Embed Size (px)
Citation preview

AACB Harmonisation Workshop13th July 2013
Dr Que LamAustin Pathology
Standardised Reporting of IronStudies
RCPA-AACB Critical LaboratoryResults Working Party

STANDARDISED REPORTING OFIRON STUDIES

But first some background ….
• Australian Iron Deficiency Expert Group• Common clinical misconceptions creating a barrier to the diagnosis &
management of IDA.
• Iron deficiency anaemia– is common– is associated with poor clinical outcomes– requires further investigation e.g. underlying malignancy.

†In an anaemic adult, a serum ferritin levelbelow 15ug/L is diagnostic of IDA and a levelbetween 15 and 30 ug/L is highly suggestive


Working Party

• http://www.rcpa.edu.au/Publications/IRONSTUDIES.htm
The College was asked by the National Blood Authority to develop a protocoldue to the difficulties being encountered in relation to the management ofpeople with iron deficiency and iron studies. The protocol, which has beendeveloped by a working party, is intended as an educational tool to assistpathologists in reporting of iron studies. It is now available to pathologists torefer to departments and organisations as required.

Pre-analytical• Serum (or heparinised plasma)• Fasting preferred• Iron studies are unreliable for several days after blood transfusion and the
ferritin level can remain elevated for 2-3 months after intravenous ironinfusion.
Numerical results
• Ferritin concentration (ug/L).• Iron concentration (umol/L).• Transferrin concentration (g/L).• Transferrin saturation is calculated from iron and transferrin results (%).
• There is no role for reporting Total Iron Binding Capacity (TIBC). (!!!)• The WP supports the reporting of transferrin instead of TIBC

Conclusions
Numerical results Conclusion
Serum ferritin concentrations withinreference interval in the absence ofclinical or laboratory evidence ofinflammation
No evidence of iron deficiency
Ferritin less than 20 ug/L in a pre-pubescent child or less than 30 ug/Lin an adult
Confirmed iron deficiency

010
2030
4050
6070
8090
100110
120130
140150
160170
180190
200
Ferritin
70
80
90
100
110
120
130
140135
Med
ian
Hb
OLD WOMEN
Courtesy: Dr Ken Sikaris

010
2030
4050
6070
8090
100110
120130
140150
160170
180190
200
Ferritin
60
65
70
75
80
85
90
95
100
Med
ian
MC
V
OLD WOMEN
Courtesy: Dr Ken Sikaris

010
2030
4050
6070
8090
100110
120130
140150
160170
180190
200
Ferritin
70
80
90
100
110
120
130
140
150
160
148M
edia
n H
b
ALL MEN
Courtesy: Dr Ken Sikaris

010
2030
4050
6070
8090
100110
120130
140150
160170
180190
200
Ferritin
65
70
75
80
85
90
95
Med
ian
MC
V
ALL MEN
Courtesy: Dr Ken Sikaris

-25.0%
-20.0%
-15.0%
-10.0%
-5.0%
0.0%
5.0%
10.0%
15.0%
0 50 100 150 200 250 300 350
ADVIA 2400ArchitectAU2700DxCModular
Courtesy: G.Koerbin
FERRITIN DIFFERENCE EQAP

0.0
100.0
200.0
300.0
400.0
500.0
600.0
0 100 200 300 400 500 600
Axis
Titl
e
Axis Title
ADVIA 2400ArchitectAU2700DxCModular
Courtesy: G.Koerbin
FERRITIN BIAS STUDY

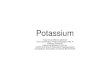
Serum ferritin (pooled specimens) by method
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50 60 70Mean Ferritin ug/L
Ferr
itin
ug/L
AbbottRocheBeckmanSiemensy=xQAP ALELQAP ALEH
While some recommendations in this document have been made based on specific numericalcut-offs it is acknowledged, especially in the case of ferritin measurement, that results will varybetween assays due to analytical differences. It is important for laboratories to assess andunderstand any biases of their assays before deciding to adopt these cut-offs or modify them.Serum-based correlations are preferred over the use of quality assurance/control material in any
assay correlations.

Conclusions
Numerical results Conclusion
Borderline ferritin concentration (20 – 60ug/L for pre-pubescent children and 30-100 ug/L for adults) with either anaemia,clinical history suggesting inflammatorydisease or positive laboratoryinflammatory markers
This result may indicate iron deficiency, asserum ferritin concentration can beelevated by inflammatory disease
Low serum iron with ferritin level withinreference interval and no clinical orlaboratory suggestion of inflammation
An isolated reduction in serum iron inisolation should never be reported as irondeficiency

Conclusions
Numerical results Conclusion
Elevated serum ferritinconcentration with transferrinsaturation less than or equal to 45%
This result may represent ironoverload, inflammation, organdamage (especially hepatic injury),malignancy or renal disease
Transferrin saturation greater than45% with or without elevated serumferritin concentration
Persistent elevations of transferrinsaturation may be the earliest sign ofiron overload

Conclusions
Numerical results Conclusion
Serum iron less than 55 umol/L, in aspecimen taken between 1 and 6hours post ingestion
Unlikely to cause serious iron toxicity
Serum iron of 55 – 310 umol/L insuspected acute iron poisoning
Clinically significant iron toxicity
Serum iron greater than 310 umol/Lin suspected acute iron poisoning
Severe iron poisoning likely to causeorgan damage

Conclusions
Numerical results Conclusion
Ferritin less than 30 ug/L in patientson therapeutic venesection
Low serum ferritin levels are thetarget of some therapeuticvenesection programmes
Elevated serum iron within 2 weeksor elevated ferritin within 2 monthsof intravenous iron fusion
Elevated levels probably reflecteffects of recent intravenous ironinfusion

Recommendations - examplesFerritin less than 30 ug/Lin a menstruating womanwith or without anaemia
During the reproductive years, irondeficiency in women is usually due tomultiparity or heavy menstrual losses.
Investigation of the gastro-intestinaltract for a source of blood loss may beindicated.
Ferritin less than 30 ug/Lin a man or post- menopausalwoman with anaemia
Iron deficiency in men and post-menopausal women suggestsabnormal blood loss. Gastro-intestinalevaluation for a source of blood lossshould be considered.Follow up serum iron, transferrin, andtransferrin saturation – are notnecessary.

Recommendations - examplesFerritin less than 20 ug/Lin a non-anaemicpre- pubescent child
In children this is usually due to either dietaryproblems or recent rapid growth and can causesignificant neuro- cognitive impairment (Sachdev,Gera and Nestel 2005). Follow up serum iron,transferrin, transferrin saturation, are notnecessary.
Recommend oral iron therapy for 6 weeks then re-check serum ferritin.
Ferritin less than 20 ug/Lin an anaemicpre- pubescent child
In children this is usually due to either dietaryproblems or recent rapid growth and can causesignificant neuro- cognitive impairment(Robertson and Tenenbein 2005). Follow up serumiron, transferrin, transferrin saturation, are notnecessary.
Recommend oral iron therapy for 3 months andthen re- check haemoglobin and serum ferritin.

Recommendations - examplesBorderline ferritin level(20 – 60 ug/L in a pre-pubescent child or 30-100 ug/L in an adult)with a clinical historysuggesting inflammatorydisease or an elevatedserum CRP
In view of inflammation (as demonstrated byhistory or CRP) the ferritin level is inconclusive.Repeat ferritin level when the inflammation hassubsided. Follow up serum iron, transferrin, andtransferrin saturation are not necessary.In some cases of known chronic illness where CRPis not elevated eg in the immuno-compromised,this concentration of serum ferritin is inconclusive.
Elevated ferritin levelwith less than or equalto 45% transferrinsaturation
Exclude ferritin elevation due to liver disease,renal impairment and inflammatory conditions.Where the cause is not known, recommendmonitoring serum ferritin every 3 to 6 months.Progressively increasing or very highconcentrations of serum ferritin warrant furtherinvestigation.

Please note that these recommendations andguidelines will not cover all cases. Conclusionsand recommendations should be based on allevidence available to the reporting pathologist,including past results, history and anyconsultations with the referring clinician.

RCPA-AACB CRITICAL LABORATORYRESULTS WORKING PARTY

Working Party• Rita Horvath• Craig Campbell• Andrew Georgiou• Penelope Coates• Robert Flatman• Grahame Caldwell• Hans Schneider• Que Lam

Clin Biochem Rev 2012, Vol 33; 149-160
• 2011 survey
• 58 responses
• 50 Aus, 6 NZ, 2 HK
• 48% public,
45% private

CK (Total) – 23/36 have critical upper limit.- 1000 (195 – 20000) U/L
Triglycerides, CRP – 10/35 laboratories have acritical upper limit.
Urea – 1/36 have a critical lower limit.
Troponin T – 9/21 have a critical upper limit.- 5/21 call through all results

Working Party Aims
1. Produce a guidance document withrecommendations for the process of criticallaboratory* results identification and notification.
1. Compile a “starter list” of critical tests and criticalvalues for laboratories to use as a basis for theirown list.
* Potential to apply to other pathology specialties.

Recommendations for theidentification and notification of
critical laboratory results
• Defining which critical results requirenotification
• Identifying critical results• Communicating critical results• Recording and Archiving communicated
critical results• Monitoring and update

Defining which critical results requirenotification
• Critical limit list• Upper and lower limits• Separate lists where appropriate for age, specialist wards, inpatient
or community setting etc.• consider delta limits• Avoid individualised limits for unique clinicians
• levels of urgency• timeframes for communication
• circumstances where notification is not necessary
• Sources: published literature (outcome studies & expert consensus)• consultation with relevant clinical groups using the laboratory.• Ready access to lists for clinicians.• Reviewed (3 years or as new information or technology arises)

Identifying critical results
• Automated flagging system
• Procedures for identifying and how to handle pre-analyticaland analytical errors.
• Where confirmatory/repeat testing to come, laboratoryshould consider notifying the preliminary result to allow theclinician time to prepare for intervention.

Communicating critical results (1)
• Define personnel responsible for delivering and receivingresults.
• Receiver– Clinician who ordered the test,– nominated delegate responsible for the patient,– someone the laboratory identifies as an appropriate person to
assume clinical responsibility for the patient.– As a last resort, the patient or carer should be contacted. (With
follow up with the requesting clinician at the next availableopportunity )
• An escalation algorithm
• Protocols should consider confidentiality.
• Up-to-date database of clinician contact details

Communicating critical results (2)• Definition of the acceptable modes of transmission for critical
results.
• Where there is automated delivery of critical results, the designshould include the recipients acknowledging receipt of result withina short predefined time period.
• If acknowledgement is not received, the laboratory must activatean alternative notification system to avoid harm due to delayedactions.
• Critical results only delivered verbally should be read back by therecipient
• Units and reference intervals must be read with the numericalresult.
• A non-communication policy for tests that have a guaranteeddefined response time and the result is available within that time.

Recording and archiving communicatedcritical results
• Communication must be recorded.– Patient– the critical result– recipient’s name (first name and surname preferable)– staff member who delivered the result– time and date of communication– Recorded in real time and be traceable in the LIS.– Explanation of any difficulties in meeting the requirements.
• For critical result only communicated verbally, whether the result wasread back by the recipient.
• For automated communication, acknowledgement of whether receiptof the result was obtained.

Monitoring and update
• Monitoring system – identify uncommunicated critical resultsfor later communication
• Quality indicators– % of critical results communicated and average times
taken.
• Auditing to identify any recurring difficulties & areas forimprovement.

G Lundberg, When to panic over an abnormal value. MLO 1972

ACTIONABLE TEST RESULTSPRIORITY 1 PRIORITY 2 PRIORITY 3
Clinical Description Life-threatening Urgent Important
Critically abnormal Significantlyabnormal
Abnormal
Time frame beforeescalation
Within 1 hour Within workinghours
Not time critical
e.g. K <3.0 mmol/L fT4 >30 pmol/L PSA> 50 ug/L firstresult
Neonatal vs. Paediatric vs. Adult vs. Pregnant patients.Disease/Conditions – dialysis, oncology, diabetic, haematologyPatient location – outpatient, ED,Pre-analytical – fasting and other patient preparations.Dynamic Tests e.g. Dexamethasone Suppression Test.

Hierarchy of Supporting Evidence forCritical Results.
Level 1 Clinical Health Outcome Studiese.g. Albumin, Sodium
Level 2 Observational Studye.g. Data mining with clinical outcome associations.
Level 3 Clinical Guidelines or Expert Consensuse.g. Thyroid in pregnancy
Level 4 State-of-the-art, current practice (laboratory or clinical)e.g. surveys
Level 5 Local consensus.

More work to do …
• Literature review.
• Ask laboratories for their critical resultsprocedures– Critical results list– Escalation policy
• Consult - laboratories, clinical groups.