Embed Size (px)
Citation preview
8/16/2019 spiritua, impact.pdf
http://slidepdf.com/reader/full/spiritua-impactpdf 1/10
The impact of nurses’ spiritual health on theirattitudes toward spiritual care, professional
commitment, and caringYi-Chien Chiang, RN, PhDa , Hsiang-Chu n Lee, RN, MSNa , Tsung-Lan Chu, RN, MSNb ,
Chin-Yen Han, RN, PhDa , Ya-Chu Hsiao, RN, EdDa ,*a Department of Nursing, Chang Gung University of Science and Technology, Taiwan, ROC
b Department of Nursing, Chang Gung Memorial Hospital at Linkou, Taiwan, ROC
a r t i c l e i n f o
Article history:Received 2 July 2015Revised 30 October 2015Accepted 9 November 2015Available online 24 November2015
Keywords:Spiritual healthSpiritual careProfessional commitmentCaring Nurse
a b s t r a c t
Background: The personal spiritual health of nurses may play an important role inimproving their attitudes toward spiritual care and their professional commit-ment and caring capabilities.Purpose: The purpose of this study was to explore the impact of nurses’ personalspiritual health on their attitudes toward spiritual care, professional commit-ment, and caring.Methods: A total of 619 clinical nurses were included in this cross-sectional sur-vey. The measurements included the spiritual health scale-short form, the
spiritual care attitude scale, the nurses’ professional commitment scale, and thecaring behaviors scale. Structural equation modeling was used to establish as-sociations between the main research variables.Results: The hypothetical model provided a good t with the data. Nurses’ spiritualhealth had a positive effect on nurses’ professional commitment and caring.Nurses’ attitudes toward spiritual care could therefore mediate their personalspiritual health, professional commitment, and caring.Conclusions: The ndings indicated that nurses’ personal spiritual health is animportant value and belief system and can inuence their attitudes towardspiritual care, professional commitment, and caring.Cite this article: Chiang, Y.-C., Lee, H.-C., Chu, T.-L., Han, C.-Y., & Hsiao, Y.-C. (2016, JUNE). The impact of nurses’ spiritual health on their attitudes toward spiritual care, professional commitment, and caring.Nursing Outlook, 64(3), 215-224. http://dx.doi.org/10.1016/j.outlook.2015.11.012 .
Introduction
Nurses’ competence in providing spiritual care andcaring is recognized as an importantfactor in improving the quality of nursing care patients receive ( Koenig,King, & Carson, 2012). Hoover (2002) indicated that
spiritual care is one of the most signicant lessons tocultivate in nursing students as it inuences their car-ing capabilities. The better the spirituality of students,the better the caring behaviors that students demon-strate. Nurses are generally recognized as those whoprovide spiritual care and caring for patients in Taiwan.In their study, McSherry and Jamieson (2011) found that
* Corresponding author: Ya-Chu Hsiao, Department of Nursing, Chang Gung University of Science and Technology, No.261, Wenhua 1stRd., Guishan Dist., Taoyuan City 333 03, Taiwan (R.O.C.).
E-mail address: [email protected] (Y.-C. Hsiao).0029-6554/$ - see front matter 2015 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.outlook.2015.11.012
Available online at www.sciencedirect.com
N u r s O u t l o o k 6 4 ( 2 0 1 6 ) 2 1 5 e 2 2 4www.nursingoutlook.org

8/16/2019 spiritua, impact.pdf
http://slidepdf.com/reader/full/spiritua-impactpdf 2/10

8/16/2019 spiritua, impact.pdf
http://slidepdf.com/reader/full/spiritua-impactpdf 3/10
1. Nurses’ spiritual health is signicantly positivelyrelated to their attitudes toward spiritual care.
2. Nurses’ attitudes toward spiritual care are signif-icantly positively related to their professionalcommitment and caring.
3. Nurses’ spiritual health is directly correlated totheir professional commitment and caring.
4. Nurses’ spiritual health is indirectly correlated totheir professional commitment and caring throughtheir attitudes toward spiritual care.
Literature Review
The Relationship Between Nurses’ Spiritual Healthand Attitudes Toward Spiritual Care
Providing spiritual care for patients is one of themain professional behaviors of nursing professionals(Narayanasamy & Owens, 2001; Ross, 2006 ). In itscode of ethics, the Taiwan Nurses Association states that nursesshould respect the life, human dignity, and values of theindividual, aswell as theindividual’sspiritualbeliefs andcustoms ( Taiwan Nurse Association, 2012 ). Spiritual carein nursing is practice based and dened as the provisionof interventions by nurses to satisfy the spiritual needsof their patients. A positive attitude toward spiritualcareimplies that nurses are willing to communicate withpatients and recognize their spiritual concerns and thusprovide nursing interventions to help these patients deal
with such concerns. The spiritual interventions thatnursesprovide to patients can be categorized in differentways, includingtheprovision of resources forspiritualityand being therapeutically present. First, nurses can pro-vide spirituality resources to patients by, for example,providing religious materials to patients, supporting patients’ spiritual/religious activities (e.g., prayer),referring patients to spiritual counselors, or helping patients make healthy connections with their signi-cant others. Second, being therapeutically present forpatients may include being present, listening, caring,respecting, instilling hope in patients, or assisting pa-tients in determining the meaning of life ( Pesut, 2008;Strang, Strang, & Ternestedt, 2002; van Leeuwen,Tiesinga, Post, & Jochemsen, 2006 ).
Nurses’ attitudes toward spiritual care may berelated to their own spiritual health. For instance, vanLeeuwen et al. (2006) indicated that nurses’ ownvalues and spiritual health may impact their attitudestoward spiritual care. Factors that may prevent nursesfrom providing spiritual care to patients are, forexample, a lack of understanding of spirituality, whichmay be due to the low emphasis on spirituality innursing education, nurses’ personal beliefs regarding spirituality, and cultural factors. Of these, studies haveshown that nurses’ belief systems regarding spiritual-ity are the most important factor that affects theirwillingness to provide spiritual care to patients ( Ross,
1994). The essential components of nurses’ belief sys-tems regarding spirituality include an awareness of spirituality, an awareness of a higher power, and theability to search for the meaning of life. A nurse whohashigher spiritual awareness is more sensitiveand/orperceptive and is more reective regarding his or herown life experiences and meaning; thus, tending tond it easier to have a positive attitude toward theprovision of spiritual care to patients ( Chung, Wong, &Chan, 2007; Meyer, 2003; Miner-Williams, 2006 ).
The Impact of Nurses’ Attitudes Toward SpiritualCare on Professional Commitment and Caring
Professional commitment has been dened as theacceptance of andbelief in professionalgoals/valuesandthe willingness to be a professional expert ( Lachman,1986; Lu, Lin, Wu, Hsieh, & Chang, 2002). In nursing, acommitment to offering the best nursing care, promot-
ing the nursing profession, and a willingness to continuewith the job are the main themes of professionalcommitment ( Jafaragaee, Parvizy, Mehrdad, & Rai,2012; Lin, Wang, Li, & Huang, 2007; Young, 1984). Pro-fessional commitment is signicantly negatively corre-lated with nurses’ turnover intentions ( Wang et al.,2010). According to a recent large-scale survey conduct-ed by the International Council of Nurses, the retentionrate (33%) and levels of job satisfaction among Taiwa-nese nurses are lower than those of other countries(Teng, 2014).
The relationship between nurses’ professionalcommitment and their attitudes toward spiritual care
has not been satisfactorily researched. Wang et al.(2010) indicated that religious beliefs can signicantlyimpact professional commitment; for example, nurseswho hold Buddhist beliefs present higher levels of pro-fessional commitment than those with other religiousafliations. Nevertheless, the authors also highlightedthe fact thatexactlyhow religionand spirituality impactnurses’ professional commitment remains unknown,and future research on the subject is required. Theconrmation of a denite relationship between nurses’attitudes toward spiritual care and their professionalcommitment may be benecial in resolving theproblemof the nursing shortage in Taiwan as it could facilitatethe development an intervention program to improvenurses’ attitudes toward spiritual care.
“Caring” from a nursing perspective comprisesconsideration and sensitivity to patients’ problems, awillingness by nurses to provide patients with theirtime, a skillful and professional work style, high workmotivation, empathic communication skills to satisfypatients’ needs, knowledge and/or a willingness tolearn, and the provision of an individual approach topatient care ( Dyson, 1996). Both patients and nursesagree that caring is one of the most important valuesfor nursing professionals ( Papastavrou et al., 2012 ). In astudy that focused on cultivating caring capabilities innursing students, the researchers unexpectedly foundthat spiritual awareness may potentially be positively
N u r s O u t l o o k 6 4 ( 2 0 1 6 ) 2 1 5 e 2 2 4 217

8/16/2019 spiritua, impact.pdf
http://slidepdf.com/reader/full/spiritua-impactpdf 4/10
correlated with “caring” ( Hoover, 2002). Hoover (2002)indicated that students may learn caring skills byactively helping people who are suffering from spiri-tual problems. Such caring skills include guiding stu-dents to show concern for people’s different situationsand teaching them how to respect people and care forothers ( Hoover, 2002 ). This seems to imply that there isa positive relationship between caring and attitudestoward spiritual care; however, previous studies havenot provided sufcient evidence to conclude that thereis a true relationship between these two concepts.
Methods
Study Design
A cross-sectional survey design was employed for
this study. The data were obtained from a large-scalestudy, the Survey of Religion, Spirituality, and Nursing (SRSN), which aimed to explore the religions, spiritual-ity, and nursing care among Taiwanese nurses. Theoriginal SRSN study included three stages. The rststage comprised a qualitative study that focused onexploring the nurses’ experiences of spirituality andreligion; the second stage consisted of the developmentof a scale for the measurement of spiritual-relatedvariables; and the third stage, a quantitative study,explored the relationships between the nurses’ spiri-tuality and related factors. The data were collectedfrom May 2011 to February 2012. This article only pre-
sents the results of the examination of the associationbetween spiritual health, spiritual care, professionalcommitment, and caring.
Participants
A convenience sample of nurses was obtained fromthree teaching hospitals in Taiwan. Nurses who satis-ed the following criteria were recruited for the study:(a) provide spiritual care for patients during their work,(b) full-time nurse, (c) over 6 months of nursing workexperience, and (d) agreement to complete the ques-tionnaires. The exclusion criteria for this study werenurses who were working in outpatient clinics andoperating rooms because such nursing professionalshave limitations in the provision of spiritual care topatients.
We tested the proposed hypotheses of this studyusing structural equation modeling (SEM). The samplesize estimation was conducted based on the root meansquare error of approximation (RMSEA), type I error rate(a ), type II error rate (1-power), and degree of freedom of the proposed model suggested by MacCallum, Browne,and Sugawara (1996) . Given that the null hypothesis(H0 ) of RMSEA 0.05, the alternative hypothesis (H 1 ) of RMSEA ¼ 0.02, the degree of freedom of the proposedmodel ¼ 109, a ¼ 0.01, and 1-power ¼ 0.99, the resultwas a minimum required sample size of 438
participants. Subsequently, 690 participants wereapproached, but 71 of these participants declined or didnot complete the questionnaires. Finally, a total of 619nurses completed the questionnaires, indicating acompletion rate of 89.71%.
Instruments
The questionnaires that were used in this studycovered spiritual health, spiritual care, professionalcommitment, caring, and sociodemographic informa-tion. All the questionnaires were developed in Chineseand were completed by Chinese-speaking participants.
Spiritual HealthFor the purposes of this study, spiritual health wasdened as an individual’s inner forces and resourcesthat allow them to develop a unique meaning of theself that is reected through their connections with the
self, others, and a higher being ( Hsiao & Huang, 2005 ).This study adopted the spiritual health scale-shortform (SHS-short form) developed by Hsiao, Chiang,Lee, and Han (2013), which had sound validity andreliability. The instrument is comprised of 24 items andis categorized into ve subscales, namely a connectionto others, meaning derived from living, transcendence,religious attachment, and self-understanding ( Hsiaoet al., 2013). The SHS-short form was designed as aLikert rating scale, and participants are asked torespond to each item with responses ranging from“strongly agree” (ve points) to “strongly disagree” (onepoint). A higher score indicates better spiritual health.
In this study, the Cronbach’s alpha of the SHS-shortform was 0.93.
Spiritual CareA positive attitude by nurses toward spiritual care isdened as an attitude in which nurses may be willing to communicate with patients to determine theirspiritual concerns and are then prepared to providenursing interventions to help these patients deal withsuch concerns. The spiritual care attitude scale (SCAS)developed by Chiang et al. (2014) was used to measurespiritual care in this study. The 15-item SCAS wasbased on in-depth interviews and literature reviews,which were used to initiate item development. Itcomprises three factors, namely, spiritual growth, coreconcepts, and spiritual nursing, explaining 71.06% of the total variance. The construct validity of the SCASwas established using conrmatory factor analysis,and the results indicated that the SCAS had acceptablemodel t indices. The Cronbach’s alpha of the SCASwas 0.94. In the SCAS, participants respond to eachitem using a ve-point Likert-type scale, for which theanswers range from “strongly agree” (ve points) to“strongly disagree” (one point).
Professional CommitmentProfessional commitment has been dened as theacceptance of and belief in professional goals/values
N u r s O u t l o o k 6 4 ( 2 0 1 6 ) 2 1 5 e 2 2 4218

8/16/2019 spiritua, impact.pdf
http://slidepdf.com/reader/full/spiritua-impactpdf 5/10
and the willingness to be a professional expert(Lachman, 1986; Lu et al., 2002 ). The nurses’ profes-sional commitmentscale (NPCS), which wasdevelopedby Lin et al. (2007), was used for this study. The NPCSconsists of three factors with 19 items: nursing pro-fessional compliance (nine items), involvement of nursing professionals (seven items), and retention of nursing professionals (three items). Each item’sdiscriminate power is > 0.9, which indicates that theitem has a higher correction within its own domainthan other domains. The internal consistency reli-ability of this scale was assessed by Cronbach’s alphacoefcient, and the value was 0.91. The 2-week intervaltest/retest reliability of the total scale was 0.91. Thesedata implied that the validity and reliability of theNPCS were acceptable. The NPCS measures each itemon a ve-point Likert scale rating from ve (stronglyagree) to one (strongly disagree). The total score canrange from 19 to 95, and a higher score signies higher
nursing professional commitment. In this study, theCronbach’s coefcient level of the NPCS was 0.90.
CaringIn this study, caring was dened as nurses’ behaviorsexpressing unconditional acceptance and empathytoward patients. The caring behaviors scale (CBS) wasconstructed and validated in a nursing student popu-lation by Lin (2001). The originally CBS comprised 56items and was divided into Form A and Form B (eachform consisting of 28 items) to measure caring behav-iors. Form B of the CBS was used to measure the nurses’caring levels in this study.
The scale measures caring behaviors according tothree factors, namely “helping patient through theillness trajectory,” “patient advocacy,” and “knowing the patient.” The CBS in the original study comprised56 items, which explained 67.4% of the total variance.The internal consistency reliability of this scale wasassessed by Cronbach’s alpha coefcient and split-half reliability, and the values were 0.98 and 0.96, respec-tively (Lin, 2001). Participants responded to eachstatement using a four-point Likert-type scale to pre-sent the frequency of caring behavior (0 ¼ never, 1 ¼sometimes, 2 ¼ usually, 3 ¼ always). The Cronbach’scoefcient level of the CBS was 0.97 in this study.
Sociodemographic InformationTo determine the participants’ sociodemographic in-formation, we collected demographic data pertaining to the participants’ sex, age, marital status, educationalstatus, and nursing work experience.
Ethical Considerations
To ensure all the participants’ rights were protected,this study was approved by the hospital’s researchethics committee. Each participant received verbal andwritten explanations about the study from one of theresearchers. After each participant’s written consentwas obtained, they were provided with a pack of
questionnaires to complete anonymously. It was esti-mated that each participant would need about 30 minto complete all the questionnaires. Finally, the partic-ipants were instructed to individually place theirquestionnaires in a sealed research box located at theirnursing stations.
Statistics
The proposed hypotheses in this study were tested bySEM performed using AMOS 7.0 (SPSS Inc., Chicago, IL).In contrast to traditional statistical methods (i.e.,regression analysis), SEM determines measurementerrors in the observational variables (the subscalesafter parceling) and estimates all the regression co-efcients (paths) simultaneously, which results in amore precise parameter estimation than that providedby traditional methods ( Hair, Black, Babin, Anderson, &Tatham, 2006 ). In this study, each SEM consisted of a
measurement model and a structural model. The cor-relation between the observational variables and theirassociated latent variable (the scale) was estimated inthe measurement model. In contrast, the associationbetween the latent variables was estimated in thestructural model.
The goodness t of SEM was assessed using absolutet indices, relative t indices, and parsimony t indices(Hair et al., 2006 ). The absolute t indices included thegoodness of t index (GFI), the adjusted GFI index(AGFI), the standardized root mean squared residual(SRMR), and the RMSEA. The relative t indices wereassessed using the normed t index (NFI), the non-NFI
(NNFI), and the comparative t index (CFI). Finally, theparsimony t indices were considered using theparsimony NFI (PNFI), the parsimony CFI (PCFI), andthe likelihood ratio ( c 2 /df ). The acceptable threshold of SRMR and RMSEA was< 0.80, that of PNFI and PGFI was> 0.50, that of c 2 /df was < 5, and that of the rest of theindices was > 0.90 (Schumacker & Lomax, 2004 ).
The internal quality of the measurement model wasfurtherveried by standardized factor loading (valuesof 0.50 or higher indicated acceptable), average varianceextraction (AVE; values of 0.50 or higher indicatedacceptable),and convergent reliability (CR; valuesof 0.70or higher indicated acceptable; Fornell & Larcker, 1981).
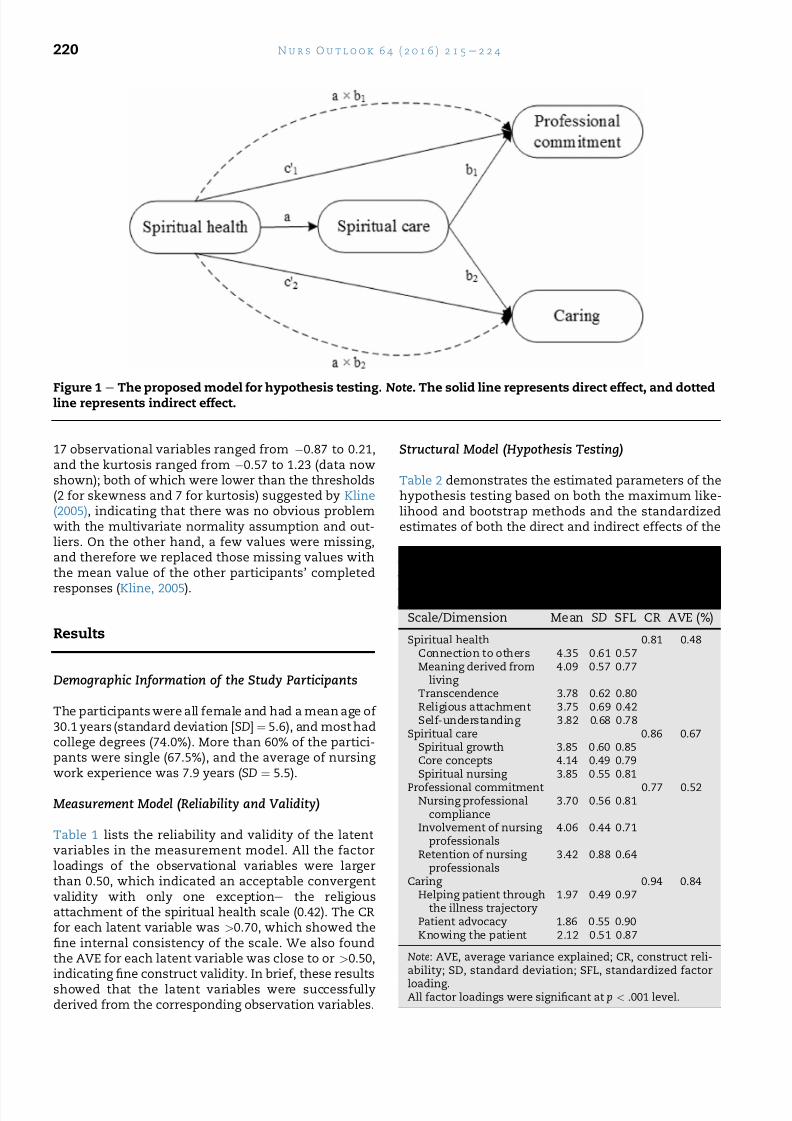
The structural model provided the estimated pa-rameters related to the proposed hypotheses and con-sisted of directand indirect effects ( Figure 1 ). Noticeably,the indirect effects involved the hypothesis of media-tion and were testedby both the conventional Sobel test(Sobel, 1987) and the bootstrap method ( Cheung & Lau,2008; Shrout & Bolger, 2002). A total of 1,000 boot-strapped samples were generated, and point estimatesand 95% bias-corrected and accelerated condence in-tervals for both the direct (a, b, c) and indirect (a b)effects were calculated. The mediated effect was veri-ed when the bootstrapped 95% condence intervals of the indirect effects did not include zero.
There is an underlying assumption of multivariatenormality when performing SEM. The skewness of the
N u r s O u t l o o k 6 4 ( 2 0 1 6 ) 2 1 5 e 2 2 4 219
8/16/2019 spiritua, impact.pdf
http://slidepdf.com/reader/full/spiritua-impactpdf 6/10
17 observational variables ranged from 0.87 to 0.21,and the kurtosis ranged from 0.57 to 1.23 (data nowshown); both of which were lower than the thresholds(2 for skewness and 7 for kurtosis) suggested by Kline(2005), indicating that there was no obvious problemwith the multivariate normality assumption and out-liers. On the other hand, a few values were missing,and therefore we replaced those missing values withthe mean value of the other participants’ completed
responses ( Kline, 2005).
Results
Demographic Information of the Study Participants
The participants were all female and had a mean age of 30.1 years (standard deviation [ SD] ¼ 5.6), and most hadcollege degrees (74.0%). More than 60% of the partici-pants were single (67.5%), and the average of nursing work experience was 7.9 years ( SD ¼ 5.5).
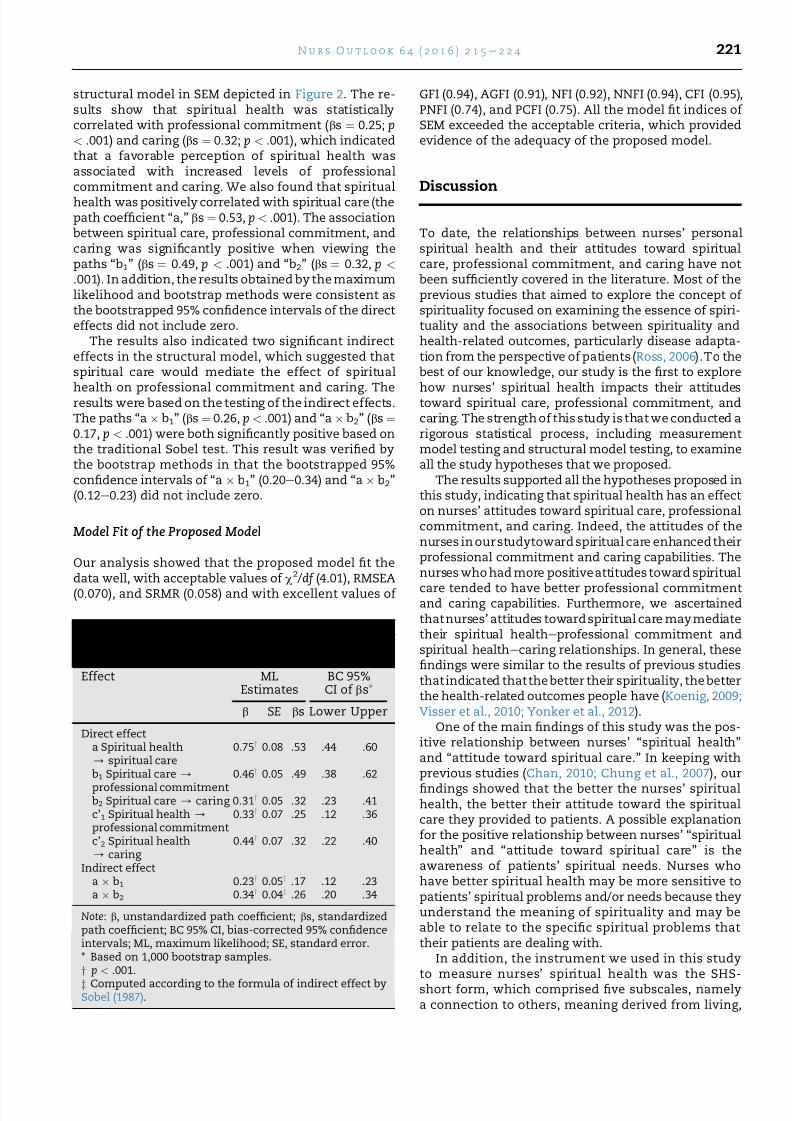
Measurement Model (Reliability and Validity)
Table 1 lists the reliability and validity of the latentvariables in the measurement model. All the factorloadings of the observational variables were largerthan 0.50, which indicated an acceptable convergentvalidity with only one exception e the religiousattachment of the spiritual health scale (0.42). The CRfor each latent variable was > 0.70, which showed thene internal consistency of the scale. We also foundthe AVE for each latent variable was close to or > 0.50,indicating ne construct validity. In brief, these resultsshowed that the latent variables were successfullyderived from the corresponding observation variables.
Structural Model (Hypothesis Testing)
Table 2 demonstrates the estimated parameters of thehypothesis testing based on both the maximum like-lihood and bootstrap methods and the standardizedestimates of both the direct and indirect effects of the
Figure 1e
The proposed model for hypothesis testing. Note . The solid line represents direct effect, and dottedline represents indirect effect.
Table 1 e The Descriptive Statistics for theObservational Variables and Convergent
Reliability and Validity for the Latent Variables inthe Measurement Model ( N [ 619)Scale/Dimension Mean SD SFL CR AVE (%)
Spiritual health 0.81 0.48Connection to others 4.35 0.61 0.57Meaning derived from
living 4.09 0.57 0.77
Transcendence 3.78 0.62 0.80Religious attachment 3.75 0.69 0.42Self-understanding 3.82 0.68 0.78
Spiritual care 0.86 0.67Spiritual growth 3.85 0.60 0.85Core concepts 4.14 0.49 0.79Spiritual nursing 3.85 0.55 0.81
Professional commitment 0.77 0.52Nursing professional
compliance3.70 0.56 0.81
Involvement of nursing professionals
4.06 0.44 0.71
Retention of nursing professionals
3.42 0.88 0.64
Caring 0.94 0.84Helping patient through
the illness trajectory1.97 0.49 0.97
Patient advocacy 1.86 0.55 0.90Knowing the patient 2.12 0.51 0.87
Note: AVE, average variance explained; CR, construct reli-ability; SD, standard deviation; SFL, standardized factorloading.All factor loadings were signicant at p < .001 level.
N u r s O u t l o o k 6 4 ( 2 0 1 6 ) 2 1 5 e 2 2 4220
8/16/2019 spiritua, impact.pdf
http://slidepdf.com/reader/full/spiritua-impactpdf 7/10
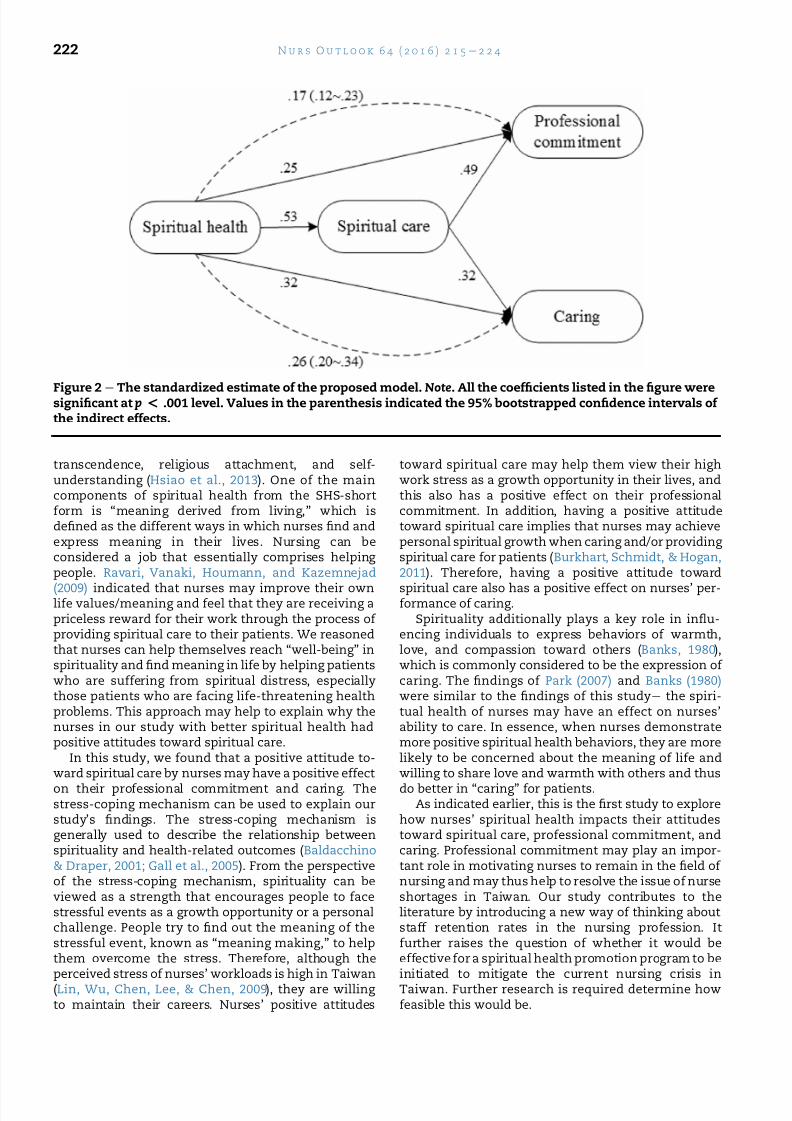
structural model in SEM depicted in Figure 2. The re-sults show that spiritual health was statisticallycorrelated with professional commitment ( bs ¼ 0.25; p< .001) and caring ( bs ¼ 0.32; p < .001), which indicatedthat a favorable perception of spiritual health wasassociated with increased levels of professionalcommitment and caring. We also found that spiritualhealth was positively correlated with spiritual care (thepath coefcient “a,” bs ¼ 0.53, p < .001). The associationbetween spiritual care, professional commitment, andcaring was signicantly positive when viewing thepaths “b 1 ” (bs ¼ 0.49, p < .001) and “b2 ” (bs ¼ 0.32, p <
.001). In addition, the results obtained by the maximumlikelihood and bootstrap methods were consistent asthe bootstrapped 95% condence intervals of the directeffects did not include zero.
The results also indicated two signicant indirecteffects in the structural model, which suggested thatspiritual care would mediate the effect of spiritual
health on professional commitment and caring. Theresults were based on the testing of the indirect effects.The paths “a b1 ” (bs ¼ 0.26, p < .001) and “a b2 ” (bs ¼0.17, p < .001) were both signicantly positive based onthe traditional Sobel test. This result was veried bythe bootstrap methods in that the bootstrapped 95%condence intervals of “a b1 ” (0.20e 0.34) and “a b2 ”(0.12e 0.23) did not include zero.
Model Fit of the Proposed Model
Our analysis showed that the proposed model t thedata well, with acceptable values of c
2 /df (4.01), RMSEA(0.070), and SRMR (0.058) and with excellent values of
GFI (0.94), AGFI (0.91), NFI (0.92), NNFI (0.94), CFI (0.95),PNFI (0.74), and PCFI (0.75). All the model t indices of SEM exceeded the acceptable criteria, which providedevidence of the adequacy of the proposed model.
Discussion
To date, the relationships between nurses’ personalspiritual health and their attitudes toward spiritualcare, professional commitment, and caring have notbeen sufciently covered in the literature. Most of theprevious studies that aimed to explore the concept of spirituality focused on examining the essence of spiri-tuality and the associations between spirituality andhealth-related outcomes, particularly disease adapta-tion from the perspective of patients ( Ross, 2006).To thebest of our knowledge, our study is the rst to explore
how nurses’ spiritual health impacts their attitudestoward spiritual care, professional commitment, andcaring. The strength of this study is that we conducted arigorous statistical process, including measurementmodel testing and structural model testing, to examineall the study hypotheses that we proposed.
The results supported all the hypotheses proposed inthis study, indicating that spiritual health has an effecton nurses’ attitudes toward spiritual care, professionalcommitment, and caring. Indeed, the attitudes of thenurses in ourstudytoward spiritual care enhancedtheirprofessional commitment and caring capabilities. Thenurses who had more positiveattitudes toward spiritual
care tended to have better professional commitmentand caring capabilities. Furthermore, we ascertainedthatnurses’ attitudes towardspiritual care maymediatetheir spiritual health e professional commitment andspiritual health e caring relationships. In general, thesendings were similar to the results of previous studiesthatindicated thatthe better their spirituality, the betterthe health-related outcomes people have ( Koenig, 2009;Visser et al., 2010; Yonker et al., 2012 ).
One of the main ndings of this study was the pos-itive relationship between nurses’ “spiritual health”and “attitude toward spiritual care.” In keeping withprevious studies ( Chan, 2010; Chung et al., 2007 ), ourndings showed that the better the nurses’ spiritualhealth, the better their attitude toward the spiritualcare they provided to patients. A possible explanationfor the positive relationship between nurses’ “spiritualhealth” and “attitude toward spiritual care” is theawareness of patients’ spiritual needs. Nurses whohave better spiritual health may be more sensitive topatients’ spiritual problems and/or needs because theyunderstand the meaning of spirituality and may beable to relate to the specic spiritual problems thattheir patients are dealing with.
In addition, the instrument we used in this studyto measure nurses’ spiritual health was the SHS-short form, which comprised ve subscales, namelya connection to others, meaning derived from living,
Table 2 e Estimated Parameters of Standard MLand Bootstrapping Methods for the HypothesisTesting in the Structural Model ( N [ 619)Effect ML
EstimatesBC 95%CI of bs*
b SE bs Lower Upper
Direct effecta Spiritual health/ spiritual care
0.75y 0.08 .53 .44 .60
b1 Spiritual care /
professional commitment0.46y 0.05 .49 .38 .62
b2 Spiritual care / caring 0.31 y 0.05 .32 .23 .41c’1 Spiritual health /
professional commitment0.33y 0.07 .25 .12 .36
c’2 Spiritual health/ caring
0.44y 0.07 .32 .22 .40
Indirect effecta b1 0.23y 0.05z .17 .12 .23a b2 0.34y 0.04z .26 .20 .34
Note: b, unstandardized path coefcient; bs, standardizedpath coefcient; BC 95% CI, bias-corrected 95% condenceintervals; ML, maximum likelihood; SE, standard error.* Based on 1,000 bootstrap samples.y p < .001.z Computed according to the formula of indirect effect bySobel (1987).
N u r s O u t l o o k 6 4 ( 2 0 1 6 ) 2 1 5 e 2 2 4 221
8/16/2019 spiritua, impact.pdf
http://slidepdf.com/reader/full/spiritua-impactpdf 8/10
transcendence, religious attachment, and self-understanding ( Hsiao et al., 2013 ). One of the maincomponents of spiritual health from the SHS-shortform is “meaning derived from living,” which isdened as the different ways in which nurses nd andexpress meaning in their lives. Nursing can beconsidered a job that essentially comprises helping people. Ravari, Vanaki, Houmann, and Kazemnejad
(2009) indicated that nurses may improve their ownlife values/meaning and feel that they are receiving apriceless reward for their work through the process of providing spiritual care to their patients. We reasonedthat nurses can help themselves reach “well-being” inspirituality and nd meaning in life by helping patientswho are suffering from spiritual distress, especiallythose patients who are facing life-threatening healthproblems. This approach may help to explain why thenurses in our study with better spiritual health hadpositive attitudes toward spiritual care.
In this study, we found that a positive attitude to-ward spiritual care by nurses may have a positive effecton their professional commitment and caring. Thestress-coping mechanism can be used to explain ourstudy’s ndings. The stress-coping mechanism isgenerally used to describe the relationship betweenspirituality and health-related outcomes ( Baldacchino& Draper, 2001; Gall et al., 2005). From the perspectiveof the stress-coping mechanism, spirituality can beviewed as a strength that encourages people to facestressful events as a growth opportunity or a personalchallenge. People try to nd out the meaning of thestressful event, known as “meaning making,” to helpthem overcome the stress. Therefore, although theperceived stress of nurses’ workloads is high in Taiwan(Lin, Wu, Chen, Lee, & Chen, 2009), they are willing to maintain their careers. Nurses’ positive attitudes
toward spiritual care may help them view their highwork stress as a growth opportunity in their lives, andthis also has a positive effect on their professionalcommitment. In addition, having a positive attitudetoward spiritual care implies that nurses may achievepersonal spiritual growth when caring and/or providing spiritual care for patients ( Burkhart, Schmidt, & Hogan,2011). Therefore, having a positive attitude toward
spiritual care also has a positive effect on nurses’ per-formance of caring.Spirituality additionally plays a key role in inu-
encing individuals to express behaviors of warmth,love, and compassion toward others ( Banks, 1980),which is commonly considered to be the expression of caring. The ndings of Park (2007) and Banks (1980)were similar to the ndings of this study e the spiri-tual health of nurses may have an effect on nurses’ability to care. In essence, when nurses demonstratemore positive spiritual health behaviors, they are morelikely to be concerned about the meaning of life andwilling to share love and warmth with others and thusdo better in “caring” for patients.
As indicated earlier, this is the rst study to explorehow nurses’ spiritual health impacts their attitudestoward spiritual care, professional commitment, andcaring. Professional commitment may play an impor-tant role in motivating nurses to remain in the eld of nursing and may thus help to resolve the issue of nurseshortages in Taiwan. Our study contributes to theliterature by introducing a new way of thinking aboutstaff retention rates in the nursing profession. Itfurther raises the question of whether it would beeffective for a spiritual health promotion program to beinitiated to mitigate the current nursing crisis inTaiwan. Further research is required determine howfeasible this would be.
Figure 2e
The standardized estimate of the proposed model. Note . All the coefcients listed in the gure weresignicant at p < .001 level. Values in the parenthesis indicated the 95% bootstrapped condence intervals of the indirect effects.
N u r s O u t l o o k 6 4 ( 2 0 1 6 ) 2 1 5 e 2 2 4222

8/16/2019 spiritua, impact.pdf
http://slidepdf.com/reader/full/spiritua-impactpdf 9/10

8/16/2019 spiritua, impact.pdf
http://slidepdf.com/reader/full/spiritua-impactpdf 10/10
Koenig, H. G. (2009). Research on religion, spirituality, and mentalhealth: A review. Canadian Journal of Psychiatry. RevueCanadienne De Psychiatrie, 54 (5), 283e 291.
Lachman, R., & Aranya, N. (1986). Job attitudes and turnoverintentions among professionals in different work settings.Organizational Studies, 7 , 279e 293.
Lin, M. C., Wu, C. L., Chen, H. H., Lee, J. C., & Chen, F. S. (2009).Association between work characteristics and burnout among hospital staff in Taiwan. Journal of Healthcare Management,10(2), 93e 110.
Lin, C. J., Wang, H. C., Li, T. C., & Huang, L. C. (2007). Reliability andvalidity of nurses’ job satisfaction scale and nurses professionalcommitment. Mid-Taiwan Journal of Medicine, 12, 65e 75.
Lin, P. F. (2001). Development and psychometric evaluation of theCaring Behaviors Scale of baccalaureate nursing students in Taiwan(Doctoral Dissertation) . Boston: Boston College .
Liu, Y. J., & Wu, C.-S. (2008). Toward a holistic health care:advocating for hospital chaplain services. Taiwan Journal of Hospice Palliative Care, 13(1), 82e 100.
Lu, K., Lin, P., Wu, C., Hsieh, Y., & Chang, Y. (2002). Therelationships among turnover intentions, professionalcommitment, and job satisfaction of hospital nurses. Journal of
Professional Nursing, 18 (4), 214e
219.MacCallum, R. C., Browne, M. W., & Sugawara, H. M. (1996). Poweranalysis and determination of sample size for covariancestructure modeling. Psychological Methods, 1(2), 130e 149.
MacLaren, J. (2004). A kaleidoscope of understandings: Spiritualnursing in a multi-faith society. Journal of Advanced Nursing,45(5), 457e 462.
McSherry, W., & Jamieson, S. (2011). An online survey of nurses’perceptions of spirituality and spiritual care. Journal of ClinicalNursing, 20 (11/12), 1757e 1767.
Meyer, C. L. (2003). How effectively are nurse educators preparing students to provide spiritual care? Nurse Educator, 28 (4),185e 190.
Miner-Williams, D. (2006). Putting a puzzle together: Making spirituality meaningful for nursing using an evolving
theoretical framework. Journal of Clinical Nursing, 15(7), 811e 821.Ministry of the Interior. (2015). Statistics of religious temples,
Churches prole. Retrieved from http://www.moi.gov.tw/stat/week.aspx .
Narayanasamy, A., & Owens, J. (2001). A critical incident study of nurses’ responses to the spiritual needs of their patients. Journal of Advanced Nursing, 33 (4), 446e 455.
O’Brien, M. E. (2014). A middle-range theory of spiritual well-being in illness. InO’Brien, M. E. (Ed.). (2014). Spirituality in nursing:Standing on holly ground, (Vol. 5) . Burlington, MA: Jones &Bartlett Learning .
Papastavrou, E., Efstathiou, G., Tsangari, H., Suhonen, R., Leino-Kilpi, H., Patiraki, E., & . , Merkouris, A. (2012). A cross-culturalstudy of the concept of caring through behaviours: Patients’
and nurses’ perspectives in six different EU countries. Journalof Advanced Nursing, 68 (5), 1026e 1037.
Park, C. L. (2007). Religiousness/spirituality and health: Ameaning systems perspective. Journal of Behavioral Medicine,30(4), 319e 328.
Pesut, B. (2008). Spirituality and spiritual care in nursing fundamentals textbooks. The Journal Of Nursing Education,47(4), 167e 173.
Ravari, A., Vanaki, Z., Houmann, H., & Kazemnejad, A. (2009).Spiritual job satisfaction in an Iranian nursing context.Nursing Ethics, 16 (1), 19e 30.
Ross, L. (2006). Spiritual care in nursing: An overview of theresearch to date. Journal of Clinical Nursing, 15(7), 852e 862.
Ross, L. A. (1994). Spiritual aspects of nursing. Journal of AdvancedNursing, 19 (3), 439e 447.
Schumacker, R. E., & Lomax, R. G. (2004). A beginner’s guide tostructural equation modeling, (Vol. 2) . Mahwah, NJ: LawrenceErlbaum Associates .
Shrout, P. E., & Bolger, N. (2002). Mediation in experimental andnonexperimental studies: New procedures andrecommendations. Psychological Methods, 7(4), 422e 445.
Sobel, M. E. (1987). Direct and indirect effects in linear structural
equation models. Sociological Methods and Research, 16(1),155e 176.Strang, S., Strang, P., & Ternestedt, B. (2002). Spiritual needs as
dened by Swedish nursing staff. Journal of Clinical Nursing,11(1), 48e 57.
Taiwan Nurse Association. (2012). Code of ethics. Retrieved fromhttp://www.ngo.e-twna.org.tw/nursing_policy_1.php .
Teng, S. W. (2014). Nursing manpower and solutions in Taiwan.The Journal of Nursing, 61(2), 5e 12.
Tzeng, H., & Yin, C. (2006). Demands for religious care in theTaiwanese health system. Nursing Ethics, 13(2), 163e 179.
van Leeuwen, R., Tiesinga, L. J., Post, D., & Jochemsen, H. (2006).Spiritual care: Implications for nurses’ professionalresponsibility. Journal of Clinical Nursing, 15(7), 875e 884.
Visser, A., Garssen, B., & Vingerhoets, A. (2010). Spirituality and
well-being in cancer patients: A review. Psycho-Oncology,19(6), 565e 572.
Wang, K., Chou, C., & Huang, J. (2010). A study of work values,professional commitment, turnover intention and relatedfactors among clinical nurses. Journal of Nursing, 57(1), 22e 34.
Wu, H. F., & Hsiao, Y. C. (2009). A study of the correlation betweenthe spiritual health status and spiritual care abilities of nurses. Journal of Nursing and Healthcare Research, 5 (1), 68e 78.
Yonker, J. E., Schnabelrauch, C. A., & Dehaan, L. G. (2012). Therelationship between spirituality and religiosity onpsychological outcomes in adolescents and emerging adults:A meta-analytic review. Journal of Adolescence, 35(2), 299e 314.
Young, K. J. (1984). Professional commitment of women innursing. Western Journal of Nursing Research, 6 (1), 11e 26.
N u r s O u t l o o k 6 4 ( 2 0 1 6 ) 2 1 5 e 2 2 4224























![[Seyyed Hossein Nasr] Man and Nature the Spiritua(BookFi.org)](https://img.pdfslide.net/doc/110x75/55cf9ad7550346d033a3abc0/seyyed-hossein-nasr-man-and-nature-the-spirituabookfiorg.jpg)





