disorder
y n10.3 89.73.0 97.0
% who develop schizophreniform
N
y ncannabis y 10 226 236
at 18 n 15 508 52325 734 759
outcomeschizophreniform disorder
y n4.2 95.82.9 97.1
% who develop schizophreniform
SLIDE 22 of 34
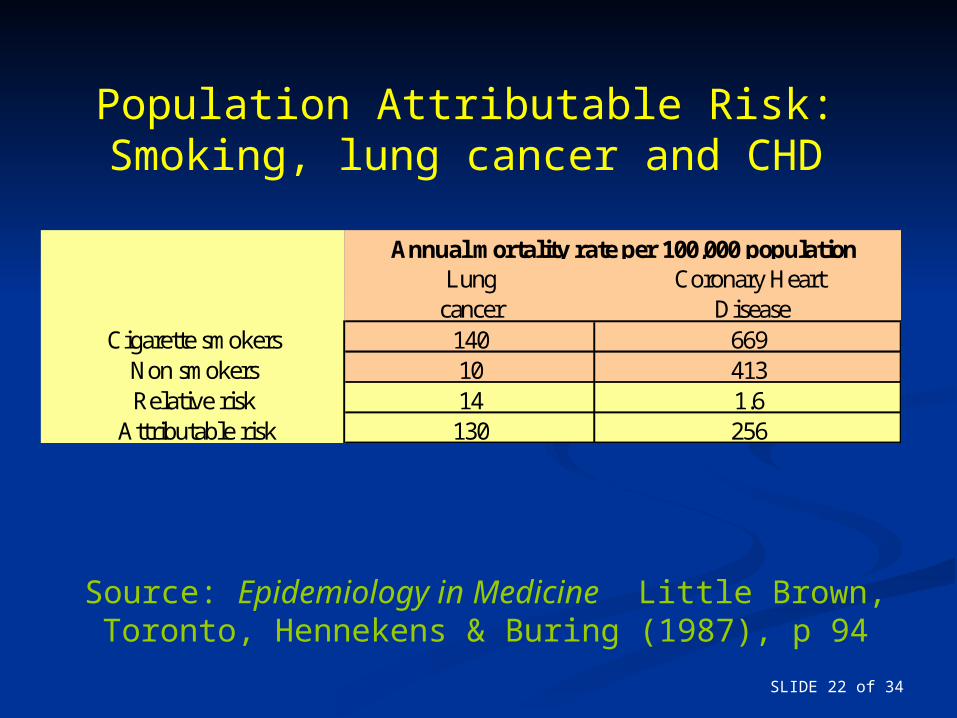
Source: Epidemiology in Medicine Little Brown, Toronto, Hennekens & Buring (1987), p 94
Population Attributable Risk:Smoking, lung cancer and CHD
Lungcancer
Coronary Heart Disease
Cigarette smokers 140 669Non smokers 10 413Relative risk 14 1.6
Attributable risk 130 256
Annual mortality rate per 100,000 population
SLIDE 23 of 34
GPRD Study questionsGPRD Study questions
1.1. What is the relative risk of psychiatric What is the relative risk of psychiatric illness among substance abusers illness among substance abusers compared to non substance abusers?compared to non substance abusers?
2.2. What is the relative risk of substance What is the relative risk of substance abuse among psychiatric cases abuse among psychiatric cases compared to non psychiatric cases?compared to non psychiatric cases?
3.3. How has the proportion of comorbid How has the proportion of comorbid patients with a primary substance abuse patients with a primary substance abuse diagnosis changed from 1993 to 1998?diagnosis changed from 1993 to 1998?
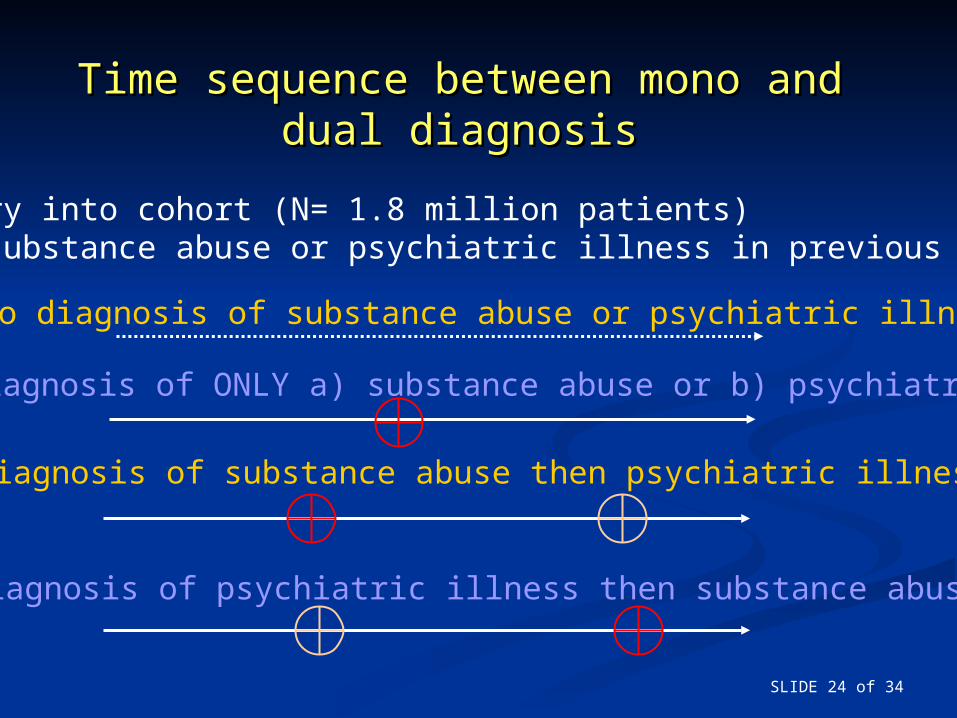
SLIDE 24 of 34
Time sequence between mono and Time sequence between mono and dual diagnosisdual diagnosis
Entry into cohort (N= 1.8 million patients)No substance abuse or psychiatric illness in previous year
1 No diagnosis of substance abuse or psychiatric illness
3 Diagnosis of substance abuse then psychiatric illness
4 Diagnosis of psychiatric illness then substance abuse
2 Diagnosis of ONLY a) substance abuse or b) psychiatric illness
SLIDE 25 of 34
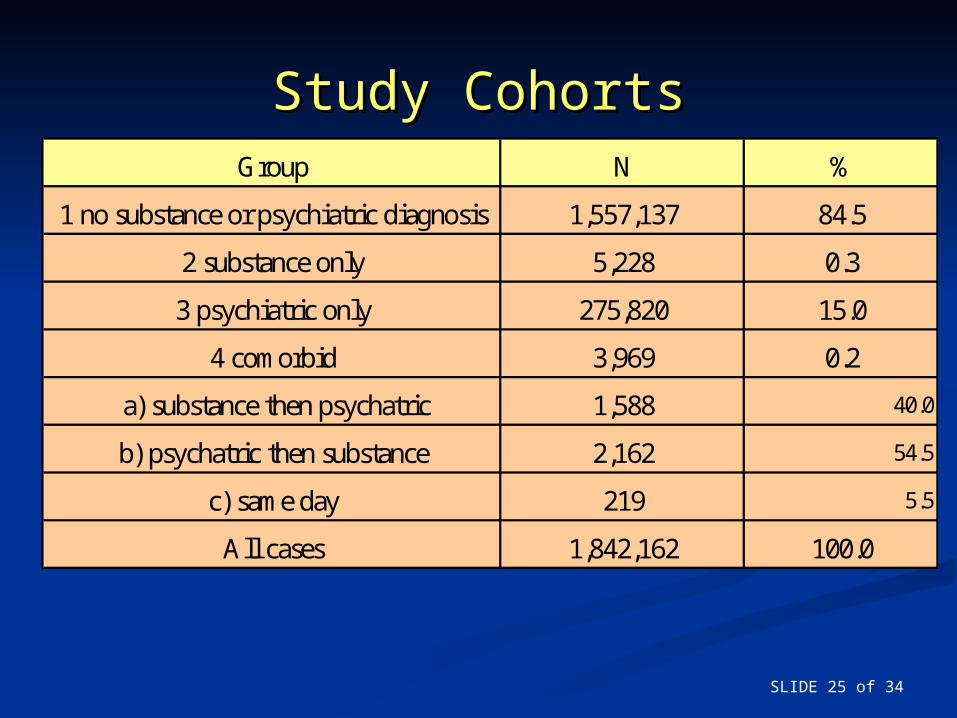
Study CohortsStudy CohortsGroup N %
1 no substance or psychiatric diagnosis 1,557,137 84.5
2 substance only 5,228 0.3
3 psychiatric only 275,820 15.0
4 comorbid 3,969 0.2
a) substance then psychatric 1,588 40.0
b) psychatric then substance 2,162 54.5
c) same day 219 5.5
All cases 1,842,162 100.0
SLIDE 26 of 34
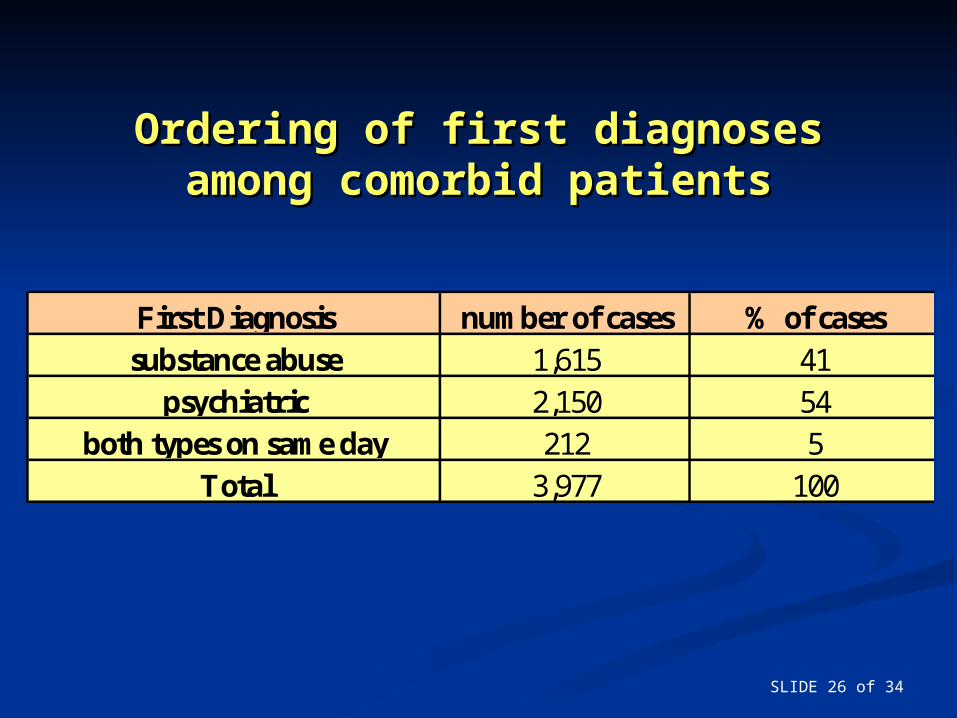
Ordering of first diagnoses Ordering of first diagnoses among comorbid patientsamong comorbid patients
First Diagnosis number of cases % of casessubstance abuse 1,615 41
psychiatric 2,150 54both types on same day 212 5
Total 3,977 100
SLIDE 27 of 34
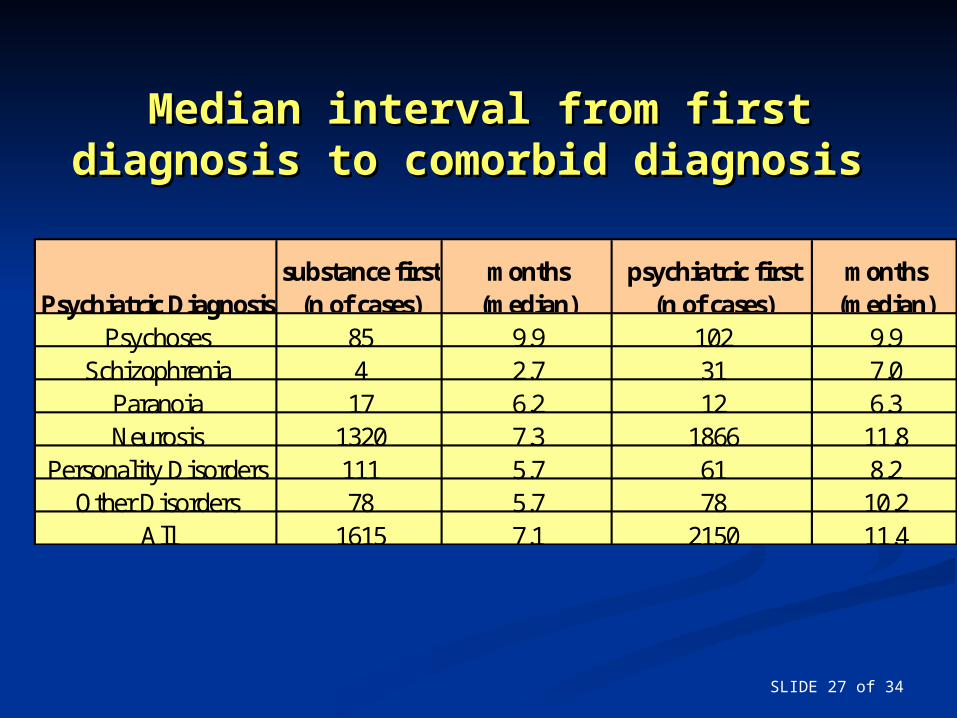
Median interval from first diagnosis to Median interval from first diagnosis to comorbid diagnosiscomorbid diagnosis
Psychiatric Diagnosissubstance first
(n of cases)months
(median)psychiatric first
(n of cases)months
(median)Psychoses 85 9.9 102 9.9
Schizophrenia 4 2.7 31 7.0Paranoia 17 6.2 12 6.3Neurosis 1320 7.3 1866 11.8
Personality Disorders 111 5.7 61 8.2Other Disorders 78 5.7 78 10.2
All 1615 7.1 2150 11.4
SLIDE 28 of 34
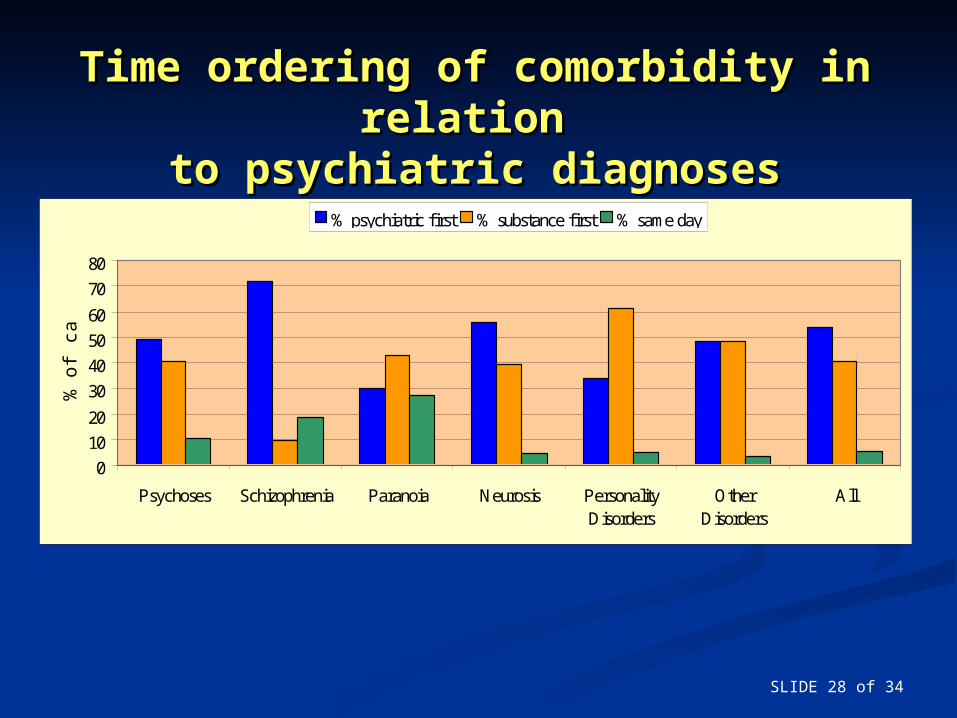
Time ordering of comorbidity in Time ordering of comorbidity in relation relation
to psychiatric diagnosesto psychiatric diagnoses
0
10
20
30
40
50
60
70
80
Psychoses Schizophrenia Paranoia Neurosis PersonalityDisorders
OtherDisorders
All
% o
f ca
ses
% psychiatric first % substance first % same day
SLIDE 29 of 34
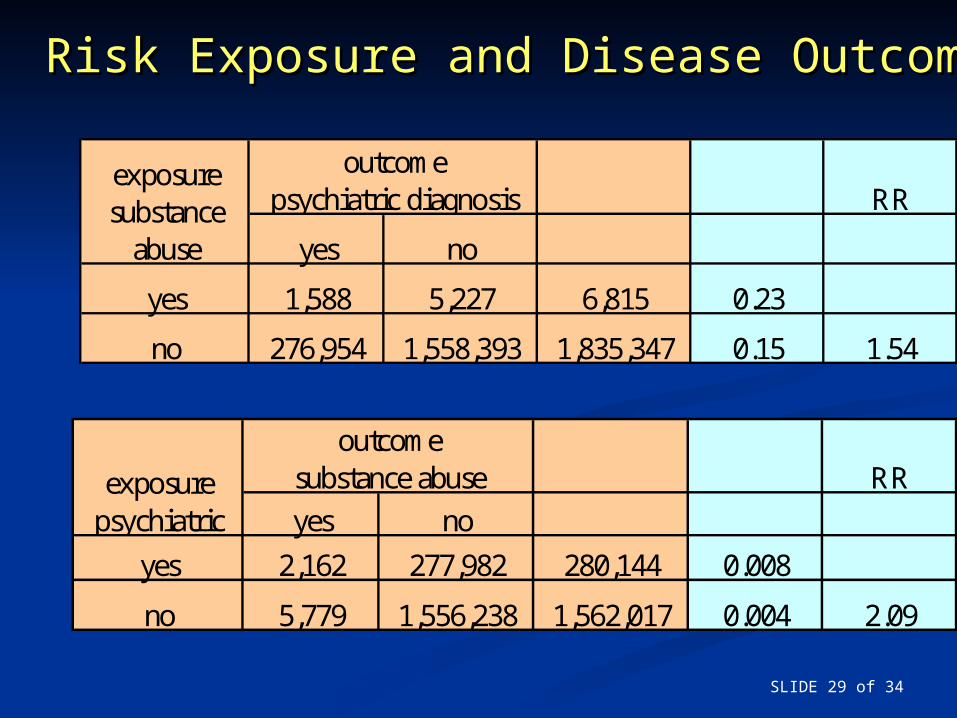
Risk Exposure and Disease OutcomeRisk Exposure and Disease Outcome
RR
yes no
yes 1,588 5,227 6,815 0.23
no 276,954 1,558,393 1,835,347 0.15 1.54
outcomepsychiatric diagnosis
exposure substance
abuse
RR
yes no
yes 2,162 277,982 280,144 0.008
no 5,779 1,556,238 1,562,017 0.004 2.09
exposure psychiatric
outcomesubstance abuse
SLIDE 30 of 34
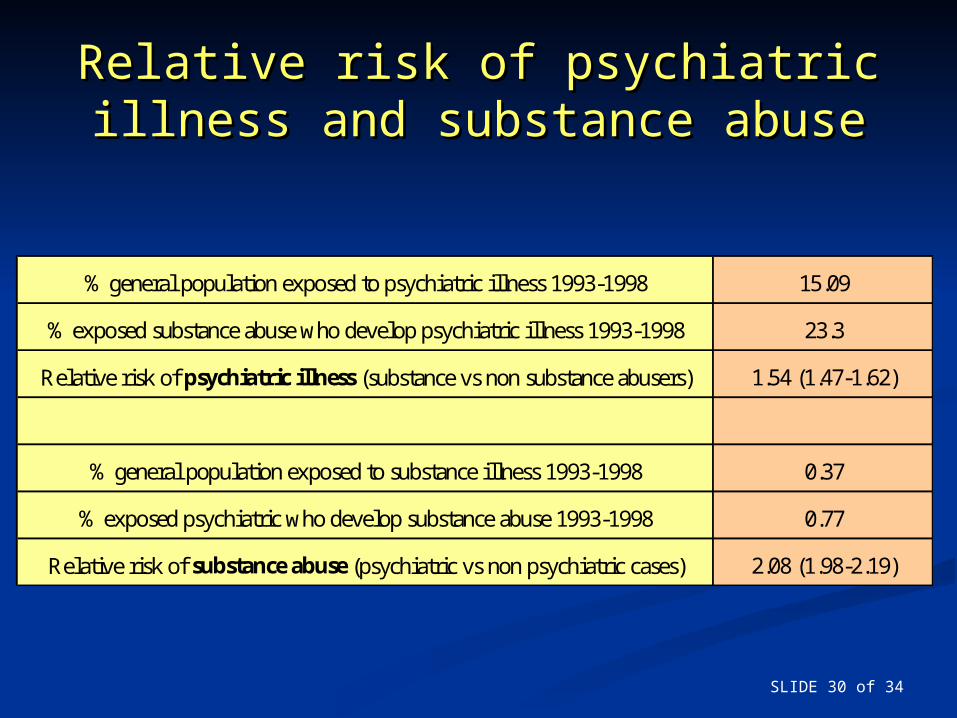
Relative risk of psychiatric illness Relative risk of psychiatric illness and substance abuseand substance abuse
% general population exposed to psychiatric illness 1993-1998 15.09
% exposed substance abuse who develop psychiatric illness 1993-1998 23.3
Relative risk of psychiatric illness (substance vs non substance abusers) 1.54 (1.47-1.62)
% general population exposed to substance illness 1993-1998 0.37
% exposed psychiatric who develop substance abuse 1993-1998 0.77
Relative risk of substance abuse (psychiatric vs non psychiatric cases) 2.08 (1.98-2.19)
SLIDE 31 of 34
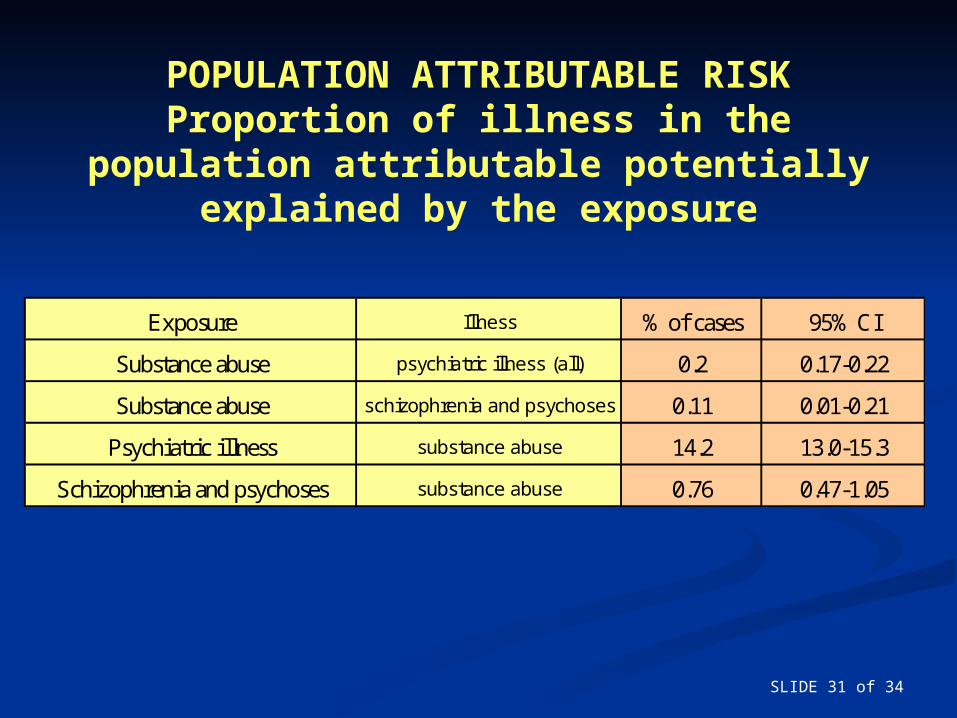
POPULATION ATTRIBUTABLE RISKProportion of illness in the
population attributable potentially explained by the exposure
Exposure Illness % of cases 95% CI
Substance abuse psychiatric illness (all) 0.2 0.17-0.22
Substance abuse schizophrenia and psychoses 0.11 0.01-0.21
Psychiatric illness substance abuse 14.2 13.0-15.3
Schizophrenia and psychoses substance abuse 0.76 0.47-1.05
SLIDE 32 of 34
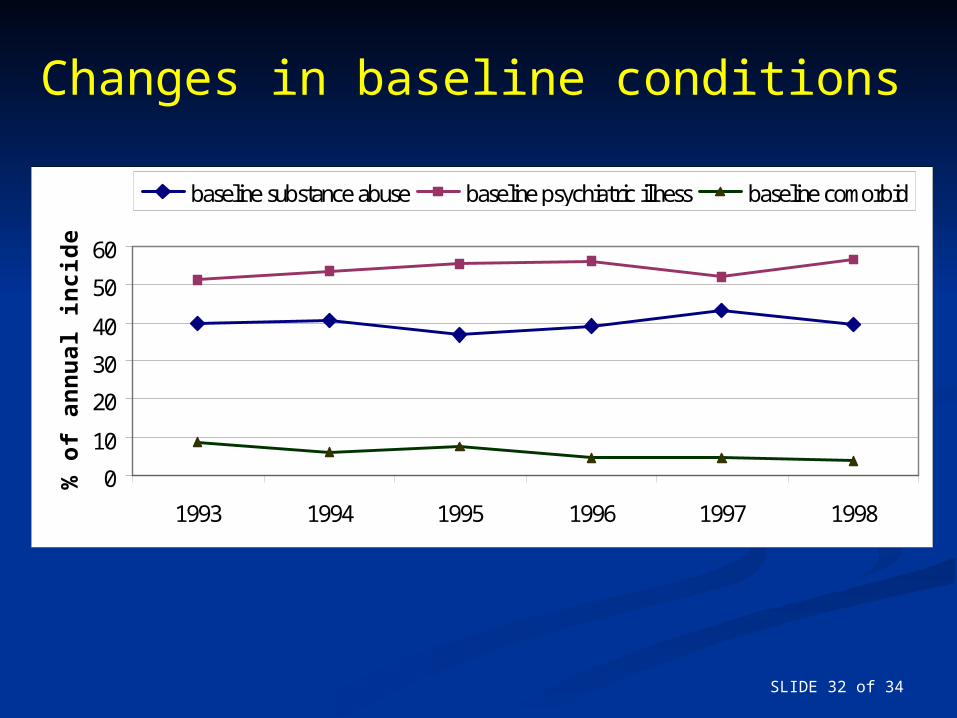
Changes in baseline conditions
0
10
20
30
40
50
60
1993 1994 1995 1996 1997 1998
% o
f an
nu
al in
cid
ent
case
s
baseline substance abuse baseline psychiatric illness baseline comorbid
SLIDE 33 of 34
Summary (1)Summary (1) The numbers of individuals newly The numbers of individuals newly
developing comorbidity in primary developing comorbidity in primary care is increasing year-on-year.care is increasing year-on-year.
Does the increase in comorbidity Does the increase in comorbidity reported here represent an actual reported here represent an actual increase in the prevalence of increase in the prevalence of comorbid conditions or the comorbid conditions or the medicalisation of social, economic medicalisation of social, economic or personal problems?or personal problems?
SLIDE 34 of 34
Summary (2)Summary (2)
Does active early recognition of Does active early recognition of comorbidity lead to better outcomes? comorbidity lead to better outcomes?
The findings of the present study do not The findings of the present study do not contradict studies in different contradict studies in different populations which have found a link populations which have found a link between certain forms of drug use and between certain forms of drug use and psychiatric illness. However they psychiatric illness. However they suggest that attempts to prevent suggest that attempts to prevent comorbidity by focusing on substance comorbidity by focusing on substance abuse will meet with only very limited abuse will meet with only very limited successsuccess..





























