Embed Size (px)
Citation preview

١�٣�/٠١/١�
١
SMALL BOWEL OBSTRUCTION
Ahmad kachooyi MD
Assistant Professor
Qom Medical University
EPIDEMIOLOGY
١. Intraluminal (e.g., foreign bodies, gallstones,
or meconium)
٢. Intramural (e.g., tumors, Crohn's disease–
associated inflammatory strictures)
٣. Extrinsic (e.g., adhesions, hernias, or
carcinomatosis)

١�٣�/٠١/١�
٢
Intra-abdominal adhesions related to prior
abdominal surgery account for up to ٧% of the
cases of small bowel obstruction.
Less prevalent etiologies for small bowel
obstruction include hernias, malignant bowel
obstruction, and Crohn's disease

١�٣�/٠١/١�
٣
PATHOPHYSIOLOGY
� With onset of obstruction, gas and fluid
accumulate within the intestinal lumen
proximal to the site of obstruction
� colicky pain and the diarrhea that some
experience even in the presence of complete
bowel obstruction.
� strangulated bowel obstruction; If the
intramural pressure becomes high enough,
intestinal microvascular perfusion is impaired,
leading to intestinal ischemia, and, ultimately,
necrosis.
� partial small bowel obstruction; only a portion
of the intestinal lumen is occluded, allowing
passage of some gas and fluid.

١�٣�/٠١/١�
�
� complete small bowel obstruction;
development of strangulation is more likely.
� closed loop obstruction; a segment of intestine
is obstructed both proximally and distally (e.g.,
with volvulus). A rapid rise in luminal pressure,
and a rapid progression to strangulation
CLINICAL PRESENTATION
� colicky abdominal pain, nausea, vomiting, and obstipation.
� Continued passage of flatus and/or stool beyond �to ١٢ hours after onset of symptoms is characteristic of partial rather than complete obstruction.
� abdominal distention
� Bowel sounds may be hyperactive initially, but in late stages of bowel obstruction, minimal bowel sounds may be heard

١�٣�/٠١/١�
LABORATORY FINDINGS
� hemoconcentration and electrolyte
abnormalities
� Mild leukocytosis

١�٣�/٠١/١�
�
FEATURES OF STRANGULATED OBSTRUCTION
� abdominal pain often disproportionate to the
degree of abdominal findings
� tachycardia, localized abdominal tenderness,
fever, marked leukocytosis
� Acidosis
� need for early surgical intervention
DIAGNOSIS
� focused on the following goals:
� (a) distinguish mechanical obstruction from
ileus
� (b) determine the etiology of the obstruction
� (c) discriminate partial from complete
obstruction
� (d) discriminate simple from strangulating
obstruction

١�٣�/٠١/١�
٧
HISTORY
� prior abdominal operations (suggesting the
presence of adhesions)
� presence of abdominal disorders (e.g., intra-
abdominal cancer or inflammatory bowel
disease)
EXAMINATION
� search for hernias (particularly in the inguinal
and femoral regions)
� The stool should be checked for gross or occult
blood, the presence of which is suggestive of
intestinal strangulation.

١�٣�/٠١/١�
٨
RADIOGRAPHIC EXAMINATION
� The abdominal series consists of ;
١. a radiograph of the abdomen with the patient
in a supine position,
٢. a radiograph of the abdomen with the patient
in an upright position,
٣. a radiograph of the chest with the patient in
an upright position.

١�٣�/٠١/١�
٩
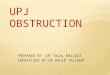
RADIOGRAPHIC EXAMINATION
� The finding most specific for small bowel
obstruction is the triad :
١. dilated small bowel loops (>٣ cm in diameter)
٢. air-fluid levels seen on upright films
٣. a paucity of air in the colon

١�٣�/٠١/١�
١٠

١�٣�/٠١/١�
١١
� False-negative findings on radiographs :
١. when the site of obstruction is located in the
proximal small bowel
٢. when the bowel lumen is filled with fluid but
no gas , preventing visualization of air-fluid
levels or bowel distention; closed-loop
obstruction
COMPUTED TOMOGRAPHIC (CT) SCANNING
� The findings of small bowel obstruction
include :
١. a discrete transition zone with dilation of
bowel proximally , decompression of bowel
distally
٢. intraluminal contrast that does not pass
beyond the transition zone
٣. a colon containing little gas or fluid

١�٣�/٠١/١�
١٢
COMPUTED TOMOGRAPHIC
� provide evidence for the presence of closed-
loop obstruction and strangulation
� Closed-loop obstruction is suggested by the
presence of a U-shaped or C-shaped dilated
bowel loop associated with a radial distribution
of mesenteric vessels converging toward a
torsion point.

١�٣�/٠١/١�
١٣
COMPUTED TOMOGRAPHIC
� Strangulation is suggested by thickening of the
bowel wall, pneumatosis intestinalis (air in the
bowel wall), portal venous gas, mesenteric
haziness, and poor uptake of IV contrast into
the wall of the affected bowel.

١�٣�/٠١/١�
١�
CT SCAN
� performed after administration of oral water
soluble contrast, or diluted barium
� The water soluble contrast has been shown to
have prognostic and therapeutic values
� appearance of the contrast in the colon within
٢� hours is predictive of nonsurgical resolution
of bowel obstruction.
LIMITATION OF CT SCANNING
� low sensitivity (<٠%) in the detection of low-grade or partial small bowel obstruction
� A subtle transition zone may be difficult to identify in the axial images obtained during CT scanning
� In such cases, contrast examinations of the small bowel, either small bowel series (small bowel follow-through) or enteroclysis, can be helpful.

١�٣�/٠١/١�
١
THERAPY
� fluid resuscitation is integral to treatment
� Isotonic fluid should be given intravenously
� indwelling bladder catheter placed to monitor
urine output.
� Central-venous or pulmonary-artery catheter
monitoring may be necessary to assist with
fluid management, particularly in patients with
underlying cardiac disease.
THERAPY
� Broad-spectrum antibiotics are given by some
because of concerns that bacterial
translocation may occur in the setting of small
bowel obstruction;
� NG tube
� The standard therapy for complete small bowel
obstruction generally has been expeditious
surgery

١�٣�/٠١/١�
١�
COMPLETE SMALL BOWEL OBSTRUCTION
� some have advocated nonoperative
approaches in management of these patients,
� closed loop obstruction is ruled out
� no evidence of intestinal ischemia.
� Such patients need to be observed closely and
undergo serial exams
� Clinical signs and currently available laboratory
tests and imaging studies do not reliably permit
the distinction between patients with simple
obstruction and those with strangulated
obstruction before the onset of irreversible
ischemia.
� the goal is to operate before the onset of
irreversible ischemia.

١�٣�/٠١/١�
١٧
� Conservative therapy, in the form of NG
decompression and fluid resuscitation is the
initial recommendation for:
١. Partial small bowel obstruction
٢. Obstruction occurring in the early
postoperative period
٣. Intestinal obstruction due to Crohn's disease
�. Carcinomatosis

١�٣�/٠١/١�
١٨
PARTIAL OBSTRUCTION
� progression to strangulation is unlikely to occur
� most patients with partial small obstruction
whose symptoms do not improve within �٨
hours after initiation of nonoperative therapy
should undergo surgery.
EARLY POSTOPERATIVE PERIOD OBSTRUCTION
� ٧�٠% patients undergoing laparotomy
� Patients undergoing pelvic surgery, especially colorectal procedures, have the greatest risk
� The presence of obstruction should be considered if symptoms of intestinal obstruction occur after the initial return of bowel function or if bowel function fails to return within the expected ٣ to days after abdominal surgery.

١�٣�/٠١/١�
١٩
EARLY POSTOPERATIVE PERIOD
� usually partial and only rarely is associated with
strangulation.
� a period of extended nonoperative therapy (٢ to ٣
weeks) consisting of bowel rest, hydration, and
total parenteral nutrition (TPN) administration is
usually warranted.
� if complete obstruction is demonstrated or if signs
suggestive of peritonitis are detected, expeditious
reoperation should be undertaken without delay.
CARCINOMATOSIS
� limited prognosis
� Management must be tailored to an individual
patient's prognosis and desires
� relief of the obstruction may be best achieved
by a bypass procedure
� avoiding a potentially difficult bowel resection

١�٣�/٠١/١�
٢٠
OPERATIVE PROCEDURE
� adhesions are lysed
� tumors are resected
� hernias are reduced and repaired
� affected intestine should be examined, and
nonviable bowel resected
CRITERIA SUGGESTING VIABILITY
� normal color
� Peristalsis
� marginal arterial pulsations
. In borderline cases:
١. Doppler probe
٢. administered fluorescein dye in the bowel wall
under ultraviolet illumination

١�٣�/٠١/١�
٢١
"SECOND-LOOK" OPERATION
� if the viability of a large proportion of the
intestine is in question, a concerted effort to
preserve intestinal tissue should be made
� the bowel of uncertain viability should be left
intact and the patient re-explored in ٢� to �٨
hours
OUTCOMES
� The majority of patients who are treated
conservatively for adhesive small bowel
obstruction do not require future readmissions;
� less than ٢٠% of such patients will have a
readmission over the subsequent years with
another episode of bowel obstruction.٢٣

١�٣�/٠١/١�
٢٢
PREVENTION
� adhesion prevention:
١. Good surgical technique
٢. careful handling of tissue
٣. minimal use and exposure of peritoneum to foreign bodies
In patients undergoing colorectal or pelvic surgery, hospital readmission rates of greater than ٣٠% over the subsequent ١٠ years have been reported for adhesive small bowel obstruction.
PREVENTION
� Use of laparoscopic surgery, when possible,
has been strongly promoted
� adhesion prevention :hyaluronan-based agents,
such as Seprafilm