Embed Size (px)
Citation preview

lable at ScienceDirect
Social Science & Medicine xxx (2014) 1e12
Contents lists avai
Social Science & Medicine
journal homepage: www.elsevier .com/locate/socscimed
The potential of social enterprise to enhance health and well-being:A model and systematic review
Michael J. Roy a, b, *, Cam Donaldson a, Rachel Baker a, Susan Kerr c
a Yunus Centre for Social Business and Health, Glasgow Caledonian University, Glasgow, UKb Glasgow School for Business and Society, Glasgow Caledonian University, Glasgow, UKc Institute for Applied Health Research, Glasgow Caledonian University, Glasgow, UK
a r t i c l e i n f o
Article history:Available online xxx
Keywords:Social enterpriseHealthcareSystematic reviewPublic healthWell-beingSocial determinants of healthHealth inequalities
* Corresponding author. Glasgow School for BusCaledonian University, Buchanan House, Cowcaddens
E-mail address: [email protected] (M.J. Roy).
http://dx.doi.org/10.1016/j.socscimed.2014.07.0310277-9536/© 2014 Published by Elsevier Ltd.
Please cite this article in press as: Roy, M.J., ereview, Social Science & Medicine (2014), ht
a b s t r a c t
In recent years civil society organisations, associations, institutions and groups have become increasinglyinvolved at various levels in the governance of healthcare systems around the world. In the UK,particularly in the context of recent reform of the National Health Service in England, social enterprise e
that part of the third sector engaged in trading e has come to the fore as a potential model of state-sponsored healthcare delivery. However, to date, there has been no review of evidence on the out-comes of social enterprise involvement in healthcare, nor in the ability of social enterprise to addresshealth inequalities more widely through action on the social determinants of health. Following thedevelopment of an initial conceptual model, this systematic review identifies and synthesises evidencefrom published empirical research on the impact of social enterprise activity on health outcomes andtheir social determinants. Ten health and social science databases were searched with no date delimitersset. Inclusion and exclusion criteria were applied prior to data extraction and quality appraisal. Het-erogeneity in the outcomes assessed precluded meta-analysis/meta-synthesis and so the results aretherefore presented in narrative form. Five studies met the inclusion criteria. The included studiesprovide limited evidence that social enterprise activity can impact positively on mental health, self-reliance/esteem and health behaviours, reduce stigmatization and build social capital, all of which cancontribute to overall health and well-being. No empirical research was identified that examined socialenterprise as an alternative mode of healthcare delivery. Due to the limited evidence available, wediscuss the relationship between the evidence found and other literature not included in the review.There is a clear need for research to better understand and evidence causal mechanisms and to explorethe impact of social enterprise activity, and wider civil society actors, upon a range of intermediate andlong-term public health outcomes.
© 2014 Published by Elsevier Ltd.
1. Introduction
The persistent and well-documented problem of health in-equalities, preventable and unfair differences in health status be-tween social groups, populations and individuals (Whitehead,1992; Whitehead et al., 2001), has challenged public health re-searchers since the relationship between income and health wasfirst established (Department of Health and Social Security, 1980;Townsend and Davidson, 1982). In the context of austerity mea-sures leading to public-sector funding cuts and faced withcontinuing, even growing, inequalities, more innovative,
iness and Society, GlasgowRoad, Glasgow G4 0BA, UK.
t al., The potential of social etp://dx.doi.org/10.1016/j.socs
community-based solutions have gained prominence (Baum, 2008;O'Mara-Eves et al., 2013). With this in mind, social enterprises e
businesses with social objectives whose surplus revenue is rein-vested for these purposes (Borzaga and Defourny, 2001; Dees,1998;Defourny et al., 2014; Kerlin, 2009; Nyssens, 2006)e could prove tobe a potentially innovative and sustainable response. Howeverthere is a significant gap in knowledge of how, and to what extent,social enterprise-led activity impacts upon health and well-being.
Furthermore, despite significant international policy attentionin recent times, most obviously from the European Commission (asrepresented by, for instance, the recent Social Business Initiative)but also by the Obama Administration (the establishment of theOffice of Social Innovation and Civic Participation and their SocialInnovation Fund), there have been very few systematic reviewsundertaken in the social enterprise/social entrepreneurship/social
nterprise to enhance health and well-being: A model and systematiccimed.2014.07.031

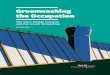
Fig. 1. Conceptual model of social enterprise ‘intervention’.
M.J. Roy et al. / Social Science & Medicine xxx (2014) 1e122
economy field in general. This is a notable absence, given thatsystematic reviews represent a cornerstone of the evidence-basedpractice and policy movement (Dixon-Woods et al., 2006).
Social enterprise as an alternative mode of delivery of state-sponsored healthcare has also had a significant amount of atten-tion in recent years (Addicott, 2011; Cook, 2006; Dawes, 2009;Drennan et al., 2007; Harris, 2007; Roy et al., 2013), particularlyin the UK, as private and third sector providers have been encour-aged to enter into the healthcare quasi-market on the underlyingassumption that they are capable of being more innovative andresponsive than their public sector counterparts (Allen, 2009;Millar, 2012).
There have also been numerous examples of state-sponsoredhealthcare systems working in partnership with community-based organisations in an attempt to better impact upon individ-ual risk factors including smoking, alcohol, diet and exercise.However, in the last couple of decades there has been a sustainedcall to re-orientate public health more closely towards “enablingthe growth of what nourishes human life and spirit, and supportinglife's own capacity for healing and health creation” (Hanlon et al.,2011, p. 35) and the so-called ‘assets-based approach’ is oneexample of this type of thinking: building upon the potentialstrengths of individuals and communities (Morgan et al., 2010)rather than focusing on deficiencies (Foot, 2012; Foot and Hopkins,2010; Kretzman and McKnight, 1993), with communities andoutside agencies often working in partnership to ‘co-produce’ so-lutions (Brandsen and Pestoff, 2006).
If it is considered that social enterprise has the potential to be aviable and sustainable way of organising such activity (Donaldsonet al., 2011; Roy et al., 2013, 2014) then a greater understandingof the health-enhancing mechanisms and causal pathways applied(or even assumed) in the work of social enterprises is undoubtedlyrequired. To explain further, our hypothesis is that practically allsocial enterprises could be said, in one way or another, to impact
Please cite this article in press as: Roy, M.J., et al., The potential of social ereview, Social Science & Medicine (2014), http://dx.doi.org/10.1016/j.socs
upon such factors as the unequal distribution of power, income,goods, and services, all of which are established as important socialdeterminants of health (Marmot et al., 2008; Wilkinson andMarmot, 2003). This is described in Fig. 1, in which we posit thata chain of causality exists from the trading activity of the socialenterprise through to health and well-being of individuals andcommunities.
Of course, in reality, the sequence is unlikely to be eithersequential or linear. The ability of the social enterprise to meet itssocial missionwill likely be dependent upon a range of internal andextraneous factors. The social enterprise ‘intervenes’ either directly(i.e. the ‘intervention’ is the trading activity) or the trading activitygenerates profits which can then be invested in the types of ‘assets’that we show in Part C of Fig. 1. These examples, which are in noway intended to be exhaustive, are adapted from Cooke et al. (2011)and can be at the levels of individuals or communities, or both. Assuch, it is considered that the impact of such activity can be viewedthrough the lens of existing theories, such as social capital/connectedness (Bourdieu, 1986; Coleman, 1988; Putnam, 2000) orSense of Coherence (Antonovsky, 1987, 1979) as shown in Part D ofthe Figure, or by employing other theoretical frameworks, such asCapabilities (Nussbaum, 2011; Sen, 1985) which all have a body ofevidence linking them to enhancements to individual and com-munity health and well-being (see for example, Lomas (1998) andUphoff et al. (2013) on social capital and Kivim€aki et al. (2000) onSense of Coherence).
2. Research aims
This paper offers two contributions to the debate on the socialenterprise/health interface. First, we offer a systematic review ofempirical evidence on this topic which is, as far as we are aware, thefirst such review undertaken in this area. Our second contributionrelates to evidencing the potential of any social enterprise to be
nterprise to enhance health and well-being: A model and systematiccimed.2014.07.031

M.J. Roy et al. / Social Science & Medicine xxx (2014) 1e12 3
thought of as a predominantly ‘upstream’ (McKinlay, 1974, 1979;Williams et al., 2008) public health intervention, rather than as amechanism for delivery of healthcare specifically. With social en-terprise existing in many shapes and forms, varying impacts onhealth and well-being would be expected, and a major aim of ourresearch agenda is to develop a theoretical framework, continuallyrefining the conceptual model shown in Fig. 1 through buildingevidence from empirical studies, for which this review is merelythe starting point. Through this work it is hoped that we can sup-port an advance in public health thinking and practice, particularlyin relation to the role of social enterprise, the wider third sector,and other (perhaps non-obvious) actors in the future of publichealth.
3. Methods
We conducted searches of public health, social science andmedical peer-reviewed journals in November and December 2012using 10 different databases: ASSIA, CENTRAL, DARE, HMIC, IBSS,MEDLINE, PsycInfo, Sociological Abstracts, SSRN and Web ofKnowledge. Each search used a combination of words related tosocial enterprise and predecessor concepts (social enterprise, socialbusiness, social entrepreneur, social firm, community enterprise,community business and affirmative business) and to healthrelated quality of life. This included both psycho-social factors (suchas sense of coherence, social capital, self-esteem, capabilities, hopefor the future, self-reported well-being, happiness) and socio-economic factors (such as income, occupation, education, and lit-eracy). Searches were not restricted by publication date. Key au-thors, identified during the course of the database searches andthrough our own personal contacts, were also approached andasked to send on articles for consideration, and further justificationfor this approach is provided in the Discussion section below. We
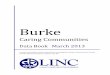
Fig. 2. Results of the search an
Please cite this article in press as: Roy, M.J., et al., The potential of social ereview, Social Science & Medicine (2014), http://dx.doi.org/10.1016/j.socs
identified 490 papers: 483 from database searches and seven sentus by key authors. Sixty two were found to be duplicates andremoved. Titles and abstracts were initially screened for relevanceand 365 were excluded at that stage. The full texts of the remaining63 studies were then reviewed independently by two authors ac-cording to the following criteria: (1) published in English; (2)empirical research on social enterprise-led activity on health andwell-being. Case studies, clinical reports, policy documents anddiscussion/opinion papers were excluded. Where disagreementsarose, the reviewers met to discuss and resolve (and a third partywould have been brought in if there was still disagreement).Following these steps, seven articles met the inclusion criteria.Three were combined (i.e. Ferguson and Islam, 2008; Ferguson,2012, 2013) as they reported on findings from the same studygroup. The total number of separate studies discussed, as shown atFig. 2, is therefore five.
A review-specific data extraction tool was developed, tested andrefined to capture a range of data to assist in the synthesis. For eachstudy the following information was collected: author(s) and yearof publication; type of ‘intervention’ and its theoretical un-derpinnings; participants; study design; sampling procedure; datacollection; sample size; the methodological perspective/analyticalapproach employed in the study; and a brief summary of the keyfindings.
Each paper was also assessed by two reviewers separately on arange of quality criteria based upon Popay (2006): whether theaims and objectives were clearly stated and addressed; the dis-cussion of the context and need for the study (i.e. the justificationfor the study); whether there was a clear description and appro-priateness of the sampling strategy and method of recruitmentpresented; the description of the intervention (including theoret-ical and underpinnings and any comparator/control interventions);whether there was a clear description and appropriateness of
d study selection process.
nterprise to enhance health and well-being: A model and systematiccimed.2014.07.031

Table 1Summary of included studies.
Paper (year)and Country
Type of SE‘intervention’
Theoretical underpinningof ‘intervention’
Aimed at Study design/Datacollection
Samplingprocedure
Sample size Methodologicalperspective/analyticalapproach
Brief summary ofkey findings
Qualityassessment
Ferguson andIslam (2008)
Ferguson(2012, 2013)
US
SocialFirm/WISE
Draws on asset-basedyouth developmentand thriving. Specifically,youths' internaldevelopmental assets arecategorized in four areas:commitment to learning,social competencies,positive values andpositive identity.Collectively, the socialenterprise intervention(SEI) components aim tostrengthen the youths'internal assets to enhancepositive outcomes andprotect them against highrisk behaviour.
Street-livingyoung adults
Mixed methodsdesignincorporating:(1) Qualitative
study basedon focus-groupinterviews
(2) Quantitative(survey)componentdeliveredvia structuredinterview
(1) Purposivesampling ofparticipantswho‘remainedwith theprogramme’
(2) Two screeningcriteria guidedrecruitment:(1) the youthshad to haveattended theAgency two ormore times aweek for themonth prior tothe study; and(2) the youthshad to committo attending theprogramme forboth the 4 monthvocational andbusiness trainingprogrammes.A separatecontrol group wasformed in theagency and anattempt wasmade to matchthe groups on age,gender andethnicity.
(1) 5(2) 16 (SEI)
and 16(ControlGroup)
(1) ConstructivistGrounded Theory,Constantcomparisonmethods
Investigator, theoryand data triangulationmethods(2) Satisfaction with
life was assessedusing theSatisfaction withLife Scale.
Family supportmeasured thefrequency withwhich the youthreported that theysee, write, or talk totheir immediatefamily.Peer support was acomposite variableof the sum of fouritems on the FriendsSubscale of the AdultSelf Report.Depression wasassessed using theReynolds DepressionScreening Inventory.
Mental Health:family respect;self-esteem andmotivation; goalorientationEmploymentoutcomes:Acquisition ofknowledge andskills, increasedexposure to theworld of work.Service RelatedOutcomes:relationship withstaff; serviceengagement;social networksBehaviouralOutcomes: respitefrom street life;avoidance ofdestructivebehaviourSocietaloutcomes: positiveaspects ofhomeless; imagewith authoritiesSatisfaction withlife: A 6.45-unitincrease in totallife satisfactionfrom baseline tothe end offollow-up,compared witha 2.25-unitdecrease in thecontrol group(P ¼ .02)Family support:0.50-unit increasein family supportover the studyperiod, as comparedto a 1.20-unitdecrease observedin the control group(P ¼ .03)Peer support:3.00-unit increasein peer support
High
M.J.Roy
etal./
SocialScience
&Medicine
xxx(2014)
1e12
4Pleasecite
thisarticle
inpress
as:Roy,M.J.,et
al.,Thepotentialofsocialenterprise
toenhance
healthand
well-being:A
modeland
systematic
review,SocialScience
&Medicine
(2014),http://dx.doi.org/10.1016/j.socscimed.2014.07.031

over the studyperiod, whereasthe control groupexperienced a0.13-unit increase(P ¼ 0.06)Depression:5.45-unit decreasein depressivesymptoms,compared with nochange observedin the controlgroup (P ¼ 0.10)
Ho andChan (2010)
Hong Kong
WorkIntegrationSocialEnterprise(WISE)
WISEs help people movefrom welfare dependencyto self-reliance by givingthem the capacity forindependent wage-earning.As well as those related tojob outcomes (learningnew job skills, enhancingemployability and movingout of poverty) reductionin the public stigmatizationof marginalized groups andbuilding social capital arealso target “social goals”.
A range ofdisadvantagedgroups: peoplewith disabilities,new immigrants,the elderly,unemployedyouths,ex-offendersand low-incomefamilies
Case studyapproach:qualitativeresearchmethodcharacterizedby selectivesampling andin-depthexaminationusingsemi-structuredinterviews
Purposivesampling of WISEsin Hong Kong,representinga wide rangeof businessactivities andtargetpopulations.
51 WISEs ConstantcomparisonInvestigatortriangulation
Because thetarget groups andthe modes ofintervention areso heterogeneous,there is no unifiedset of outcomespresented. Thereare outcomesdrawn fromspecific examplese.g. 40% ofparticipants nolonger reliant uponsocial security,about half becomingemployable in theopen market, whichincreases theiropportunity toincrease their and“resume theirdignity”.WISEs address theissue of socialexclusion in thelabour marketPeople gain betteremployability andthus the opportunityto move fromwelfare toself-reliance.WISEs facilitate thebuilding of socialcapital among theiremployees.WISEs cultivate aself-help spirit and asense of belongingamong marginalizedgroups in poorneighbourhoods, andbecome a meansthrough which they
Moderate
(continued on next page)
M.J.Roy
etal./
SocialScience
&Medicine
xxx(2014)
1e12
5
Pleasecite
thisarticle
inpress
as:Roy,M.J.,et
al.,Thepotentialofsocialenterprise
toenhance
healthand
well-being:A
modeland
systematic
review,SocialScience
&Medicine
(2014),http://dx.doi.org/10.1016/j.socscimed.2014.07.031

Table 1 (continued )
Paper (year)and Country
Type of SE‘intervention’
Theoretical underpinningof ‘intervention’
Aimed at Study design/Datacollection
Samplingprocedure
Sample size Methodologicalperspective/analyticalapproach
Brief summary ofkey findings
Qualityassessment
expand their socialand supportivenetworks andcooperate witheach other formutual benefiton the basis oftrust.For persons withdisabilities, WISEsalso enhance jobsatisfaction,facilitate therealization of theirpotential andexpedite theprogress ofrecovery.For sociallystigmatized groupslike people withmental healthproblems andex-offenders,WISEs improvemutualunderstandingand interactionwith thecommunity,and hence facilitatesocial recognitionand a supportivesocial environmentfor socialintegration.
Krupa et al.(2003)
Canada
‘Affirmativebusiness’akaWISE/socialfirm
Examines the outcomesassociated with anorganisation which usedthe resources of asheltered workshop in aprovincial psychiatrichospital to evolveaffirmative businesses/social firms forpeople receiving mentalhealth services.Unlike vocationalrehabilitation efforts thatfocus on helpingindividuals to “fit in”to the existingemployment market,affirmative businesses
Owners/operatorswith psychiatricdisabilities
A three stage approachwas taken which employed:(1) analysis of historicaland accounting recordsand interviews with formerparticipants in shelteredworkshops; (2) a survey ofpeople who decided not tobe involved in theprogramme;and (3) a series ofsemi-structured focus groupsof owner/operators andbusiness support staff
(1) not specified(2) all people who had
decided in the past notto be involved wereinvited to complete asurvey in an attempt toidentify a comparatorgroup
(3) Sampling procedurefor choosing owner/operators was notspecified
(1) Not specified(2) 73 surveys(3) 32 people
Straussian dataanalysis, datacoding and axialcoding to identifykey themes,associationsbetween themesand causalconditions.Investigator/datatriangulationmethods
Success of theapproach wasevaluated by boththe economicsustainability ofbusinesses andthe well-being ofthe ‘consumercommunity’.Measures ofwell-beingincluded(1) increasedemploymentopportunities;(2) increasedlevel of personalinvolvement
Moderate
M.J.Roy
etal./
SocialScience
&Medicine
xxx(2014)
1e12
6Pleasecite
thisarticle
inpress
as:Roy,M.J.,et
al.,Thepotentialofsocialenterprise
toenhance
healthand
well-being:A
modeland
systematic
review,SocialScience
&Medicine
(2014),http://dx.doi.org/10.1016/j.socscimed.2014.07.031

use a communityeconomic developmentapproach to neutralizelabour force conditionsof individualism,competition and profitthat perpetuateemploymentdisadvantage.
and ownership;(3) improvementin living conditions;and (4) meeting orexceeding standardsfor fair employment
Tedmanson andGuerin (2011)
Australia
Socialenterprisegenerally
Based upon“strengths-based”approaches tocommunitydevelopment, whichemphasizes the socialcapital assets ofcommunities, aim toreinforce local talents,and build localcapacity.
“Remote”indigenousAustraliancommunitycontexts
Interviews and participantobservation
Not specified Not specified Not specified Enhancements ininterdependenceand independence.Concomitant mentalhealth and socialwell-being dividendsaccrue over timeto communitiesengaged inself-determinedenterprise activities.Socialentrepreneurshipbuilds social capitalthat supports socialwell-being.Strengths-basedapproaches to socialentrepreneurshipcan assuagedisempoweringeffects of welfarethrough shifting thefocus onto productiveactivities generatedon people's ownterms.
Low
Williams et al.(2010)Australia
SocialFirm/WISE
Ongoing, secureemploymentprovides pathways toeconomic participation,social inclusion andrecovery.Social firms orenterprises aim tooffer sustainableemployment insupportive workplacesfor people who aredisadvantaged in thelabour market.
Employeeswith psychiatricdisabilities
Interviews using theWork EnvironmentImpact Scale (Version 2.0).Interviews wereaudiotaped, transcribedand analysed inductivelyusing thematic andnarrative analysis.
Adults experiencingpsychiatricdisability;comfortableconversing inEnglish; andemployed for 6months or longerin the social firm.
7 people The WEISv2.0 isdesignedspecifically toexplore a worker'sperception of thework environmentthrough questionsabout physicaland socialworkplace factorsthat may have apositive or negativeimpact on theworker.
The participantsperceived rewards,interactions withothers, work schedulesand task demandsat the social firmpositively. Theparticipants sustainedtheir employmentbecause theyperceived that theirjobs were differentto other jobs: thesocial firm offeredsecure employment;supportive andinclusive workrelationships; andregular schedulesand tasks thatparticipants believedthey could completewell, leading to high
Moderate
(continued on next page)
M.J.Roy
etal./
SocialScience
&Medicine
xxx(2014)
1e12
7
Pleasecite
thisarticle
inpress
as:Roy,M.J.,et
al.,Thepotentialofsocialenterprise
toenhance
healthand
well-being:A
modeland
systematic
review,SocialScience
&Medicine
(2014),http://dx.doi.org/10.1016/j.socscimed.2014.07.031

Table
1(con
tinu
ed)
Paper
(yea
r)an
dCou
ntry
Typeof
SE‘in
terven
tion
’
Theo
reticalunderpinning
of‘in
terven
tion
’
Aim
edat
Studydesign/D
ata
colle
ction
Samplin
gprocedure
Sample
size
Method
olog
ical
persp
ective
/an
alytical
approach
Brief
summaryof
keyfindings
Quality
assessmen
t
leve
lsof
job
satisfaction
.Fu
rther,theworke
rsperceived
that
workingat
thesocial
firm
benefi
tedtheir
emotional
andphysical
well-be
ing,
specifically
contributingpositively
totheirhea
lth,
econ
omic
circumstan
cesan
doc
cupational
life-co
urse.
M.J. Roy et al. / Social Science & Medicine xxx (2014) 1e128
Please cite this article in press as: Roy, M.J., et al., The potential ofreview, Social Science & Medicine (2014), http://dx.doi.org/10.101
social e6/j.socs
methods used to collect and analyse data; the attempts made toestablish the reliability and validity of quantitative data and thecredibility of qualitative data (i.e. the rigour of the process) and;whether there was inclusion of sufficient original data to mediatebetween evidence and interpretation. No papers were discountedon grounds of quality, but, for the sake of validity or credibility(Lincoln and Guba, 1985) it was deemed important to provide somecommentary of the studies in terms of their quality. Each of theseven quality elements was rated at between 0 and 2. A qualityrating of ‘High’ meant a score between 10 and 14, ‘Moderate’ be-tween 5 and 9, and ‘Low’, a score of between 0 and 4. These ratingsare not intended to be definitive by any means: they are simplypresented to facilitate the interpretation of the findings. Due to thevariety of measures and study designs employed across studies itwas not possible to perform a meta-analysis or meta-ethnographyand so narrative synthesis (Popay et al., 2006) has been employed.An example of a database search with the full range of search termsemployed and the breakdown of the quality assessment of thepapers are both available as (Online) Supplementary files.
4. Results
Findings from the five separate studies that met the inclusioncriteria are summarised in Table 1. The earliest study was publishedin 2003 and the remainder between 2008 and 2013. Four of the fivestudies focused upon a specific type of social enterprise knownvariously as a social firm, an affirmative business, or a Work Inte-gration Social Enterprise (WISE). All of these terms relate to aspecific type of social enterprise that has workforce developmentand/or job creation for disadvantaged populations as its core pur-pose (Krupa et al., 2003; Lysaght et al., 2012; Spear and Bidet, 2005;Vidal, 2005;Warner andMandiberg, 2006) andmay also combine amission to address social exclusion (Teasdale, 2010, 2012) withproviding a product or service needed by society (Ferguson, 2012).No empirical research was identified which examines social en-terprise as an alternative mode of healthcare delivery.
As can be seen from Table 1, only one of the studies was rated asbeing of ‘high’ quality, three were rated as ‘moderate’ and one as‘low’ quality. One of the studies was undertaken in the US, two inAustralia, one in Canada and one in Hong Kong. All five of thestudies employed qualitative methods with two (Ferguson, 2012,2013; Krupa et al., 2003) employing mixed methods. As is oftenthe case with qualitative studies, sample sizes were low, rangingfrom five people (Ferguson and Islam, 2008) to seven people(Williams et al., 2010) to 32 people (Krupa et al., 2003) to 51 or-ganisations (Ho and Chan, 2010) while one study did not specifytheir sample size (Tedmanson and Guerin, 2011). In the two studiesthat also employed quantitative components, one used the re-sponses of 16 individuals compared with a control group also of 16people (Ferguson, 2012, 2013) matched as far as possible on age,race and gender, while the other (Krupa et al., 2003) utilised surveyresponses from 73 individuals.
To aid understanding of our synthesis of the health and well-being outcomes presented in the studies, these are presented inthree categories: physical health, mental health and social de-terminants. In reality, of course, these categories are interrelated:they impact upon and reinforce each other.
4.1. Physical health
One of the studies (Ferguson and Islam, 2008) explicitly pro-vided qualitative evidence that working in the social enterprise wasa viable mechanism to encourage participants not to engage in thetypes of destructive or illicit behaviours known to be detrimental tophysical health. Another study (Williams et al., 2010) presented
nterprise to enhance health and well-being: A model and systematiccimed.2014.07.031

M.J. Roy et al. / Social Science & Medicine xxx (2014) 1e12 9
limited qualitative evidence of a perception that working at thesocial enterprise benefited participants' physical well-being.
4.2. Mental health
All five of the studies (Table 1) presented evidence that theparticipants experienced several positive mental health changes asa result of their involvement with the social enterprise. It was foundthat, if participants had continued relationships with their family,then participation in such a goal-focused vocational training pro-gramme would lead to increased feelings of familial respect andsense of self, particularly in relation to their accomplishments(Ferguson and Islam, 2008). Furthermore, the studies presented arange of evidence which stated that social enterprises can enhancenon-vocational outcomes such as self-confidence or self-esteem(Ferguson and Islam, 2008; Ho and Chan, 2010; Williams et al.,2010) and motivation and commitment to goals/life direction(Ferguson and Islam, 2008; Krupa et al., 2003). It was reported inthree of the studies (Ferguson and Islam, 2008; Krupa et al., 2003;Williams et al., 2010) that the social enterprise work environmenthelped the participants to feel calm and relaxed, so that, forinstance, they were better able to express their ideas (Ferguson andIslam, 2008).
The only quantitative analysis undertaken (Ferguson, 2012,2013) on mental health outcomes used four indicators: satisfac-tion with life, family support, peer support and depression, all ofwhich were positively impacted in comparison to a control group.The studies suggested too that the social enterprise enabled peoplewith mental health problems to fulfil their desire “to participate inmeaningful occupation” (Williams et al., 2010, p. 536) and limiteddepressive symptoms through “providing the financial incentive toparticipate in activities that hold meaning and give direction andstructure” (Krupa et al., 2003, p. 363) and demonstrated that, foremployees with psychiatric disabilities, working in such an envi-ronment made them feel better, kept them healthy and preventedboredom (Krupa et al., 2003).
4.3. Social determinants
All five studies, as Table 1 indicates, referred to the social de-terminants of health in some way. Indeed, two of them (Fergusonand Islam, 2008; Tedmanson and Guerin, 2011) explicitly drewupon theories regarding ‘assets’ (specifically asset-based youthdevelopment and thriving (Benson et al.,1999; Benson, 2003) in theformer) or ‘strengths’ to explain the role of social enterprise as amechanism for sustainably helping to generate or preserve thefactors that influence upon individual and community health andwell-being. All five studies, for instance, emphasised in variousways the enhancement of knowledge and skills as being of keyimportance to enhancing employability, and, indeed, to helpingpeople to maintain and find a job in future. The social enterpriseserved as a “springboard” (Ho and Chan, 2010, p. 38) or “stepping-stone” (Krupa et al., 2003, p. 362) to employment throughproviding on-the-job training which increased the chance ofemployment down the line, or which assisted people to becomeself-employed, with the aim to facilitate the integration of disad-vantaged groups into both the job market and the community and“resume their dignity” (Ho and Chan, 2010, p. 40). Two of the fivestudies (Ferguson and Islam, 2008; Ho and Chan, 2010) reportedthat a key outcome was a reduction in the public stigmatization ofmarginalized groups, such as people living on the street, peoplewith mental health problems, or ex-offenders: it was found thatsocial enterprises “provide a window of opportunity for mutualunderstanding and interaction with the community, and hencefacilitate social recognition and a supportive social environment for
Please cite this article in press as: Roy, M.J., et al., The potential of social ereview, Social Science & Medicine (2014), http://dx.doi.org/10.1016/j.socs
social integration” (Ho and Chan, 2010, p. 41) and play a critical rolein reducing public stigmatization by demonstrating that membersof marginalized groups can be capable, productive workers andmembers of society. Three of the five studies (Ferguson, 2012; Hoand Chan, 2010; Tedmanson and Guerin, 2011) specificallymentioned that social enterprises were a mechanism for buildingsocial capital, providing an opportunity for disadvantaged andmarginalized groups to expand their social networks and developsocial trust, facilitating social trust and co-operation, strengtheningtheir existing peer support groups, and enhancing their futurecareer prospects.
5. Discussion
Our systematic review of the empirical evidence presentlyavailable on the interface between health and social enterprise hasrevealed that there is currently no available evidence fromwhich toassess social enterprise as an alternative mechanism for healthcaredelivery in comparisonwith any other model. That they are capableof being more innovative and responsive than their public sectorcounterparts, at least in the health arena, remains simply anassumption in the absence of any supporting or refuting evidence.The heterogeneity of the outcomes explored and the fact that muchof the data is qualitative limits what can be said about the effec-tiveness of social enterprise as a public health intervention.Nevertheless, it is important that a systematic approach was takenas it provides clear evidence of the current very limited evidencebase and the need for quantitative studies to explore effectivenessand qualitative studies to exploremechanisms of action. There are alimited number of common lessons that can be drawn from thestudies reviewed more-formally here, but also from the wider lit-eratures on social enterprise and public health. We set these outbriefly with a view to contributing to a future research agenda inthis area.
5.1. Common lessons from the review
The evidence suggests that Work Integration Social Enterprises/Social Firms may be a good model for supporting people disad-vantaged from the labour market and that there are a range ofadvantages, at a number of different levels, both to the participantsand to wider society. Social enterprises can impact in various waysupon health: they can be a good mechanism for enhancing skillsand employability, which leads to increased self-reliance andesteem, they can reduce stigmatization, particularly of marginal-ized groups, and they can work to build social capital and improvehealth behaviours, all of which can contribute to overall health andwell-being. While the heterogeneity of the study designs, thevarying quality of the studies, the low sample sizes used and thevery specific contexts in which the studies took place all makegeneralisable claims difficult, by bringing these factors together,they can help to inform future hypotheses and theoreticaldevelopment.
The second aim of our review was to build upon and refine ourinitial hypothesis around the potential of any social enterprise to bethought of as a predominantly ‘upstream’ intervention. The limitedevidence presented in this review shows that social enterprises canwork to maintain and build the types of ‘assets’ that we show inPart C of Fig. 1, although patently there is a need for many moreempirical studies involving more people in more settings, andcovering a wider range of research methods, including quantitativecomparative evaluations. Hopefully, such future empirical work canbe informed by the methodological strengths and limitations of thestudies that we identified in this review.
nterprise to enhance health and well-being: A model and systematiccimed.2014.07.031

M.J. Roy et al. / Social Science & Medicine xxx (2014) 1e1210
5.2. Supplementary literature from social enterprise
By employing an integrative approach (Whittemore and Knafl,2005) it has been possible to provide a narrative synthesis of awide range of study types, offering a comprehensive overview ofthe available published evidence. However, it is, of course, possiblethat not all of the relevant literature has been captured. Ourstrategy to broaden the reach of the electronic searches involvedcontacting the handful of researchers across the world with pub-lished work in the social enterprise/health interface and presentingour initial findings at conferences. This led us to a small body ofinteresting and relevant work that fell just outside the scope of thisreview, notably the work of Pestoff (2000) on the psycho-socialwork environment within social co-operatives in the Swedishcare sector and relatedwork, also undertaken in Sweden, by Stryjan(1995). It also led us tomore recent work by Bertotti et al. (2012) onsocial enterprises as instruments for building social capital indisadvantaged areas of London, work by Barraket (2013) on theimpact of WISEs upon immigrants and refugees in the Australianstate of Victoria, recent work by Farmer et al. (2012) on the role ofsocial enterprise as a means of addressing disadvantage in remoteand rural communities and work by Teasdale (2010) on social en-terprise as a means of addressing social exclusion in inner citycommunities. This small body of additional literature, although ithas not been subject to the same level of rigorous analysis as theother papers identified, broadly supports the plausibility of thefindings and conceptualisations presented herein.
Despite much being made of the importance of social enterpriseto aid development, and as a mechanism to alleviate poverty(Cooney andWilliams Shanks, 2010; Yunus andWeber, 2009) all ofthe studies identified in the review took place in so-called‘advanced’ economies, and none from developing countries. Evenwithin advanced economies, the absence of studies from Europewas a particular surprise, particularly given strong traditions ofsocial enterprise activity there, notably thework of Italian social co-operatives (Borzaga and Depedri, 2013; Borzaga and Galera, 2012;Mancino and Thomas, 2005) which emerged at the end of the1970s, mainly on the initiative of a small groups of volunteers andworkers who were dissatisfied by poor provision of social andcommunity care services.
One can also come at this issue from the point of view of thosewho see social enterprise as one response to the excesses of theunfettered market, which have exacerbated and accelerated healthinequalities (Mooney, 2012; Scambler, 2007). Here, social enterprisecould be seen as a means of ‘re-embedding’ the market (Polanyi,1944) so that it is seen as simply one of three ‘poles’ of the econ-omy (i.e. state,market and community). The social enterprise acts asa ‘hybrid’ (Defourny and Nyssens, 2006) form of organisation thatworks across and between these three ‘poles,’ not limited to themarket principle of exchange or the principle of redistribution, butwhich also takes account of the principle of reciprocity (Gardin,2006) which means that social enterprises are able to draw upon aplurality of resources and mobilize different kinds of market andnon-market resources to sustain their goals. The social purpose,therefore, “to contribute to the welfare of well-being in a given hu-man community” (Peredo and McLean, 2006, p. 59) is not a conse-quence, or a side-effect, of economic activity, but its motivation(Defourny and Nyssens, 2006).
Furthermore, social enterprises (at least in mainstream con-ceptualisations) are, at their heart, community-based organisations:their roots are to be found inplaces, communities of interest, orwhatMandiberg describes as ‘enclave communities’ (Mandiberg, 2010).The concept of ‘story’, the personal narratives of people's everydaylives, is integral to their success, as the first chapter of John Pearce'sseminal text Social Enterprise in Anytown so aptly demonstrates
Please cite this article in press as: Roy, M.J., et al., The potential of social ereview, Social Science & Medicine (2014), http://dx.doi.org/10.1016/j.socs
(Pearce, 2003, pp. 8e23). Attending to personal narratives can helporient occupational therapists, case managers in mental health ser-vices andvocational serviceproviders towardsprovidingsupportandadvocacy, to start to address barriers that limit their clients' careerdevelopment (Williams et al., 2012) such as addressing inflexiblebenefit systems or a lack of supported education and training op-portunities, all of which may have important health effects.
5.3. Supplementary literature from public health
As we said in our introduction, for some time now conceptual-izations of health and well-being have been shifting away from afocus on individual pathologies and risk factors towards a greaterawareness of the importance of social relationships, communityprocesses and social contexts in producing health and well-being.The so-called ‘Fifth Wave’ of thinking in public health (Hanlonet al., 2011) owes its origins to several decades of debate and at-tempts to reconfigure practice, and the recent policy attention on‘assets-based’ approaches is only the latest policy manifestation ofsuch thinking. It is clear, however, that new conceptualisations ofwhat a public health intervention could or should look like in this(still evolving) paradigm are required. Social enterprise could pre-sent a number of benefits, at multiple levels, to ‘operationalise’ suchFifth Wave thinking, particularly as a means of building socialcapital and assets such as self-esteem and self-reliance in a sus-tainable e at least in theory e fashion.
It could be envisaged that “many of the key players [of the FuturePublic Health] may not consider themselves to be involved formallyin public health at all: their influence on health will be a product oftheir primary intent” (Hanlon et al., 2012, p. 169) but while theremay not have been a great deal of empirical research undertakenfrom a ‘Fifth Wave’ standpoint, which is just starting to penetratethe consciousness of public health researchers, over the last coupleof decades we have seen a number of large-scale flagship pro-grammes, such as the WHO Healthy Cities Programme, and the UKGovernment's Sure Start Programme, which have attempted to actupstream. Healthy Cities, established formally in 1987, was one ofthe first major initiatives following the Ottawa Charter for HealthPromotion in 1986 and one of its core principleswas the broadeningof the scope of public health actors to include those that would notbe termed immediately obvious e.g. third sector organisations andlocal authority departments not chiefly responsible for health(Tsouros,1995). EvelynDe Leeuw,who has published extensively onthe Healthy Cities programme, recognised back in 1999 that socialentrepreneurs would be “vital for the future development of healthpromotion, as they offer away of tackling the social determinants ofhealth and disease through community-based action” (De Leeuw,1999, p. 261) before the terms ‘social enterprise’ or ‘social entre-preneurship’ were even being talked about to any meaningfulextent in an academic context. Sure Start, on the other hand, aimedto act upon the vital early years in a child's development throughimprovement of childcare, early education, health and family sup-port, and, it has been argued, explicitly as an upstream interventionon health inequalities (Gidley, 2007). Many social enterprises havebeen involved as providers of local Sure Start services, and thisprogramme acted as a catalyst for a large number of new socialenterprises being started in the UK (France, 2007). Both of theseinitiatives, and many more throughout the world, have contributedto our knowledge of what ‘focusing upstream’ entails, and the po-tential, in public health terms, of doing so.
5.4. The future research agenda
The evidence presented in this review suggests that the po-tential of social enterprise and other civil society actors to focus
nterprise to enhance health and well-being: A model and systematiccimed.2014.07.031

M.J. Roy et al. / Social Science & Medicine xxx (2014) 1e12 11
impact upon upstream social determinants of public health re-quires continued theoretical and conceptual development and e
crucially e further empirical work to help inform and test initia-tives that may arise from such thinking. In particular, this reviewhas identified that a clear gap in knowledge exists regarding thecausal mechanisms at work, through which social enterprises andother civil society actors seek to impact upon a range of interme-diate and long-term public health outcomes. In recognition of thisgap, a five-year programme of research to evidence the impact of‘social enterprise as a public health intervention’ has been fundedjointly by the UK's Medical Research and Economic and SocialResearch Councils, which commenced in January 2014 (GlasgowCaledonian University, 2013).
It is incumbent upon Governments, particularly in advancedeconomies, to seek a way out of the cycle of diminishing returnsfrom investment into public healthcare systems, to bridge the ‘in-genuity gap’ (Homer-Dixon, 2000) between the problems we faceand the availability of adequate solutions. Social enterprises, withtheir emphasis upon reinvesting profits into the community to-wards achieving a social mission,may well present such a potential,community-based, solution, but one which requires equally-sophisticated research evidence to inform its development andsupport in such a role. In turn, this may help convince Governmentsof the health and well-being merits, or otherwise, of subsidisingand regulating to help provide an enabling and supportive envi-ronment in which community-led social enterprises can prosper.
Acknowledgements
We thank the anonymous reviewers for their constructivefeedback and suggestions, all of which added considerable value.We also acknowledge the support and assistance of most of theprimary authors of the studies presented in this Review and thosewho have provided useful feedback at conferences. The support ofKristin Ferguson was especially welcome and valuable.
Appendix A. Supplementary data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.socscimed.2014.07.031.
References
Addicott, R., 2011. Social Enterprise in Health Care: Promoting Organisational Au-tonomy and Staff Engagement. The King's Fund, London. Retrieved from: http://www.kingsfund.org.uk/publications/social-enterprise-health-care.
Allen, P., 2009. Restructuring the NHS again: supply side reform in recent Englishhealth care policy. Financ. Acc. Manag. 25 (4), 373e389.
Antonovsky, A., 1979. Health, Stress and Coping. Jossey-Bass Publishers, SanFrancisco.
Antonovsky, A., 1987. Unraveling the Mystery of Health: How People Manage Stressand Stay Well. Jossey-Bass Publishers, San Francisco.
Barraket, J., 2013. Fostering wellbeing of immigrants and refugees? Evaluating theoutcomes of work integration social enterprise. In: Denny, S., Seddon, F. (Eds.),Social Enterprise: Accountability and Evaluation Around the World. Routledge,Abingdon, Oxon.
Baum, F., 2008. The New Public Health. Oxford University Press, Oxford.Benson, P., 2003. Developmental assets and asset-building community: conceptual
and empirical foundations. In: Lerner, R., Benson, P. (Eds.), Developmental As-sets and Asset-Building Communities, vol. 1. Kluwer Academic/Plenum Publ.,New York, pp. 19e43.
Benson, P.L., Scales, P.C., Leffert, N., Roehlkepartain, E.C., 1999. A Fragile Foundation:the State of Developmental Assets Among American Youth. Search Institute,Minneapolis, MN.
Bertotti, M., Harden, A., Renton, A., Sheridan, K., 2012. The contribution of a socialenterprise to the building of social capital in a disadvantaged urban area ofLondon. Community Dev. J. 47 (2), 168e183.
Borzaga, C., Defourny, J. (Eds.), 2001. The Emergence of Social Enterprise. Routledge,London.
Borzaga, C., Depedri, S., 2013. When social enterprises do it better: efficiency andefficacy of work integration in Italian social cooperatives. In: Denny, S.,
Please cite this article in press as: Roy, M.J., et al., The potential of social ereview, Social Science & Medicine (2014), http://dx.doi.org/10.1016/j.socs
Seddon, F. (Eds.), Social Enterprise: Accountability and Evaluation Around theWorld. Routledge, Abingdon, Oxon.
Borzaga, C., Galera, G., 2012. The concept and practice of social enterprise. Lessonsfrom the Italian experience. Int. Rev. Soc. Res. 2 (2), 95e112.
Bourdieu, P., 1986. The forms of capital. In: Richardson, J. (Ed.), Handbook of Theoryand Research for the Sociology of Education. Greenwood Press, Westport,Connecticut, pp. 241e258.
Brandsen, T., Pestoff, V., 2006. Co-production, the third sector and the delivery ofpublic services. Public Manag. Rev. 8 (4), 493e501.
Coleman, J.S., 1988. Social capital in the creation of human capital. Am. J. Sociol. 94(Suppl.: Organizations and Institutions: Sociological and Economic Approachesto the Analysis of Social Structure), S95eS120.
Cook, R.R., 2006. What does social enterprise mean for community nursing? Br. J.Commun. Nurs. 11 (11), 472e474.
Cooke, A., Friedli, L., Coggins, T., Edmonds, N., Michaelson, J., O'Hara, K., Snowden, L.,Stansfield, J., Steuer, N., Scott-Samuel, A., 2011. Mental Wellbeing ImpactAssessment: a Toolkit for Well-being. National MWIA Collaborative (England),London.
Cooney, K., Williams Shanks, T., 2010. New approaches to old problems: market ebased strategies for poverty alleviation. Soc. Serv. Rev. 84 (1), 29e55.
Dawes, D., 2009. How nurses can use social enterprise to improve services in healthcare. Nurs. Times 105 (1), 22e25.
De Leeuw, E., 1999. Healthy cities: urban social entrepreneurship for health. HealthPromot. Int. 14 (3), 261e270.
Dees, J.G., 1998. Enterprising nonprofits. Harv. Bus. Rev. 76 (1), 54e67.Defourny, J., Nyssens, M., 2006. Defining social enterprise. In: Nyssens, M. (Ed.),
Social Enterprise: At the Crossroads of Market, Public Policies and Civil Society.Routledge, Abingdon.
Defourny, J., Hulgård, L., Pestoff, V. (Eds.), 2014. Social Enterprise and the ThirdSector: Changing European Landscapes in a Comparative Perspective. Rout-ledge, Abingdon, Oxon.
Department of Health and Social Security, 1980. Inequalities in Health: Report of aResearch Working Group. DHSS, London. Retrieved from: http://www.sochealth.co.uk/public-health-and-wellbeing/poverty-and-inequality/the-black-report-1980/.
Dixon-Woods, M., Bonas, S., Booth, A., Jones, D.R., Miller, T., Sutton, A.J., Shaw, R.L.,Smith, J.A., Young, B., 2006. How can systematic reviews incorporate qualitativeresearch? A critical perspective. Qual. Res. 6 (1), 27e44.
Donaldson, C., Baker, R., Cheater, F., Gillespie, M., McHugh, N., Sinclair, S., 2011.Social business, health and well-being. Soc. Bus. 1 (1), 17e35.
Drennan, V., Davis, K., Goodman, C., Humphrey, C., Locke, R., Mark, A., Murray, S.F.,Traynor, M., 2007. Entrepreneurial nurses and midwives in the UnitedKingdom: an integrative review. J. Adv. Nurs. 60 (5), 459e469.
Farmer, J., Hill, C., Mu~noz, S.-A., 2012. Community Co-production: Social Enterprisein Remote and Rural Communities. Edward Elgar Publishing, Cheltenham.
Ferguson, K.M., 2012. Merging the fields of mental health and social enterprise:lessons from Abroad and cumulative findings from research with homelessyouths. Commun. Ment. Health J. 48 (4), 490e502.
Ferguson, K.M., 2013. Using the social enterprise intervention (SEI) and individualplacement and support (IPS) models to improve employment and clinicaloutcomes of homeless youth with mental illness. Soc. Work Ment. Health 11 (5),473e495.
Ferguson, K.M., Islam, N., 2008. Conceptualizing outcomes with street-living youngadults: grounded theory approach to evaluating the social enterprise inter-vention. Qual. Soc. Work: Res. Pract. 7 (2), 217e237.
Foot, J., 2012. What Makes Us Healthy? The Asset Approach in Practice: Evidence,Action, Evaluation. Retrieved from: www.janefoot.co.uk http://www.janefoot.co.uk/downloads/files/healthy%20FINAL%20FINAL.pdf.
Foot, J., Hopkins, T., 2010. A Glass Half-full: How an Asset Approach Can ImproveCommunity Health and Well-being. Improvement and Development Agency(Great Britain), London. Retrieved from: http://janefoot.com/downloads/files/Glass%20half%20full.pdf.
France, E.S., 2007. Applying Social Enterprise Approaches to Services for Children,Young People and Families. VCS Engage, London. Retrieved from: http://www.ncb.org.uk/media/43170/vcssocial_enterprise_approaches.pdf.
Gardin, L., 2006. A variety of resource mixes inside social enterprises. In:Nyssens, M. (Ed.), Social Enterprise: At the Crossroads of Market, Public Policiesand Civil Society. Routledge, Abingdon, pp. 111e136.
Gidley, B., 2007. Sure start: an upstream approach to reducing health inequalities?In: Scriven, A., Garman, S. (Eds.), Public Health: Social Aontext and Action. OpenUniversity Press, Maidenhead, pp. 144e153.
Glasgow Caledonian University, 2013, November 29. £2m Study Will ExamineImpact of Social Enterprise on Health in Scotland. Retrieved December 9, 2013,from. http://www.gcu.ac.uk/yunuscentre/newsevents/news/article.php?id¼68021.
Hanlon, P., Carlisle, S., Hannah, M., Lyon, A., 2012. The Future Public Health. OpenUniversity Press, Maidenhead.
Hanlon, P., Carlisle, S., Hannah, M., Reilly, D., Lyon, A., 2011. Making the case for a“Fifth wave” in public health. Public Health 125 (1), 30e36.
Harris, C., 2007. Social enterprises and the NHS. Commun. Pract. 80 (6), 44e46.Ho, A.P., Chan, K., 2010. The social impact of work-integration social enterprise in
Hong Kong. Int. Soc. Work 53 (1), 33e45.Homer-Dixon, T.F., 2000. The Ingenuity Gap: Facing the Economic, Environmental,
and Other Challenges of an Increasingly Complex and Unpredictable World.Vintage Books, New York.
nterprise to enhance health and well-being: A model and systematiccimed.2014.07.031

M.J. Roy et al. / Social Science & Medicine xxx (2014) 1e1212
Kerlin, J.A. (Ed.), 2009. Social Enterprise: a Global Comparison. University Press ofNew England, Lebanon, NH.
Kivim€aki, M., Feldt, T., Vahtera, J., Nurmi, J.-E., 2000. Sense of coherence and health:evidence from two cross-lagged longitudinal samples. Soc. Sci. Med. 50 (4),583e597.
Kretzman, J.P., McKnight, J.L., 1993. Building Communities from the Inside Out: aPath Toward Finding and Mobilizing a Community's Assets. The Asset-BasedCommunity Development Institute, Institute for Policy Research, North-western University, Evanston, IL. Retrieved from: http://www.units.muohio.edu/servicelearning/sites/edu.servicelearning/files/BuildingCommunitiesInsideOut.pdf.
Krupa, T., Lagarde, M., Carmichael, K., 2003. Transforming sheltered workshops intoaffirmative businesses: an outcome evaluation. Psychiatr. Rehabil. J. 26 (4),359e367.
Lincoln, Y.S., Guba, E.G., 1985. Naturalistic Inquiry. SAGE Publications, ThousandOaks, CA.
Lomas, J., 1998. Social capital and health: implications for public health andepidemiology. Soc. Sci. Med. 47 (9), 1181e1188.
Lysaght, R., Jakobsen, K., Granhaug, B., 2012. Social firms: a means for buildingemployment skills and community integration. Work 41 (4), 455e463.
Mancino, A., Thomas, A., 2005. An Italian pattern of social enterprise: the socialcooperative. Nonprofit Manag. Leadersh. 15 (3), 357e369.
Mandiberg, J.M., 2010. Another way: enclave communities for people with mentalillness. Am. J. Orthopsychiatry 80 (2), 170e176.
Marmot, M.G., Friel, S., Bell, R., Houweling, T.A., Taylor, S., 2008. Closing the gap in ageneration: health equity through action on the social determinants of health.Lancet 372 (9650), 1661e1669.
McKinlay, J., 1974. A case for refocusing upstream: the political economy of illness.In: Proceedings of American Heart Association Conference on ApplyingBehavioural Science to Cardiovascular Risk. American Heart Association, Seattle,WA.
McKinlay, J., 1979. A case for refocusing upstream: the political economy of illness.In: Gartley, J. (Ed.), Patients, Physicians and Illness: a Sourcebook in BehavioralScience and Health. Free Press, New York, pp. 9e25.
Millar, R., 2012. Social Enterprise in health organisation and management: hybridityor homogeneity. J. Health Organ. Manag. 26 (2), 143e148.
Mooney, G.H., 2012. The Health of Nations: Towards a New Political Economy. ZedBooks, London.
Morgan, A., Davies, M., Ziglio, E. (Eds.), 2010. Health Assets in a Global Context:Theory, Methods, Action: Investing in Assets of Individuals, Communities andOrganizations. Springer, New York.
Nussbaum, M.C., 2011. Creating Capabilities: the Human Development Approach.Belknap Press of Harvard University Press, Cambridge, MA.
Nyssens, M. (Ed.), 2006. Social Enterprise: At the Crossroads of Market, PublicPolicies and Civil Society. Routledge, Abingdon.
O'Mara-Eves, A., Brunton, G., McDaid, D., Oliver, S., Kavanagh, J., Jamal, F.,Matosevic, T., Harden, A., Thomas, J., 2013. Community engagement to reduceinequalities in health: a systematic review, meta-analysis and economic anal-ysis. Public Health Res. 1 (4), 1e548.
Pearce, J., 2003. Social Enterprise in Anytown. Calouste Gulbenkian Foundation,London.
Peredo, A.M., McLean, M., 2006. Social entrepreneurship: a critical review of theconcept. J. World Bus. 41 (1), 56e65.
Pestoff, V.A., 2000. Enriching Swedish Women's work environment: the case ofsocial enterprises in day care. Econ. Indust. Democr. 21 (1), 39e70.
Polanyi, K., 1944. The Great Transformation: the Political and Economic Origins ofOur Time, Second Beacon Paperback Edition Published in 2001. Beacon Press,Boston, MA.
Popay, J., 2006. Moving Beyond Effectiveness in Evidence Synthesis: MethodologicalIssues in the Synthesis of Diverse Sources of Evidence. National Institute forHealth and Clinical Excellence, London.
Please cite this article in press as: Roy, M.J., et al., The potential of social ereview, Social Science & Medicine (2014), http://dx.doi.org/10.1016/j.socs
Popay, J., Roberts, H., Sowden, A., Petticrew, M., Arai, L., Rodgers, M., Britten, N.,Roen, K., Duffy, S., 2006. Guidance on the Conduct of Narrative Synthesis inSystematic Reviews. Lancaster University, UK. Institute for Health Research.
Putnam, R., 2000. Bowling Alone: the Collapse and Revival of American Community.Simon & Schuster, New York.
Roy, M.J., Donaldson, C., Baker, R., Kay, A., 2013. Social enterprise: new pathways tohealth and well-being? J. Public Health Policy 34 (1), 55e68.
Roy, M.J., McHugh, N., Hill O'Connor, C., 2014. Social innovation: worklessness,welfare and well-being. Soc. Policy Soc. 13 (3), 457e467.
Scambler, G., 2007. Social structure and the production, reproduction and durabilityof health inequalities. Soc. Theory Health 5, 297e315.
Sen, A., 1985. Commodities and Capabilities. Oxford University Press, New York.Spear, R., Bidet, E., 2005. Social enterprise for work integration in 12 European
Countries: a descriptive analysis. Ann. L'�economie Publique Soc. Coop�erative 76(2), 195e231.
Stryjan, Y., 1995. Kooperativa Dagis e De F€orsta Aren (Cooperative Day Care e theFirst Years) in Kooperation & V€alf€ard (Cooperatives and Welfare). F€oreningenKooperativa Studier, Stockholm.
Teasdale, S., 2010. How can social enterprise address disadvantage? Evidence froman inner city community. J. Nonprofit Public Sect. Mark. 22 (2), 89e107.
Teasdale, S., 2012. Negotiating tensions: how do social enterprises in the home-lessness field balance social and commercial considerations? Hous. Stud. 27 (4),514e532.
Tedmanson, D., Guerin, P., 2011. Enterprising social wellbeing: social entrepreneurialand strengths based approaches to mental health and wellbeing in “Remote”indigenous community contexts. Australas. Psychiatr. 19 (Suppl. 1), S30eS33.
Townsend, P., Davidson, N., 1982. Inequalities in Health: the Black Report. Penguin,Harmondsworth.
Tsouros, A.D., 1995. The who healthy cities project: state of the art and future plans.Health Promot. Int. 10 (2), 133e141.
Uphoff, E.P., Pickett, K.E., Cabieses, B., Small, N., Wright, J., 2013. A systematic reviewof the relationships between social capital and socioeconomic inequalities inhealth: a contribution to understanding the psychosocial pathway of healthinequalities. Int. J. Equity Health 12 (1), 54.
Vidal, I., 2005. Social enterprise and social inclusion: social enterprises in the sphereof work integration. Int. J. Public Adm. 28 (9e10), 807e825.
Warner, R., Mandiberg, J., 2006. An update on affirmative businesses or social firmsfor people with mental illness. Psychiatr. Serv. 57 (10), 1488e1492.
Whitehead, M., 1992. The concepts and principles of equity and health. Int. J. HealthServ. 22 (3), 429e445.
Whitehead, M., Dahlgren, G., Gilson, L., 2001. Developing the policy response toinequities in health: a global perspective. In: Evans, T., Whitehead, M.,Diderichsen, F., Bhuiya, A., Wirth, M. (Eds.), Challenging Inequities in Health:From Ethics to Action. Oxford University Press, Oxford, pp. 309e323.
Whittemore, R., Knafl, K., 2005. The integrative review: updated methodology.J. Adv. Nurs. 52 (5), 546e553.
Wilkinson, R.G., Marmot, M.G. (Eds.), 2003. Social Determinants of Health: the SolidFacts, second ed. World Health Organization, Regional Office for Europe,Copenhagen.
Williams, A., Fossey, E., Harvey, C., 2010. Sustaining employment in a social firm:use of the work environment impact scale V2.0 to explore views of employeeswith psychiatric disabilities. Br. J. Occup. Ther. 73 (11), 531e539.
Williams, A., Fossey, E., Harvey, C., 2012. Social firms: sustainable employment forpeople with mental illness. Work 43 (1), 53e62.
Williams, D.R., Costa,M.V., Odunlami, A.O.,Mohammed, S.A., 2008.Moving upstream:how interventions that address the social determinants of health can improvehealth and reduce disparities. J. Public Health Manag. Pract. 14 (Suppl.), S8.
Yunus, M., Weber, K., 2009. Creating a World Without Poverty: Social Business andthe Future of Capitalism. Public Affairs, Philadelphia.
nterprise to enhance health and well-being: A model and systematiccimed.2014.07.031