Embed Size (px)
Citation preview
START NOW: Implementing and Evaluating a Cognitive Behavioral
Intervention for Offenders
Susan Sampl, PhDRobert L. Trestman, PhD, MDKirsten Shea, MBAMalini Varma, MAWalter Krauss, PsyDAmy Houde, MSW, LCSW
Correctional Managed Health CareUniversity of Connecticut Health CenterFarmington CT USA

OBJECTIVES1.Understand the theoretical and research background
of START NOW
2. Articulate recommendations for successfully implementing a structured cognitive behavioral intervention within corrections.
3. Identify methods and results of evaluating START NOW in correctional settings.
DISCLOSURE
• No financial Conflicts of Interest


Using SCID II with 508 inmates in Connecticut jails in an IRB approved National Institute of Justice Study:
(Trestman et al, 2007)
Personality Disorder Male (N=307)
Female (N=201)
Total (N=508)
Freq % Freq % Freq %
Paranoid 29 9.6 20 10.1 49 9.8
Borderline 39 12.9 45 23.2 84 16.9
Antisocial 120 39.5 53 27.0 173 34.6


• Participants: English-speaking women (n=18) and men (n=45)
• Results: Significant reduction in targeted behavior was found from baseline to following the16 week DBT-CM skills treatment groups. Both case management and DBT coaching were significant at 12month follow-up.
• Conclusions: The study supports the value of DBT-CM for management of aggressive behaviors in prison settings.

• PARTICIPANTS: 38 male adolescents• RESULTS: Significant changes were
found in physical aggression, distancing coping methods, and number of disciplinary tickets for behavior.
• CONCLUSION: The study supports the value of DBT-CM for the management of incarcerated male adolescents with difficult-to-manage aggressive behaviors.
CHALLENGES: TRANSITION FROM RESEARCH TO PRACTICE
• Costs of training• Staff turnover• Optimum language level• Costs and copyright issues

Background of START NOW:Research
• START NOW is an evidence-informed coping skills therapy designed to treat offenders with behavioral disorders and associated behavioral problems.
• START NOW grew out of National Institute of Justice funded research at the University of CT Health Center and the Connecticut DOC.
http://cmhc.uchc.edu/programs_services/startnow.aspx

Structure & Design of START NOW• 32 CBT/Coping Skills group sessions
• Clinical Tools– Participant workbooks
• 5th grade reading level• Gender specific• Spanish version available
– Facilitator manual• Highly structured, detailed• Basic scripts and examples provided
– Standardized protocol and tools for training and fidelity monitoring
Background of START NOW: Theory
• An integrative skills training model informed by a number of theoretical approaches & models-– Primarily a cognitive behavior therapy (CBT) model– Includes motivational interviewing principles &
practices to enhance motivation for change– Infused with elements of cognitive neuro-rehabilitation,
in consultation with correctional neuro-cognitive researcher, D. Fishbein (Fishbein et al., 2009).
– Theories of criminal behavior, including relevant examples in participant workbooks.

CBT for a Correctional Population • There is much support in the literature for the
use of CBT in the treatment of criminal conduct (Thigpen, 2007; Wilson, Bouffard, & Mackenzie, 2005).
• Several meta analyses support the use of CBT to reduce criminal recidivism (Pearson, Lipton, Cleland,
& Yee, 2002).
• Group oriented CBT was found to reduce criminal behavior 20-30% compared to control (Wilson, Bouffard, & Mackenzie, 2005).

CBT within START NOW • CBT procedures during group:
– Brainstorming– Role play– problem-solving– shaping of desired behaviors
• “Real life practice exercises” between group sessions
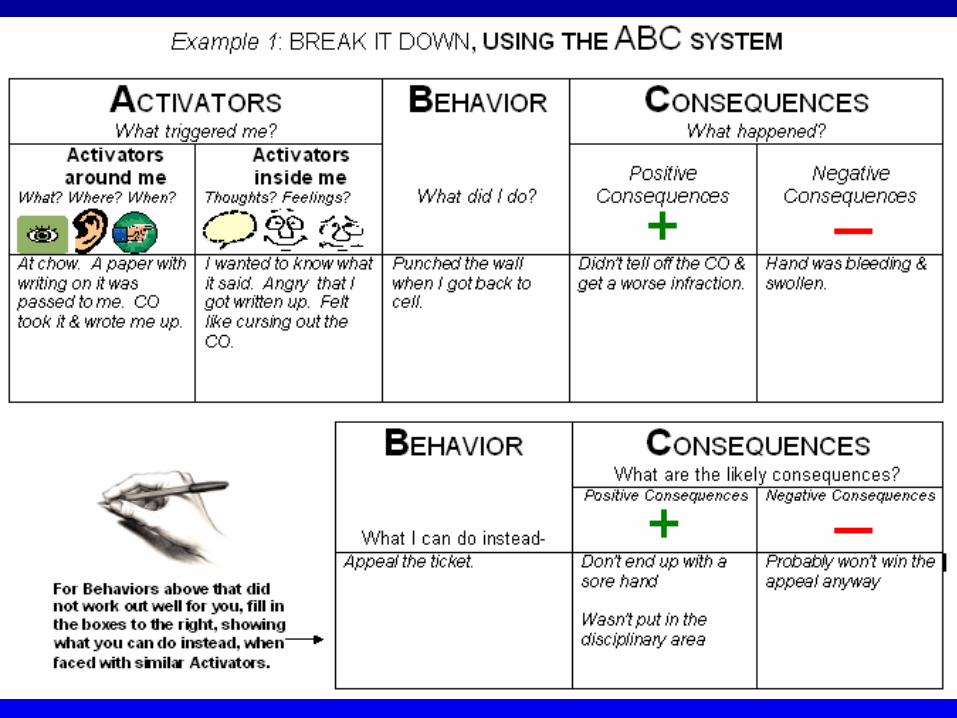
• “ABC System” for functional analysis of behavior
Incorporating Motivational Interviewing
• Focuses on developing motivation for change (Miller
& Rollnick, 2002), including changing criminal behavior (Chambers et al., 2008; Howells & Day, 2006).
• MI & CBT have been combined in other effective interventions (Dennis et al., 2004; Diamond et al., 2002; Steinberg et al., 2005).
• Research supports use of MI with offenders, resulting in improved addictions treatment compliance (Davis et al., 2003), reduced criminal attitude and substance related problems (Harper &
Hardy, 2000), reduced reconviction rates (Antiss,
Polascek & Wilson, 2011), and reduced DUI behaviors in adolescents (Stein et al., 2006).
Motivational Interviewing Influence on START NOW strategies:
• Emphasis on accepting ambivalence about change and “rolling with resistance”
• “Supporting self-efficacy” through focusing on strengths
• Many opportunities to elicit change talk & work through ambivalence are built into the START NOW clinical materials

Offender Focused Interventions Influence on START NOW strategies:
• Illustrative examples & coping behaviors are relevant to forensic situations
• Concepts & language are simplified given cognitive limitations of many offenders
• Numerous icons included in the participant workbook- especially useful with TBI or verbally limited participants
• Facilitator manual includes numerous tips for engaging difficult-to-engage participants: eg, shaping by reinforcing any movement toward the desired behavioral change.

Standard CBT Session Structure
• Introduce any new members & review group rules (5 min.)
• Review of real life practice exercise from previous session (10 – 15 min.)
• Practice Focusing or ABC Skills (10 – 15 min.)
• Rationale & overview of new coping skill (10 min.)• In-session practice exercise (15 min.)
• Assign new real life practice exercise (5 min.)
Unit 1- My Foundation: Starting with Me
• Focuses on developing increased self-control & ability to cope with stressors
• Includes setting a treatment goal, increasing wellness skills, accepting yourself & your situation, & enhancing your spirituality, values & personal boundaries.
Unit 2- My Emotions: Dealing with Upset Feelings
Includes:
• Recognizing & understanding emotions.
• Coping with emotions through actions, or through thoughts & imagery.
• Coping with depression, anger, anxiety & grief.
Unit 3- My Relationships: Connecting with Others
• Focuses on developing positive relationship skills including:– Listening skills– Assertiveness– Setting boundaries– Asking for support– Avoiding destructive
relationships– Responding to feedback– Coping with rejection

Unit 4- My Future:Setting & Meeting my Goals
• Focuses on preparing for a positive future by:– Developing hope– Setting realistic goals &
breaking them down into steps
– Learning problem solving skills
– Learning to set & meet educational & vocational goals

Developing & Maintaining Fidelity of Implementation
• Training, in absence of coaching, is insufficient. (National Implementation Research Network- Fixsen et al., 2005)
• Network of START NOW Trainers developed covering the entire CT DOC system
• START NOW Trainer Role:– Serve as local expert & point of communication– Provide centralized and local training– Observe groups for fidelity monitoring & coaching
Supporting the Sustainability of START NOW
• Enhanced by a standardized manual-guided intervention
• Results in reasonable cost of training to allow for staff turnover within corrections
• Requires a committed coordinating team, as well as an organized system to track provision of care

Creating an Information System

DATA!
• Repository for resources• Internal• External
• Program generated data• Outcome Measures• Methods to retrieve data/Reporting tools

http://cmhc.uchc.edu/programs_services/startnow.aspx

Program Generated Data
• Group Data• Attendance Data• Program Outcomes• Satisfaction Questionnaires

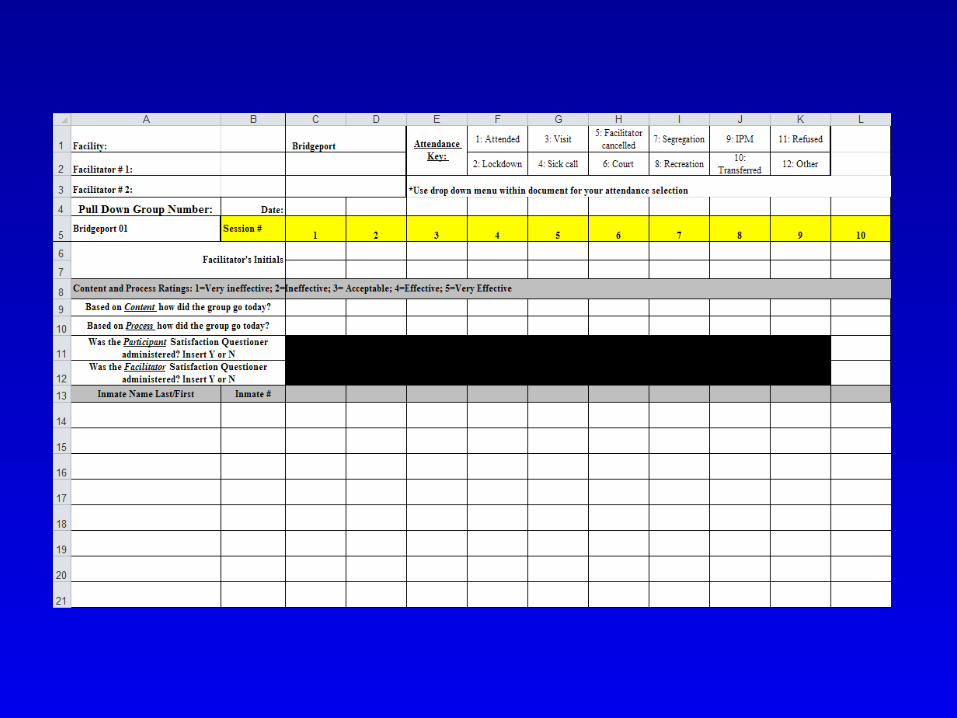

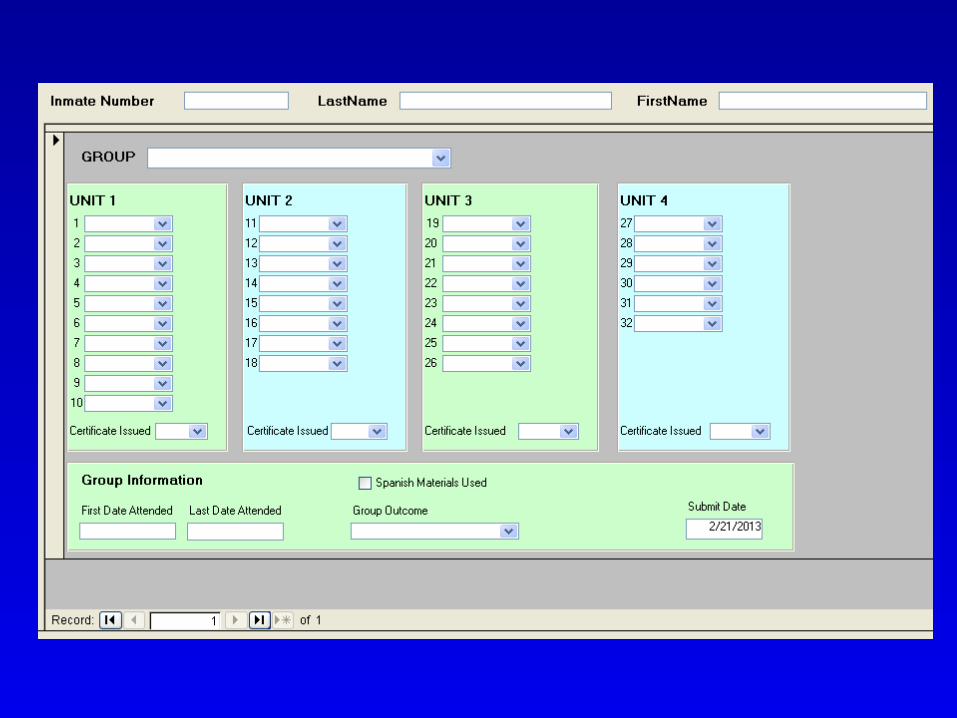
Building a data set
• Identifying information– Inmate name– Inmate number
• Start date of group• End date of group• Number of sessions completed
Outcome Measures
• Identify available data


Outcome Measures
• Identify available and relevant data pieces
• Disciplinary Tickets• Days spent as MH inpatient• Psychological measure assessment (computerized)
• Buss-Perry Aggression Questionnaire• Inventory of Interpersonal Problems• Barrett Impulsiveness Scale
Outcome Measures
• Target new measures• Self-injurious behaviors• Medication adherence• Crisis encounters per month• Recidivism
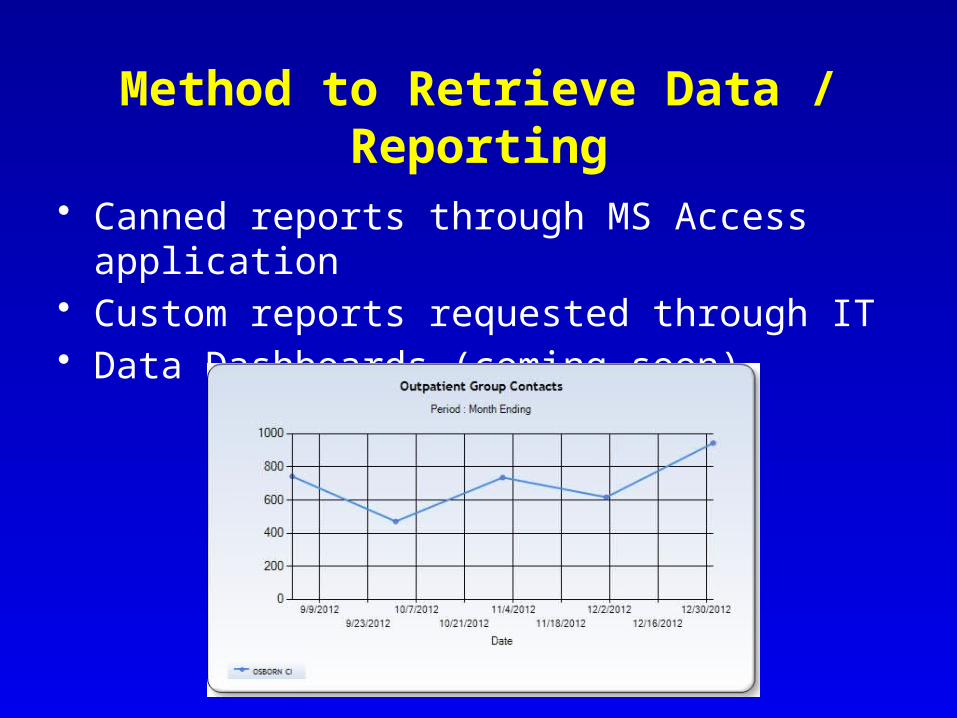
Method to Retrieve Data / Reporting
• Canned reports through MS Access application• Custom reports requested through IT• Data Dashboards (coming soon)
START NOW Program
• 13 CDOC facilities have active START NOW programs
• 57 clinicians are currently trained• 215 individuals are in active treatment
Data as of February 28, 2013

START NOW Participant Satisfaction
Data
Through December 2012

Satisfaction Survey Procedures
• N=619• 10 questions; 8 Likert Scale, 2 open-
ended• Completed at the end of every unit• Anonymous
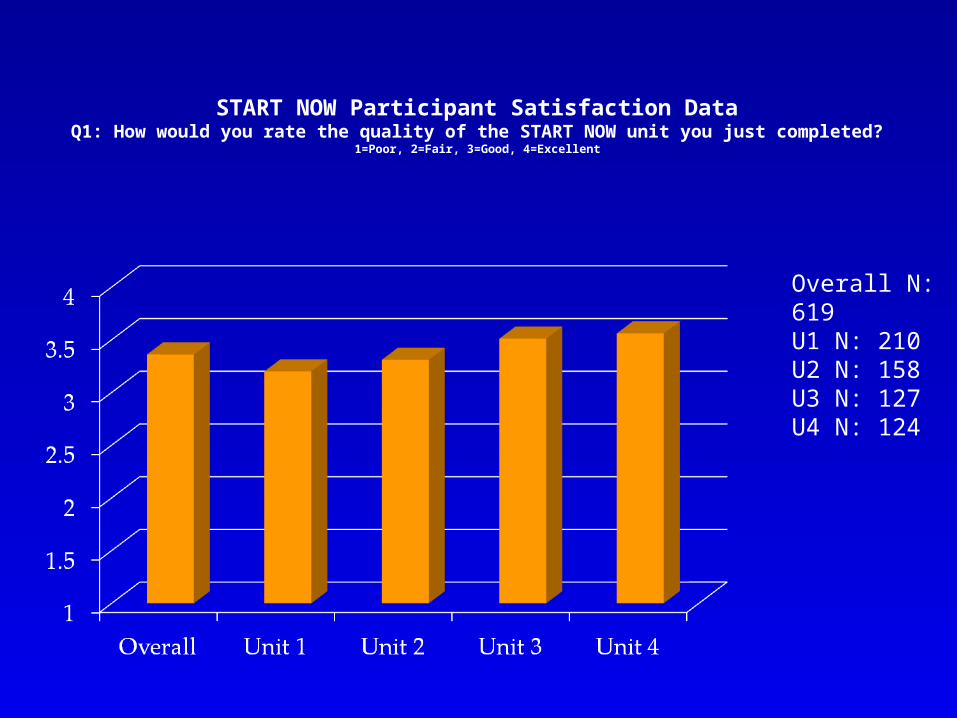
Overall N: 619U1 N: 210U2 N: 158U3 N: 127U4 N: 124
START NOW Participant Satisfaction DataQ1: How would you rate the quality of the START NOW unit you just completed?
1=Poor, 2=Fair, 3=Good, 4=Excellent

START NOW Participant Satisfaction DataQ5: How satisfied are you with the amount of help you have received?
1=Quite Dissatisfied, 2=Indifferent or mildly dissatisfied, 3=Mostly satisfied, 4=Very satisfied
Overall N: 619U1 N: 210U2 N: 158U3 N: 127U4 N: 124

START NOW Participant Satisfaction DataQ6: Has this START NOW unit helped you to deal more effectively with
your problems? 1=No, it seemed to make things worse, 2=No, it really didn’t help, 3=Yes, it helped, 4=Yes, it helped a great
deal
Overall N: 619U1 N: 210U2 N: 158U3 N: 127U4 N: 124
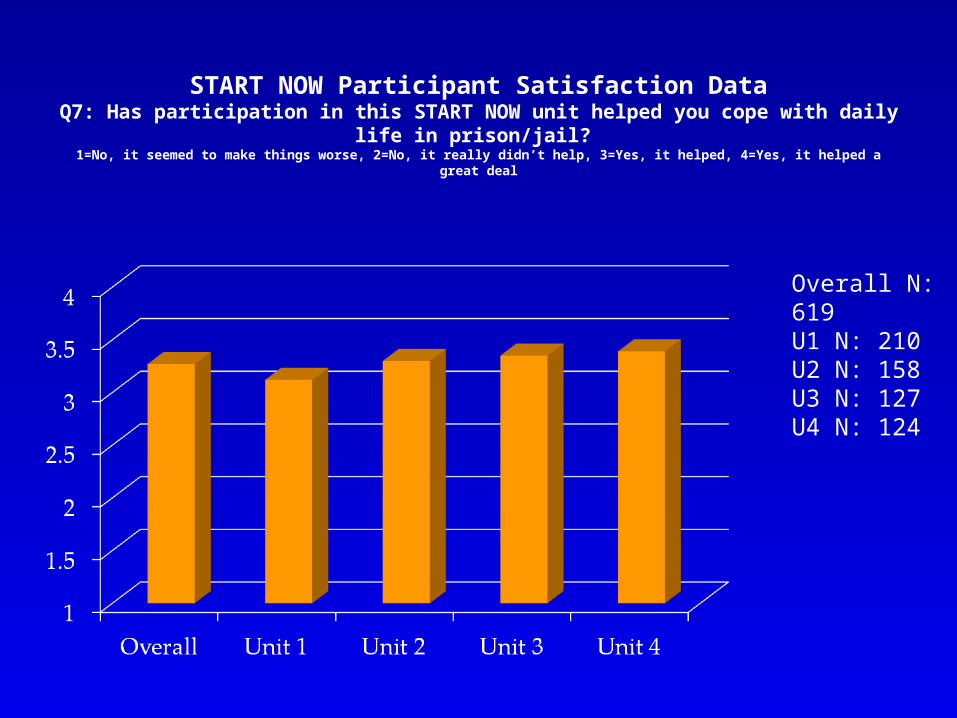
START NOW Participant Satisfaction DataQ7: Has participation in this START NOW unit helped you cope with
daily life in prison/jail? 1=No, it seemed to make things worse, 2=No, it really didn’t help, 3=Yes, it helped, 4=Yes, it helped a great
deal
Overall N: 619U1 N: 210U2 N: 158U3 N: 127U4 N: 124

Overall N: 619U1 N: 210U2 N: 158U3 N: 127U4 N: 124
START NOW Participant Satisfaction DataQ8: If you were to seek help again would you participate in this START NOW
unit? 1=No, definitely not, 2=No, I don’t think so, 3=Yes, I think so, 4=Yes, definitely
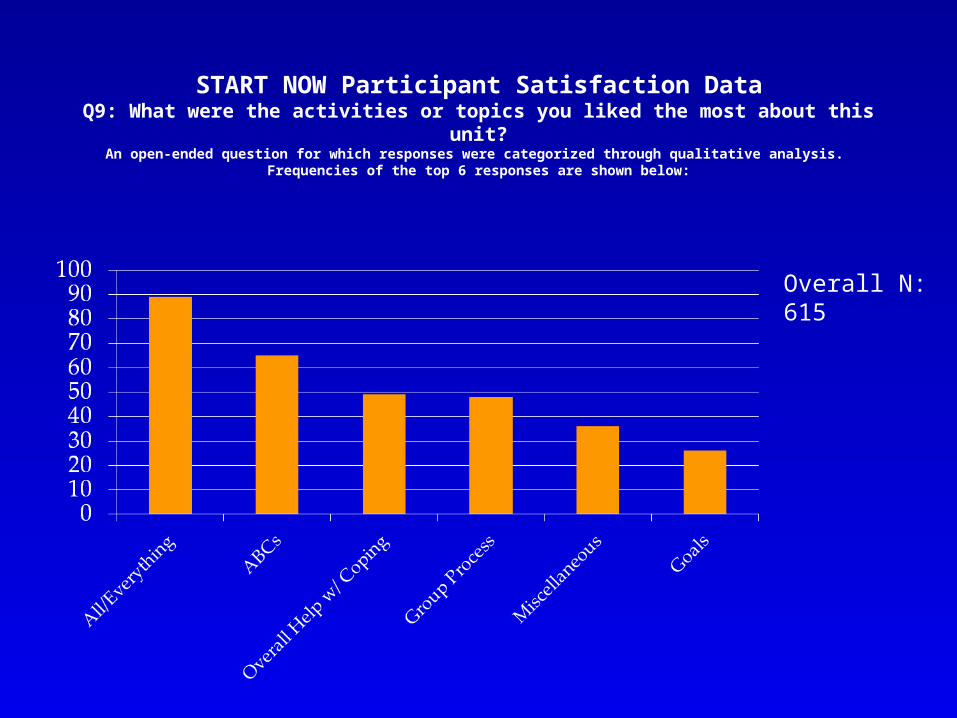
START NOW Participant Satisfaction DataQ9: What were the activities or topics you liked the most about this unit?
An open-ended question for which responses were categorized through qualitative analysis. Frequencies of the top 6 responses are shown below:
Overall N: 615
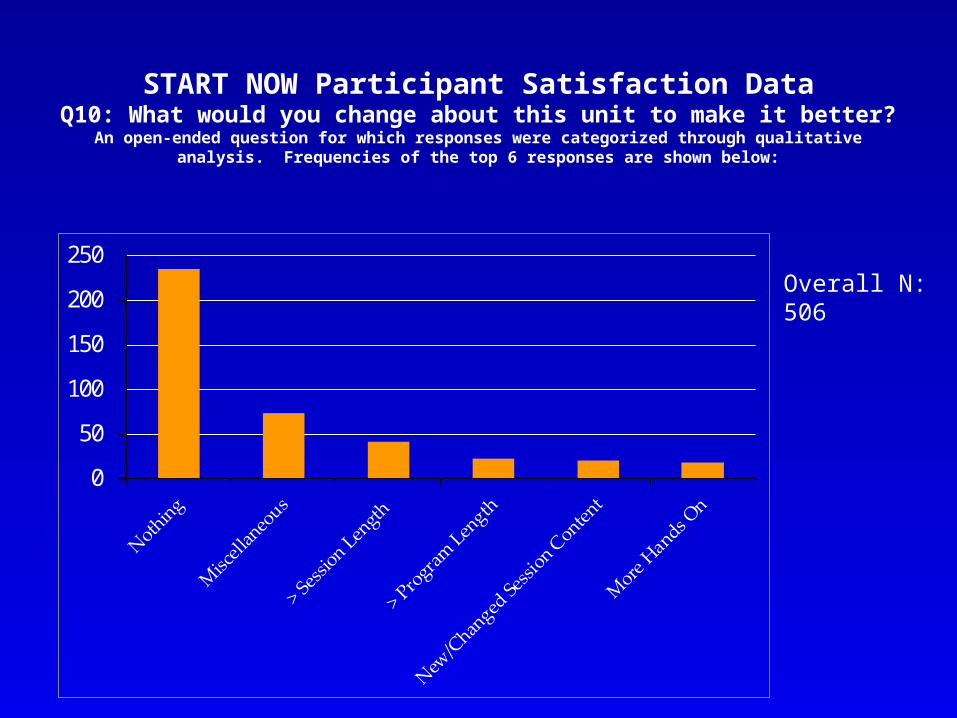
START NOW Participant Satisfaction DataQ10: What would you change about this unit to make it better?
An open-ended question for which responses were categorized through qualitative analysis. Frequencies of the top 6 responses are shown below:
0
50
100
150
200
250Overall N: 506

ADAPTATION of START NOW Alternative to Incarceration (AIC)
Program• DMHAS AIC program for Dually- Diagnosed SMI
clients (ASIST)• Significant effect for START NOW on reduced
re-incarceration (b=-.024, S.E.=0.008, p=0.003, OR=0.98); Cox regression, adjusted for illness severity
• Dose Response: Each START NOW session yields a 2.0% reduction in the odds of re-incarceration
• Frisman LK, Lin H, Rodis E, & Grzelak J. Final Report: Evaluation of the ASIST Program. CT Department of Mental Health & Addiction Services, internal document, 9/12/11
SUMMARY
• These interventions have a role to play in empowering individuals to gain greater control over their lives as they work toward recovery and effective integration into the community
• Implementation of evidence-based or evidence-informed treatment has many real world challenges that can be met both in institutional correctional and forensic settings