Embed Size (px)
Citation preview

1
Spindle Cell Lesions
A.A. Sahin, M.D. Professor of Pathology and Translation Molecular
Pathology Section Chief of Breast Pathology
23rdAnnual Seminar in Pathology
Outline
• Morphologic features of spindle cells
lesions
• Differential diagnosis
• Case presentations
Wide Spectrum
• Bland, low grade spindle cells
•High grade, pleomorphic spindle cells

2
Fibroblastic/Myofibroblastic Lesions
•Nodular fasciitis
• Fibromatosis
•Myofibroblastoma
• Scar
Other Benign Mesenchymal Spindle Cell Lesions
• Pseudoangiomatous stromal hyperplasia (PASH)
•Neurofibroma
• Schwannoma
• Leiomyoma of nipple
Case 1
• 29 yo female with palpable right breast mass

3

4
Case 2
• 64 yo female, mammogram revealed a 2 cm mass

5
β-catenin

6
Fibromatosis of Breast
• Females > males
• Peak 20-50 years
• Painless, firm, slow-growing mass
• May closely mimic carcinoma – Can be stellate radiologically
• May be associated with FAP, other desmoid type tumors
• Treatment: wide local excision
• Local recurrence 15-30%
Fibromatosis of Breast
• Most cases < 5 cm
• Histologically similar to desmoids in other sites
• Long fasicles of bland spindled cells
• Entrapment of breast parenchyma
• May resemble fasciitis
• Peripheral lymphocytic infiltrate common
• Local recurrence in 27%

7
Nodular Fasciitis
• Young adults
• Short duration, often tender
•Most < 5 cm
• Rare local recurrence
Nodular Fasciitis
• Circumscribed
• Plump spindled cells
• Brisk mitotic rate
• Microcystic & myxoid areas
• Inflammatory infiltrate throughout lesion
• Extravasated RBC’s
• Normal breast parenchyma not entrapped
Case 3
• 41 year-old female with right breast mass

8

9
CK
CK

10

11
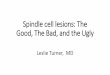
Fibromatosis-Like Spindle Cell
Carcinoma • First described as fibromatosis like metaplastic tumor
• Non-metastasizing – Gobbi, et al. Cancer 1999
• Recent study showed to be a low grade tumor
• Potential for local recurrence and distant metastasis
• No involvement axillary nodes
• Lumpectomy with clear margins or simple mastectomy
•A variant of metaplastic ca
•Discrete nodule, infiltrative
borders
•Spindle cells in intersecting
fascicles, storiform pattern
(>90-95%)
•Collagenous stroma
Fibromatosis-Like Spindle Cell Carcinoma

12
•Slender nuclei with
tapered edges
•Mild nuclear
pleomorphism
•Low mitotic rate
•Epitheloid or
squamous foci
•Focal heterologous or
in situ component
Fibromatosis-Like Spindle Cell Carcinoma
Fibromatosis
Fibromatosis-Like Spindle Cell Carcinoma
Fibromatosis-Like Spindle Cell Carcinoma
• Thorough sampling is essential to demonstrate epithelial elements and exclude aggressive components
• It is important to search for epithelial differentiation even in bland spindle cell lesions

13
Fibromatosis-Like Spindle Cell Carcinoma
Immunohistochemistry
• Cytokeratin (gold standard) – Patchy
• 34ßE12 + (CK903)
• AE1/AE3 +
• CK7 –
• EMA +/-
• SMA + in CK+/- cells
• ER/PR -
• Her-2/neu -
Differential Diagnoses
• Fibromatosis
• Nodular fasciitis
• Fibromatosis like spindle cell carcinoma
Differential Diagnoses
Spindle Cell Ca Nodular Fasciitis Fibromatosis
Epitheloid Areas +/- - -
Tumor Edge Infiltrative Well defined Infiltrative
Ducts & Lobules Entrapped Push aside Entrapped
Fascicles Short Short Long broad
Mitosis
Infrequent Numerous Infrequent or
Focally numerous
Cytokeratin Positive Negative Negative

14
Differential Diagnosis
CK beta-Catenin
Spindle Cell Ca + N/A
Fibromatosis - nuclear +
• 75 yo male with h/o myelodysplastic syndrome, now develops a left breast mass
Case 4

15

16
SMA
CK
Myofibroblastoma
- Males = females
- Concurrent gynecomastia in male
- Peak 50 – 75 years
- Increasingly detected on mammogram
- Mammogram: homogeneous, lobulated, well-circumscribed and lacks microcalcifications
- Findings suggestive of fibroadenoma or hamartoma

17
Myofibroblastoma
•Solitary, slow growing nodule or mass
•Located in breast parenchyma and range in size from 0.9 to 10cm
Myofibroblastoma
•Cut surface is gray-pink to tan-white
•Cysts and hemorrhage are absent
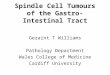
Myofibroblastoma
Histology: - Circumscribed, devoid of
mammary ducts and lobules, compressed parenchyma forms a pseudocapsule
- Moderately cellular with uniform,
ovoid to spindle cells arranged diffusely or in clusters
- Broad bands of hyalinized
collagen distributed throughout the tumor

18
Myofibroblastoma
- Lack atypia, necrosis, or significant mitotic figures, 0 – 1/ 10 HPF
- Mast cells are seen in many cases - Occasionally has cartilaginous metaplasia – no
influence on clinical behavior - Variant forms: collagenized / fibrous epithelioid cellular infiltrative myxoid
Fibrous Infiltrative
Epithelioid Myxoid
Differential Diagnosis
• Metaplastic carcinoma (CK+)
• Reactive spindle cell lesion/nodular fasciitis – Plump myoid cells,
– Inflammatory reaction
– Foci of microcystic myxoid change
– RBC extravasation
– Desmin –
• Fibromatosis – Infiltrative margins w/finger-like extension of monotonous
fibroblasts
– Entrapped glands

19
Differential Diagnosis
• Spindle cell lipoma
–more abundant adipose tissue and mast cells
• Solitary fibrous tumor
–Bland spindle cells admixed w/thin, or less frequently, thick collagen
–Hemangiopericytoma-like vascular pattern
–Desmin -
Case 5
• 58 yo female with 3 cm slow growing mass in the right breast over the past 3 years

20

21

22
ER
Pan-CK
Desmin

23
CD34
Myofibroblastomawith epithelioid and adipocytic
components
Diagnosis
Myofibroblastoma
• Resembles spindle cell lipoma
But. . .
• More cellular and fascicular
• Rare smooth muscle/cartilage metaplasia
• CD34 / desmin positive, SMA variable
• Loss of 13q and 16q
• Cytogenetic relationship to spindle cell/ pleomorphic lipoma (may be related)

24
Differential Diagnosis
Myofibroblastoma Nodular fasciitis
Fibromatosis Spindle cell
lipoma
Edge Well defined Well defined Infiltrative Well defined
Ducts & lobules Not entrapped Not entrapped Entrapped Not entrapped
Mitosis Infrequent Numerous Infrequent or
focally numerous
Infrequent
Inflammatory infiltrates
Peripheral Central Peripheral N/A
SMA + + + -
Desmin + - - -
CD34 + Focal + - +
High Grade Spindle Cell Neoplams
•Metaplastic (sarcomatoid) carcinoma
• Bona fide sarcoma
•Malignant phyllodes tumor
Spindle Cell Sarcomas of the Breast
-Extremely uncommon-
• Post-radiation sarcoma, NOS
• Leiomyosarcoma
• MPNST
• Metastasis from elsewhere
*Must rule out recurrent malignant phyllodes tumor!

25
Case 6
• 47 yo female with 7 cm left breast mass

26
CK
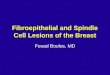
Metaplastic (Sarcomatoid) Carcinoma Main Morphologic Patterns
• Spindle cell
• Pleomorphic (MFH-like) +/- giant cells
• With squamous metaplasia
• With heterologous elements (usually osteosarcoma / chondrosarcoma)
Metaplastic (Sarcomatoid) Carcinoma
Diagnostic Clues
• Adjacent DCIS/ invasive ductal carcinoma (not always present)
• Squamous metaplasia
• Plump, somewhat more epithelioid atypical spindle cells
• Always do pan-cytokeratin
– Multiple keratins may be needed
– Especially HMW keratins

27
Metaplastic Carcinoma Immunophenotype
• Keratin ~100%
• SMA 70-80%
• P63 50%
• EMA 10-20% (rare cells)
• S-100 protein 10%
• ER/PR/HER2 negative
Metaplastic Carcinoma
Key Points:
• More common than primary spindle cell sarcoma in breast!
• Significant subset shows myoepithelial differentiation
• <5% lymph node metastasis in predominantly metaplastic tumors
• Frequently aggressive behavior
• Suggested to be managed as sarcoma
Case 7
• 57 yo female with 5 cm right breast mass

28

29
Prior lesion in the same patient

30

31
Conclusions
• Always think first about common lesions
• Carcinoma
• Phyllodes tumor
• May need to use multiple IHC markers
• Do not overcommit on needle biopsies
• Clinical history/imaging features is crucial
Take Home Messages
• Always first consider the possibility of metaplastic (spindle cell) carcinoma or phyllodes tumor
• Clinicopathologic correlation is often crucial in the diagnosis
• Accurate diagnosis on the needle biopsy may be impossible