-
Vincenzo Foppa, 1462“The miracle of the salvaged foot” Cappella
Portinari, S. Eustorgio Church Milan, Italy
Small artery disease (SAD) and medial artery calcification (MAC)
are changing the fate of CLI patients
-
- SAD is a major cause of CLTI
- MAC is strongly associated with PAD
- Are SAD & MAC the same non-atherosclerotic disease?
- SAD-MAC is a leading actor in CLI pts
SAD: small artery diseaseMAC: medial artery calcification
-
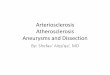
Claudicants CLTI
0.51 (0.29 - 0.89)
0 artery ref.1 artery 1.7 (0.76 - 3.83)2 arteries 1.86 (0.72 -
4.83)3 arteries 4.84 (1.12 - 20.88)
0 artery ref.1 artery 1.69 (0.74 - 3.87)2 arteries 5.81 (1.91 -
17.62)3 arteries 5.71 (1.03 - 31.78)
Any of BTA and Arch
13.25 (1.69 - 104.16)
0.53 (0.26 - 1.1)
1.17 (0.68 – 2.01)
Prox
BTK
Dist
BTK
BTA
vessels
Arch
P-TPT
SFA
ATG
Aggregated segments
Risk factors for CLTIOdds Ratio (95% CI)
-
SAD is strongly and independently associated with CLTI, diabetes
and dialysis and must be considered as a leading actor in CLTI
-
- SAD is a major cause of CLTI
- MAC is strongly associated with PAD
- Are SAD & MAC the same non-atherosclerotic disease?
- SAD-MAC is a leading actor in CLI pts
SAD: small artery diseaseMAC: medial artery calcification
-
What is MAC?
MAC, also known as Mönckeberg's medial
sclerosis, occurs independently of
atherosclerosis and is strongly associated with
aging, DM and CKD. MAC tends to affect the
artery diffusely, appearing as a linear
contiguous rail-track pattern of calcification
on plain radiography.
MAC is a strong marker of future
cardiovascular events and death
P. Lanzer et al., “Medial vascular calcification revisited:
review and
perspectives,” Eur. Heart J., vol. 35, no. 23, pp. 1515–1525,
Jun. 2014
K. L. Jablonski and M. Chonchol, “Vascular calcification in
end-stage
renal disease,” Hemodial. Int. Int. Symp. Home Hemodial., vol.
17 Suppl
1, pp. S17-21, Oct. 2013
K. J. Rocha-Singh, T. Zeller, and M. R. Jaff, “Peripheral
arterial
calcification: prevalence, mechanism, detection, and
clinical
implications,” Catheter. Cardiovasc. Interv. Off. J. Soc. Card.
Angiogr.
Interv., vol. 83, no. 6, pp. E212-220, May 2014
W. L. Lau and J. H. Ix, “Clinical detection, risk factors,
and
cardiovascular consequences of medial arterial calcification: a
pattern
of vascular injury associated with aberrant mineral
metabolism,”
Semin. Nephrol., vol. 33, no. 2, pp. 93–105, Mar. 2013
S. Lehto et al. “Medial artery calcification. A neglected
harbinger of
cardiovascular complications in non-insulin-dependent
diabetes
mellitus,” Arterioscler. Thromb. Vasc. Biol., vol. 16, no. 8,
pp. 978–983,
Aug. 1996
L. Niskanen et al. “Medial artery calcification predicts
cardiovascular
mortality in patients with NIDDM,” Diabetes Care, vol. 17, no.
11, pp.
1252–1256, Nov. 1994
G. M. London et al. “Arterial media calcification in end-stage
renal
disease: impact on all-cause and cardiovascular mortality,”
Nephrol.
Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. - Eur.
Ren. Assoc.,
vol. 18, no. 9, pp. 1731–1740, Sep. 2003
-
MAC & PAD are strongly associated
Histopathological studies on amputated limbs
of patients with PAD demonstrated that MAC
is highly prevalent, suggesting MAC as one of
the main determinants of PAD, in
combination or not with atherosclerosis
MAC and elevated ABI are associated with
foot ulcer, occlusive PAD and amputation
G. S. Soor et al. “Peripheral vascular disease: who gets it and
why? A
histomorphological analysis of 261 arterial segments from 58
cases,” Pathology
(Phila.), vol. 40, no. 4, pp. 385–391, Jun. 2008
N. Narula et al., “Pathology of Peripheral Artery Disease in
Patients With Critical Limb
Ischemia,” J. Am. Coll. Cardiol., vol. 72, no. 18, pp.
2152–2163, 30 2018
W. C. O’Neill et al. “Prevalence of nonatheromatous lesions in
peripheral arterial
disease,” Arterioscler. Thromb. Vasc. Biol., vol. 35, no. 2, pp.
439–447, Feb. 2015
J. A. Mustapha et al. “Infrapopliteal calcification patterns in
critical limb ischemia:
diagnostic, pathologic and therapeutic implications in the
search for the endovascular
holy grail,” J. Cardiovasc. Surg. (Torino), vol. 58, no. 3, pp.
383–401, Jun. 2017
C. David Smith et al. “Medial artery calcification as an
indicator of diabetic peripheral
vascular disease,” Foot Ankle Int., vol. 29, no. 2, pp. 185–190,
Feb. 2008, doi:
10.3113/FAI.2008.0185.
N. Abou-Hassan et al. “The clinical significance of medial
arterial calcification in end-
stage renal disease in women,” Kidney Int., vol. 87, no. 1, pp.
195–199, Jan. 2015
W. S. An et al., “Vascular calcification score on plain
radiographs of the feet as a
predictor of peripheral arterial disease in patients with
chronic kidney disease,” Int.
Urol. Nephrol., vol. 42, no. 3, pp. 773–780, Sep. 2010
M. S. Randhawa et al. “Prevalence of Tibial Artery and Pedal
Arch Patency by
Angiography in Patients With Critical Limb Ischemia and
Noncompressible Ankle
Brachial Index,” Circ. Cardiovasc. Interv., vol. 10, no. 5, May
2017
V. Aboyans et al. “The association between elevated ankle
systolic pressures and
peripheral occlusive arterial disease in diabetic and
nondiabetic subjects,” J. Vasc.
Surg., vol. 48, no. 5, pp. 1197–1203, Nov. 2008
E. Lew et al. “Lower extremity amputation risk factors
associated with elevated ankle
brachial indices and radiographic arterial calcification,” J.
Foot Ankle Surg. Off. Publ.
Am. Coll. Foot Ankle Surg., vol. 54, no. 3, pp. 473–477, Jun.
2015
-
The wrong concept:MAC as a non-obstructive disease
Despite this strong association between MAC
and PAD, the interaction in determining the
clinical manifestations of the disease is still
unknown, essentially because MAC is
considered by most authors a “non-
obstructive” disease.
Due to this concept, the hypothetic
“mechanisms of action” are supposed to be
indirect effects of the arterial wall stiffening:
loss of vasomotion and adverse remodeling
predisposing to an accelerated vascular aging,
atherosclerosis and plaque rupture
P. Lanzer et al., “Medial vascular calcification revisited:
review and
perspectives,” Eur. Heart J., vol. 35, no. 23, pp. 1515–1525,
Jun. 2014
K. J. Rocha-Singh, T. Zeller, and M. R. Jaff, “Peripheral
arterial
calcification: prevalence, mechanism, detection, and
clinical
implications,” Catheter. Cardiovasc. Interv. Off. J. Soc. Card.
Angiogr.
Interv., vol. 83, no. 6, pp. E212-220, May 2014
J. A. Mustapha, L. J. Diaz-Sandoval, and F. Saab,
“Infrapopliteal
calcification patterns in critical limb ischemia: diagnostic,
pathologic
and therapeutic implications in the search for the endovascular
holy
grail,” J. Cardiovasc. Surg. (Torino), vol. 58, no. 3, pp.
383–401, Jun.
2017
C. Y. Ho and C. M. Shanahan, “Medial Arterial Calcification:
An
Overlooked Player in Peripheral Arterial Disease,”
Arterioscler.
Thromb. Vasc. Biol., vol. 36, no. 8, pp. 1475–1482, 2016,
doi:
10.1161/ATVBAHA.116.306717.
P.-W. Fok and P. Lanzer, “Media sclerosis drives and
localizes
atherosclerosis in peripheral arteries,” PloS One, vol. 13, no.
10, p.
e0205599, 2018
-
- SAD is a major cause of CLTI
- MAC is strongly associated with PAD
- Are SAD & MAC the same non-atherosclerotic disease?
- SAD-MAC is a leading actor in CLI pts
SAD: small artery diseaseMAC: medial artery calcification
-
At the best of our knowledge, SAD and MAC were
never considered directly correlated
However, in our daily practice in treating CLTI patients,
we very often observe their coexistence, raising the
question if they could be expression of different
pathophysiological conditions or of the same
underlying non-atherosclerotic disease, leading to
common clinical symptoms
-
In our daily practice we
observe a strong association
between SAD & MAC
-
N
Patients 221 100%
Mean age 74 yy
Male 194 76%
DM 191 86%
ESRD-HD 53 24%
Limbs 259 100%
WIfI-WOUND 1 37 14%
WIfI-WOUND 2 198 77%
WIfI-WOUND 3 24 9%
Mean FU19 months
(3-59)
Preliminary analysis, preparing for publication
Pts selection criteria
- 2014-2018
- Consecutive CLTI pts →WIfI Ischemia grade 3
- Tissue loss → RTF 5-6 = WIfI Wound 1-2-3
- Pts with a detailed angiographic imaging of the foot vessels
in 2 projections
- Patients living in our region followed in our outpatient
clinic
Study on MAC-score & SAD-score
-
No SADAbsence of disease or mild disease with a well-represented
network of forefoot and calcaneal arteries
Moderate SADDiffuse disease with narrowing and poverty of arch,
metatarsal, digital and calcaneal arteries
Severe SAD Occlusion or severe disease with extreme poverty of
arch, metatarsal, digital and calcaneal arteries
SAD-score
-
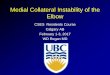
- 5-steps MAC-score- Simple foot X-ray: latero-lateral and
antero-posterior- Look for “rail-tracking” calcification length
0-1 ≥20 mm
0-1≥10 mm
0-1 ≥20 mm
0-1 ≥20 mm
0-1 ≥10 mm
0-1 ≥10 mm
0-1 ≥10 mm
MAC-score
-
Preliminary analysis, preparing for publication
MAC-scoreNo MAC
21%
Moderate MAC35%
Severe MAC44%
0-1 = no-MAC
2-3 = moderate MAC
4-5 = severe MAC
Distribution in 259 CLTI-limbs
SAD-score
No-SAD26%
Moderate SAD29%
Severe SAD45%
-
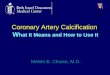
MAC-score versus SAD-score
MAC-score sensitivity specificity
0-1 no-MAC 100 % 98.1 %
2-3 moderate MAC 99.1 % 92.7 %
4-5 severe MAC 100 % 98.1 %
Preliminary analysis, preparing for publication
-
MAC-score versus SAD-score
SAD & MAC are the same disease! From now on I will talk
about SAD-MAC
Preliminary analysis, preparing for publication
-
- SAD is a major cause of CLTI
- MAC is strongly associated with PAD
- Are SAD & MAC the same non-atherosclerotic disease?
- SAD-MAC is a leading actor in CLI pts
SAD: small artery diseaseMAC: medial artery calcification
-
Healing rate
Global population MAC-score groups SAD-score groups
Preliminary analysis, preparing for publication
-
Limb salvage
Preliminary analysis, preparing for publication
Global population MAC-score groups SAD-score groups
-
Survival
Preliminary analysis, preparing for publication
Global population MAC-score groups SAD-score groups
-
Survival
Preliminary analysis, preparing for publication
Global population MAC-score groups SAD-score groups
-
Amputation-free survival
Preliminary analysis, preparing for publication
Global population MAC-score groups SAD-score groups
-
Freedom from foot surgical reintervention
Preliminary analysis, preparing for publication
Global population MAC-score groups SAD-score groups
-
Freedom from redo-PTA
Preliminary analysis, preparing for publication
Global population MAC-score groups SAD-score groups
-
SAD-MAC is a single non-atherosclerotic disease and must be
considered the leading actor in CLTI
CLTI-pts with high SAD-MAC scores present at 2yy:- only 30%
healing rate without reulceration- double risk of major amputation
and death- higher rate of foot and vascular reinterventions
These no-option CLTI pts should be considered for alternative
therapies such as:
- primary major amputation
- palliative care
- foot vein arterialization
In the last 50 yy our attention was focalized on pure
atherosclerotic BAD-PAD, for which we developed wonderful weapons:
bypass, PTA, drugs. Now we are facing a worldwide epidemic of
old/DM/CKD CLTI pts that are not pure-BAD-PAD
-
Vincenzo Foppa, 1462“The miracle of the salvaged foot” Cappella
Portinari, S. Eustorgio Church Milan, Italy
Small artery disease (SAD) and medial artery calcification (MAC)
are changing the fate of CLI patients