Embed Size (px)
Citation preview

S P E C I A L V A S C U L A R E D I T I O N
Photograph supplied by Peter Kennelly, Cardiff Imaging Manager
AUTUMN EDITION 2010
ISSUE 16

1 IMAGING UPDATE - SPECIAL VASCULAR EDITION 2010, ISSUE 16
Muswellbrook, which we anticipate will be of great benefit to Upper Hunter referrers.
CT in Scone
Our new premises in Scone are almost complete and CT services will commence shortly after taking occupancy of the premises. The new premises are co-located with the Scone Medical Practice. The building and facilities are of a very high standard and we are looking forward to providing this new service.
Additional MRI at Cardiff
In Issue 15 of Imaging Update I forecast the installation of an additional state-of-the-art MRI at Cardiff. The installation was extremely well project managed and came in on schedule with first patients being scanned in December. It is now fully operational and has been instrumental in significantly reducing waiting times for MRI. The new scanner has breast MRI capability and in the coming months we will be announcing more about breast MRI and its role with Hunter Women’s Imaging.
PACS (Picture Archiving and Communications System)In late December we also began the rollout of a fully integrated RIS/PACS system in all of our practices from Belmont to Tamworth. While we have had soft copy reporting for almost 10 years, we are now moving to a totally integrated system. Until now this has been limited by the bandwidth available to the many different locations of Hunter Imaging. This is a major undertaking but we expect the
Welcome to Issue 16 of Imaging Update.
4/28 Portside CresentMaryville NSW 2293Phone: 02 4925 5451 Fax: 02 4925 5452Email: [email protected]: http://www.hunterimaging.com.au/
FRONT COVER: Nobby’s Beach
Hunter Imaging Group
Carotid Scanningand InterventionsPAGE 2
Staff Profile:Paul MyersPAGE 5
Downloading Referrers Guide to Vascular UltrasoundPAGE 5
Cardio Vascular CentreMuswellbrookPAGE 6
Brook St
RAILWAY STATIONBri
dg
e St
Sow
erb
y A
ve
New
En
gla
nd
Hig
hw
ay
William St
Market St
Will
iam
St
Ordering Request Forms Online for CVCPAGE 6
Maitland Receives Digital Radiography Unit UpgradePAGE 7
Attention All ReferrersPAGE 7
To M
etford
Gram
mar
School
Chisholm
Road
Molly M
organ Drive
New England H’way
Maitl
and
Private
Hospita
l
Maitl
and
Specialis
t
Centre
Molly
Morg
an
Hotel
N
To Newcastle
Norfolk Stre
Chelmsfo
rd D
Mr Peter SchultzChief Executive, Hunter Imaging Group
whole project to be completed before the end of June 2010. On completion this will mean faster turnaround of reports for you our valued referrers. It also facilitates subspecialist reporting and faster second opinions.
Peer Review
For many years we have run a successful internal peer review system. However with the advent of integrated PACS we are taking the opportunity to enhance our Peer Review Protocol and over the coming months will be looking at the process of inviting your participation as a referring doctor to enhance our ability to deliver optimal patient care on your behalf.
CT Coronary Angiography (CTCA)
Our congratulations to Dr Stuart Slater who has become the first doctor in the Hunter to be recognised as a CTCA Specialist. In order to be recognised as a CTCA Specialist, Cardiologists, Nuclear Medicine Physicians and Radiologists need to demonstrate that they have completed the requisite training criteria. The requisite training criteria are quite demanding and I’d like to thank Stuart for the big effort he put in to achieve CTCA Specialist recognition.
Thank you for your continued support.
Welcome to this special edition of imaging update focusing on Carotid Scanning and Interventions. Our thanks to Dr Paul Myers for his work and contribution to this edition. We are proud of the quality work our highly skilled sonographers perform at the Cardio Vascular
Centre in consultation with our consultant vascular surgeons and I am sure you will find the content of Paul’s article practical and useful.

2HUNTER IMAGING GROUP NEWSLETTER
For this reason imaging of the extra-
cranial carotid and vertebral circulation
is extremely important.
There are a number of modalities for
imaging the carotid and vertebral circulation,
including duplex scanning, digital subtraction
angiography, CT angiography, and magnetic
Carotid artery disease is involved in approximately 30% of all acute cerebral neurological events, mainly cerebrovascular accidents (CVA). CVA’s due to carotid disease are, in the main, preventable if the carotid changes are diagnosed prior to symptoms occurring.
CONTINUES PG 3.
Carotid Scanningand InterventionsBy Dr Paul Myers
resonance angiography. The least invasive of
these is duplex scanning.
Duplex scanning involves pulsed Doppler
systems with real-time spectral analysis and
fast-fourier transformation in association with
B-mode ultrasound, thus “duplex scanning”.
As always, these examinations remain highly
operator and reporter dependent.
As the reliability and technical capability
of scanners has increased, so too has the
reliability of scanning of these vessels using
duplex ultrasound. Most disease of the
carotids is atherosclerotic stenosis which
mostly occurs at the origins of the internal and
external carotid arteries.
For technical reasons the degree of stenosis
cannot be specified as a specific percentage.
Rather, classifications may be reported as
follows:
1. Normal
2. < 15% diameter reduction
3. 10-20% diameter reduction
4. 20-40% diameter reduction
5. 30-50% diameter reduction
6. 50-60% diameter reduction
7. 60-80% diameter reduction
8. 80-99% diameter reduction
9. Occluded
These classifications are assigned using
a number of criteria including systolic and
diastolic velocities, waveforms, internal carotid
artery (ICA), external carotid artery (ECA), and
common carotid artery (CCA) ratios.
Colour Doppler waveform, Internal Carotid Artery with 80% stenosis

3 IMAGING UPDATE - SPECIAL VASCULAR EDITION 2010, ISSUE 16
CONTINUED FROM PAGE 2
Although the exact parameters and the way
they are expressed vary, the meaning of
the features is constant and is in line with
haemodynamic concepts.
Colour Doppler represents the signal as a
vector. Thus, objects moving towards the
transducer will appear in red, and objects
moving away from the transducer will appear
in blue.
The faster the velocity, the brighter the colour
and the lower the velocity, the darker the colour.
Thus, colour duplex allows greater definition of
the lesion.
It has now been established in numerous trials
that duplex scanning is safe, non-invasive,
reliable and can be reproduced in appropriate
operator and reporter hands.
What To Do With The Results?
This has been conclusively established by
the North American Symptomatic Carotid
Endarterectomy Trial (NASCET), and the
European Carotid Surgery Trial (ECST), both
large, randomised Class I studies.
These found that, for symptomatic patients
with a 70% or more stenosis, an intervention
was required to prevent stroke. This
recommendation has not changed.
There are a number of studies done also
looking at asymptomatic patients, particularly
the European Asymptomatic Carotid Surgery
Carotid Scanning and Interventions
Colour Doppler, Internal Carotid Artery with 80% stenosis
Trial (ACST). Here, the recommendations are
that those with a stenosis of > 80% should
have an intervention.
There is also evidence that symptomatic
patients with less severe carotid occlusions
(50-60%) show a benefit from intervention,
albeit less so. Additionally, patients who are
asymptomatic but have a stenosis > 60% also
benefit from intervention, but only if their co-
morbidities and anatomy put them in a very
low-risk group.
For maximum benefit symptomatic patients
should be operated on soon after a TIA or
stroke, preferably within the first month.
The standard procedure for many years was
carotid thrombo-endarterectomy (CTEA).
This procedure has well defined mortality and
morbidity figures in good hands. But many
complications, such as up to 10% local nerve
dysfunction, can also be quite significant.
Recent years have seen the development of
carotid artery stenting (CAS) as an alternative
to CTEA.
CAS has seen numerous registries and trials
compiled and performed.
The Stent-Protected Angioplasty Versus
Carotid Endarterectomy (SPACE) trial was
stopped because the numbers needed to
reach statistical significance were not able to
be achieved because the recruitment was too
slow and the trial funding ceased. It did not
show that CTEA was superior to CAS or the
reverse.
The Endarterectomy versus Angioplasty in
patients with severe Carotid Stenosis (EVA -
3S) trial, a French trial, purported to show that
CAS was inferior to CTEA. However, there
have been serious doubts raised about the
methodology of this trial and hence the validity
of the results.
The International Carotid Stenting Study (ICSS)
trial has very recently released preliminary
results.
Whilst these appear to indicate that CAS
may not be as good as CTEA, there are also
significant issues with this trial.
4HUNTER IMAGING GROUP NEWSLETTER
The jury “remains out” on the best treatment.
The Carotid Revascularisation Endorterectomy
versus Stenting Trial (CREST) in the USA,
has released its preliminary results. The trial
has shown that CAS and CTEA are, overall,
equivalent. Patients aged less than 70 years
did marginally better with CAS, while patients
aged over 70 years did marginally better with
CTEA. The rates for stroke and death for both
procedures were the lowest reported in any
trial to date.
Regardless, all the trials and the data confirm
that those patients who are symptomatic,
particularly those who have amaurosis fugax,
transient ischaemic attack or stroke and who
have an appropriate carotid lesion, should
have an intervention.
Medical ManagementThe use of statins over the last 10-15 years,
in addition to the availability of more effective
anti-platelet agents such as clopidogrel, has
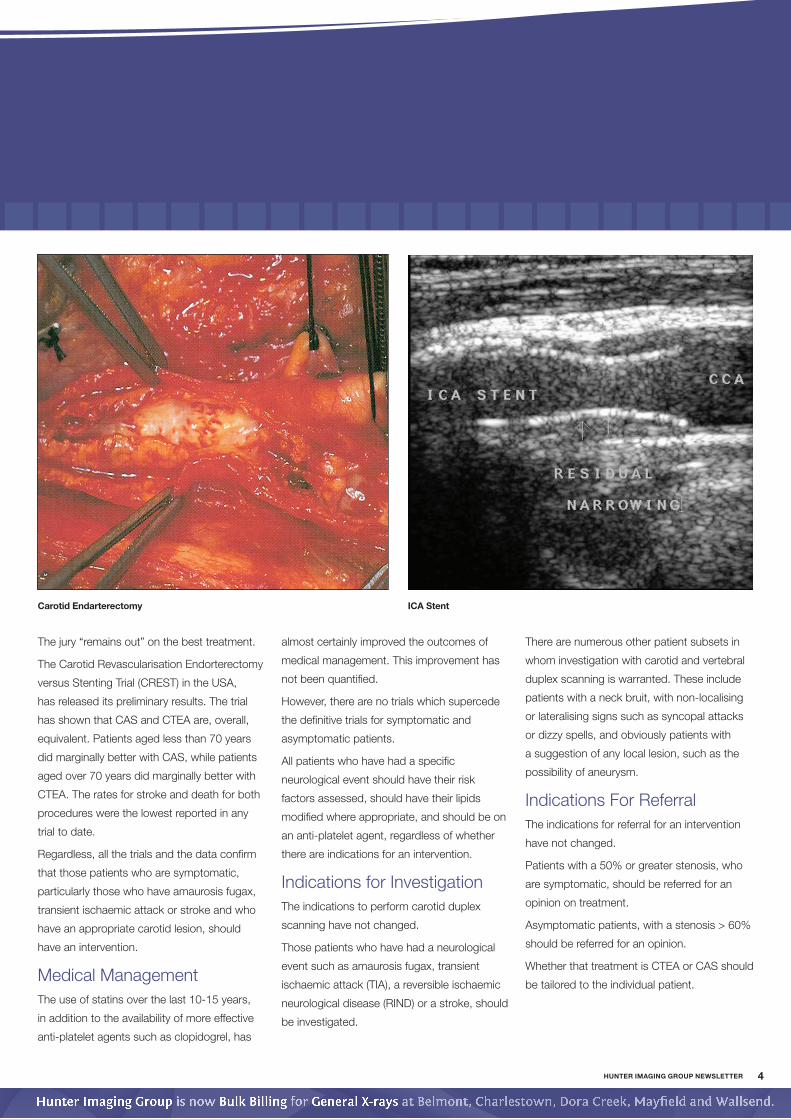
Carotid Endarterectomy ICA Stent
almost certainly improved the outcomes of
medical management. This improvement has
not been quantified.
However, there are no trials which supercede
the definitive trials for symptomatic and
asymptomatic patients.
All patients who have had a specific
neurological event should have their risk
factors assessed, should have their lipids
modified where appropriate, and should be on
an anti-platelet agent, regardless of whether
there are indications for an intervention.
Indications for InvestigationThe indications to perform carotid duplex
scanning have not changed.
Those patients who have had a neurological
event such as amaurosis fugax, transient
ischaemic attack (TIA), a reversible ischaemic
neurological disease (RIND) or a stroke, should
be investigated.
There are numerous other patient subsets in
whom investigation with carotid and vertebral
duplex scanning is warranted. These include
patients with a neck bruit, with non-localising
or lateralising signs such as syncopal attacks
or dizzy spells, and obviously patients with
a suggestion of any local lesion, such as the
possibility of aneurysm.
Indications For ReferralThe indications for referral for an intervention
have not changed.
Patients with a 50% or greater stenosis, who
are symptomatic, should be referred for an
opinion on treatment.
Asymptomatic patients, with a stenosis > 60%
should be referred for an opinion.
Whether that treatment is CTEA or CAS should
be tailored to the individual patient.

5 IMAGING UPDATE - SPECIAL VASCULAR EDITION 2010, ISSUE 16
Step 1Go online and access
the website at:
www.hunterimaging.com.au/cvc
Step 2Once on the Cardio Vascular
Centre home page select
“Information for Our
Referrers” at the top of the
page. When the drop down
menu is visualised click on
“Publications”
By accessing the Cardio Vascular Centre’s website you or your staff can download or print
a copy of Referrers Guide to Vascular Ultrasound. It’s quick and easy. See the instructions
below to see how this can be done.
Step 3Double click to open file and
from there you can download
onto your desktop or print a
copy.
rofilePaul Myers is a Vascular and Endovascular
Surgeon based in Newcastle.
He has been a consultant to the Cardio
Vascular Centre, now part of the Hunter
Imaging Group, since 1988.
He trained initially in general surgery and
subsequently vascular surgery in Australia and
England.
He finds the new techniques in vascular surgery
extremely exciting especially for endovascular
procedures for aortic aneurysm, carotid artery
disease, peripheral and visceral artery disease
and those being introduced for below knee
arterial disease.
He is in private practice with rooms at
Newcastle Private Hospital (NPH) Medical
Suites. He also consults in Maitland, Singleton
and Tamworth.
He is a Conjoint Associate Professor at the
University of Newcastle.
He is a Member of the Executive of the ANZ
Society of Vascular Surgery.
He is a Member of the Executive of the Hunter
Post Graduate Medical Institute.
He is a Councillor of the NSW AMA,
representing the Hunter and Central Coast
regions.
He remains active in the Army Reserve in the
rank of Colonel, having served overseas on
numerous deployments
profileprofile
M.B.B.S.(Syd), F.R.C.S. (Eng), F.R.A.C.S., AIMM
Paul Myers
Contact Details:Suite 2.1, NPH Medical Suites
24 Lookout Road, New Lambton Heights
NSW 2305
Phone: 02 4953 9615
Fax: 02 4953 9618
Downloading Referrers Guideto Vascular Ultrasound Did you know that you can download a Referrers Guide to Vascular Ultrasound from the Cardio Vascular Centre’s website to your desktop?

6HUNTER IMAGING GROUP NEWSLETTER
N
Brook St
RAILWAY STATIONBri
dg
e St
Sow
erb
y A
ve
New
En
gla
nd
Hig
hw
ay
William St
Market St
Will
iam
St
This new location at 55 Brook
Street Muswellbrook will assist you
and your patients in providing the
imaging service required for diagnosis of
vascular disease.
Our sonographer, Helen Charlwood,
already scans for general ultrasound
with Hunter Imaging Group and has
had inhouse training with senior CVC
sonograpghers to gain competency with:
Arterial Leg scans •
Carotid Artery scans•
AAA scans•
DVT scans•
Over the coming months she will attend
more training to be proficient with:
Renal Artery scans•
Endoluminal graft scans•
She is enjoying the challenge of new
examinations and looks forward to being
able to perform more examinations in the
future to help provide a great service to
patients in the area.
Ordering RequestForms Online for CVC
Step 1Go online and access
the website at:
www.hunterimaging.com.au/cvc
Did you know that you can order Cardio Vascular Centre request forms online?
By accessing the Cardio Vascular Centre’s website you or your staff can order a range of
request forms. It’s quick and easy. See the instructions below to see how this can be
done.
Step 2Once on the Cardio Vascular
Centre home page select
“Information for Our Referrers”
at the top of the page. When the
drop down menu is visualised
click “Request Pads Order”
Step 3Fill in data.
Scroll further down the screen
and make your selection and
click on “Submit”
Cardio Vascular Centre
MuswellbrookCardio Vascular Centre is pleased to announce that we have opened a branch in the Upper Hunter Valley.
If you would like to know more or wish to speak to our signing doctors or sonographers about a specific case please contact our referrer services team on 49255 430.

7 IMAGING UPDATE - SPECIAL VASCULAR EDITION 2010, ISSUE 16
The upgrade of equipment means shorter, more
comfortable examinations for patients.
With high performance attributes such as:
Increased field of exposure, to cover more anatomy in 1.
one exposure;
Increased number of exposure chambers to read 2.
exposures more accurately, this will reduce patient dose;
Excellent image quality with scintillator that has high 3.
resolution ratio;
Fixed detector with excellent pixel ratio, which leads to 4.
reduction in exposure level to patient; and
High projection ability, equipment can be moved around 5.
patient instead of patient being placed in awkward
positions during examinations.
Maitland Receives Digital Radiography Unit Upgrade Hunter Imaging Group has recently installed a new Philips Digital Radiography unit at its Maitland rooms.
We are no longer at Mitchell Drive, moving to our new location
two years ago. Some of you would still have old request forms
with the Mitchell Drive address and map on it (confusing
some patients), so if you would like updated request forms please contact
Referrer Services 49255430 or e-mail [email protected]
or order online at website; www.hunterimaging.com.au/cvc (see page 6
for detailed instructions)
Attention All ReferrersCardio Vascular Centre has rooms at East Maitland.
Cardio Vascular Centre, East Maitland
Level 1, Suite 7
Maitland Specialist Medical Centre - Maitland Private Hospital
Corner Chisholm Road and New England Highway, East Maitland
New Address To M
etford
Gram
mar
School
Chisholm
Road
Molly M
organ Drive
New England H’way
Maitl
and
Private
Hospita
l
Maitl
and
Specialis
t
Centre
Molly
Morg
an
Hotel
N
To Newcastle
Norfolk Street
Chelmsfo
rd D
rive





























