Embed Size (px)
Citation preview
GIRNARGUJARAT’S INTERIM REVIEW OF NOTEWORTHY
ACTIONS IN RESPONSE TO COVID-19
An Intra-Action Review
State Health System Resource Centre Gujarat
G U J A R A T

GIRNARGujarat’s Interim Review of Noteworthy
Actions in Response to COVID-19An Intra-Action Review
State Health System Resource Centre Gujarat
G U J A R A T
INDIAN INSTITUTE OF MANAGEMENT AHMEDABAD
Opp. Airforce Head Quarters, Nr. Lekawada Bus Stop, Lekawada CRPF P.O Gandhinagar , Gujarat India – 382042
State Health System Resource Centre Gujarat
World Health Organization Country Office - India R.K. Khanna Tennis Stadium, Africa Avenue, Safdarjung Enclave, New Delhi - 110029
First floor, NHM Bhavan, Civil hospital campus,Sector 12B, Gandhinagar - 382012. Gujarat
Vastrapur, Ahmedabad, Gujarat 380015
G U J A R A T
iii
List of abbreviations ............................................................................................................ v
Preface ............................................................................................................................... xi
Executive summary ......................................................................................................... xiii
Intra-action review lead team .............................................................................................xx
1. Intra-action review methodology ..................................................................... 1
2. COVID-19 and Gujarat .................................................................................... 3
3. Strategies, challenges and recommendations ................................................. 9
Pillar 1: Coordination, planning, and monitoring ..................................................... 9
Pillar 2: Risk communication & community engagement ................................... 13
Pillar 3: Surveillance, response, and containment ............................................... 18
Pillar 4: Points of entry capacities ......................................................................... 22
Pillar 5: Laboratory capacities and quality assurance .......................................... 24
Pillar 6: Infection prevention and control .............................................................. 27
Pillar 7: Case management & hospital preparedness .......................................... 30
Pillar 8: Operational support & logistics ................................................................ 35
Pillar 9: Research, innovation & knowledge sharing ............................................. 37
Pillar 10: Maintaining essential health services .....................................................41
4. Conclusions and way forward ....................................................................... 45
5. References .................................................................................................. 47
TABLE OF CONTENTS
iv
6. Annexures ................................................................................................... 48
Intra-action review support team ........................................................................... 48
Acknowledgements ...............................................................................................49
List of stakeholders ................................................................................................ 50
v
AEFI Adverse Event Following Immunization
AIIMS All India Institute of Medical Sciences
AMC Amdavad Municipal Corporation
ANM Auxiliary Nurse Midwife
AOP Association of Paediatricians
APMC Agriculture Produce Market Committee
ARI Acute Respiratory Infection
ART Anti-Retroviral Therapy
AS Aarogya Setu
ASHA Accredited Social Health Activist
AYUSH Ayurveda, Yoga & Naturopathy, Unani, Siddha and Homoeopathy
BJMC B. J. Medical College
BMJ British Medical Journal
BMW Bio-Medical Waste
CBNAAT Cartridge- Based Nucleic Acid Amplification Test
CCIC COVID-19 Community Isolation Centres
CCMC Certificate Course in Management of COVID-19
CCTV Closed-Circuit Television
CDGR Compound Daily Growth Rate
CDHO Chief District Health Officer
CEO Chief Executive Officer
CHCs Community Health Centres
LIST OF ABBREVIATIONS
vi
CHO Community Health Officers
CISF Central Industrial Security Force
CM Chief Minister
CMO Chief Minister’s Office
COO Chief Operating Officer
COVID-19 Coronavirus Disease
CoWIN Covid Vaccine Intelligence Work
CPO Chief Personnel Officer
CrPC Criminal Procedure Code
CSBC Centre for Social and Behaviour Change
CSO Civil Service Organizations
DG Director-General
DIKSHA Digital Infrastructure Knowledge Sharing
EMRI Emergency Management and Research Institute
e-OPD Electronic-Outpatient Department
FDCA Food and Drug Control Authority
FLW Front Line Worker
FOGSI Federation of Obstetrics and Gynaecological Societies of India
FW Family Welfare
GEM Government E-Marketplace
GIS Geographic Information System
GMERS Gujarat Medical Education & Research Society
GMSCL Gujarat Medical Services Corporation Limited
GoG Government of Gujarat
GoI Government of India
GSDP Gross State Domestic Product
GVK-EMRI Gunupati Venkata Krishna Reddy – Emergency Management and Research Institute
H&FWD Health and Family Welfare Department
HCW Health Care Workers
vii
HFNC High Flow Nasal Cannula
HFW Health & Family Welfare
HIV/AIDS Human Immunodeficiency Virus and Acquired Immune Deficiency Syndrome
HR Human Resource
HTP High Threat Pathogen
IAP Indian Academy of Paediatrics
IAR Intra-Action Review
I-CAD Infection Control Assist Device
ICD International Statistical Classification of Diseases and Related Health Problems
ICDS Integrated Child Development Services
ICMR Indian Council of Medical Research
ICU Intensive Care Unit
IDSP Integrated Disease Surveillance Program
IEC Institutional Ethics Committee
IFA Iron and Folic Acid
iGOT Integrated Government Online Training
IHBT Immuno Hematology & Blood Transfusion
IHIP Integrated Health Information Platform
IHR International Health Regulations
IIMA Indian Institute of Management Ahmedabad
IIPHG Indian Institute of Public Health Gandhinagar
ILI Influenza Like Illness
IMA Indian Medical Association
IPC Interpersonal Communication
IPC Infection Prevention and Control
IT Information Technology
ITIHAS Integrated Hotspot Analysis System
viii
LART Link Anti-Retroviral Therapy
LCD Liquid Crystal Display
LED Light Emitting Diode
MBBS Bachelor of Medicine and Bachelor of Surgery
MD Managing Director
MO Medical Officers
MoU Memorandum of Understanding
MPHW Multipurpose Health Worker
MS Medical Services
NABH National Accreditation Board for Hospitals & Healthcare Providers
NGO Non-Governmental Organization
NHM National Health Mission
NIC National Informatics Centre
NIDHI-TBI National Initiative for Developing and Harnessing Innovations- Techno Business Incubator
NQAS National Quality Assurance Standards
NTEP National Tuberculosis Elimination Program
OSD Officer on Special Duty
PDU Pandit Dindayal Upadhyay
PH Public Health
PHC Primary Health Centre
PHCs-MO Primary Health Centres - Medical Officers
PIB Press Information Bureau
PLWHA People Living with HIV /AIDS
PoE Points-of-Entry
PPE Personal Protective Equipment
PPP Public-Private Partnerships
RAT Rapid Antigen Test (for COVID-19)
RCCE Risk Communication and Community Engagement
RKS Rogi Kalyan Samiti
ix
RRTs Rapid Response Teams
RSS Rashtriya Swayamsevak Sangha
RT-PCR Reverse Transcription–Polymerase Chain Reaction
SARI Severe Acute Respiratory Infections
SBCC Social and Behaviour Change Communication
SHSRC State Health System Resource Centre
SIHFW State Institute of Health and Family Welfare
SMIMER Surat Municipal Institute of Medical Education and Research
SOP Standard Operating Procedure
SQAS State Quality Assurance Standards
SSC State Steering Committee
SSGH Sir Sayajirao General Hospital
TAZ-HOPES-T Thiamine, Ascorbic Acid, Zinc, Heparin, Oxygen therapy, Prone position, Eliminate exertion, Steroids, Tocilizumab
TB Tuberculosis
THR Take-Home Rations
UHCs Urban Health Centres
UNDP United Nations Development Programme
UNICEF United Nations Children’s Fund
USP Unique Selling Proposition
WHO World Health Organization

x
xi
PREFACE
Ever since the World Health Organization (WHO) declared the outbreak of 2019 novel coronavirus (COVID-19) as a public health emergency, the Government of India and the Government of Gujarat have collectively undertaken and implemented several pandemic responses that include measures on preparedness, prevention, mitigation, control and recovery. Gujarat, in particular, has developed its own operational response plan and implemented several strategic measures to combat the spread of COVID-19 and secure the welfare of its people.
Acknowledging the fact that the COVID-19 pandemic is likely to continue in the near future, it becomes imperative to review the ongoing responses of the state administration. The objective and motivation behind this is to qualitatively review the public health management actions already undertaken, to identify the current best practices, the achievements and the challenges faced. This process of response review is knowledge enriching in itself and may help all interested stakeholders in improved handling of public health emergencies that enables long-term health security.
This review used a new WHO tool developed for country intra-action reviews (IAR). The review report highlights important success factors and provides recommendations across ten important areas. The review also documents the challenges that the stakeholders faced while dealing with the outbreak and recommends critical improvements required to ramp up the health response.
IAR is a consolidated repository of identified challenges and recommendations for the state to further build upon the learnings from the pandemic as well as an evident guidance for future emergencies. We hope this report will also facilitate some actionable insights to other states and countries and help improve pandemic resilience towards a safer world.

xii
xiii
The intra-action review (IAR) presents a qualitative assessment of the strategic responses of the Government of Gujarat in managing the ongoing COVID-19 pandemic. The main objective of the IAR is to facilitate sharing of experiences and enable mutual learning. In the process of documentation, the IAR draws out the key reflections from COVID-19 management in the state under 10 different response pillars as identified by the WHO. The IAR was conducted by bringing together a small group of COVID-19 responders with knowledge of public health response and holding personal interviews with these stakeholders. The responses of the stakeholders were then analysed to identify the best practices in efficient management of COVID-19 crisis. Evaluation of transcription and audio summaries of 79 stakeholders were considered and consolidated for the IAR process. By reviewing the strategic responses, the IAR also compiles stakeholder perceptions and identifies the gaps and lessons learned in the management process.
The report focusses on the various COVID-19 aspects related to the epidemiological situation and the responses to the ten pillars. These pillars align with the WHO Global COVID-19 Strategic Preparedness and Response Plan. They are classified as 1) Coordination, planning & monitoring; 2) Risk communication & community engagement; 3) Surveillance, response & containment; 4) Points of entry capacities; 5) Laboratory capacities & quality assurance; 6) Infection prevention & control; 7) Case management & hospital preparedness; 8) Operational support & logistics; 9) Research, Innovation & knowledge sharing; and 10) Maintaining essential health services.
The crisis induced by the pandemic was unprecedented. In the face of this challenge, Gujarat responded nimbly by learning, unlearning, relearning based on available resources and evidence. The state’s response was spearheaded by a strong and committed leadership, proactive administration, and a robust and resilient public health system. Regular monitoring by a Core Committee comprising of the Chief Minister, senior leaders and officers along with inputs from COVID-19 task force of clinical and public health specialists provided much needed impetus. A special Inter Personal Communication toolkit was created for use by the frontline workers to effectively engage with the community and
EXECUTIVE SUMMARY
xiv
sustain the gains of the multi-pronged communication strategy. Arogya Setu ITIHAS was leveraged to identify hotspots and plan community surveillance. Stringent contact tracing and community pulse oximetry helped in early identification and preventing transmission. USP of the surveillance strategy was Dhanvantari Raths (mobile medical vans), which not only undertook symptomatic and thermal screening, pulse oximetry, rapid antigen testing in the community but also ensured continuity of essential health services during and after lockdown by providing medical care for common illnesses at doorstep. Uninterrupted logistics and supplies were ensured through High level Purchase Committee. Three tiered COVID-19 care facilities were setup across all districts. Beds across all categories as well as testing facilities were exponentially increased. Rapid antigen tests were widely used for walk-in-testing at Kiosks, on call home-based testing, mobile testing vans and across most public health facilities. Gujarat was one of the first states to ensure access of latest drugs and oxygen therapy in its government facilities free of cost. Online tele-mentoring sessions were regularly conducted for all COVID-19 treating centres for sharing knowledge and guidance. Large scale online capacity building was done evident from the fact that the state ranked first in the country for i-GOT based COVID-19 training. Research was actively promoted; innovations were supported, and essential services were quickly restored. The state geared up for the COVID-19 vaccination role out with formation of state steering committee, AEFI committees, dry run, and community engagement.
Several challenges were faced in managing the pandemic, including: enforcing containment zones and quarantine, managing migrants, misinformation and rumours, sustaining COVID-19 appropriate behaviour, reporting and recording data, testing in initial phase, changing guidelines, shortage and apprehensions among healthcare staff and continuity of essential services in initial phase. Various strategies and innovations were implemented to try and address these.
Based on the good practices implemented, challenges faced, and lessons learnt, some of the major and key recommendations, pillar-wise, for overall health systems strengthening and pandemic resilience are provided below. These will serve as a ready reckoner for other states and nations to conceive and strengthen COVID-19 response and other pandemic management strategies.
Pillar 1: Coordination, planning & monitoring
▶ Mechanism to regularly review state disaster vulnerability and risks of high threat pathogens through a multi-hazard risk assessment may be institutionalized. Overall disaster preparedness and response capacity across districts can be reviewed and updated periodically based on risk assessment, vulnerability mapping, coping capacities, infrastructure and resources available.
xv
▶ Learnings from COVID-19 pandemic management may be institutionalized to develop a comprehensive emergency preparedness and response system, which would include strategy, planning, human resources and capacity building to ensure an enabling environment for mitigation and response; with well-defined roles and responsibilities of different sectors / ministries / agencies.
▶ Continue working with private sector, civil society partners and NGOs for enhanced access to healthcare services and strengthen these networks further through sustained engagement. Evolving a regulatory framework for a more formal engagement will help strengthen essential healthcare service delivery and disease surveillance.
▶ Based on experiences of managing human resources (HR) during the pandemic, regular planning and review of HR may include provisioning for staff motivation, support, coping strategies and prevention of fatigue/burnout; so as to ensure effective response to any evolving pandemic situation.
▶ An Integrated Health Information Platform (IHIP) has been developed by Government of India. It may be implemented in an accelerated manner to augment the epidemiology and public health capacity of the system.
▶ Even after the COVID-19 ceases to be a pandemic, other emerging diseases with pandemic potential remain a significant public health concern. This inter-pandemic phase may be used for strengthening and capacity building of the health systems through coordinated efforts of the technical, training and implementation divisions.
Pillar 2: Risk communication & community engagement
▶ Even with the rollout of vaccination, the strategies of Risk Communication and Community Engagement (RCCE) will remain the mainstay of the COVID- 19 response. The existing Health Education Bureau, Social and Behavior Change division may be strengthened to integrate IEC needs of all departments and stakeholders as well as devise, implement and monitor strategies contextualized to the local needs.
▶ Efforts at innovating risk communication strategies / tools, such as the inter-personal communication toolkit, may be continued to integrate need-based messages. A system for rapidly developing and disseminating new information products as per evolving epidemiology will aid effective community engagement.
▶ Sharing COVID-19 success stories to motivate people and boost patients’ morale under stressful conditions and to develop confidence of people in management efforts of the government has given good results. This initiative may be institutionalized and leveraged to improve utilization of essential health services across all levels.
▶ Community involvement, as done for COVID-19, may be expanded by further identification of lead community influencers (religious leaders, prominent public figures like singers, sports people, village level influential people) and building a system of their orientation on a continuous basis to ensure a ready mechanism / network to tap for mass awareness and social behaviour change communication, especially during public health emergencies.
xvi
Pillar 3: Surveillance, response & containment
▶ Current pandemic management involved robust surveillance at different levels by different teams. The epidemic response mechanism starting from command and control center, early identification of warning signals, surveillance and rapid response can be further strengthened based on experiences of this pandemic.
▶ Existing network of IDSP may be strengthened by ensuring wider participation of private sector (including private sector labs). Consistent engagement and capacity building of the private sector may be done for reporting of key syndromes and triggers.
▶ Aarogya Setu (AS), ITIHAS helped boost surveillance efforts. An appropriate regulatory framework will help set up a mechanism which would leverage the IT and GIS platform (like in AS-ITIHAS, IHIP) and have inter-operability with various surveillance systems run by local health departments, hospitals and laboratories.
▶ Leveraging the national Integrated Health Information Platform (IHIP) will help moving from aggregate based reporting to case-based reporting. Overall, surveillance systems could be targeted considering the ‘One Health’ approach and include the other key departments which can identify the possible high threat pathogen outbreaks.
▶ Death Audit is being carried out in the state. However, in the longer run there could be targeted efforts to strengthen the existing systems for capturing vital statistics including the death reviews. All-cause mortality data may be registered by utilizing the ICD reporting systems.
Pillar 4: Points of entry capacities
▶ Risk assessment (based on traffic load, destinations covered, human or cargo traffic etc.) of all major Points of Entry (airports, seaports and ground crossings) may be conducted to identify areas needing further strengthening. A roadmap for systematic investments for improvement as per IHR (2005) can be developed.
▶ Contingency plans at designated Points-of-Entry (PoE) can be updated, with clear roles and responsibilities of all key departments. These plans may be tested once a year through tabletop/mock exercises. Technical working groups can be constituted at every designated PoE for co-ordination and interstate convergence.
▶ Active partnership and formal engagement with employers, civil society, NGO partners, humanitarian agencies as seen during COVID-19 migrant management may be continued to ensure that they are well covered as per various state policies.
Pillar 5: Laboratory capacities & quality assurance
▶ Existing six regional labs may be upgraded and the scope of molecular, serology and other specialized tests at district and block levels may be expanded to meet the demands of any health emergency. State-of-the-art reference laboratory at state level with advanced virology capacity can be established.
▶ Laboratory surge capacity plan, for an outbreak of High Threat Pathogen (HTP), may be developed.
xvii
▶ State laboratory network may be expanded to involve private labs. Uniform recording formats, standards, SoPs and trainings can be adopted across all networked labs.
▶ Develop a laboratory surge capacity plan, for an outbreak of High Threat Pathogen (HTP).
▶ An advanced and exclusive Public Health Laboratory Training Centre, linked to Medical Colleges, can be setup for supporting training needs of regional and district public health laboratories including biosafety and biosecurity. It can also facilitate analysis of data for better understanding of the dynamics of local disease transmission.
▶ With focus on quality of care, several state labs have been accredited. A roadmap for accreditation of all labs may be planned, starting with the district level in the first phase followed by those in the periphery.
Pillar 6: Infection prevention & control
▶ Existing infection prevention and control (IPC) policy/framework can be made more comprehensive by including infrastructure, systems and capacity building. Monitoring and Evaluation of IPC practices including regular IPC audits in hospital settings may also be incorporated and practiced beyond the pandemic.
▶ The state has developed a State Quality Assurance Standards (SQAS) on the lines of NQAS and many centres are accredited under different standards. Universally implementing quality assurance standards like SQAS, NABH, NQAS, Kayakalp will ensure better IPC practices at the health care centers.
Pillar 7: Case management & hospital preparedness
▶ Developing further upon the positive experiences, the state can undertake meticulous resource and financial planning to augment capacity for combating pandemic/emergency surge at field hospital level. It should continue active engagement with private providers and evolve mechanisms for further building and sustaining these networks, including a regulatory framework for surge capacity and preparedness for any such emergencies.
▶ Tele-mentoring has aided knowledge sharing, capacity building and hand holding of the all clinicians involved in COVID-19 care across the state. This can be institutionalized and extended to other diseases of public health importance.
▶ Post COVID-19 clinics may be setup to manage and document long term morbidity due to COVID-19, which will also assist in further strengthening the existing body of evidence and developing guidelines.
▶ The practice of issuing standard treatment guidelines during COVID-19 may be institutionalized and a compendium of treatment guidelines and protocols for all notifiable diseases may be issued which gets reviewed regularly and updated in view of new evidences.
▶ Initiatives taken for hospital safety and hazard preparedness may be made an inclusive part of continuing medical education and training programs for healthcare cadres to efficiently deal with complex emergencies in future.
xviii
Pillar 8: Operational support & logistics
▶ Practices like high level purchase committee, decentralization of procurement, pre- approvals for purchase of critical items, team of experts for quality check and approval may be institutionalized and practiced well beyond the pandemic.
▶ The state ensured surge capacity for trained HR through online trainings. This mechanism can be institutionalized and include different domains across different cadres. State-level health / medical universities, overarching all the medical, nursing, paramedical courses will ensure optimal capacity building and coordinated response in pandemic and other eventualities.
▶ Healthcare infrastructure, logistics and procurement division may be strengthened financially and logistically by enabling them to garner emergency funding and support from donors and other departments.
Pillar 9: Research, innovation & knowledge sharing
▶ Gujarat was one of the first states to establish a state level COVID-19 research committee with State Health System Resource Centre as the nodal agency. Institutionalizing this along with a state specific public health journal will help create an enabling environment for research and assist in undertaking, collaborating and disseminating locally relevant research.
▶ A consortium of institutions of repute, from various sectors, may be instituted to engage in research on cross cutting themes on COVID-19 and other diseases.
▶ A COVID-19 State Task Force, composed of eminent clinicians and academicians, was constituted to support the administration in managing the pandemic. Such a mechanism can be considered as a standing taskforce for non-emergency situations as well. Eminent experts, outside government may be regularly consulted for their inputs and opinions.
▶ Several effective innovative approaches were adopted by the state to combat COVID-19, for ensuring continuity of essential health services viz. Dhanvantri Rath, 1100 helpline, e-Sanjeevani. These may be sustained and extended for routine care.
▶ Engagement of the public health and IT department, as during COVID-19 pandemic (AS ITIHAS) may be institutionalized and systematic appraisal of the role of health technology for generating scientific evidence, planning and service delivery may be promoted.
▶ Documentation of effective interventions and strategy, as through IAR, may be promoted for all public health challenges and threats. System for collaborating with eminent institutions and development partners in the state, country or abroad may be institutionalized. State specific public health newsletter and research journal can help quickly disseminate these.
▶ Several effective innovative approaches were adopted by the state to combat COVID-19, for ensuring continuity of essential health services viz. Dhanvantari Rath, 1100 helpline, e-Sanjeevani. These may be sustained and extended for routine care.

xix
Pillar 10: Maintaining essential health services
▶ The state has taken an initiative to address urban health needs by rolling out urban health clinics (Deendayal clinics) for the urban poor. Further strengthening of the system through adequate technical and financial resources will help to ensure continuum of care for the marginalized urban populations and universal health coverage.
▶ Continuity of essential healthcare services was largely maintained during current pandemic. Mechanisms to ensure the same, also involving private health providers and other sectors, may be institutionalized. It can also involve strategies for better integration of ASHA, Aanganwadi and other grassroot workers for community based delivery of essential health care including mental health services.
▶ Communication strategies to encourage health seeking behavior, seek timely access to essential health services and adopt healthy behaviors may be reinforced and continued.
xx
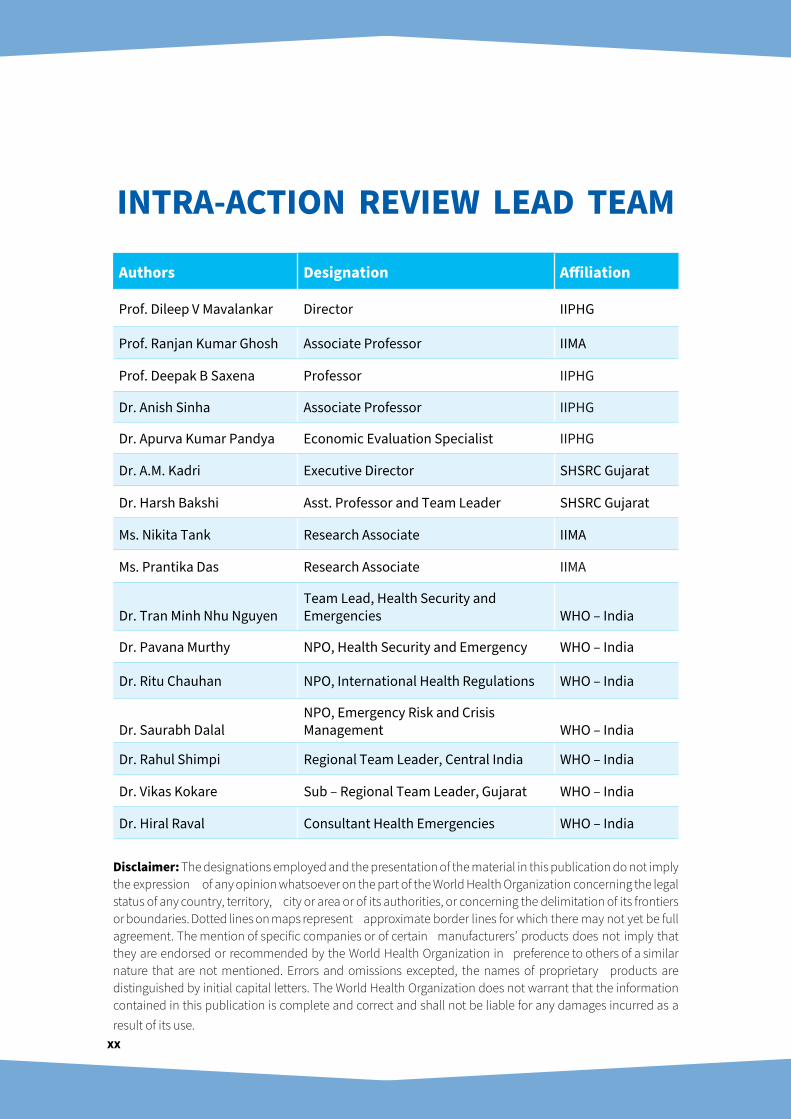
Authors Designation Affiliation
Prof. Dileep V Mavalankar Director IIPHG
Prof. Ranjan Kumar Ghosh Associate Professor IIMA
Prof. Deepak B Saxena Professor IIPHG
Dr. Anish Sinha Associate Professor IIPHG
Dr. Apurva Kumar Pandya Economic Evaluation Specialist IIPHG
Dr. A.M. Kadri Executive Director SHSRC Gujarat
Dr. Harsh Bakshi Asst. Professor and Team Leader SHSRC Gujarat
Ms. Nikita Tank Research Associate IIMA
Ms. Prantika Das Research Associate IIMA
Dr. Tran Minh Nhu NguyenTeam Lead, Health Security and Emergencies WHO – India
Dr. Pavana Murthy NPO, Health Security and Emergency WHO – India
Dr. Ritu Chauhan NPO, International Health Regulations WHO – India
Dr. Saurabh DalalNPO, Emergency Risk and Crisis Management WHO – India
Dr. Rahul Shimpi Regional Team Leader, Central India WHO – India
Dr. Vikas Kokare Sub – Regional Team Leader, Gujarat WHO – India
Dr. Hiral Raval Consultant Health Emergencies WHO – India
Disclaimer: The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. The World Health Organization does not warrant that the information contained in this publication is complete and correct and shall not be liable for any damages incurred as a result of its use.
INTRA-ACTION REVIEW LEAD TEAM
1
1
The IAR process was planned and implemented in three phases i.e., pre, during and post Intra-Action Review
During the pre-IAR phase, team members were identified and trained for conducting interviews and documenting responses. The list of probable stakeholders to be included in the review process during the phase 2 was also identified. The detailed list of the stakeholders engaged in the process is included in Annexure 1. The proposal was subjected to ethical clearance from Institutional Ethics Committee (IEC) of IIPH Gandhinagar. Based on the advice of the IEC, the observations and verbatim quotes were anonymized.
During the Intra-Action Review: The State Health System Resource Centre (SHSRC) Gujarat coordinated the interviews which were audio recorded, transcribed, and summarized. A series of workshops were undertaken to consolidate and analyze the lessons learnt, challenges and recommendations.
79 interviews were conducted in total and responses to the 10 identified pillars were identified and categorized. Recommendations and short videos were framed specific to each pillar.
Post Intra-Action Review: The IAR report draft was shared among the partners for their review.
INTRA-ACTION REVIEW METHODOLOGY

2
3
Gujarat state of India is one of the most industrialized states and is a manufacturing hub of the country. The state is located in the western region with a population of approximately 60 million and covers 196,024 sq. km area. The economy of Gujarat is the fifth-largest in India, with a gross state domestic product (GSDP) of ₹15.03 trillion (US$210 billion). Gujarat has one major international airport1.
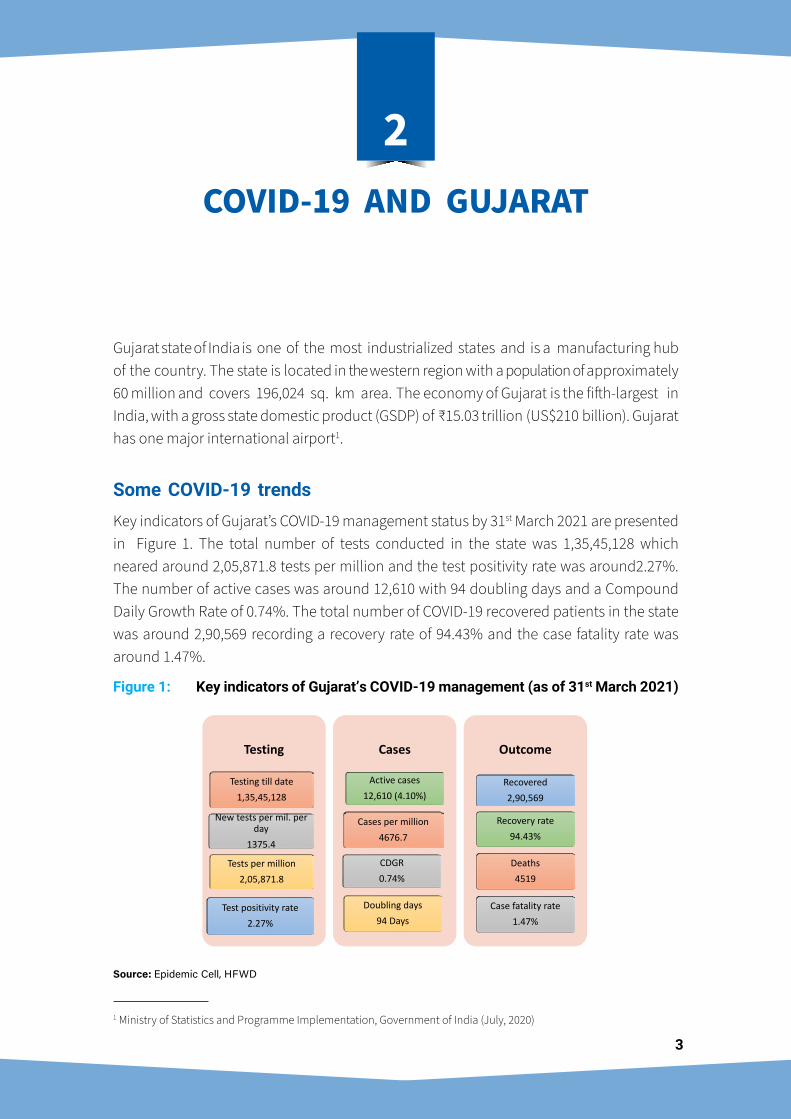
Some COVID-19 trendsKey indicators of Gujarat’s COVID-19 management status by 31st March 2021 are presented in Figure 1. The total number of tests conducted in the state was 1,35,45,128 which neared around 2,05,871.8 tests per million and the test positivity rate was around2.27%. The number of active cases was around 12,610 with 94 doubling days and a Compound Daily Growth Rate of 0.74%. The total number of COVID-19 recovered patients in the state was around 2,90,569 recording a recovery rate of 94.43% and the case fatality rate was around 1.47%.
Figure 1: Key indicators of Gujarat’s COVID-19 management (as of 31st March 2021)Figure 1
Figure 2:
Testing
Testing till date1,35,45,128
New tests per mil. per day
1375.4
Tests per million2,05,871.8
Test positivity rate2.27%
Cases
Active cases12,610 (4.10%)
Cases per million4676.7
CDGR 0.74%
Doubling days94 Days
Outcome
Recovered2,90,569
Recovery rate94.43%
Deaths4519
Case fatality rate 1.47%
Cumulative cases, 307698
Deaths, 4519
Recovered, 290569
Active cases, 12610
0
50000
100000
150000
200000
250000
300000
350000
19-M
ar27
-Mar
04-A
pr12
-Apr
20-A
pr28
-Apr
06-M
ay14
-May
22-M
ay30
-May
07-Ju
n15
-Jun
23-Ju
n01
-Jul
09-Ju
l17
-Jul
25-Ju
l02
-Aug
10-A
ug18
-Aug
26-A
ug03
-Sep
11-S
ep19
-Sep
27-S
ep05
-Oct
13-O
ct21
-Oct
29-O
ct06
-Nov
14-N
ov22
-Nov
30-N
ov08
-Dec
16-D
ec24
-Dec
01-Ja
n09
-Jan
17-Ja
n25
-Jan
02-F
eb10
-Feb
18-F
eb26
-Feb
06-M
ar14
-Mar
22-M
ar30
-Mar
Cumulative cases Deaths Recovered Active cases
Source: Epidemic Cell, HFWD
1 Ministry of Statistics and Programme Implementation, Government of India (July, 2020)
COVID-19 AND GUJARAT
2
4
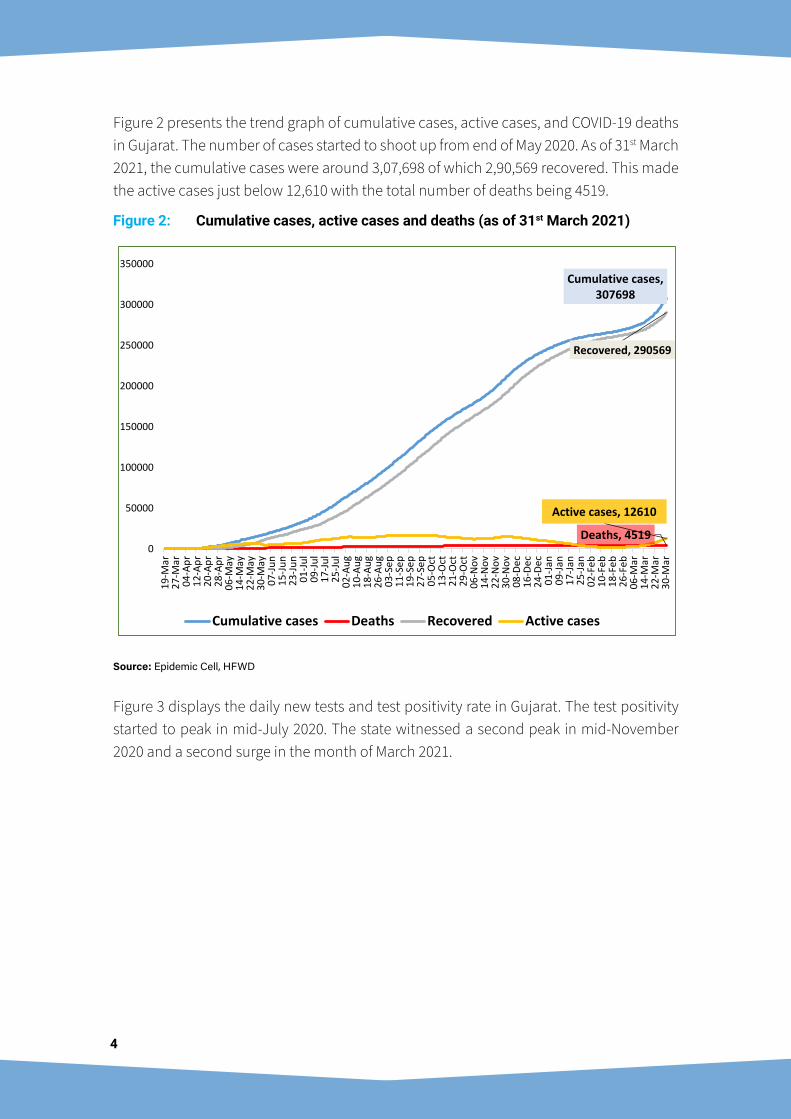
Figure 2 presents the trend graph of cumulative cases, active cases, and COVID-19 deaths in Gujarat. The number of cases started to shoot up from end of May 2020. As of 31st March 2021, the cumulative cases were around 3,07,698 of which 2,90,569 recovered. This made the active cases just below 12,610 with the total number of deaths being 4519.
Figure 2: Cumulative cases, active cases and deaths (as of 31st March 2021)
Figure 1
Figure 2:
Testing
Testing till date1,35,45,128
New tests per mil. per day
1375.4
Tests per million2,05,871.8
Test positivity rate2.27%
Cases
Active cases12,610 (4.10%)
Cases per million4676.7
CDGR 0.74%
Doubling days94 Days
Outcome
Recovered2,90,569
Recovery rate94.43%
Deaths4519
Case fatality rate 1.47%
Cumulative cases, 307698
Deaths, 4519
Recovered, 290569
Active cases, 12610
0
50000
100000
150000
200000
250000
300000
350000
19-M
ar27
-Mar
04-A
pr12
-Apr
20-A
pr28
-Apr
06-M
ay14
-May
22-M
ay30
-May
07-Ju
n15
-Jun
23-Ju
n01
-Jul
09-Ju
l17
-Jul
25-Ju
l02
-Aug
10-A
ug18
-Aug
26-A
ug03
-Sep
11-S
ep19
-Sep
27-S
ep05
-Oct
13-O
ct21
-Oct
29-O
ct06
-Nov
14-N
ov22
-Nov
30-N
ov08
-Dec
16-D
ec24
-Dec
01-Ja
n09
-Jan
17-Ja
n25
-Jan
02-F
eb10
-Feb
18-F
eb26
-Feb
06-M
ar14
-Mar
22-M
ar30
-Mar
Cumulative cases Deaths Recovered Active cases
Source: Epidemic Cell, HFWD
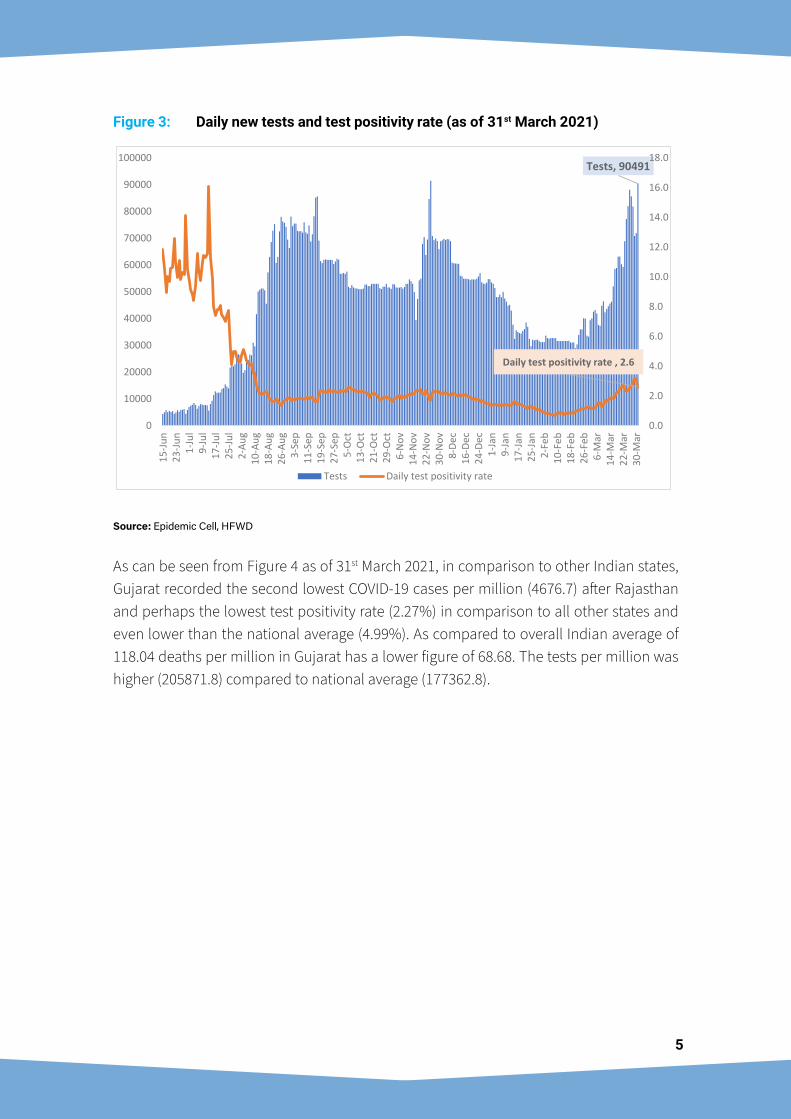
Figure 3 displays the daily new tests and test positivity rate in Gujarat. The test positivity started to peak in mid-July 2020. The state witnessed a second peak in mid-November 2020 and a second surge in the month of March 2021.
5
Figure 3: Daily new tests and test positivity rate (as of 31st March 2021)
Figure 3
Figure 4
Tests, 90491
Daily test positivity rate , 2.6
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
10000015
-Jun
23-Ju
n1-
Jul
9-Ju
l17
-Jul
25-Ju
l2-
Aug
10-A
ug18
-Aug
26-A
ug3-
Sep
11-S
ep19
-Sep
27-S
ep5-
Oct
13-O
ct21
-Oct
29-O
ct6-
Nov
14-N
ov22
-Nov
30-N
ov8-
Dec
16-D
ec24
-Dec
1-Ja
n9-
Jan
17-Ja
n25
-Jan
2-Fe
b10
-Feb
18-F
eb26
-Feb
6-M
ar14
-Mar
22-M
ar30
-Mar
Tests Daily test positivity rate
Source: Epidemic Cell, HFWD
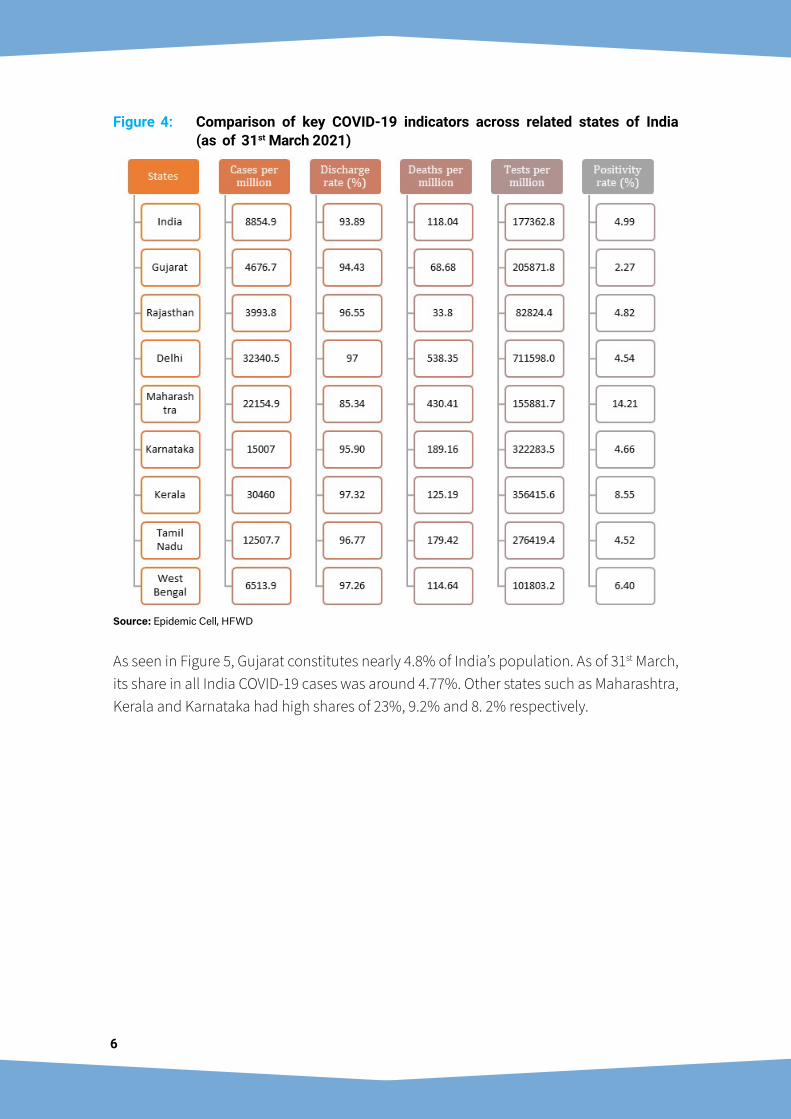
As can be seen from Figure 4 as of 31st March 2021, in comparison to other Indian states, Gujarat recorded the second lowest COVID-19 cases per million (4676.7) after Rajasthan and perhaps the lowest test positivity rate (2.27%) in comparison to all other states and even lower than the national average (4.99%). As compared to overall Indian average of 118.04 deaths per million in Gujarat has a lower figure of 68.68. The tests per million was higher (205871.8) compared to national average (177362.8).
6
Figure 4: Comparison of key COVID-19 indicators across related states of India (as of 31st March 2021)
Figure 5
17.8
9.2 8.96.5 6.1 6.0 5.1 4.8 4.8 3.8 3.3 2.7 2.7 2.2 1.5
5.1
23.0
2.24.8
2.4 2.7
7.3 8.2
2.5
7.4
2.8 2.5
9.2
2.0
5.4
0.0
5.0
10.0
15.0
20.0
25.0
Utt
ar P
rade
sh
Mah
aras
htra
Biha
r
Wes
t Ben
gal
Mad
hya
Prad
esh
Raja
stha
n
Tam
il N
adu
Karn
atak
a
Guj
arat
Andh
ra P
rade
sh
Oris
sa
Tela
ngan
a
Kera
la
Punj
ab
Delh
i
% Population of India % Cases of India
Source: Epidemic Cell, HFWD
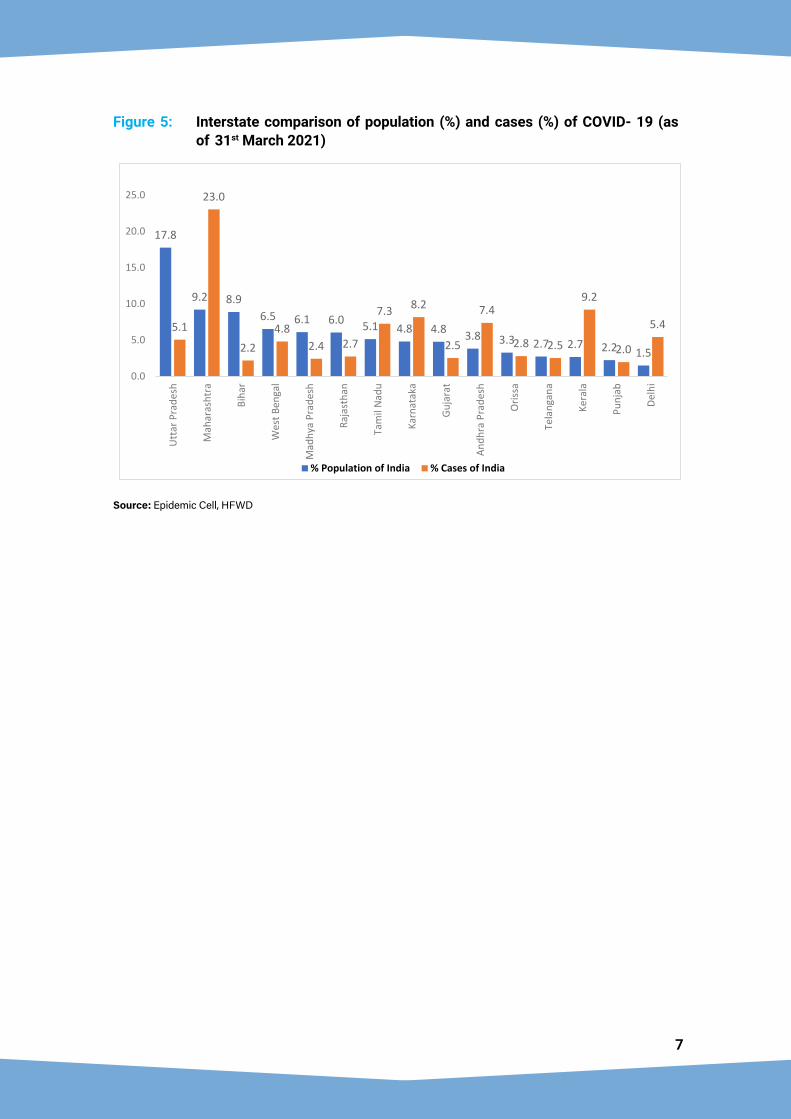
As seen in Figure 5, Gujarat constitutes nearly 4.8% of India’s population. As of 31st March, its share in all India COVID-19 cases was around 4.77%. Other states such as Maharashtra, Kerala and Karnataka had high shares of 23%, 9.2% and 8. 2% respectively.
7
Figure 5: Interstate comparison of population (%) and cases (%) of COVID- 19 (as of 31st March 2021)
Figure 5
17.8
9.2 8.96.5 6.1 6.0 5.1 4.8 4.8 3.8 3.3 2.7 2.7 2.2 1.5
5.1
23.0
2.24.8
2.4 2.7
7.3 8.2
2.5
7.4
2.8 2.5
9.2
2.0
5.4
0.0
5.0
10.0
15.0
20.0
25.0
Utt
ar P
rade
sh
Mah
aras
htra
Biha
r
Wes
t Ben
gal
Mad
hya
Prad
esh
Raja
stha
n
Tam
il N
adu
Karn
atak
a
Guj
arat
Andh
ra P
rade
sh
Oris
sa
Tela
ngan
a
Kera
la
Punj
ab
Delh
i
% Population of India % Cases of India
Source: Epidemic Cell, HFWD

8
9
Pillar 1: Coordination, planning, and monitoringIntroduction
The Disaster Management Act 2005 and the Epidemic Diseases Act, 1897 were evoked on 13th March 2020 by Government of Gujarat. This facilitated in setting up flu corners and isolation / quarantining of persons from affected countries. This included mandatory detention and quarantining of suspected patients who refused voluntary isolation. Guidelines were issued and preventive measures were undertaken for all government offices and employees.
Strengths and Achievements
Leadership and decision makingThe COVID-19 response witnessed highest-level of engagements from the Chief Minister (CM) of Gujarat, the Deputy Chief Minister, the Chief Secretary, and senior officials in the CMO and Health and Family Welfare Department (H&FWD). There was involvement of the Home Department and the Food and Civil Supplies Departments. To facilitate procurement
STRATEGIES, CHALLENGES AND RECOMMENDATIONS
3

10
procedures, a high-level purchase committee was constituted under chairmanship of Additional Chief Secretary (Revenue) with Principal Secretary (Health and Family Welfare), Principal Secretary (Industries & Mines) and Commissioner (Health) as members. At the district and city level, planning implementation were carried out under the supervision of a core committee, consisting of the District Collector, Municipal Commissioner, District Development Officers and the nodal officer. The core committee conducted daily reviews. A state level task force under the chairmanship of Principal Secretary (Health) for COVID-19 was set up to provide technical guidance with clinical and public health experts from the private and public sector.
Initial preparation for COVID-19: Rapid expansion of hospital capacityDedicated COVID-19 hospitals were established in four major cities – Ahmedabad, Vadodara, Surat, and Rajkot. In all districts at least one hospital was designated as a COVID-19 hospital. Within a span of 7-10 days, a 1200 bed hospital was established in Ahmedabad, and in the case of Rajkot and Surat, 250 to 500 beds were introduced. In Vadodara, the 400-bed and 800-bed hospital capacity were increased to 1,500 beds, and 2,000 beds respectively. Health infrastructure such as ventilatory support and oxygen lines were gradually increased. There was enhanced effort and focus on strengthening the state health infrastructure, manpower capacity and efficient handling and management of cases. For instance, in Surat the civil hospital was converted to an oxygen facility and in Vadodara data driven actions and committed leadership helped enhance hospital capacity ahead of peak surge.
Public-Private Partnership (PPP) modelA strong public-private partnership ensured better coordination for handling the surge of severe cases that needed hospitalization. Around 50% of the beds in private hospitals were reserved for patients referred through government / corporation system. Private practitioners were consulted to ensure treatment of non-COVID-19 health issues. One of the early adopters of these best practices was the Amdavad Municipal Corporation (AMC).
11
Community and non-governmental stakeholder supportThe NGOs, media, police, and industry sectors provided support in different ways. Surat was a good example to start community isolation centers with support of volunteers. Around 30 million people were fed during the lockdown. The media played an important role by highlighting issues and difficulties faced by the patients. It also acted as a medium to amplify risk communication messages, contribution of plasma donors, and the good work being done by the doctors, nurses and other medical staff. The industry stakeholders provided support in establishing COVID-19 care centers.
Religious leaders, community leaders and local food suppliers all participated actively. Many volunteered to get themselves tested to eliminate fear in the community. Another best practice was in Rajkot, where a joint team consisting of officials from the revenue officials, municipal corporation a n d police department were stationed for 24 hours in three shifts to coordinate with the local community leader and volunteers.
Monitoring and coordination of home isolated patientsMonitoring and coordination of home isolation was strengthened at different levels especially for health workers at the grassroot level followed by medical officer (MO), specialist doctors and a call center for the overall monitoring. Regular meetings between officials such as the district development officer and municipal commission facilitated information sharing and informed strategy.
Adoption of technology innovationTechnological innovation was used to gather information and inform decision making. A ‘Tracker’ application was used for the International travelers and those advised home isolation and team visits in case of non-compliance. Acute respiratory infection (ARI) surveillance was undertaken covering all public and private hospitals and clinics. Daily information was collected through m obile and web-based applications. In Surat city, around 2000 private clinics reported ARI cases on Jaimini application which led to identification of hotspots and enabled quick response to outbreaks. AS- ITIHAS applications were very useful to plan surveillance activities, placement of Dhanvantari Raths (see sections below) and in defining the containment zones and hotspots.
GIS based applications under the Smart City Project were integrated and it assisted in ARI Surveillance, COVID-19 positive early identification, quarantine, isolation, and planning. The pharmacy store chemists in 6 districts were given a new application to report persons with symptoms.
Preparations for COVID-19 vaccine roll outThe state ensured registration of almost all HCWs from public as well as private sector for the first phase of vaccination. Dry runs were done to check the system preparedness
12
and identify potential bottlenecks. A State Steering Committee (SSC) was formed to oversee the COVD-19 vaccination. SSC was chaired by Chief Secretary and all the cabinet secretaries were members of the steering committee along with UN development partners (WHO, UNICEF and UNDP) and Presidents of IMA, AOP state chapters. The SSC met regularly to review the progress and swiftly acted upon the operational bottlenecks and systematically directed the state machinery to resolve vaccine hesitancy. COVID-19 vaccination was effectively rolled out. As on 31st March 2021 a total of 56,85,273 vaccine doses were delivered. Of these 1st dose HCW was 4,94,429 (87%), 2nd dose HCW was 321542 (78%), 1st dose of FLW was 562282 (92%), 2nd dose of FLW was 3,14,345 (72%) and others 1st dose was 39,56,141 (77%) while 2nd dose was 36,534.
Challenges and Strategies
Declaring of containment zoneIn the initial phase, the declarations regarding large containment zones were met with resistance, especially after the lockdown got lifted. For better management, the concept of micro-containment zones was eventually introduced.
Issuance of permits for essential servicesPermits were issued from the district collector’s office within the span of half a day, and responses were also provided via email to support emergency travel.
Dealing with the migrantsMigrants were provided special transportation arrangements for their safe return to other states and special buses for inter-district transfer and to other states. In the interim, stay and food arrangements were provided through shelter homes. Helpline numbers at state and district level were set up.
One of the best practices was Surat making available early 450 trains to places such as Uttar Pradesh, Bihar, Jharkhand and Orissa. In spite of insufficient funds, the Gram Panchayats still managed to arrange community kitchens and the police personnel arranged for tickets.
Meeting daily essentials requirementsProactive volunteering efforts by civil societies supported the essential daily requirements, including at community kitchens and community isolation centers as the guidelines for isolation of cases, quarantine of contacts and notification for containment was strict.
Recommendations
• Mechanism to regularly review state disaster vulnerability and risks of high threat pathogens through a multi-hazard risk assessment may be institutionalized. Overall disaster preparedness and response capacity across districts can be reviewed and updated periodically based on risk assessment, vulnerability mapping, coping capacities, infrastructure and resources available.

13
• Learnings from COVID-19 pandemic management may be institutionalized to develop a comprehensive emergency preparedness and response system, which would include strategy, planning, human resources and capacity building to ensure an enabling environment for mitigation and response; with well-defined roles and responsibilities of different sectors / ministries / agencies.
• Continue working with private sector, civil society partners and NGOs for enhanced access to healthcare services and strengthen these networks further through sustained engagement. Evolving a regulatory framework for a more formal engagement will help strengthen essential healthcare service delivery and disease surveillance.
• Based on experiences of managing human resources (HR) during the pandemic, regular planning and review of HR may include provisioning for staff motivation, support, coping strategies and prevention of fatigue/burnout; so as to ensure effective response to any evolving pandemic situation.
• An Integrated Health Information Platform (IHIP) has been developed by Government of India. It may be implemented in an accelerated manner to augment the epidemiology and public health capacity of the system.
• Even after the COVID-19 ceases to be a pandemic, other emerging diseases with pandemic potential remain a significant public health concern. This inter-pandemic phase may be used for strengthening and capacity building of the health systems through coordinated efforts of the technical, training and implementation divisions.
Pillar 2: Risk communication & community engagementIntroduction
In early phase of the pandemic, there was a widespread panic in the community. In order to address the same, the government adopted the approach of transparency and proactive risk communication. Some of the key initiatives of the state government included extensive use of IEC such as mass communication, Interpersonal Communication (IPC) and Social and Behaviour Change Communication (SBCC). Other modes of media communication included extensive use of television, radio, social media networks, public hoardings etc. In addition, community engagement was widely encouraged to facilitate active surveillance, testing and treatment.
Strengths and Achievements
Developing and implementing targeted IECCommunication content was prepared in the initial phase of the pandemic. Targeted intervention for high-risk groups e.g., elderly, pregnant women, persons with co-morbidities, young adults, health care providers and police personnel were prioritized.

14
At the district level, a local need based decentralized approach for IEC was undertaken. Messages were prepared in a regional context to promote positive behaviour.
Extensive use of interpersonal communication toolkitsGujarat developed Interpersonal Communication (IPC) toolkit with the Centre for Social and Behaviour Change (CSBC) at the Ashoka University. Frontline workers were trained with this toolkit which provided guiding notes on symptom recognition, reporting, handwashing, wearing of masks, physical distancing, protecting elders and immunity boosting. For a wider public outreach, the IPC communication toolkit has been issued both in Gujarati and English language. Use of IPC toolkits helped the state to influence attitudes and social norms ultimately contributing to prevention and control of transmission.
Provision of right message to right people at right timeThe Government of Gujarat initiated IEC activities focusing on delivery of key messages and promoting behavioural change. Content was developed that included preventive (hand washing, social distancing, wearing mask, precautions taken during quarantine, guidelines for travelers), promotive (immunity boosting healthy diets, breathing exercises, Ayurvedic kaadha) and curative (when to seek treatment) aspects of COVID-19.
Specific IEC channels used included television, newspaper, radio, social-media, hoardings, banners, leaflets, and daily press briefs. Advertisement was provided in around 93 newspapers in three different languages (Gujarati, English, and Hindi language) since the first cases appeared in Gujarat. Initially maximum focus was given to television, which involved advertising 5-7 times a day in Gujarati news channels to reach the local population. Post the first phase of lockdown lifting, other modes were also prioritized such as radio jingles on seven FM radio-stations.
15
At later stages, focusing on the precautionary steps to be followed in the un-lockdown phases and reverse quarantine have been essential part of the IEC activities. Innovative measures such as video bytes were prepared and featured on YouTube, websites, social media handles like Facebook, Instagram, Twitter etc. Around 2200 creatives were prepared and circulated in various social media sites. ‘Namaste Gujarat’ sign was placed in all government offices and LCD/LED screen advertisements at railway stations for corona awareness.
Implemented collaborative approach to facilitate information delivery at local levelNational IEC material was suitably modified according to the regional context and translated to local languages to promote behavioural change in local population. I nter-departmental collaboration with support of stakeholders were held s u c h a s panchayat, tribal, Integrated Child Development Services (ICDS) were held, and specific modules were prepared. Webinars were conducted for orientation of health care providers.
Adopted need based and localized approach for information deliveryAt district level, a local need based decentralized approach was adopted. Messages were prepared in accordance with the regional context in a way to promote positive behavioral change in the local population to reduce COVID-19 transmission and mortality. Messages were based on the changing COVID-19 scenario of Gujarat, policy decisions, testing strategies and community behavior.
Adopted innovative and creative modes to spread awareness in rural areas‘COVID-19 Vijay Rath’ was developed by the Press Information Bureau (PIB) and UNICEF wherein teams of four theatrical members visited different regions for raising awareness regarding COVID-19. This was useful in reaching remote rural areas.
Community engagement for curtailing movementTo prevent imported cases, “Gram Yodhdha Committee” were formed in various villages, especially in the Ahmedabad district. The committee included Sarpanch, Talati, Health Workers, Teachers, Social leaders and Gram Rakshak Dal/Constable that monitored movement of people in their village. A movement register was maintained at village level.
Role of mediaIn the initial phase, since only government facilities were managing COVID-19, they were overwhelmed. Further, they were the focal point for referral of all critical cases which had poor outcome and this led to apprehension in the minds of the people regarding quality of care being provided at these dedicated COVID-19 setups. In the initial phase, there were instances of sensational journalism with a polarized view of government efforts and facilities. At one point, the government system and services came under severe criticism from print media.
16
The system responded by inviting editors of print media and other media houses to observe the CM dashboard and understand the nuances of the state’s response. They were thoroughly briefed on the several steps taken and behind the scene actions. The leadership and bureaucracy regularly engaged with media. The Chief Minister and State Task Force addressed separate press conferences to address all concerns and disseminate correct information.
Ultimately, the media played a crucial role in COVID-19 response by helping with proactive risk communication and SBCC. Television spots, radio jingles, daily Q&A sessions, interviews with eminent doctors/celebrities/personalities helped dispelling myths and creating awareness. There was prudent and responsive journalism whereby factual data and events were shared, interviews with corona patients on treatment and recovered were broadcasted/published, video documentation of service delivery, success stories and good practices were shared. All forms of mass media proactively engaged with the community to ensure compliance with COVID-19 appropriate behaviour and guidelines. Several government efforts and initiatives were widely disseminated through various media channels. Overall, media played an important role in replacing stigma and anxiety in the community with confidence and prudence.
Social cooperation aided in expanded and swift provision of COVID-19 careCommunity engagement played an important role in IEC, surveillance, and treatment. COVID- 19 Community Isolation Centres (CCIC) were initiated with the help of community leaders and municipal corporations. All expenses for beds, doctors and paramedical staff, food supply and community halls were borne by the community and all the technical support and trainings were facilitated by the municipal corporations. One of the first was Surat, where 18 CCIC were established involving different communities. Initially CCIC was initiated with intent to serve only the respective communities but after unanimous agreement between all community leaders, the CCICs were open to all communities. Local leaders supported advocacy, for example, the Vadodara Muslim Doctors Association and CCIC in Surat and Saurashtra. This supported more persons for testing and finally helped in decreasing community transmission.
Role of industry associationsThe Gujarat government engaged traders, industrialists, and business associations for risk communication during the pandemic. The industrial associations jointly with the state health department formulated detailed SOPs to handle COVID-19 situation, operation of businesses under COVID-19 conditions, testing of workers and managers through them.
The Diamond and Textile industry association in Surat district in coordination with the district Commissioner and the municipal corporation bodies facilitated implementation of SOPs in their daily work procedures to prevent or decrease the transmission among workers, sellers, and customers through IEC. The president of the textile unit or marketplace
17
showed preparedness for IEC and hoarding boards. Precautionary announcements in marketplaces were made every hour for reminding citizens to wear masks, identify symptoms, and do appropriate testing. In addition, testing units were set in each market according to numbers of shops with the help of corporations.
In addition, the state Government also mobilized functionaries from within the government such as teachers, Anganwadi workers and staff from the collector/revenue department. Community awareness content also included endorsement by celebrities, religious leaders and famous senior doctors.
Challenges and Strategies
Negative publicity and evidence-based rebuttalsInformation was disseminated using videos, and social media in a very dynamic day-to-day scenario, reaching out to all the different strata of the society. This countered a lot of misinformation that was generated.
Appreciation of corona warriors such as doctors, healthcare workers, police and sanitation- workers were done by preparing 20 minutes long documentaries to motivate these warriors, raise awareness and positive public image about the work done by them. This helped to reduce the stigma against those working on the frontline.
Dealing with rumorsDaily press release by the Principal Secretary of Health and Family Welfare aided in subsiding and supported in managing the situation. An extensive risk communication campaign was a solution for dealing with misinformation and promoting of facts from trusted sources like Government of India websites and WHO web portal.
Uncertainty due to lack of past experiences with the diseaseThis being a new disease, the government lacked previous experience and, therefore, the strategies evolved as a combination of field experiences and best available evidence. Global and national guidance were always considered before enacting a state specific guidance.
Other routine health activities affectedDuring the pandemic, routine health activities were severely impacted. To address this, specific messaging and awareness material regarding malaria, dengue, immunization etc. was also produced along with COVID-19.
Success stories used to deal with stigma, discrimination and panicMany success stories of recovered patients were prepared to build confidence in the population. Interviews of the patients and helpline numbers provided positive responses for the initiatives undertaken by the Gujarat Government. Feedback responses from them were also acknowledged and accordingly appropriate changes were made in services and COVID-19 management responses.
18
COVID-19 vaccine hesitancyThe government undertook IEC measures prior to the roll out to ensure good compliance and coverage. All forms of print, electronic and social media were extensively engaged to allay any fear and apprehension. Good media engagement and partnerships helped contain the rumours and misconceptions about vaccine. Vaccine hesitancy was observed among some HCWs but that was overcome through motivation and counselling, experience sharing and engagement with leading doctors and nurses.
Recommendations
• Even with the rollout of vaccination, the strategies of Risk Communication and Community Engagement (RCCE) will remain the mainstay of the COVID- 19 response. The existing Health Education Bureau, Social and Behavior Change division may be strengthened to integrate IEC needs of all departments and stakeholders as well as devise, implement and monitor strategies contextualized to the local needs.
• Efforts at innovating risk communication strategies / tools, such as the IPC toolkit, may be continued to integrate need-based messages. A system for rapidly developing and disseminating new information products as COVID-19 as per evolving epidemiology will aid effective community engagement.
• Sharing COVID-19 success stories to motivate people and boost patients’ morale under stressful conditions and to develop confidence of people in management efforts of the government has given good results. This initiative may be institutionalized and leveraged to improve utilization of essential health services across all levels.
• Community involvement, as done for COVID-19, may be expanded by further identification of lead community influencers (religious leaders, prominent public figures like singers, sports people, village level influential people) and building a system of their orientation on a continuous basis to ensure a ready mechanism / network to tap for mass awareness and social behaviour change communication, especially during public health emergencies.
Pillar 3: Surveillance, response, and containmentIntroduction
Gujarat has a very well-established Integrated Disease Surveillance Programme (IDSP) with regular analysis of the data and weekly alerts.
IDSP in Gujarat has its district teams and Rapid Response Teams (RRT) to carry out quick disease surveillance of any infectious disease outbreak. The RRT teams at district level were trained by the state IDSP and experts via face-to-face as well as online modules. The data gathered were analyzed at the district level and submitted to the state through an online IDSP portal.
19
Strengths and Achievements
Integrating surveillance with existing surveillance systemOne of the major strengths of the Government of Gujarat was the already established system of IDSP networks with both public and private reporting sites.
The COVID-19 surveillance system in Gujarat focused on 3-Ts: Test, Track and Treat. The state initiated a very well designated system of putting surveillance at all ports of entry such as Airports, Railways and Roads. Health teams from the state initiated screening of international travelers. Passengers were mandatorily screened and self-quarantined.
Human resource for surveillance activitiesDuring early phase of the pandemic, at state level, more than 5,000 health teams were engaged in carrying out the daily surveillance activities. Gujarat was one of the first few states that initiated house-to-house surveillance for COVID-19 in both urban and rural areas. Micro plans were prepared under the supervision of district/taluka/municipal health officials engaging Accredited Social Health Activist (ASHA), Multipurpose Health Worker (MPHW) and Community Health Officers (CHO) who were allocated the duty to screen rural communities. Urban ASHA workers along with the RRT teams and private practitioners were also allocated the duty of screening to cover the urban population in each affected district. Surveillance of influenza like illness and severe acute respiratory infections (ILI/SARI) were carried out using mobile application by private practitioners. Moreover, because of high incidence of infection in the state, the IDSP collaborated with SARI surveillance to carry out timely surveillance of COVID-19 infection.
Engaging private practitionersPrivate practitioners were sensitized early by the state regarding COVID-19 screening and management.
Use of technology in surveillanceAarogya Setu – a national mobile based surveillance data management application was used extensively in Gujarat. This digital service facilitated contact tracing, syndromic
20
mapping and self-assessment of the patients. The Government of Gujarat also initiated active contact tracing which was carried out by the Department of Community Medicine through a network of medical colleges across states and the data was analyzed daily at the state and municipal levels and supported key policy decisions.
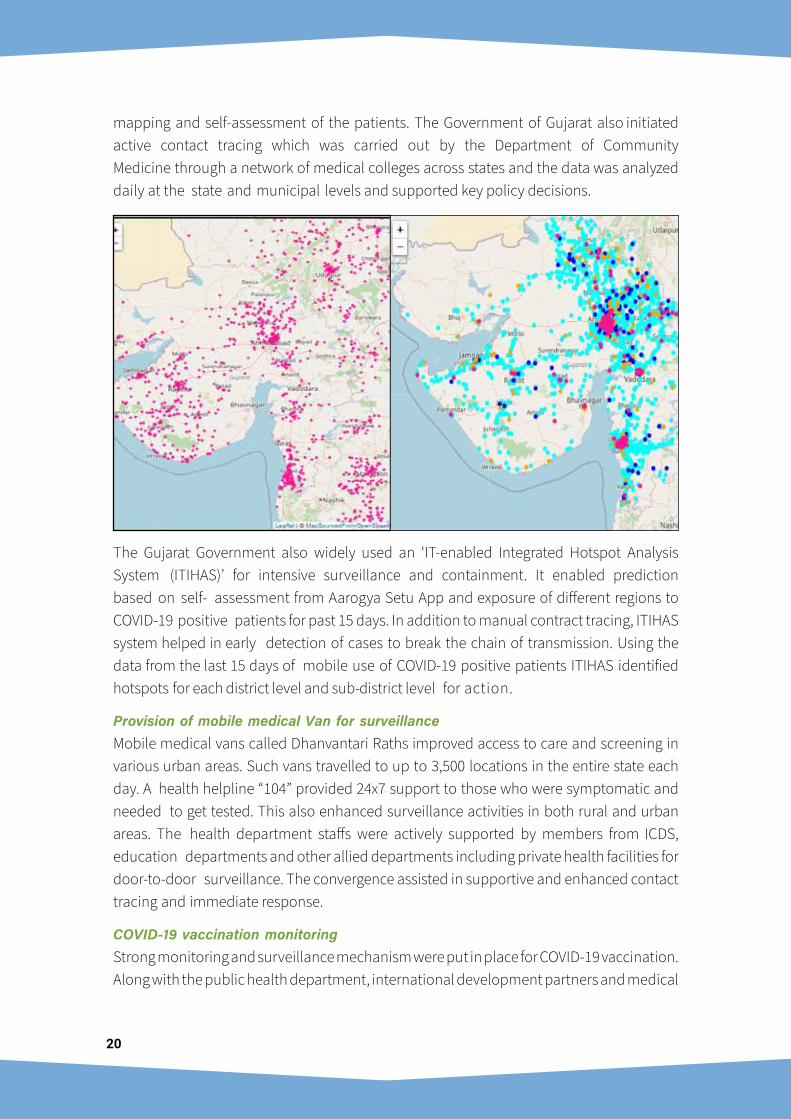
The Gujarat Government also widely used an ‘IT-enabled Integrated Hotspot Analysis System (ITIHAS)’ for intensive surveillance and containment. It enabled prediction based on self- assessment from Aarogya Setu App and exposure of different regions to COVID-19 positive patients for past 15 days. In addition to manual contract tracing, ITIHAS system helped in early detection of cases to break the chain of transmission. Using the data from the last 15 days of mobile use of COVID-19 positive patients ITIHAS identified hotspots for each district level and sub-district level for action.
Provision of mobile medical Van for surveillanceMobile medical vans called Dhanvantari Raths improved access to care and screening in various urban areas. Such vans travelled to up to 3,500 locations in the entire state each day. A health helpline “104” provided 24x7 support to those who were symptomatic and needed to get tested. This also enhanced surveillance activities in both rural and urban areas. The health department staffs were actively supported by members from ICDS, education departments and other allied departments including private health facilities for door-to-door surveillance. The convergence assisted in supportive and enhanced contact tracing and immediate response.
COVID-19 vaccination monitoringStrong monitoring and surveillance mechanism were put in place for COVID-19 vaccination. Along with the public health department, international development partners and medical
21
colleges undertook supportive supervision of the vaccine preparation, cold chain, and vaccine sessions. District and State level AEFI committees were established with a nodal center at BJ Medical College for creating enabling mechanism for surveillance, capacity building and media monitoring.
Challenges and Strategies
IDSP was adapted to the COVID-19 pandemic as conventionally, it focused more on the vector borne and diarrhoeal diseases. Implementing the new reporting formats was challenging. Staff were doing multi-tasking roles and complex micro planning along with surveillance.
Densely populated and crowded areas were also targeted for intense surveillance activities. Due to fear, persons with symptoms avoided visits to hospitals, resulting in complications and high mortality.
Due to the surge in the cases, contact tracing was very challenging. Staff burn out and deaths of healthcare workers due to COVID-19 added to mounting panic. Due to increasing case load, systematic death analysis and review was difficult.
To provide a sense of security to citizens about availability of medical services, a centralized control point was created with information on vacancy in private and government hospitals. People could also seek advice via call on 108. Daily media briefings managed to address the rumors and kept the public informed. Private hospitals were networked with referrals to major hospitals.
Recommendations
• Current pandemic management involved robust surveillance at different levels by different teams. The epidemic response mechanism starting from command and control center, early identification of warning signals, surveillance and rapid response can be further strengthened based on experiences of this pandemic.
• Existing network of IDSP may be strengthened by ensuring wider participation of private sector (including private sector labs). Consistent engagement and capacity building of the private sector may be done for reporting of key syndromes and triggers.
• AS-ITIHAS helped boost surveillance efforts. An appropriate regulatory framework will help set up a mechanism which would leverage the IT and GIS platform (like in AS-ITIHAS, IHIP) and have inter-operability with various surveillance systems run by local health departments, hospitals and laboratories.
• Leveraging the national Integrated Health Information Platform (IHIP) will help moving from aggregate based reporting to case-based reporting. Overall, surveillance systems could be targeted considering the ‘One Health’ approach and include the other key departments which can identify the possible high threat pathogen outbreaks.
22
• Death Audit is being carried out in the state. However, in the longer run there could be targeted efforts to strengthen the existing systems for capturing vital statistics including the death reviews. All-cause mortality data may be registered by utilizing the ICD reporting systems.
Pillar 4: Points of entry capacitiesIntroduction
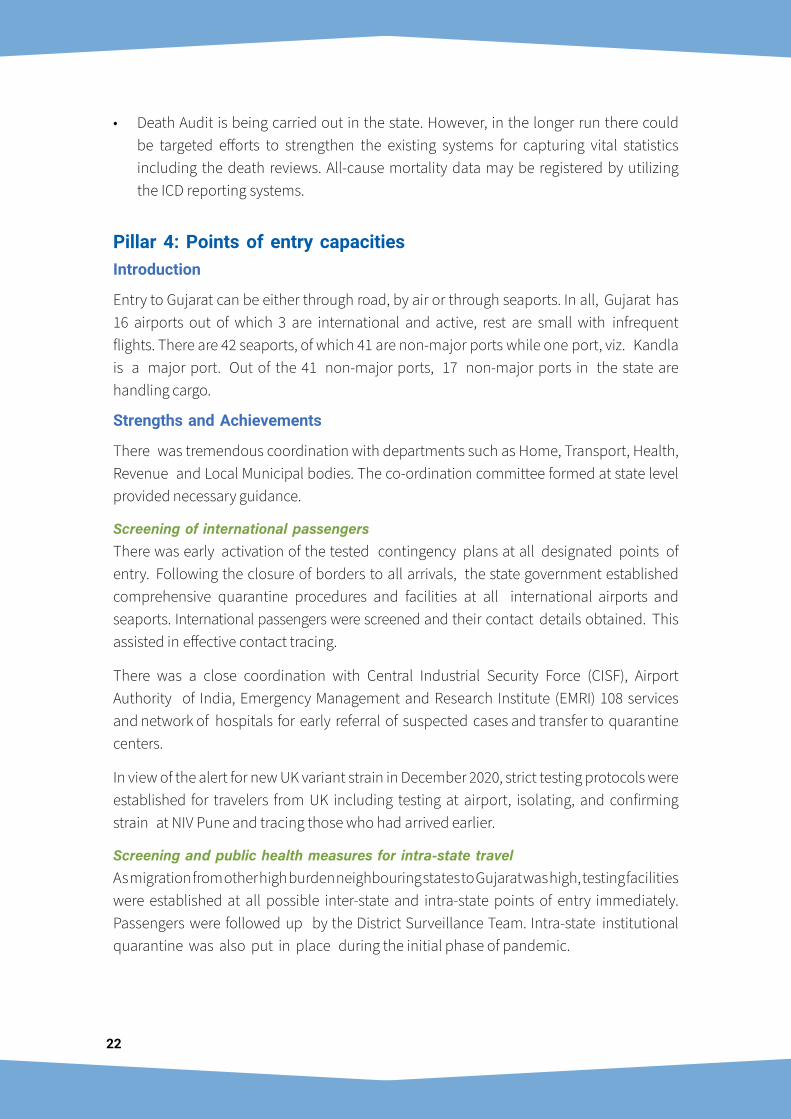
Entry to Gujarat can be either through road, by air or through seaports. In all, Gujarat has 16 airports out of which 3 are international and active, rest are small with infrequent flights. There are 42 seaports, of which 41 are non-major ports while one port, viz. Kandla is a major port. Out of the 41 non-major ports, 17 non-major ports in the state are handling cargo.
Strengths and Achievements
There was tremendous coordination with departments such as Home, Transport, Health, Revenue and Local Municipal bodies. The co-ordination committee formed at state level provided necessary guidance.
Screening of international passengersThere was early activation of the tested contingency plans at all designated points of entry. Following the closure of borders to all arrivals, the state government established comprehensive quarantine procedures and facilities at all international airports and seaports. International passengers were screened and their contact details obtained. This assisted in effective contact tracing.
There was a close coordination with Central Industrial Security Force (CISF), Airport Authority of India, Emergency Management and Research Institute (EMRI) 108 services and network of hospitals for early referral of suspected cases and transfer to quarantine centers.
In view of the alert for new UK variant strain in December 2020, strict testing protocols were established for travelers from UK including testing at airport, isolating, and confirming strain at NIV Pune and tracing those who had arrived earlier.
Screening and public health measures for intra-state travelAs migration from other high burden neighbouring states to Gujarat was high, testing facilities were established at all possible inter-state and intra-state points of entry immediately. Passengers were followed up by the District Surveillance Team. Intra-state institutional quarantine was also put in place during the initial phase of pandemic.
23
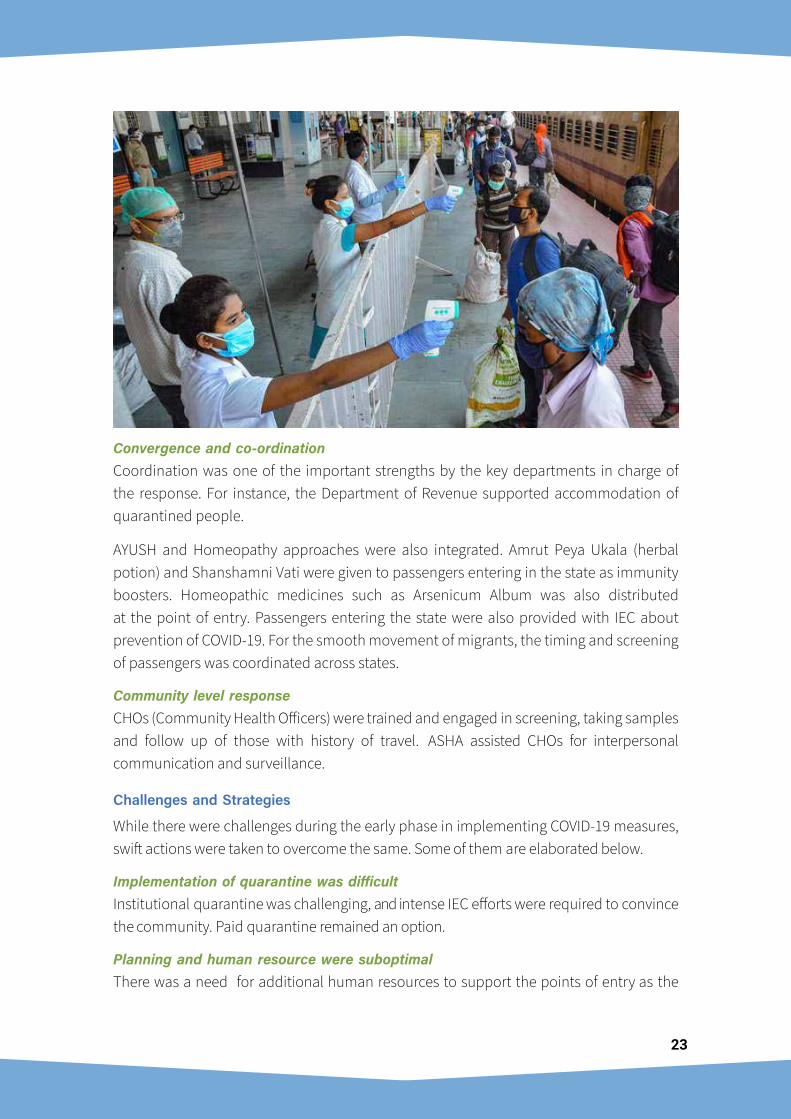
Convergence and co-ordinationCoordination was one of the important strengths by the key departments in charge of the response. For instance, the Department of Revenue supported accommodation of quarantined people.
AYUSH and Homeopathy approaches were also integrated. Amrut Peya Ukala (herbal potion) and Shanshamni Vati were given to passengers entering in the state as immunity boosters. Homeopathic medicines such as Arsenicum Album was also distributed at the point of entry. Passengers entering the state were also provided with IEC about prevention of COVID-19. For the smooth movement of migrants, the timing and screening of passengers was coordinated across states.
Community level responseCHOs (Community Health Officers) were trained and engaged in screening, taking samples and follow up of those with history of travel. ASHA assisted CHOs for interpersonal communication and surveillance.
Challenges and Strategies
While there were challenges during the early phase in implementing COVID-19 measures, swift actions were taken to overcome the same. Some of them are elaborated below.
Implementation of quarantine was difficultInstitutional quarantine was challenging, and intense IEC efforts were required to convince the community. Paid quarantine remained an option.
Planning and human resource were suboptimalThere was a need for additional human resources to support the points of entry as the
24
state has many possible entry points and in the initial phase of the pandemic, adequate health system control measures at all entry points were not in place. However, detailed planning, staffing and adequate budget support provided by the state proactively assisted in sustaining the POE activities.
Initial shortage of PPE and testing kitsInitial efforts to contain COVID-19 spread was hampered by scarcity of personal protective equipment (PPE) and testing kits. Gradually the proactive efforts by the state to provide the district officials additional financial and procurement powers eased the challenge.
Limited engagement with migrantsWith total lockdown, migrant workers and labourers could neither earn nor return to their homes. As a result, the state needed a comprehensive plan to engage and ease the sufferings of migrants. Rumors around testing, isolation of cases and quarantine of those suspected of the disease also made the task a bit difficult for the system. While there were continuous guidelines from the State, many civil society organizations, Non-Governmental Organizations and philanthropic institutions joined hands with district and local officials for optimal care, transport, and food provision for migrant workers. After the lockdown was partially lifted, some of the transportation services for migrants were initiated. The migrants underwent screening before they entered or exited any state.
Recommendations
• Risk assessment (based on traffic load, destinations covered, human or cargo traffic etc.) of all major Points of Entry (Airports, seaports, and Ground crossings) may be conducted to identify areas needing further strengthening. A roadmap for systematic investments for improvement as per IHR (2005) can be developed.
• Contingency plans at designated Points-of-Entry (PoE) can be updated, with clear roles and responsibilities of all key departments. These plans may be tested once a year through tabletop / mock exercises. Technical working group can be constituted at every designated PoE for co-ordination and interstate convergence.
• Active partnership and formal engagement with employers, civil society, NGO partners and humanitarian agencies as seen during COVID-19 migrant management may be continued to ensure that they are well covered as per various state policies.
Pillar 5: Laboratory capacities and quality assuranceIntroduction
Over a period of time, the Integrated Disease Surveillance Project (IDSP) in Gujarat has also strengthened the public health laboratories in the state at various levels in phased manner to provide diagnostic facilities for epidemic prone diseases. There is a well-

25
crafted Referral Lab Network plan already in place in Gujarat, covering all districts across Gujarat with support from Government and Gujarat Medical Education Research Society (GMERS) Medical colleges. Further to this, the government also engages with private sector labs proactively for epidemic prone diseases and to provide referral diagnostic services to the state. Before the first case in Gujarat, there was only one designated laboratory for RT-PCR testing. This was rapidly increased to 9 by March end 2020 and to 96 by March 2021 with a testing capacity of over 29,000.
Strengths and Achievements
With a strong network of the public and private laboratories under IDSP the testing capacity was increased. The state initiated active efforts to develop capacities and capabilities of both public and private laboratories set ups. Government initiated large scale testing in all Government medical colleges as well Gujarat Medical Education Research Society (GMERS) led medical colleges. Presently, a l l districts conduct either a Reverse Transcription–Polymerase Chain Reaction (RT-PCR) or Cartridge- Based Nucleic Acid Amplification Test (CBNAAT) /TrueNAT2. Samples are collected at Urban Health Centres (UHCs), Community Health Centres (CHCs), sub-district hospitals, district hospitals and medical college hospitals. The samples are then transported to the nearest laboratory. The reference labs at medical colleges are supervised and technically supported by the Department of Microbiology, who assist in training in the districts including the Rapid Response Team. Permissions were granted by the government to accredited private labs to increase the testing capacity of the state. Public-private partnerships (PPP) model improved testing.
Soon after the introduction of Rapid Antigen Test (RAT) for COVID-19, RAT kits were made available in every district which greatly increased the testing capacities. This further enabled on demand and doorstep testing up to grassroot level. Testing kiosks were setup in major cities to allow for walk in tests.
2 TrueNat is a small chip-based, portable, battery-operated device that was originally developed to detect TB.
26
Human resources were trained extensively. Centers with well trained staff and with accreditation were established as training facilities. These centers ensured that the SOPs are in place at COVID-19 testing laboratories. This included instructions for sample collection, transportation, and testing. Indian Council of Medical Research (ICMR) portal was used to manage data.
Challenges and Strategies
Public health labs needed further strengthening such as infrastructure and for vital equipment that were required for the surge in the COVID-19 samples. During the initial phase and during the lockdown there was paucity of trained and skilled manpower to assist in COVID-19 testing. As a result, manpower from other sectors and departments were deployed.
The cost of testing in private sector was high. However, the pricing was made uniform and capped to ensure affordability and avoid malpractice. More and more accredited laboratories were permitted for testing and the pricing was revised periodically. There is no Biosafety Level-3 lab in Gujarat and thus virological research could not be carried out.
Recommendations
• The existing six regional labs may be upgraded and the scope of molecular, serology and other specialized tests at district and block levels may be expanded to meet the demands of any health emergency. State-of-the-art reference laboratory at state level with advanced virology capacity can be established.
• Laboratory surge capacity plan, for an outbreak of High Threat Pathogen (HTP), may be developed.
• State laboratory networks may be expanded to involve private labs. Uniform recording formats, standards, SoPs and trainings can be adopted across all networked labs.
• Develop a laboratory surge capacity plan, for an outbreak of High Threat Pathogen (HTP).
• An advanced and exclusive Public Health Laboratory Training Centre, linked to Medical Colleges, can be setup for supporting training needs of regional and district public health laboratories including biosafety and biosecurity. It can also facilitate analysis of data for better understanding of the dynamics of local disease transmission.
• With focus on quality of care, several state labs have been accredited. A roadmap for accreditation of all labs may be planned, starting with the district level in first phase followed by others in the periphery.
27
Pillar 6: Infection prevention and controlIntroduction
The Gujarat government has been strategically investing in training of various cadres of health care provider on Infection Prevention and Control based on past experiences w i th Crimean Congo Haemorrhagic fever, avian and seasonal flu. I t imposed Section 144 of Criminal Procedure Code (CrPC) which prohibits assembly of 4 or more people in public places across all the major cities & districts like Ahmedabad, Surat, Vadodara, Rajkot, and Jamnagar even before the announcement of nationwide lockdown in late March 2020. Also, based on some previous epidemic experiences, orders were circulated for closure of malls, multiplexes, swimming pools, dance classes, gyms, clubhouses, sports complexes, and educational institutes, among others. In the initial stage of the outbreak, the state set up COVID-19 hospitals at major locations, i.e., Ahmedabad, Surat, Rajkot, and Vadodara. In Gujarat, wearing masks, hand hygiene, social distancing, travel restrictions, and facility closures have been key interventions to prevent community spread. To keep the environment clean in the hospitals wet mopping is undertaken at least twice a day by sodium hypochlorite solution. To check the sanitary conditions, round the clock Infection Control Nurse and Sanitary Inspector are available. Spitting in public was declared as a punishable offence in the state.
Strengths and Achievements
Timely issue of notification on standard precautionsNotifications were issued on standard precautions in all the areas of healthcare facilities that included hand hygiene, use of PPE to avoid direct contact with patients’ blood, body fluids, secretions (including respiratory secretions) and non-intact skin. Standard precautions also included prevention of needle-stick or sharps injury, safe waste
28
management, cleaning and disinfection of equipment, disinfection of bag housing dead body, and cleaning of the environment.
Following standard safety procedures during collection and transportation of sampleAll specimens collected for laboratory investigations were treated as potentially infectious, and health care workers who collected, or transported clinical specimens were advised to adhere rigorously to infection prevention and control guidelines and national or international regulations for the transport of dangerous and infectious substances to minimize the possibility of exposure to pathogens.
Following standard operating procedures for handling of dead bodiesBased on available guidance from the Centre, the state had developed a standard operating procedure for the disposal of dead bodies. Diseased bodies were covered in plastic body-bags and the face was kept visible through the transparent plastic cover. Municipal corporation and fire brigade departments were given charge of cremation of dead bodies in the special crematorium allocated, in some of the districts. Guidance for dead body management was strictly followed, and the risks were communicated to the family members.
Management of Bio-medical waste (BMW)The state has created – as per the Biomedical Waste Disposal guidelines and rules – colour coded drums (Yellow, Red, Black). Waste is collected twice a day as per these rules. Frequency of the waste collection increased during the pandemic. Bio-medical waste was managed in accordance with the rules. As government of India came up with amendment of BMW as per the COVID-19 status, the state government initiated refresher training, webinars and targeted IEC pertaining disposal of the BMW both in health care facility as well disposal of mask and other items generated because of home isolation and quarantine.
GIS and geo-fencing for strengthening adherence to home quarantineIn the beginning, there were instances of people violating the norms of home quarantine. To address this challenge, under the direction of the Chief Minister’s Office (CMO), the state agencies launched a Geographic Information System (GIS)-based mobile application that alerted the concerned authorities if the person under home quarantine moved away from a specific area with his or her cell phone. This application helped police authorities take notice of the violators and assist in breaking the chain of transmission and better adherence to IPC strategies in communities.
Facilitating capacity building for infection prevention and controlContinuous training was provided to the health workers. The state provided iGOT platform for the training of infection control to all the staff before joining COVID-19 duty. More than
29
9 lakh HCW registered for the training. An induction training on COVID-19 was provided to students from medical and paramedical courses. An innovative peer monitoring mechanism named buddy system to ensure optimal IPC practices were initiated in some of the COVID-19 care hospitals.
Installation of preventive care at isolation facilitiesHand washing stations were set up including alcohol-based hand sanitizer, water, soap and paper tissues at all the isolation facilities with 24/7 running tap water and charts showing six steps of hand washing techniques.
Development of standard operative procedures for different sectorsStandard Operative Procedures (SOPs) were developed by the state with the concerned stakeholders giving special attention to sej15ctors having higher capacity for spreading the virus such as diamond industries, government offices, Agriculture Produce Market Committee (APMC), textile industries, courts, and similar.
Challenges and Strategies
Increasing capacity building and delivery of information regarding IPC in short spanThe state faced an urgent need of training doctors, medical staff, paramedical staff, and attendants in a short duration. Online lectures and demonstrations supported the training of medical staff. For doctors it was difficult to manage the medical care and basic ward services as they could not take help from the relatives of patients in the case of COVID-19. To add to this was their own fears of contracting the diseases. Also, there were challenges faced in the initial period to disseminate information among all the health workers, although the state planned a series of tiered trainings.
Hesitation and fear of contacting disease made dead body disposal challengingDisposal of COVID-19 affected dead bodies posed another challenge to the administration with resistance in disposal near their areas. This needed risk communication and community engagement (RCCE). Infection among the HCWs was also challenging.
30
Encouraging and motivating the health care workersDue to risks of persistent exposure to the virus, long and intense duty hours of the HCWs in conducting testing, contact tracing and monitoring patients it was crucial to keep them encouraged and motivated. High infection levels in HCWs led to fear and discouragement in co-HCWs, thus leading to health staff shortage. For this, the state also initiated a large-scale community mobilization for appreciating the role of COVID-19 warriors. Cash incentives were offered, and any staff isolated or put under quarantine, were sent on leave with salary. Families of the health workers from Gujarat who died due to coronavirus infection in the line of duty, were paid an insurance value of INR 50 lakhs along with other welfare measures. The compensation, in the form of insurance pay-out, was paid under the Pradhan Mantri Garib Kalyan Package.
Monitoring adherence of the standard operating proceduresSOPs were issued for different operational activities and sectors such as for tea stalls, shopping malls, religious places, hotels, clubs, workplaces, yoga and gymnasium, visitors coming home and hospitality services. However, monitoring the adherence of these SOPs at all levels was challenging due to lack of adequate health staff in the local health department.
A command and control centre was established with the objective of ensuring compliance to SOPs and uniformity of patient care across all COVID-19 treating centres. CCTV and physical monitoring of Medical College and District hospital COVID-19 facilities was done to ensure that all required facilities are functioning properly and IPC procedures and patient management are followed as per guidelines
Recommendations
• Existing infection prevention and control (IPC) policy/framework can be made more comprehensive by including infrastructure, systems and capacity building. Monitoring and Evaluation of IPC practices including regular IPC audits in hospital settings may also be incorporated and practiced beyond the pandemic.
• The state has developed State Quality Assurance Standards (SQAS) on the lines of NQAS and many centres are accredited under different standards. Universally implementing quality assurance standards like SQAS, NABH, NQAS, Kayakalp will ensure better IPC practices at the health care centers.
Pillar 7: Case management & hospital preparednessIntroduction
This pillar describes actions taken to manage and care for cases, manage fatalities, as well as to share clinical information regarding cases. In addition, this pillar also documents

31
how clinicians, both public and private were involved in identification of the effective treatment for COVID-19 patients.
Strengths and Achievements
Gujarat has a strong public health care network and a long history of engagement with the private sector including Indian Medical Association (IMA), Indian Academy of Paediatrics (IAP) and Federation of Obstetrics and Gynaecological Societies of India (FOGSI). Gujarat also has a very strong private sector in addition to public sector with availability of multiple experts, facilities and treatment options. It is known as an important hub of medical tourism in the country. Even during the COVID-19 pandemic, the health system actively engaged the in- house expertise with the private sector to develop effective case management protocols and guidelines.
Development and updating of the evidence based clinical management guidelinesGujarat was one of the first states to have their own clinical treatment protocols and guidelines which was made available by the end of the March-2020 for physicians from public and private sectors. The clinical management protocols developed by the Gujarat team was endorsed by experts from premier institutes such as All India Institute of Medical Sciences (AIIMS). The Director of AIIMS New Delhi, Dr.Randeep Guleria, visited Gujarat and reviewed and endorsed the clinical protocols. . The state promoted uniform management protocol for moderate to severe cases through TAZ-HOPES-T: Thiamine, Ascorbic Acid, Zinc, Heparin, Oxygen therapy, Prone position, Eliminate exertion, Steroids, Tocilizumab.
Tele-mentoring In order to increase the capacity, ensure uniformity, discuss difficult cases and get guidance from experts, online tele-mentoring sessions were regularly conducted for all COVID-19 treating centers. State level experts discussed treatment protocols and individual cases with service providers in periphery. This was subsequently decentralized across 6 regional centres.
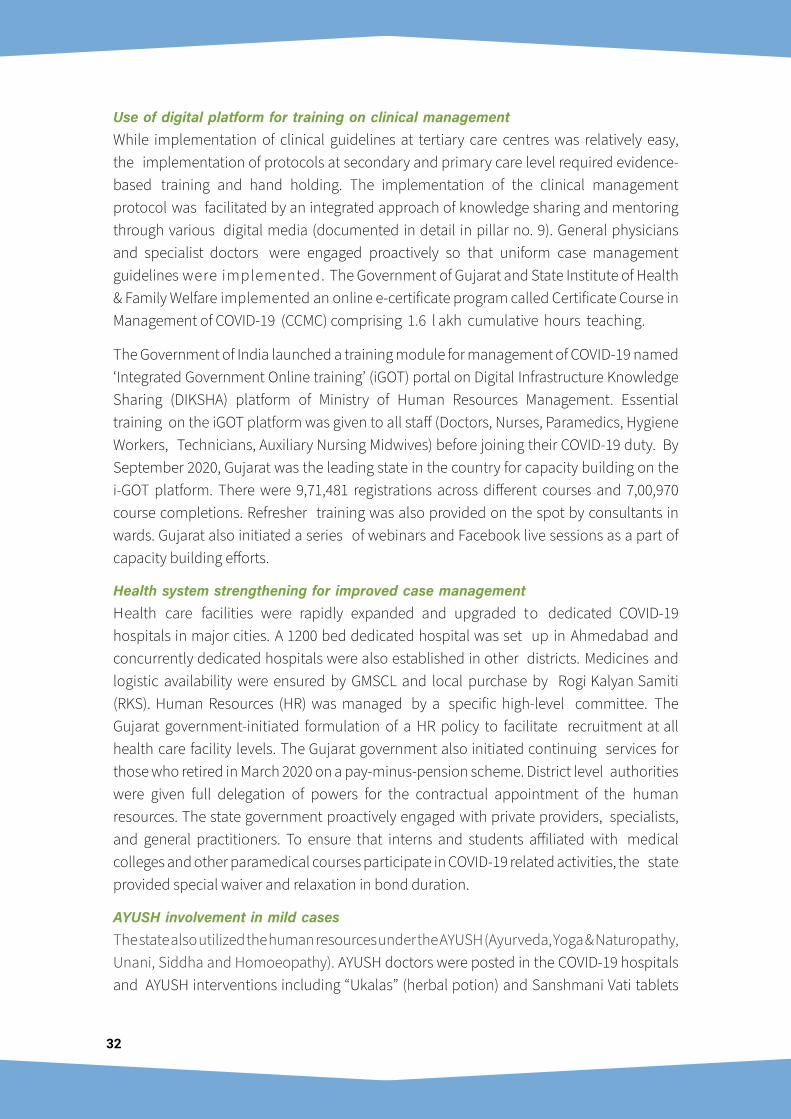
32
Use of digital platform for training on clinical managementWhile implementation of clinical guidelines at tertiary care centres was relatively easy, the implementation of protocols at secondary and primary care level required evidence-based training and hand holding. The implementation of the clinical management protocol was facilitated by an integrated approach of knowledge sharing and mentoring through various digital media (documented in detail in pillar no. 9). General physicians and specialist doctors were engaged proactively so that uniform case management guidelines were implemented. The Government of Gujarat and State Institute of Health & Family Welfare implemented an online e-certificate program called Certificate Course in Management of COVID-19 (CCMC) comprising 1.6 l akh cumulative hours teaching.
The Government of India launched a training module for management of COVID-19 named ‘Integrated Government Online training’ (iGOT) portal on Digital Infrastructure Knowledge Sharing (DIKSHA) platform of Ministry of Human Resources Management. Essential training on the iGOT platform was given to all staff (Doctors, Nurses, Paramedics, Hygiene Workers, Technicians, Auxiliary Nursing Midwives) before joining their COVID-19 duty. By September 2020, Gujarat was the leading state in the country for capacity building on the i-GOT platform. There were 9,71,481 registrations across different courses and 7,00,970 course completions. Refresher training was also provided on the spot by consultants in wards. Gujarat also initiated a series of webinars and Facebook live sessions as a part of capacity building efforts.
Health system strengthening for improved case managementHealth care facilities were rapidly expanded and upgraded to dedicated COVID-19 hospitals in major cities. A 1200 bed dedicated hospital was set up in Ahmedabad and concurrently dedicated hospitals were also established in other districts. Medicines and logistic availability were ensured by GMSCL and local purchase by Rogi Kalyan Samiti (RKS). Human Resources (HR) was managed by a specific high-level committee. The Gujarat government-initiated formulation of a HR policy to facilitate recruitment at all health care facility levels. The Gujarat government also initiated continuing services for those who retired in March 2020 on a pay-minus-pension scheme. District level authorities were given full delegation of powers for the contractual appointment of the human resources. The state government proactively engaged with private providers, specialists, and general practitioners. To ensure that interns and students affiliated with medical colleges and other paramedical courses participate in COVID-19 related activities, the state provided special waiver and relaxation in bond duration.
AYUSH involvement in mild casesThe state also utilized the human resources under the AYUSH (Ayurveda, Yoga & Naturopathy, Unani, Siddha and Homoeopathy). AYUSH doctors were posted in the COVID-19 hospitals and AYUSH interventions including “Ukalas” (herbal potion) and Sanshmani Vati tablets
33
were used for prevention and cure of mild COVID-19 cases. AYUSH interventions were also used in quarantine facilities. The state government encouraged homeopathic treatment during isolation as well as quarantine, in accordance with the Government of India guidelines for AYUSH practitioners for COVID-19.
Dhanavantari arogya rath – mobile medical vanDhanavantari Raths [see Pillar 10 for more details] – a mobile medical van with a medical officer and equipped with mini laboratory, medicine and pulse oximeter facility – were pressed into action for early identification of cases and to provide medical care at doorsteps of people. Rapid antigen testing facility was also provided inside the mobile van. By 31st March 2021, over 3,61,09, 362 subjects were screened, treatment for minor illnesses given and around 58,650 were referred to higher centres. On an average, over 1000 vans were deployed covering about 2500 sites daily. Pulse oximeter was provided to front line health workers. It was used extensively for screening which had a major role in early referrals of serious cases.
Health Care worker with Dhanvantari Rath using Pulse oximeter
Challenges and Strategies
Development of the clinical management guidelines in short timeThis being a new disease with limited scientific literature and evidence available regarding disease epidemiology, it was very challenging in the beginning. Several deliberations and discussions led to of a robust scientific evidence-based case management protocol.
Reluctance and fear of unknown amongst healthcare workersThere was an initial reluctance of the HCWs to take up duties for COVID-19 management, owing largely due to rumours and misinformation about the nature of the novel coronavirus. Human resource burnout was common due to reports of high infectivity and case fatality. To overcome staff demotivation, the government conducted several orientation
34
programmes, induction programmes and on-site trainings. There were special sessions by psychiatrists for the staff engaged in COVID-19 duties. The government also ensured adequacy of good quality PPE kits, face shields in intensive care unit (ICU), masks and gloves. Moreover, staff were put on rotational duty in non-COVID-19 wards to further boost their morale.
Tackling relatives or attendants of hospitalized patientsDuring the initial phase there were some challenges towards optimal communication to attendants and relatives of COVID-19 patients. Although help desks were available in COVID- 19 care centres, the patient’s relatives requested round the clock information regarding health status of the admitted cases. The state subsequently introduced use of a software to provide periodic updates about a patient’s condition to counsellor at the help desk, from where relatives could be apprised about their patient’s condition.
Other challengesInitially, even mild cases were also admitted to the hospital which led to a surge in the admissions in mid-April. Early discharge policy and proactive home isolation policy was developed timely which decreased load on the hospitals. There was some resistance for local quarantine and isolation, but they were resolved by involving local religious leaders and health workers. Gujarat also witnessed a few fire incidents in COVID-19 hospitals. This prompted implementation of periodic fire safety audits and mock drills in government hospitals.
Tackling post Diwali second wave of casesDespite all awareness activities, people who were at home since a long time came out in large numbers for Diwali festival shopping leading to non-adherence to preventive guidelines. This led to a significant surge of cases post Diwali and consequently scarcity in the bed capacity especially at Ahmedabad. A 400 beds new facility at a new kidney hospital campus at Manjushree mill compound and inclusion of more private facilities supported the situation. A three days’ curfew was imposed in 4 major cities followed by continued night curfew to control cases.
After the initial surge and passage of time, there were multiple reports and evidences of post- COVID-19 complication. As the epidemiology of COVID-19 is not fully understood, this poised a greater challenge and will continue to keep the health system on vigil.
Recommendations
• Developing further upon the positive experiences, the state can undertake meticulous resource and financial planning to augment capacity for combating pandemic / emergency surge at field hospital level. It should continue active engagement with private providers and evolve mechanisms for further building and sustaining these networks, including a regulatory framework for surge capacity and preparedness for any such emergencies.
35
• Tele-mentoring has aided knowledge sharing, capacity building and hand holding of the all clinicians involved in COVID-19 care across the state. This can be institutionalized and extended to other diseases of public health importance.
• Post COVID-19 clinics may be setup to manage and document long term morbidity due to COVID-19, which will also assist in further strengthening the existing body of evidence and developing guidelines.
• Practice of issuing standard treatment guidelines during COVID-19 may be institutionalized and a compendium of treatment guidelines and protocols for all notifiable diseases may be issued which gets reviewed regularly and updated in view of new evidences.
• Initiatives taken for hospital safety and hazard preparedness may be made an inclusive part of continuing medical education and training programs for healthcare cadres to efficiently deal with complex emergencies in future.
Pillar 8: Operational support & logisticsIntroduction
The COVID-19 pandemic has not only taken the lives of individuals, but also seriously crippled the economy. Growing cases and the evolving pandemic situation together with institution of public health and social measures put tremendous pressure on the supply chain of healthcare products and medical equipment like personal protective equipment (PPE), masks and pharmaceuticals. Gujarat Medical Services Corporation Limited (GMSCL) is an autonomous nodal agency for the state of Gujarat for systematic procurement and supply of drugs, equipment and diagnostic services. GMSCL initiated early procurement of PPE kits, N-95 triple layered masks through GEM (Government E-Marketplace). The state also appointed a special purchase committee to facilitate purchase and keep a check on hospital services and preparedness and conduct hospital audits.
36
Strengths and Achievements
Logistic managementThere was an increasing demand for medical equipment, ventilators, hospitals beds etc. The central government started supporting supplies of ventilators as well as PPE kits, so that the state governments can cope with the situation. Local entrepreneurs were encouraged to make triple layered masks and PPE kits. GMSCL developed a repository of technical specification of essential items / equipment that might be required for management of COVID-19 in order to ease out timely procurement.
By the end of March, around 600,000 PPE kits, 48 million triple layered masks and 4 million N95 masks were procured and distributed to various hospitals. The Gujarat government purchased about 95 high end ventilators and received about 3000 ventilators from the Government of India. GMSCL helped in distribution of ventilators and facilitated inter-hospital transfer in case of high demand of ventilators in districts like Surat, Jamnagar, and Rajkot.
Fleet managementThe GMSCL ordered special bio-safety cabinets to protect HCWs. Over-6 lakh pulse oximeters and enough rapid antigen test kits were procured.
Financial managementA ‘Khaas Kharid’ committee (High level Purchase Committee) was empowered to monitor spending as well as budget allocation. Checks and balances were followed by the market research team for quality checks of the masks, PPE kits and other equipment. The AYUSH treatment demanded purchase of 12 machines to prepare medicines, which were then procured by the same committee.
COVID-19 vaccination preparednessThe mass vaccination campaign meant that logistics and systems had to be strengthened. This was promptly done. The cold chain was strengthened to accommodate and handle the load. All the necessary logistics were made available. Alternate Vaccine Delivery systems were strengthened to ensure smooth conduction of sessions.
37
Challenges and Strategies
Manpower deficitIt has been identified that the need for more trained manpower was one of the major challenges in battling COVID-19 for the operational support. Several strategies were adopted to recruit the HR including extension of retiring staff, contracts, hiring of staff on contractual basis, transfers, and decentralizing recruitment. Enforced restrictions of movement during lockdown and containment zones led to inaccessibility of operational and logistic experts.
Ensuring medical support amidst rising cases and limited supplies in initial phaseThere was a sudden increase in the number of COVID-19 patients, who were immediately identified and isolated. Giving them adequate care was a great challenge. There was limited access to ventilators and oxygen supply. Ventilator management training was given to MBBS, Dental and AYUSH (Ayurveda, Yoga & Naturopathy, Unani, Siddha and Homoeopathy) doctors. Provision of adequate Oxygen capacity, oxygen concentrators and units was also made by the health administration.
Recommendations
• Practices like high level purchase committee, decentralization of procurement, pre- approvals for purchase of critical items, team of experts for quality check and approval may be institutionalized and practiced well beyond the pandemic.
• The state ensured surge capacity for trained HR through online trainings. This mechanism can be institutionalized and include different domains across different cadres. The state-level health and medical universities that overarches all the medical, nursing, paramedical courses should ensure optimal capacity building and coordinated response in pandemic and other eventualities.
• Healthcare infrastructure, logistics and procurement division may be strengthened financially and logistically by enabling them to garner emergency funding and support from donors and other departments.
Pillar 9: Research, innovation & knowledge sharingIntroduction
Without knowledge sharing initiatives, control of pandemic was impossible. The pandemic has resulted in large volumes of region-specific data being generated and disseminated, with the potential to impact country’s COVID-19 response in geographically diverse regions. Research, innovation, and knowledge sharing are important activities for not only understanding epidemiological trends, identifying determinants of COVID-19 disease progression and other factors but also aid effective implementation of COVID-19

38
measures, identify gaps, and synthesize lessons learned from other States or countries. The Government took numerous knowledge sharing activities based on the COVID-19 scenario in the state and complemented by policy decision and testing strategies.
Strengths and Achievements
Participation in large scale national and international trials & conducting local clinico-epidemiological researchThe state was proactive to be a part of multi-centric National and International Trials for drugs and vaccine as well. A fast track of technical and ethical permission was established for fostering the process. Several clinical trials and epidemiological studies were initiated across the state and scientific papers were published.
Permission for using innovative methods and technologiesThe Government of Gujarat was pro-active in allowing innovations by faculties from academic institutions and entrepreneurs to control COVID-19 in state. For example, the government was prompt in discussing and allowing use of I-CAD (Infection Control Assist Device), designed by an Indian doctor in the UK and facilitated by the National Initiative for Developing and Harnessing Innovations-Techno Business Incubator (NIDHI-TBI) centre at IIPHG, as a formative study in hospitals.
The government also encouraged innovative methods like ‘Advanced COVID-19 Syndromic Surveillance’, for real-time tracing of COVID-19 suspects. The system, developed by National Informatics Centre (NIC) Gujarat Unit and Gujarat Institute of Disaster Management, was expanded to 6 Districts in Gujarat is helping health workers to take necessary action like recommending further testing and hospitalization etc. It also tracked over the counter drug consumption for COVID-19 suspects.
Pathological post-mortem examination and research was started at medical college Rajkot to better understand the local pathophysiology in cases of COVID deaths.
39
Engaging private medical colleges in COVID-19 actionsThe Government initiated MoUs and dedicated COVID-19 Care Centres were established at private medical colleges for effective management of cases in the State. This also ensured that people get services free of charge. Apart from these, private hospitals were engaged in providing care services to cater the demand. Private hotels were hired to provide accommodation to healthcare staff.
Engaging medical colleges and public health institutes for health promotion and rehabilitation activitiesVarious departments of medical colleges contributed to health promotion activities at the COVID-19 Care Centres. Ayush kits were distributed to the patients and their family; yoga sessions were arranged for the patients through video conference; and television sets were provided inside the wards. Rehabilitation activities and lung exercises were facilitated by the Physiotherapy department in the Medical Colleges. Post COVID-19 Rehabilitation Care was also encouraged. IIPHG organized media interviews, scientific webinars and prepared videos for public education and knowledge sharing among technical staff and HCPs.
Challenges and Strategies
Information overload, misinformation, and rumoursThe COVID-19 pandemic generated a parallel pandemic of information overload, misinformation, and rumours. There was negative publicity of government’s preparedness, conditions of the hospitals, availability of medicines and other logistics. It was important to engage with the community with evidence-based information. But government and academic institutions made systematic effort to counter misinformation with correct scientific knowledge in simple language.
Priority settingDuring the initial phase of the outbreak, the priorities were more towards optimal treatment than research, but as the things started easing out, research and other areas also picked up.
Establishments of district knowledge cellsDistricts knowledge cells were established at the district level with an objective to assist in acceptance and reducing the resistance towards the change of new normal which includes mask and social distancing. These knowledge cells helped in upgrading the knowledge of the community. It also assisted in reducing the mass fear among people regarding the disease and denial for getting themselves tested.
Proactive engagement with researchDuring the initial phase of outbreak, the government was proactive in establishing a research committee to generate new evidence in the body of literature. A high-level
40
expert group comprising of members from the academic community, private providers and the State Health and Resource Centre was established at the state level to ensure that the evidence are collated in a systematic manner and is being shared with program managers and policy planners to ensure control of pandemic. Medical colleges and public health institutes were encouraged to take up research in different domains of COVID-19 pandemic management.
Data sharing with stakeholders including academic institutionsDuring the initial phase of the pandemic, the daily dissemination of positive cases, data on isolation and quarantine was shared with general community via media. The government was proactive in sharing the raw data collected by system for use by academic institutions. This facilitated estimation of Secondary Attack rate among household contacts for Gujarat, through primary telephone interview, by IIPHG, SHSRC and Community Medicine Departments of Medical Colleges. Essential data and locations for Geo-spatial analysis was also provided to members of academia within Gujarat. A research article on community seroconversion in Ahmedabad Municipal Corporation has been accepted for publishing by the British Medical Journal (BMJ). Several other articles topics were published in important international journals.
CoWIN portal registrationGoI introduced the CoWIN portal for registering beneficiaries and vaccine could be given only after successful registration. In the initial phase, there were some issues in the portal. To ensure smooth conduction of sessions, Surat Municipal Corporation developed a vaccine tracker system as a backup for data management in case of issues with CoWIN portal.
Recommendations
• Gujarat was one of the first states to establish a state level COVID-19 research committee with State Health System Resource Centre Gujarat as nodal agency. Institutionalizing this along with a state specific public health journal will help create an enabling environment for research and assist in undertaking, collaborating and disseminating locally relevant research.
• A COVID-19 State Task Force, composed of eminent clinicians and academicians, was constituted to support the administration in managing the pandemic. Such a mechanism can be considered as a standing taskforce for non-emergency situations as well. Eminent experts, outside government may be regularly consulted for their inputs and opinions.
• Several effective innovative approaches were adopted by the state to combat COVID-19, for ensuring continuity of essential health services viz. Dhanvantri Rath, 1100 helpline, e-Sanjeevani. These may be sustained and extended for routine care.
41
• Engagement of the public health and IT department, as during COVID-19 pandemic (AS-ITIHAS) may be institutionalized and systematic appraisal of role of health technology for generating scientific evidence, planning and service delivery may be promoted.
• A consortium of institutions of repute, from various sectors, may be instituted to engage in research on cross-cutting themes on COVID-19 and other diseases.
• Documentation of effective interventions and strategy, as through IAR, may be promoted for all public health challenges and threats. System for collaborating with eminent institutions and development partners in the state, country or abroad may be institutionalized. State specific public health newsletter and research journal can help quickly disseminate these.
Pillar 10: Maintaining essential health servicesIntroduction
When health system capacity is overburdened due to the demands of the COVID-19 outbreak, the provision of routine healthcare services tends to take a step back. Consequently, it might have an adverse impact on other essential health services.
Strengths and Achievements
Gujarat has a robust network of public healthcare facilities in rural, urban, and hard-to-reach areas. The state has pioneered functioning of Health and Wellness Centres. More than 3000 Community Health Officers were trained and placed in various health centres and have been a mainstay in providing essential health services at grass root level.
Challenges and Strategies
The fear and the lack of information around COVID-19 had an adverse impact on utilization of other essential services. There were instances where communities delayed seeking assistance for essential health services. Staff shortage was a challenge and staff burn-out was noticed over the period of time. There were some instances of challenges
42
faced by people living with HIV-AIDS (PLWHA) as they were not able to travel to the nearest Anti-Retroviral Therapy (ART) or Link Anti-Retroviral Therapy (LART) centre for drugs.
Initiate several essential health servicesInitially most of the grass root workers were engaged in the surveillance and contact tracing. Gradually, the various essential services were successfully operationalized. Immunization services were initiated in full swing by May 2020. Special efforts were made to cover those children who had missed the vaccination because of COVID-19 in both low risk as well as red zones. A revised micro plan was prepared and there was re-orientation training of the front-line workers on how to restore immunization services again.
The Mamata divas targeted for pregnant women were functional after lockdown was lifted and essential services like vaccination, IFA supplementation and referral of high-risk pregnancies were initiated. Home delivery of take-home rations (THR) as well as cooked food (Sukhadi) was also made available to the beneficiaries through Anganwadi centers.
Continuity of services were ensured especially for those requiring regular blood transfusions or dialysis. Provisions were made to ensure supply of drugs to HIV patients on Anti-Retroviral Therapy. Tuberculosis patients on treatment under the National Tuberculosis Elimination Program (NTEP) program were also ensured uninterrupted supply of drugs. The front-line workers were also instructed to keep a close contact with the enrolled patients through mobile phones to ensure treatment continuation.
Dhanavantari Arogya Raths assisted a lot in providing the essential health services at primary level across Gujarat. A micro plan was prepared for each of the routes. Each Rath used to cover 10,000 to 15,000 population per day. It was manned by a Medical Officer, Nurse and auxiliary nurse midwife (ANM). Besides providing essential health services, Dhanavantari Raths also provided lab and medicine facilities. It also focused on treatment, testing and counselling of non-communicable diseases including Hypertension and Diabetes.
“1100” helpline provided medico psychosocial support services to the general population for general medical advice and psychosocial support, follow-up of discharged patients of COVID-19 and follow-up of patients of COVID-19 on home isolation. This followed the flow of the telemedicine helpline managed by GVK-EMRI. Technological support was provided from GVK-EMRI including supervisory support whereas human resource support for operating calls and specialized services was provided by the government.
The government deputed dedicated AYUSH doctors for receiving calls and providing general health information, PHC-MOs for specialized medical advice and Psychiatrist and Clinical Psychologists for psychosocial support. Psychological issues include provisional diagnosis, e-prescription, counselling, and psychotherapy. AYUSH medical doctors are trained on Telemedicine guidelines, operation of application, and basic counselling.
43
Mental health and psychosocial careFaced with unprecedented threat and uncertainty, fear and anxiety were widespread in the community and even health care providers. It became critical to address this need alongside clinical care. Various initiatives were taken to offer essential mental health care. About 28,459 persons were counselled by counsellors whereas psychologists approximately helped 25,740 persons. Around 60 healthcare workers were counselled by psychologists posted at COVID-19 hospitals. In Rajkot, a Psychological Intervention Centre was set up at the Collectorate in association with the Saurashtra University and the Psychiatry department of the Civil Hospital, to address the psychological problems faced by people. There was a team of about 15 counsellors who were round the clock available at the call centre.
Gujarat Digital Academy developed a module on “Psychosocial Care during COVID-19 Pandemic” and have trained over 6250 personnel including Chief District Health Officer (CDHO), MO and Anganwadi workers and other medical staff to offer psychological first aid. The health department collaborated with National Institute of Mental Health and Neurosciences to provide mental health support not only for COVID-19 related issues but also were providing counselling and guidance for other mental morbidities. A total of 6000 people was trained on mental health and psychosocial care with support from UNICEF including HCWs and corona-warriors who reported symptoms of stress, anger and burnout.
Civil service organizations for extending psychosocial careLocal civil service organizations (CSOs) were engaged in supporting mental health awareness, anxiety among people, social, psychological and behavioural problems during pandemic. Around 1200 volunteers of different CSOs like Nari Niketan, Shri Sangathan and RSS Gujarat health volunteers were trained to provide psychosocial support. Around 1000 students of psychology and social work from institutions such as Maharaja Sayajirao University of Baroda, Gujarat University, National Forensic Sciences University, Kutch University, and others were trained as they are the catalyst between the professionals and community. Online yoga psycho-therapy sessions were started with the help of Kutch University and Om Foundation.
Community sensitizationThe government of Gujarat also made efforts to sensitize the community of about 104 helplines which can be accessed for essential health issues.
Telemedicine “e-Sanjeevani” programGovernment initiated e-Sanjeevani tele-consultation and e-OPD in sync with Government of India’s initiative. This is an application which various consultants such as physicians, gynecologists, surgeons, skin specialists and radiologists opted for video-consultation. Any person visiting any HWC / PHC can be connected to consultants who are sitting at the Hub in Gandhinagar.
44
Special intervention to allow HIV/TB patients follow-up servicesThe H&FW Department and Gujarat State AIDS Control Society along with the Home Department made special provision to allow people living with HIV and TB to access HIV/TB treatment care services.
Recommendations
• The state has taken an initiative to address urban health needs by rolling out urban health clinics (Deendayal clinics) for the urban poor. Further strengthening of the system through adequate technical and financial resources will help to ensure continuum of care for the marginalized urban populations and universal health coverage.
• Continuity of essential healthcare services was largely maintained during current pandemic. Mechanism to ensure the same, also involving private health providers and other sectors, may be institutionalized. It can also involve strategies for better integration of ASHA, Aanganwadi and other grassroots workers for community based delivery of essential health care including mental health services.
• Communication strategies to encourage health seeking behavior, seek timely access to essential health services and adopt healthy behaviors may be reinforced and continued.
45
The IAR was conducted by interviewing select COVID-19 officials with knowledge of health response. By reviewing the responses, best practices, stakeholder perceptions, needs and lessons learnt were documented.
The crisis induced by the pandemic was unprecedented. In the face of this challenge, Gujarat responded nimbly by learning, unlearning, relearning based on available resources and evidences. State’s response was spearheaded by a strong and committed leadership, proactive administration and a robust and resilient public health system. H’ble Chief Minister (CM), aided by a core committee of Deputy CM, cabinet members, senior bureaucrats and officials, took stock of the situation daily and also inducted several senior officers to aid Health Department in the response. A state level COVID-19 taskforce of eminent doctors and engagement with private sector provided much needed impetus. AS-ITIHAS was leveraged to identify hotspots and plan community surveillance. Stringent contact tracing and community pulse oximetry helped in early identification and preventing transmission. USP of the surveillance strategy was Dhanvantari Raths (mobile medical vans), which not only undertook symptomatic and thermal screening, pulse oximetry, rapid antigen testing in the community but also ensured continuity of essential health services during and after lockdown by providing medical care for common illnesses at doorstep. Three tiered COVID-19 care facilities were setup across all districts and beds across all categories were exponentially increased. State’s testing capacity was rapidly increased, from 9 labs in March to 91 in December. Rapid antigen tests were widely used for Walk in testing at Kiosks, on call home-based testing, mobile testing vans and across most public health facilities. Large scale online capacity building was done such that the state ranked first in the country for i-GOT based COVID-19 training. Gujarat was one of the first states to ensure access of latest drugs viz. Remdesivir and Tocilizumab in its government facilities free of cost. HFNCs and oxygen concentrators were made available. Online tele-mentoring sessions are regularly conducted for all COVID-19 treating centres for sharing knowledge and guidance. Gujarat was one of the highest users of the AYUSH formulations viz. Ayurvedic Ukala, Sanshamni Vati, Arsenicum Album; in
CONCLUSIONS AND WAY FORWARD
4

46
prevention of COVID-19. A special Inter Personal Communication toolkit was created for use by the frontline workers to effectively engage with the community and sustain the gains of the multi-pronged communication strategy. COVID-19 vaccination was effectively rolled out with 87% of the registered HCW (4.94 lakhs) and 92% of the registered FLW (5.62 lakh) being given 1st dose of vaccination by 31st March, 2021 and another 39.56 lakh comorbid and geriatric beneficiaries also received first dose.
COVID-19 has forced us to adapt to a new normal, balancing health safety with normalcy. This challenge has been a catalyst for various reforms and measures to strengthen the existing health system which will ultimately help future eventualities as well. High health literacy among people, sustained safe behaviour in community and strong health system will help combat COVID-19 and other public health emergencies. Various innovations were tried and strategies were implemented producing favourable outcomes. The resulting gains now need to be sustained. The need is to build upon the experiences, systematize and institutionalize the learnings and partnerships for a better, resilient system.
47
1. Circular of Gujarat Government to Control COVID-19, Department of General Administration, Government of Gujarat
2. Policy on Human Resource Management in Dedicated COVID-19 Facilities, Government of Gujarat
3. Directorate of Information, Government of Gujarat
4. Online resources: https://www.gidb.org/; https://gmbports.org/
REFERENCES
5
48
ANNEXURES
Intra-action review support team
Supporting MembersDr. Bharat Desai Scientist D IIPHGDr. Abid Qureshi Course Manager IIPHGMs. Khushi Kansara Research Associate IIPHGMs. Priyanka Shah Research Assistant IIPHGDr. Nikita Vadsaria Research Officer IIPHGMs. Yogini Kandre Program Associate IIPHGMs. Kalpana Pachillu PhD Scholar IIPHGDr. Priya Bhavsar Consultant IIPHGMs. Anushree Joshi PhD Scholar IIPHGDr. Farzana Memon Consultant IIPHGMs. Shweta Yadav Research Associate IIMAMr. Pratik Suthar Research Intern IIMAMr. Paresh A. Staff Member IIMADr. J. K. Kosambiya Professor, Community Medicine Government Medical College, SuratDr. Mohua Moitra Professor, Community Medicine Baroda Medical College, VadodaraDr. Shobha Misra Professor, Community Medicine PDU Medical College, RajkotDr. A. Bhagyalaxmi Professor, Community Medicine BJ Medical College, Ahmedabad
Dr. Sangeeta Patel Associate Professor, Community Medicine Baroda Medical College, Vadodara
Dr. Irfan Momin Associate Professor, Community Medicine Government Medical College, Surat
Dr. Shikha Jain Assistant Professor, Community Medicine BJ Medical College, Ahmedabad
Dr. Shailee Vyas Assistant Professor, Community Medicine Government Medical College, Surat
Dr. Kalpita Shringarpure Tutor, Community Medicine Baroda Medical College, Vadodara
Dr. Parimal Patel Tutor, Community Medicine BJ Medical College, Ahmedabad
Dr. Khushbu Makadia Tutor, Community Medicine GMERS Medical College, Himmatnagar
5

49
Acknowledgements
Name Designation
Dr. Jayanti S. Ravi Principal Secretary (HFW)
Shri Jai Prakash Shivahare Commissioner (Health)
Shri M. A. Pandya Mission Director (NHM)
Dr. Navnath Gavhane Chief Personnel Officer (CPO)
Dr. Dinkar Raval Additional Director (PH)
Dr. R Dixit Additional Director (ME)
Dr. H. K. Bhavsar Additional Director (MS)
Dr. Neelam Patel Additional Director (FW)
Dr. J. O. Madhak Director (SIHFW)
Dr. H. G. Koshia Commissioner (FDCA)
Dr. Bhavna Patel Director (AYUSH)
Dr. N. B. Dholakia Ex Additional Director (MS & FW)
Mr. Gautam Patel Policy Advisor, Gandhinagar
Mr. Adarsh PillaiLead Consultant & Director, 360 Degree Resource Solutions, Ahmedabad
Dr Roderico Ofrin WHO Representative to India
Ms. Payden Deputy Head of WHO Country Office – India
Dr. Aniket Rana WHO Surveillance Medical Officer, Ahmedabad
Dr Anoop Singh Rajput WHO Surveillance Medical Officer, Bhavanagar
Dr Vinay Kumar WHO Surveillance Medical Officer, Jamnagar
Dr Arthur Macwan WHO Surveillance Medical Officer, Panchmahal
Dr Amol Bhosale WHO Surveillance Medical Officer, Rajkot
Dr Chirag Valia WHO Surveillance Medical Officer, Surat
Dr Anand Sontake WHO Surveillance Medical Officer, Vadodara
50
List of stakeholdersSN Name Designation
1 Shri Anil Mukim Chief Secretary, GoG
2 Shri Ashish Bhatia Director General of Police, GoG
3 Shri Pankaj Kumar Additional Chief Secretary (Revenue), GoG
4 Dr. Rajiv Kumar Gupta Additional Chief Secretary (Forest & Environment), GoG
5 Shri M. K. Das Additional Chief Secretary (Industries & Mines), GoG
6 Dr. Jayanti S. Ravi Principal Secretary (Health & Family Welfare), GoG
7 Shri Manoj Aggarwal Police Commissioner, Rajkot
8 Shri Ashwini Kumar Secretary (Information & Broadcasting) & Secretary to Chief Minister, GoG
9 Ms. Sonal Mishra Secretary (Narmada), GoG & Nodal Officer (COVID-19) Surat
10 Dr. Vinod Rao Secretary (Primary & Secondary Education), GoG & Nodal Officer (COVID-19) Vadodara
11 Shri Milind Torawane Secretary (Economic Affairs) & Nodal Officer (COVID-19) Bhavnagar
12 Shri Jai Prakash Shivahare Commissioner (Health), GoG
13 Dr. Rahul Babubhai Gupta
Industries Commissioner, Gandhinagar & Nodal Officer (COVID-19) Rajkot
14 Shri Banchhanidhi Pani Commissioner, Surat Municipal Corporation, Surat
15 Shri R. B. Barad Collector and District Magistrate, Mahisagar
16 Shri Ravi Shanakar Collector and District Magistrate, Jamnagar
17 Ms. Remya Mohan Moothadath Collector & District Magistrate, Rajkot
18 Shri M. A. Pandya Mission Director (National Health Mission - Gujarat)
19 Shri Dhaval Patel Collector & District Magistrate, Surat
20 Shri Udit Agrawal Commissioner, Rajkot Municipal Corporation, Rajkot
21 Shri Ashish Kumar District Development Officer, Anand
22 Ms. Neha Kumari District Development Officer, Mahisagar
23 Dr. Navnath Gavhane Chief Personnel Officer, Commissionerate of Health, GoG

51
SN Name Designation
24 Shri J. D. Desai Former Mission Director (National Health Mission - Gujarat)
25 Dr. Dinkar Raval Additional Director (Public Health)
26 Dr. R. Dixit Additional Director (Medical Education)
27 Dr. H. K. Bhavsar Additional Director (Medical Services)
28 Dr. Neelam Patel Additional Director (Family Welfare)
29 Dr J. O. Madhak Director (SIHFW)
30 Dr. H. G. Koshia Commissioner (Food & Drug Control Administration)
31 Dr. Bhavna Patel Director (AYUSH)
32 Dr. G. C. Patel Deputy Director (Epidemic)
33 Dr. N. P. Jani Deputy Director (Urban & Rural Health)
34 Dr. Ajesh Desai Chief Executive Officer (GMERS)
35 Dr. Pranay Shah Dean, BJ Medical College, Ahmedabad
36 Dr. Pankaj Buch Medical Superintendent, PDU Government Hospital, Rajkot
37 Dr. Ragini Varma Medical Superintendent, Civil Hospital, Surat
38 Dr. J. V. Modi Medical Superintendent, Civil Hospital, Ahmedabad
39 Dr. Pina Soni Medical Superintendent, GMERS Medical College Hospital, Ahmedabad
40 Dr. Chetna Desai General Manager, Gujarat Medical Service Corporation Ltd.
41 Dr. Bina Vadalia Regional Deputy Director (Health), Gandhinagar Region
42 Dr. Rupali Mehta Regional Deputy Director (Health), Rajkot Region
43 Dr. Ajay Chauhan Program Officer (Mental Health)
44 Dr. J. K. Kosambiya Professor & Head, Community Medicine, Government Medical College, Surat
45 Dr. Nidhi Sood Professor & Head, Microbiology, PDU Medical College, Rajkot
46 Dr. Rakesh Joshi Additional Medical Superintendent, Civil Hospital, Ahmedabad
47 Dr. Bipin Amin Professor, Medicine, BJMC, Ahmedabad
48 Dr. Ami Parikh Professor, Medicine, SVP Hospital, Ahmedabad
52
SN Name Designation
49 Dr. A. Bhagyalaxmi Professor, Community Medicine, BJ Medical College, Ahmedabad
50 Dr Deepak Shukla Professor, Medicine, SMIMER, Surat
51 Dr. Tinkal Patel Professor, Medicine, Govt Medical College, Surat
52 Dr. Osman B. BelimAssociate Professor & Head, Emergency Medicine and Administrative Nodal Officer - COVID Hospital, SSGH, Vadodara
53 Dr. Nidhi Bhatnagar Associate Professor & Head, IHBT, Civil Hospital, Ahmedabad
54 Dr. Hetal Kyada Associate Professor & Head, Forensic Medicine, PDU Medical College, Rajkot
55 Dr. Prakash Patel Associate Professor, Community Medicine, SMIMER Surat
56 Dr. Mayur Jarag Associate Professor, IHBT, Govt Medical College Surat
57 Dr. Kartikey Parmar Assistant Professor, Medicine, BJ Medical College, Ahmedabad
58 Dr. Nimesh Shah Assistant Professor, Medicine, SMIMER, Surat
59 Dr. Ashish Naik Deputy Municipal Commissioner (Health & Hospital), Surat Municipal Corporation, Surat
60 Dr. Devesh Patel Medical Officer of Health, Vadodara Municipal Corporation, Vadodara
61 Dr. Pradeep Umrigar Medical Officer of Health, Surat Municipal Corporation, Surat
62 Dr. Bhavin Solanki Medical Officer of Health, Amdavad Municipal Corporation, Ahmedabad
63 Dr. Tushar Patel Critical Care Specialist & State Task force for COVID-19 member
64 Dr. Atul Patel Infectious Disease Specialist & State Task force for COVID-19 member
65 Dr. Dinesh Barot State Program Officer, Health and Wellness Cell, Gandhinagar
66 Dr. Nitesh Shah State Epidemiologist, Epidemic Cell, Gandhinagar
67 Dr. Kartik Shah State Quality Assurance Medical Officer, Gandhinagar
53
SN Name Designation
68 Dr. Lipy Shukla Medical Lecturer & Demonstrator, SIHFW, Vadodara
69 Dr. Harshad Rathod Medical Officer, Health Education Bureau, Gandhinagar
70 Dr. Umang Mishra Medical Officer, Epidemic Cell, Gandhinagar
71 Dr. Jayesh Solanki Epidemic Medical Officer, Anand
72 Dr. Birendra Singh Quality Assurance Medical Officer, Mahisagar
73 Col. Sanjay Kumar OSD, Quality, Gandhinagar
74 Dr. Chintan Patel Medical Officer, TeCHO, Gandhinagar
75 Dr. Rohan Desai Director, Plexus MD
76 Dr. Geetika Madan Director, Parul University, Waghodiya
77 Dr. Mohommed Hussain President, Baroda Muslim Doctors' Association, Vadodara
78 Shri Jitendra Jhakharia Nursing Superintendent, PDU Medical College, Rajkot
79 Shri Jashvant Prajapati Chief Operations Officer, GVK-EMRI
54
OPP. AIRFORCE HEAD QUARTERS, NR. LEKAWADA BUS STOP, LEKAWADA CRPF P.O
GANDHINAGAR , GUJARAT INDIA – 382042Web: https://iiphg.edu.in/
e-mail: [email protected] Phone: +91-079-6674 0700
World Health Organization Country Office - India R.K. Khanna Tennis Stadium, Africa Avenue,
Safdarjung Enclave, New Delhi - 110029 web: who.int/india
INDIAN INSTITUTE OF MANAGEMENT AHMEDABAD (IIMA)
Vastrapur, Ahmedabad, Gujarat 380015Web: www.iima.ac.in
e-mail: [email protected]: +91-79-7152-4427
State Health System Resource CentreFirst floor, NHM Bhavan, Civil hospital campus,
Sector 12B, Gandhinagar - 382012. Gujarat
State Health System Resource Centre GujaratG U J A R A T










![Untitled-1 []Shree Girnar Metal Industries AN ISO 9001 : 2015 Certified Company Tackle The Toughest Jobs with Quality Products Of Shree Girnar Metal Industries. Shree 0/1 Girnar Metal](https://img.pdfslide.net/doc/110x75/5f1e4b3e01e2f30fa94ac8ca/untitled-1-shree-girnar-metal-industries-an-iso-9001-2015-certified-company.jpg)