Embed Size (px)
Citation preview

Postgraduate Medical Journal (September 1982) 58, 554-557
CLINICAL REPORTS
The distal form of spinal muscular atrophy: an unusual case demonstrating theintermediate variety
D. A. ISENBERG* PAULINE A. KAHNtM.B., B.S., M.R.C.P. M.B., Ch.B.*Department ofRheumatology, University College Hospital, London WC1 and tDepartment of Neuropathology,Whittington Hospital, London N19
SummaryA 14-year-old boy with a long history of distal muscleweakness affecting primarily and predominantly theupper limbs is described. There is a family history ofpes cavus and congenital dislocation of the hip.Electromyography and histopathological studies ofskeletal muscle showed conclusive evidence of aneurogenic muscular disorder, and excluded primarymuscle disease. The muscle biopsy showed groupatrophy. As many target fibres which are identical tostructured cores were a prominent feature of thebiopsy, central core disease was considered. How-ever, it was concluded on clinical, neurophysiologicaland histological evidence that the patient was suffer-ing from distal spinal muscular atrophy of an interme-diate type designated by previous authors.A review of the current concepts of distal muscle
weakness is included.
IntroductionIt has become apparent within the past few years
that patients presenting with predominantly distalmuscle weakness may be suffering from a variety ofclinical syndromes. The earliest descriptions ofpatients presenting with peroneal muscular atrophywere those of Charcot and Marie (1886) and Tooth(1886). They described a disease presenting inchildhood causing progressive weakness and atrophyof distal muscles and some sensory deficit, affectingthe lower limbs and much later, the upper limbs.Subsequent clinical descriptions indicated that awide variety of variants existed. A more orderedclassification became possible with the introductionof nerve conduction studies in the mid-nineteen-fifties.
In 1968 Dyck and Lambert defined two broadgroups. Group I comprised cases with severely
reduced motor and sensory nerve conduction velo-city, sometimes with hypertrophic nerves. Some casesof Charcot-Marie-Tooth disease fall into this group.In Group II nerve conduction velocity was relativelypreserved and this group included the 'neuronal'form of Charcot-Marie-Tooth disease. Subsequently,these two groups have been termed hereditary motorand sensory neuropathy (HMSN) types I and II(Thomas and Calne, 1974; Thomas, Calne andStewart, 1974; Dyck, 1975).Harding and Thomas (1980) reviewed 262 cases of
peroneal muscular atrophy. A total of 228 cases wereclassified as HMSN types I or II. The remaining 34cases had the clinical syndrome ofperoneal muscularatrophy without sensory loss, which displayed elec-tromyographic evidence of denervation in the distalmusculature, normal or slightly reduced motor nerveconduction velocities and normal sensory actionpotentials. These patients were classified as examplesof distal spinal muscular atrophy.The spinal muscular atrophies are a heterogeneous
group of disorders which may present from birth toadult life, in which progressive degeneration oflowermotor neurones occurs leading to neuropathicatrophy of muscles. It is usually the proximal muscleswhich are affected but occasionally distal muscles ofthe lower limbs are involved (Martin-Sneesens, 1962;Dyck and Lambert, 1968; Brust, Lovelace and Devi,1978). Very rarely the distal muscles of the upperlimbs are predominately affected (O'Sullivan andMcLeod, 1978). We describe a case which supportsthe existence of an 'intermediate' distal spinal mus-cular atrophy (SMA) in which the distal muscles ofboth arms and legs are involved from the earlieststages of the disease.
Case reportA 14-year-old schoolboy presented with a history
of weakness in his hands for as long as he couldCorrespondence and requests for reprints to Dr Pauline Kahn.
0032-5473/82/0900-0554 $02.00 © 1982 The Fellowship of Postgraduate Medicine
Protected by copyright.
on Novem
ber 17, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.58.683.554 on 1 Septem
ber 1982. Dow
nloaded from

Clinical reports 555
I 1 <2
II
laI 1 ~2 e4 3
m 1 q(2 it 3 g4 d'5t
I Propositus 0 Pes cavus 0 Congenital hip dislocation
FIG. 1. Family tree showing the presence ofpes cavus and congenitalhip dislocation.
remember. For four years he had been particularlyaware of the problem as it had prevented him fromnormal participation in gymnastics. For two years hehad been unable to lift heavy objects and foundwriting increasingly difficult. He had found difficultyin doing up his shirt buttons for one month. He alsocomplained of intermittent cramps in the hands andforearms for one year. He had not noted any
exacerbation of his symptoms during cold weather.He did not walk until age 17 months and had 2operations when aged 3 and 6 years, for a leftcongenital hip dislocation. He had been aware ofslight weakness of feet and ankles for about 4 years,though he was not greatly restricted by this. Therewas a family history of pes cavus and congenital hipdislocation (Fig. 1). Examination of the patient'sparents and siblings revealed no abnormalities apartfrom the scar of an operation for congenital hipdislocation in the younger sister (case III 3).On examination, pes cavus, a slight kyphoscoliosis
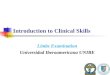
and the scar of his operations were evident. Therewere no abnormalities in his cardiovascular, respira-tory or abdominal systems. His cranial nerves werenormal. In his upper limbs slight wasting of thedeltoids and forearm muscles and more markedwasting of the small muscles ofthe hands (Fig. 2) wasevident. Tone was a little reduced bilaterally andthere was no evidence of myotonia. Power wasreduced to 4+ (MRC grading) in the proximalmuscles and 4- in the flexors and extensors of thewrist and in the small muscles of the hand. Deeptendon reflexes were uniformly absent. The abdomi-nal reflexes were present. There were no sensoryabnormalities. In the lower limbs mild calf hyper-trophy was present. There was no muscle wasting oralteration in tone. Power was 4+ in all muscle groupsexcept in the ankle dorsiflexors and evertors of thefeet which were grade 4. Deep tendon reflexes wereabsent and the plantar responses were both flexor.Sensation was normal.
.........:,. ..rg'15 l #gEE
..sJi * .. xm ........... i l li l 11_~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~||l|¢,|,,̂,L~~~~~~~~~~~.. ....
,T.. . _ | | | X =
FIG. 2. Palmar aspect of the hands of the patient. There is wasting of thenar and hypothenare eminences.
Protected by copyright.
on Novem
ber 17, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.58.683.554 on 1 Septem
ber 1982. Dow
nloaded from

556 Clinical reports
Investigations
The full blood count, urea and electrolytes, liverfunction tests, serum calcium and phosphorus wereall normal. His creatine phosphokinase was 81 iu./l(normal 0-50) and the 24-hr urine creatine was 1380mmol (normal 0-400).
Electromyography showed no evidence of a myo-pathic process. However, sampling of several limbmuscles showed continuous fibrillation with themuscles relaxed and fasciculation of either single orgrouped units, some of large amplitude. Thesechanges were most marked in the distal muscles. Themotor conduction velocity of the median nerve was40 m/s (normal mean 55-1 m/s, s.d. ± 5 2) and of theulnar nerve was 31 m/s (normal mean 59-4 m/s,s.d. ± 5 0). Testing for sensory function of the medianand ulnar nerves at the wrist revealed no abnor-malities. Motor conduction velocity for the lateralpopliteal nerve (knee to ankle segment) was 37 m/s(normal mean 52-0 m/s, s.d. ± 4 0). The normalmeans and standard deviations are those quoted byJohnson (1980). A normal sural nerve action poten-tial was recorded.A biopsy of the left vastus lateralis muscle was
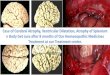
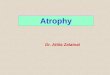
examined by light and electronmicroscopy. Therewas prominent atrophy of groups of fibres-groupfibre atrophy (Fig. 3). There were areas of mildendomyseal fibrosis and occasional intrafascicular fatcells. On transverse sections several fibres had palecentral zones, best demonstrated on phosphorylaseand on oxidative enzyme histochemical preparations
YJ
FIG. 3. Group fibre atrophy is seen and scattered atrophic fibres ofboth types 1 and 2. ATPase at 9-4 x 100.
Kw*m - w -
J' o ¼i2i
4~~-
-iS.-,84wF .__-* wn w _t F _
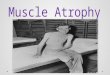
FIG. 4. In this field a large proportion ofgrouped type 1 fibres exhibit'core targetoid' zones (arrows). NADH-TR x 100.
(Fig. 4). On electron microscopy these 'core zones'were sharply defined, devoid of organelles and hadcentral electron dense material.
DiscussionAs discussed in the introduction, the clinical
syndrome of peroneal muscular atrophy may bedesignated as HMSN type I and II or as distal spinalmuscular atrophy. The differential diagnosis con-sidered in this case was between these conditions and,on account of the histological appearances of themuscle, central core disease.A diagnosis of HMSN was considered untenable
since the main problems in the patient described werein the distal part of the upper limbs rather than thelower limbs, the sensory system was normal onclinical and electrophysiological testing, and therewas electromyographic and histological evidence of aneurogenic disorder.The core zones seen in the muscle fibres could be
either central cores which are the characteristicfeature of a primary muscle disorder, central coredisease, or they are targetoid areas, a feature of targetfibres, sometimes seen in neurogenic atrophy.
Skeletal muscle fibres can be divided into types 1and 2, the former being rich in oxidative enzymes, the
Protected by copyright.
on Novem
ber 17, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.58.683.554 on 1 Septem
ber 1982. Dow
nloaded from

Clinical reports 557
latter in glycolytic enzymes. Targetoid or core zonesare seen only in type 1 fibres. In central core diseasethere is a preponderance of type 1 fibres and 90%o ofthese exhibit central cores (Dubowitz and Brooke,1973). These criteria were absent in this musclebiopsy so the diagnosis of central core disease was nottenable.
Target fibres in this number and distribution are acharacteristic of denervating disease (Engel, 1961).Furthermore, the unequivocal and prominent groupfibre atrophy is only seen in denervation atrophy.Thus the biopsy findings endorsed the neurophysio-logical criteria which pointed to a diagnosis of spinalmuscular atrophy.
Clinically the case described fits the earlier descrip-tion of distal spinal muscular atrophy recentlyreviewed by Harding and Thomas (1980). Theynoted onset of the disease during the first decade in22 out of 34 cases, a higher incidence amongst malesand variable patterns of inheritance. Sporadic caseswere the commonest comprising 23% of the total.Given our patients's family history of pes cavus it islikely that there may be a genetically determinedskeletal defect in this family. However, as bothparents were normal on examination it cannot be asimple autosomal dominant defect.The recent clinical classification of spinal muscular
atrophy into 7 types by Pearn (1980) is most usefuLbut in some respects confusing. In particular, hisreference to a distal form as 'Charcot-Marie-Toothlike' does not prove to be a homogeneous group whenthe cases quoted by him to support the separateexistence of this subgroup are studied. For example,the cases quoted by Dyck and Lambert (1968) and byPearn and Hudgson (1979) describe patients in whomthe lower limbs bore the brunt of the disease. Incontrast, the cases described by Meadows andMarsden (1969) and the first patient described byMagee (1960) showed the upper limbs to be predomi-nantly involved. We suggest a more appropriateclassification of this subgroup should be consideredaccording to the clinical observations ofHarding andThomas (1980). They proposed that there are inter-mediate cases between the common form of distalspinal muscular atrophy which predominantly in-volves the legs and the much rarer variety with pureupper limb involvement, as described by Larder,Eadie and Tyner (1976) and O'Sullivan and McLeod(1978).
In the intermediate category there is markedweakness of the upper limbs with less severe prob-lems in the lower limbs, as described in family 3 byHarding and Thomas (1980). Young and Harper(1980) described a young patient who is best classi-fied in this category. He noted weakness in his handsfollowed shortly afterwards by lower limb weakness.He had normal sensory nerve conduction and slight
slowing of motor conduction (41 m/s) in the ulnarnerve. We suggest that it is in this unusual interme-diate category of distal spinal muscular atrophy thatthe patient described in our paper may best beclassified.
AcknowledgmentsThe authors are indebted to the late Dr Peter Croft for permission
to report this case. We are grateful to Professor R. H. T. Edwards forthe use of his laboratory facilities, to Dr Jennifer McDougall forelectron microscopy and to Mrs Kathy Deed for typing andsecretarial help.
ReferencesBRUST, J.C.M., LOVELACE, R.E. & DEVI, S. (1978) Clinical and
electro-diagnostic features of Charcot-Marie-Tooth syndrome.Acta Neurologica Scandinavia, S8, Suppl. 68, 1.
CHARCOT, J.M. & MARIE, P. (1886) Sur une forme particuliered'atrophie musculaire progressive, souvent familiale, debutant parles pieds et les jambes, et atteignant plus tard les mains. Revue deMddecine (Paris), 6, 97.
DuBowITz, V. & BROOKE, M.H. (1973) Muscle Biopsy: A ModernApproach, p. 254. W. B. Saunders, London.
DYCK, P.J. (1975) Inherited neuronal degeneration and atrophyaffecting peripheral motor, sensory and autonomic neurons. In:Peripheral Neuropathy (Ed by Dyck, PJ., Thomas, P.K. &Lambert, E.H.), Vol. 2, p. 285. W. B. Saunders, Philadelphia.
DYCK, P.J. & LAMBERT, E.H. (1968) Lower motor and primarysensory neuron diseases with peroneal muscular atrophy. 1.Neurologic, genetic and electrophysiologic findings in hereditarypolyneuropathies. Archives of Neurology (Chicago), 18, 603.
ENGEL, W.L. (1961) Muscle target fibres, a newly recognised sign ofdenervation. Nature (London), 191, 389.
HARDING, A.D. & THOMAS, P.K. (1980) Hereditary distal spinalmuscular atrophy. A report on 34 cases and a review of theliterature. Journal of the Neurological Sciences, 45, 337.
JOHNSON, E.W. (1980) Practical Electromyography. Williams &Wilkins, Baltimore.
LARDER, C.M., EADIE, M.J. & TYNER, J.M. (1976) Hereditary motorperipheral neuropathy affecting the arms. Journal of the Neuro-logical Sciences, 28, 389.
MAGEE, K.R. (1960) Familial progressive bulbospinal muscularatrophy. Neurology (Minneapolis), 10, 295.
MARTIN-SNEESENS, L. (1962) Formes a evolution tres prolonges del'amyotrophie spinale de Werdnig-Hoffman. Journal de genetiquehumaine (Geneva), 11, 251.
MEADOWS, J.C. & MARSDEN, C.D. (1969) A distal form of chronicspinal muscular atrophy. Neurology (Minneapolis), 19, 53.
O'SULLIVAN, D.G. & McLEoD, J.G. (1978) Distal chronic spinalmuscular atrophy involving the hands. Journal of Neurology,Neurosurgery and Psychiatry, 41, 653.
PEARN, J.P. (1980) Classification of spinal muscular atrophies.Lancet, L 919.
PEARN, J. & HUDGSON, P. (1979) Distal spinal muscular atrophy: Aclinical and genetic study. Journal ofthe Neurological Sciences, 43,183.
THOMAS, P.K. & CALNE, D.B. (1974) Motor nerve conductionvelocity in peroneal muscular atrophy: evidence for geneticheterogeneity. Journal ofNeurology, Neurosurgery and Psychiatry,37, 68.
THOMAS, P.K., CALNE, D.B. & STEWART, G. (1974) Hereditarymotor and sensory polyneuropathy (peroneal muscular atrophy).Annals ofHuman Genetics, 38, 11 1.
TOOTH, H.H. (1886) The Peroneal Type of Progressive MuscularAtrophy. H.K. Lewis, London.
YOUNG, I.D. & HARPER, P.S. (1980) Hereditary distal spinalmuscular atrophy with vocal cord paralysis. Journal ofNeurology,Neurosurgery and Psychiatry, 43, 413.
Protected by copyright.
on Novem
ber 17, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.58.683.554 on 1 Septem
ber 1982. Dow
nloaded from