Embed Size (px)
Citation preview

Stabilisation of preterm infants with
intact umbilical cord
Ronny Knol
47th Annual Conference BVK
Brussels, March 21st 2019

Introduction

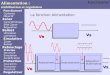
Modified from Rudolph AM. Congenital diseases of the heart. Chicago: Year Book Publishers; 1974, p. 1-48; and from Freed MD. Fetal
and transitional circulation. In: Fyler DC, editor. Nadas’ pediatric cardiology. Philadelphia: Mosby-Year Book; 1992. p. 57-61.
Introduction

Introduction

Delayed Cord Clamping in preterm infants:
More haemoglobin
Less hypotension
Less IVH
Less NEC

Fogarty et al. Am J Obstet Gynecol 2018

Introduction
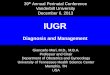
Van Vonderen et al. Neonatology 2014

Bhatt et al. J Physiol feb 2013
Introduction
Clamp Vent

Introduction
Bhatt et al. J Physiol feb 2013

Blank et al. ADC FN 2017



Duley et al. ADC FNN 2017

Duley et al. ADC FNN 2017

Katheria et al. J Pediatr 2016

Winter et al. Am J Perinatol 2016

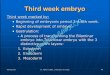
Aeration, breathing and then clamping Physiological based cord clamping

Physiological based cord clamping
Illustrations by Sophie Cramer, 2018

Physiological based cord clamping
Cord Clamping:
Spontaneous breathing with CPAP
Heart rate > 100 bpm
SpO2 > 90%
FiO2 < 0.4

Aeration, Breathing, Clamping
1. Feasibility study, single-center
2. Effectiveness study, 2 centers, non-inferiority
Randomised
3. (Inter)national multi-center randomised clinical trial

ABC1 study, feasibility
Brouwer et al. ADC FN 2018
Perinatal outcomes
All infants (n=37)
PBCC 33 (89.2)
Cord clamping time, min 4:23 [3:00 – 5:11]
Apgar score 1 min 7 [5 – 8]
Apgar score 5 min 8 [8 – 9]
Umbilical cord – pH 7.25 ± 0.10
Respiratory support at delivery
CPAP
PPV
Intubation
35 (94.6)
35 (94.6)
11 (29.7)
0
Maternal blood loss, ml 300 [200 – 475]
Temperature at admission, °C 36.0 ± 0.70
Hemoglobin < 24 h, mmol/l 11.18 ± 1.73

Aeration, Breathing, Clamping
1. Feasibility study, single-center
2. Effectiveness study, 2 centers, non-inferiority
Randomised
3. (Inter)national multi-center randomised clinical trial
Brouwer et al. ADC FN 2018
37 preterm infants

ABC2 study
• Randomised clinical trial, non-inferiority design
P: Preterm infants 24 - 31+6 weeks GA
I: Physiological Based Cord Clamping (PBCC)
C: Standard care (Time Based Cord Clamping, TBCC)
O: Time to stabilisation
• Definition of ‘stabilisation’:
Spontaneous breathing with CPAP, HR > 100/min, SpO2 > 90%, FiO2 < 40%.

Infant baseline characteristics
PBCC (n=19)
Control (n=17)
Gestational age, weeks 29.0 ± 1.8 29.2 ± 2.3
Birthweight, grams 1183 ± 270 1306 ± 437
Twins, infants 5 (26.3) 3 (17.6)
Antenatal steroids 19 (100%)
17 (100%)
Caesarean Section 9 (47.4) 9 (52.9)
PE/HELLP 3 (15.8) 2 (11.8)
Premature contractions 14 (73.7) 12 (70.6)
ABC2 study, results

Primary outcomes (intention-to-treat)
PBCC (n=19)
Control (n=17)
P value
Time to stabilisation (from birth)
5:54 ± 2:27 7:07 ± 2:54 0.18
Time to cord clamping
5:33 ± 2:24 1:02 ± 0:30 0.00
ABC2 study, results

Safety parameters (intention-to-treat)
PBCC (n=17)
Control (n=16)
P value
Postoperative infection (after CS) 0/9 0/8
Maternal blood loss, mL 300 [200-700] 450 [263-537] 0.557
PPH, >1000 mL 2 (11.8) 2 (12.5)
PBCC (n=19)
Control (n=17)
Infant temperature at admission 36.5 ± 0.9 36.7 ± 0.6 0.58
Infant temperature < 36.0 4 (23.5) 1 (5.9) 0.19
ABC2 study, results

Aeration, Breathing, Clamping
1. Feasibility study, single-center
2. Effectiveness study, 2 centers, non-inferiority
Randomised
3. (Inter)national multi-center randomised clinical trial
Brouwer et al. ADC FN 2018
37 preterm infants
36 preterm infants

Physiological based cord clamping
Cord Clamping:
Heart rate > 100 bpm
SpO2 > 85%
FiO2 < 0.4
Trial of CPAP before clamping

ABC3 study
• Multicenter randomised clinical trial (2 x 330 infants)
P: Preterm infants ≤ 29+6 weeks GA
I: Physiological Based Cord Clamping (PBCC)
C: Standard care (Time Based Cord Clamping, TBCC)
O: Survival without major cerebral injury (IVH≥2, PVL≥2, venous infarction) and/or
necrotizing enterocolitis (NEC≥2).

TAKE HOME
Stabilisation of preterm infants with intact umbilical cord may result in a
more stable cardiopulmonary transition.
Stabilisation of preterm infants with intact umbilical cord is feasible and
at least as effective as standard stabilisation.
Timing of cord clamping should be based on transitional physiology:
Physiological Based Cord Clamping
Need for more physiological and clinical data…

Aeration, Breathing, Clamping
Leiden University Medical Center:
Arjan te Pas
Frans Klumper
Thomas van den Akker
Emma Brouwer
Romy Berkhout
Enrico Lopriore
Amsterdam University Medical Center:
Anton van Kaam
Netherlands Neonatal Research Network (NNRN):
Wes Onland
Debbie Nuytemans
Erasmus Medical Center, Rotterdam:
Ronny Knol
Philip DeKoninck
Marijn Vermeulen
Nanda van Vliet
Irwin Reiss
Monash University, Melbourne, Australia:
Stuart Hooper
Graeme Polglase