Embed Size (px)
Citation preview

Slipped Capital Femoral Epiphysis Occurred in Patients over 20 Years - Two cases -
Slipped Capital Femoral Epiphysis Occurred in Patients over 20 Years - Two cases -
Sung-Taek Jung
Jin Choi
Bong-Hyun Bae
Yong-Uk Kim*
Sung-Man Rowe
Department of Orthopedics Chonnam National University Hospital,
Department of OrthopedicsGwangju City Hospital *

Case 1
• 30 year-old, male • C/C: Left hip pain & restriction of joint movement (minor trauma 7 days prior to visit)

• P/H: Surgical removal of pituitary gland at 17 year-old d/t craniopharyngioma Residual tumor resection at 22 year-old
Case 1
• Chronologic Age: 30 year-old
• Bone Age: 13 year-old
• Height: 157 cm
• Weight: 40 Kg
• Small genitalia
• No pubic & axillary hair

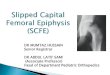
Case 1
• Radiographic findings (Preop)

Case 1
• Endocrinologic lab. findings
Hormone Patient Normal level
T3 63 ng/dl 80-220
Free T4 0.14 ng/dl 0.7-2
LH 0.21 mIU/ml 10-25
FSH 0.01 mIU/ml 10-30
Growth H <0.1 ng/ml 1-5
Testosterone <0.01 ng/ml 1.88-8.96
Cortisol <0.1 ug/dl 3-23
Prolactin 6.59 ng/ml 0-25
• Chromosomal study : 46, XY
T3; triiodothyronine, T4; thyroxine, LH; luteinizing hormone, FHS; follicular stimulating hormone

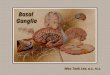
Case 1
• Radiographic findings (Postop)

Case 2
• 24 year-old, female • C/C: Left hip pain & restriction of joint movement ( slip down 3 weeks prior to visit)

• Chronologic Age: 24 year-old
• Bone Age: 12.6 year-old
• Height: 173 cm
• Weight: 55.8 Kg
• No closure of epiphyseal plates
• Brain MRI: Non-specific finding
Case 2
• P/H: Growth hormone therapy at 12 year-old d/t short stature

• Amenorrhea
• Breast: Tanner stage I
• No pubic & axillary hair
• Sonography: 2 cm sized uterus & no ovary
Case 2

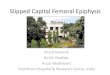
Case 2
• Radiographic findings (Preop)

Case 2
• Endocrinologic lab. findings
Hormone Patient Normal level
T3 123 ng/dl 80-220
T4 5.6 ng/dl 4.5-12.5
LH 0.01 mIU/ml 10-25
FSH 0.30 mIU/ml 10-30
Estradiol 20 pg/ml 30-120
Growth H <0.1 ng/ml 1-5
Cortisol 0.1 ug/dl 3-23
Prolactin 11.15 ng/ml 0-25
• Chromosomal study : 46, XX
T3; triiodothyronine, T4; thyroxine, LH; luteinizing hormone, FHS; follicular stimulating hormone

Case 2
• Radiographic findings (Postop)

DiscussionDiscussion

- Zondek, 1936 - Rubinsten, 1939
- Ray et al, 1941 - Gardner et al, 1943
- Harris, 1950 - Chung, 1976
Endocrinopathy in SCFEEndocrinopathy in SCFE• Growth hormone (GH)
Proliferation of chondrocytes Accelerated development of epiphysis Weakened the support for the shear force
• Sex hormone (SH) Suppress the proliferation of chondrocytes Termination of growth of physeal plate

• Absolute increase of GH
• Absolute decrease of SH
• Relative reduction of SH
• Thickness of physeal plate
• Weakened binding of epiphysis to metaphysis
SCFE

• Hypothyroidism
• Hypogonadism
• Panhypopituitarism
• Growth hormone therapy
EndocrinologicEndocrinologic factorsfactors

Ratio of GH & SHRatio of GH & SHCase I Patient Normal Growth H <0.1 ng/ml 1-5
Testosterone <0.01 ng/ml 1.88-8.96
Ratio (G/S) 10/1 1/8.9 ~ 2.7/1
Case II Growth H <0.1 ng/ml 1-5
Estradiol 20 pg/ml 30 -120
Ratio (G/S) 5/1 8.3/1 ~ 166.7/1
Growth hormone therapy history (+)
SCFE in HypopituitarismSCFE in Hypopituitarism

• Preop. & Postop. Management Preop. & Postop. Management : Glucocorticoids should be administered

• Reported SCFE with hypopituitarism: Kim et al, 1988 Moorefield et al, 1976
• Proper management : Preop. & Postop. Glucocorticoids Prophylactic pinning
• Incidence of pituitary tumor: 1.6~1.8 / 100,000
Discussion PointsDiscussion Points
Be aware of Possibility of Be aware of Possibility of SCFE with hypopituitarism SCFE with hypopituitarism

Thank You for
Your Kind Attention !
Thank You for
Your Kind Attention !