Embed Size (px)
Citation preview

So
TS
IUW
BpeaitomsldcctsenmMetBmslrmscvadfclop
ALs
GASTROENTEROLOGY 2008;134:2111–2121
tem Cell Therapy for Liver Disease: Parameters Governing the Successf Using Bone Marrow Mesenchymal Stem Cells
OM K. KUO,* SHUN–PEI HUNG,‡ CHIAO–HUI CHUANG,§ CHIEN–TSUN CHEN,� YU–RU V. SHIH,*ZU–CHING Y. FANG,¶ VINCENT W. YANG,# and OSCAR K. LEE‡,§,¶
nstitutes of *Biopharmaceutical Science, ‡Clinical Medicine, and �Biochemistry and Molecular Biology and ¶Stem Cell Research Center, National Yang-Mingniversity, Taipai, Taiwan; §Department of Medical Research and Education, Taipei Veterans General Hospital, Taipei, Taiwan; and #Department of Medicine and
inship Cancer Institute, Emory University School of Medicine, Atlanta, Georgiaotaaoavtpdeeptapbpfv
iptvtfrcmpaiib
omsfi
BA
SIC–L
IVER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
ackground & Aims: Liver transplantation is therimary treatment for various end-stage hepatic dis-ases but is hindered by the lack of donor organsnd by complications associated with rejection andmmunosuppression. There is increasing evidenceo suggest the bone marrow is a transplantable sourcef hepatic progenitors. We previously reported thatultipotent bone marrow– derived mesenchymal
tem cells differentiate into functional hepatocyte-ike cells with almost 100% induction frequency un-er defined conditions, suggesting the potential forlinical applications. The aim of this study was toritically analyze the various parameters governinghe success of bone marrow– derived mesenchymaltem cell– based therapy for treatment of liver dis-ases. Methods: Lethal fulminant hepatic failure inonobese diabetic severe combined immunodeficientice was induced by carbon tetrachloride gavage.esenchymal stem cell– derived hepatocytes and mes-
nchymal stem cells were then intrasplenically or in-ravenously transplanted at different doses. Results:oth mesenchymal stem cell– derived hepatocytes andesenchymal stem cells, transplanted by either intra-
plenic or intravenous route, engrafted recipientiver, differentiated into functional hepatocytes, andescued liver failure. Intravenous transplantation was
ore effective in rescuing liver failure than intra-plenic transplantation. Moreover, mesenchymal stemells were more resistant to reactive oxygen species initro, reduced oxidative stress in recipient mice, andccelerated repopulation of hepatocytes after liveramage, suggesting a possible role for paracrine ef-ects. Conclusions: Bone marrow– derived mesen-hymal stem cells can effectively rescue experimentaliver failure and contribute to liver regeneration andffer a potentially alternative therapy to organ trans-lantation for treatment of liver diseases.
wide variety of liver diseases lead to the impairmentof liver function and require medical intervention.
iver transplantation is the primary treatment for end-
tage hepatic diseases, with a 4-year survival rate of 70%Downloaded for Anonymous User (n/a) at National Yang-Ming UniverFor personal use only. No other uses without permission. Cop
r greater for most clinical indications.1,2 Although effec-ive, extensive clinical application is limited by the lack ofvailability of donor organs. Other adverse factors suchs rejection, problems associated with the long-term usef immunosuppressants, and perioperative morbiditynd mortality contribute to additional complications.3 Iniew of these shortfalls, cell-based hepatocyte transplan-ation is of particular interest and believed to hold greatromise because of the simpler and less invasive proce-ure. A single donor could serve multiple recipients, andxcess cells could be cryopreserved for future use.4 How-ver, studies have shown that less than 20%–30% of trans-lanted hepatocytes survive upon transplantation andhat multiple transplantation procedures are required tochieve meaningful liver repopulation.5 Furthermore, therocurement of transplantable hepatocytes is hamperedy the paucity of cadaveric liver, the limited replicativeotential, the concomitant loss of characteristic hepaticunctions upon in vitro culture, and reduced numbers ofiable and functional cells upon cryopreservation.6,7
There is increasing evidence in the literature suggest-ng bone marrow as a transplantable source of hepaticrogenitors.8 –10 However, which cell populations withinhe bone marrow hold clinical promise remains contro-ersial. Initial reports of the hepatic potential of hema-opoietic stem cells were later shown to have resultedrom fusion between transplanted donor cells and theesident recipient hepatocytes.11–13 Mesenchymal stemells (MSCs) are a stem cell population within the bonearrow that has been shown to have increasing thera-
eutic potentials in a wide range of diseases.14 –18 MSCsre defined as plate-adhering, fibroblast-like cells possess-ng self-renewal ability with the capacity to differentiatento multiple mesenchymal cell lineages such as osteo-lasts, chondrocytes, and adipocytes. MSCs are readily
Abbreviations used in this paper: B2M, �2-microglobulin; FACS, flu-rescence-activated cell sorting; FHF, fulminant hepatic failure; MDH,esenchymal stem cell–derived hepatocyte; MSC, mesenchymal
tem cell; NOD-SCID, nonobese diabetic severe combined immunode-cient; ROS, reactive oxygen species.
© 2008 by the AGA Institute0016-5085/08/$34.00
doi:10.1053/j.gastro.2008.03.015
sity from ClinicalKey.com by Elsevier on April 16, 2020.yright ©2020. Elsevier Inc. All rights reserved.

aubsilpsmlgmttitda
dtsp
baVcabpcip
cUAoGmaCta
cu
g(2sAbl
nvsw
tmwiba1fmsgaaamsl0
crgptit1fo1trMscc
BA
SIC–LIV
ER,
PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
2112 KUO ET AL GASTROENTEROLOGY Vol. 134, No. 7
vailable from a variety of tissues such as bone marrow,mbilical cord blood, trabecular bone, synovial mem-rane, and adipose tissue.19 –23 In our previous studies, wehowed that clonally derived human MSCs, under chem-cally defined conditions, differentiate into hepatocyte-ike cells that not only express liver-specific genes butossess functions of adult hepatocytes.20,24 We furtherhowed that in utero transplantation of human MSCs in
ice contributed to numerous tissues, including theiver.25 Subsequently, others have shown the hepatic en-raftment of transplanted MSCs using sublethal animalodels of liver injury, further signifying the clinical po-
ential of MSCs in the treatment of liver diseases.26,27 Inhis study, we critically analyzed the parameters govern-ng the success of using bone marrow– derived MSCs forreatment of liver disease, including the cell type and cellose for transplantation and the route of administrationnd compared their effects on functional recovery.
Materials and MethodsDetails of the materials and methods used are
escribed in the supplementary material (see supplemen-ary material online at www.gastrojournal.org). A briefummary of the animal model and cells used for trans-lantation is given in the following text.
CellsThe isolation and characterization of MSCs from
one marrow was as reported previously24,28 and waspproved by the institutional review board of the Taipeieterans General Hospital. MSCs used in this study werelonally derived, and their surface immune phenotypend multilineage differentiation potentials into osteo-lasts, adipocytes, chondrocytes, and hepatocytes werereviously characterized.24,28 For generation of mesen-hymal stem cell– derived hepatocytes (MDHs), hepaticnduction was performed for 3 weeks using the 2-steprotocol that we previously reported.24
Animal ModelNonobese diabetic severe combined immunodefi-
ient (NOD-SCID) mice were purchased from Tzu Chiniversity Laboratory Animal Center (Hualien, Taiwan).ll animal experiments were performed with the approvalf the Animal Care Committee of the Taipei Veteranseneral Hospital. Carbon tetrachloride was dissolved inineral oil at 10% concentration and administered to
nimals by gavage. Dosages between 0.2 and 0.4 mLCl4/kg body wt were tested for hepatotoxicity and le-
hality. Transplants were performed at 24 hours afterdministration of CCl4.
Preparation of Liver Cell SuspensionLiver tissues were minced in collagenase buffer
ontaining 3 mg/mL collagenase for 40 minutes at 37oC
nder gentle agitation. Cells were collected by centrifu- tDownloaded for Anonymous User (n/a) at National Yang-Ming UniverFor personal use only. No other uses without permission. Cop
ation, resuspended in fluorescence-activated cell sortingFACS) buffer, and successively passed through 23- and6-gauge needles and a 40-�m cell strainer to yield aingle cell suspension. Red blood cells were removed byCK lysing buffer. Cell viabilities were �93% by trypanlue dye exclusion, and total cells produced from each
iver was consistently greater than 5 � 107.
Statistical AnalysisData are presented as mean � SD of n determi-
ations as indicated in the figure legends. Animal sur-ival was analyzed by log-rank tests, and P values are ashown. All other data were analyzed by paired t test,here P � .05 was considered significant.
ResultsMSCs and MDHs Rescue Lethal FulminantHepatic FailureThe lethality of CCl4 on NOD-SCID mice was
ested by gavage. We determined that doses at �0.24L/kg body wt could not induce sufficient lethality,hile doses at �0.32 mL/kg body wt elicited hyperacute
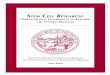
njuries leading to rapid death. A dose of 0.28 mL/kgody wt was deemed optimal, resulting in lethality in allnimals at 6 days after administration of CCl4 (FigureA). All subsequent experiments were therefore per-ormed at this dose. Biochemical assays showed a dra-
atic elevation in the serum levels of marker proteinsuch as serum glutamyl oxaloacetic transaminase, serumlutamyl pyruvic transaminase, albumin, total bilirubin,nd lactate dehydrogenase, confirming the infliction ofcute extensive liver injury by CCl4 (Table 1). Postmortemnalysis showed that the presence of centrilobular sub-assive necrosis of the liver (Supplementary Figure 1; see
upplementary material online at www.gastrojournal.org)ed to hepatic failure in animals treated with a dose of.28 mL/kg body wt.
Given the clinical shortage of hepatocytes, the chemi-ally defined hepatic differentiation system we previouslyeported24 meant that large quantities of MDHs could beenerated for transplantation. To assess the therapeuticotential of MDHs, 4 different cell doses ranging be-ween 1.4 � 106 and 4.2 � 107 cells/kg body wt werentrasplenically transplanted at 24 hours after adminis-ration of CCl4. Transplantation of 1.4 � 106 and 4.2 �06 MDHs/kg body wt failed to rescue recipient animalsrom fulminant hepatic failure (FHF), while 2 of 6 and 4f 12 mice recovered from doses of 1.4 � 107 and 4.2 �07 MDHs/kg body wt, respectively (Figure 1B). Al-hough only one third of the recipients were successfullyescued by transplantation of 1.4 � 107 and 4.2 � 107
DHs/kg body wt, the results suggest that MDHs mayerve as alternative sources for cell transplantation be-ause the cell doses administered are comparable to thoseurrently used for hepatocyte transplantation into pa-
ients with FHF.29,30sity from ClinicalKey.com by Elsevier on April 16, 2020.yright ©2020. Elsevier Inc. All rights reserved.

Fowti
BA
SIC–L
IVER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
June 2008 MSC THERAPY FOR HEPATIC FAILURE 2113
igure 1. MDHs and MSCs rescue lethal FHF. (A) Effect of CCl4 on NOD-SCID mice survival at 0.2–0.4 mL/kg administered by gavage. Survival curvesf NOD-SCID mice that underwent intrasplenic transplantation with 1.4 � 106 to 4.2 � 107/kg of (B) MDHs and (C) MSCs and intravenous transplantationith 1.4 � 106 to 4.2 � 107/kg of (D) MDHs and (E) MSCs at 24 hours after administration of 0.28 ml/kg CCl4. Statistical analysis was performed by log-rank
est (intrasplenic MSC vs intrasplenic MDH: 4.2 � 107/kg, P � .0001; 1.4 � 107/kg, P � .0018; 4.2 � 106/kg, P � .0190; 1.4 � 106/kg, P � .0190;
ntravenous MSC vs intravenous MDH: 4.2 � 107/kg, P � .1380; 1.4 � 107/kg, P � .0190; 4.2 � 106/kg, P � .0047; 1.4 � 106/kg, P � .0009).Downloaded for Anonymous User (n/a) at National Yang-Ming University from ClinicalKey.com by Elsevier on April 16, 2020.For personal use only. No other uses without permission. Copyright ©2020. Elsevier Inc. All rights reserved.

two1gtbSracca(
pciwMwtwboiad
rksiefe
criotpsocsowctas
T
NPP
P
P
P
P
NI
BA
SIC–LIV
ER,
PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
2114 KUO ET AL GASTROENTEROLOGY Vol. 134, No. 7
To compare the therapeutic potential of MSCs withhat of MDHs, 1.4 � 106 to 4.2 � 107 MSCs/kg body wtere transplanted under identical conditions. Two thirdsf the animals recovered from transplantation of 1.4 �06 and 4.2 � 106 MSCs/kg body wt (4/6 mice in eachroup), and all recipients were rescued from FHF byransplantation of 1.4 � 107 and 4.2 � 107 MSCs/kgody wt (12/12 and 16/16 mice, respectively) (Figure 1C).urprisingly, transplantation of MSCs showed superiorescuing potentials than MDHs at all 4 doses (P � .05 inll cases). To attribute the rescuing effect to MSCs, re-ipient mice underwent transplantation with a fibroblastell line FS-5 at 1.4 � 107 cells/kg body wt, but allnimals died by 6 days after CCl4 administration (n � 3)results not shown).
To determine whether the route of administrationlays an important role in the therapeutic regimen, weompared the effectiveness of intravenous with that ofntrasplenic transplantation. A cell dose-dependent effectas observed from intravenous transplantation ofDHs; all animals infused with 1.4 � 106 cells/kg bodyt died of hepatic failure, 1 of 6 mice survived following
ransplantation of 4.2 � 106 cells/kg body wt, 2 of 6 miceere rescued by transplantation of 1.4 � 107 cells/kgody wt, and 4 of 6 mice recovered from transplantationf 4.2 � 107 cells/kg body wt (Figure 1D). Remarkably,
ntravenous transplantation of MSCs effectively rescuedll recipient animals from hepatic failure at all 4 cell
able 1. Liver Function Tests of NOD-SCID Mice That Were AWith MSCs, MDHs, or Placebo Control
Serum glutamylpyruvic transaminase
(IU/L)
Serum glutamyloxaloacetic transaminase
(IU/L)
ormal NOD-SCID 15 � 2.5 63 � 2.3ost CCl4 day 1 6490 � 453.7 390 � 22.5ost CCl4 day 3Placebo 497 � 35.5 387 � 20.5IS-MSC 125 � 8.62 446 � 18.9IS-MDH 104 � 7.64 667 � 19.1
ost CCl4 day 5Placebo 430 � 25.2 346 � 8.50IS-MSC 19 � 2.5 146 � 15.3IS-MDH 21 � 3.5 178 � 15.1
ost CCl4 day 7Placebo ND NDIS-MSC 17 � 3.5 27 � 4.0IS-MDH ND ND
ost CCl4 day 14Placebo ND NDIS-MSC 32 � 6.4 60 � 5.7IS-MDH ND ND
ost CCl4 day 30Placebo ND NDIS-MSC 22 � 8.5 67 � 8.3IS-MDH ND ND
OTE. Data are presented as mean � SD of 3 determinations.S, intrasplenic transplantation; ND, not done.
oses investigated (Figure 1E). Although the superior o
Downloaded for Anonymous User (n/a) at National Yang-Ming UniverFor personal use only. No other uses without permission. Cop
escuing potential of MSCs over MDHs (4.2 � 107 cells/g, not significant; P � .05 for other cell doses) wasimilar to the findings for intrasplenic transplantations,t is noteworthy that recipient survival was apparentlynhanced by intravenous compared with intrasplenic in-usions regardless of the cell type transplanted, with thexception of 4.2 � 107 and 1.4 � 107 MSCs/kg.
Transplanted Donor Cells Engraft inthe Liver and Can Differentiate IntoFunctional HepatocytesWe next investigated whether transplanted cells
an differentiate and engraft in the liver parenchyma ofecipient animals. Recipient animals that were rescued byntrasplenic transplantation of 4.2 � 107 cells/kg body wtf either MDHs or MSCs were killed at 4 weeks post-ransplantation, and histologic evaluations showed com-lete regeneration of the liver (Supplementary Figure 2A;ee supplementary material online at www.gastrojournal.rg). An antibody against human albumin that does notross-react with murine albumin (Supplementary Figure 2B;ee supplementary material online at www.gastrojournal.rg) was used to stain liver sections of rescued mice at 4eeks posttransplantation. Albeit rare, a small number of
lusters of human albumin-positive cells were found inhe perivenous region of the liver of both MDH-rescuednd MSC-rescued recipients (Supplementary Figure 2C;ee supplementary material online at www.gastrojournal.
istered 0.28 mL/kg CCl4 and Underwent Transplantation
umin (g/dL) Total bilirubin (mg/dL) Lactate dehydrogenase (IU/L)
.5 � 0.35 0.53 � 0.058 608 � 42.7
.9 � 0.25 4.3 � 0.058 2746 � 145.9
.4 � 0.17 1.6 � 0.25 1367 � 46.72
.3 � 0.32 1.4 � 0.15 1806 � 53.057 � 0.21 1.0 � 0.15 2074 � 128.0
.2 � 0.058 1.3 � 0.25 1159 � 103.4
.9 � 0.31 0.33 � 0.058 914 � 77.1
.6 � 0.25 0.40 � 0.10 1814 � 55.18
ND ND ND.0 � 0.29 0.23 � 0.058 444 � 23.9
ND ND ND
ND ND ND.5 � 0.25 0.73 � 0.058 535 � 50.7
ND ND ND
ND ND ND.7 � 0.40 0.53 � 0.058 547 � 22.3
ND ND ND
dmin
Alb
25
11
0.9
111
2
2
2
rg). To verify that transplanted donor cells had differ-
sity from ClinicalKey.com by Elsevier on April 16, 2020.yright ©2020. Elsevier Inc. All rights reserved.

etl(m4Bs4t
crpoccmchst
gpacdedsaotbda
wmppsg
Fpar , mea
BA
SIC–L
IVER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
June 2008 MSC THERAPY FOR HEPATIC FAILURE 2115
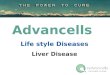
ntiated into hepatocytes, we used FACS to isolate cellshat expressed human �2-microglobulin (B2M) from theiver of recipient mice at 4 weeks posttransplantationFigure 2A) and analyzed them for expression of liver
arker genes (Figure 2B). From 3 independent FACS,.2% � 0.88% of cells in the liver were positive for human2M (a representative plot is shown in Figure 2A). Aseen, albumin, cytokeratin 18, hepatocyte nuclear factor, �1-antitrypsin, cytochrome P450, and glutamine syn-hetase were detected by Western blotting (Figure 2B).
Previous studies have shown that transplanted stemells may acquire hepatic cell fate through cell fusionather than differentiation, leading to different inter-retations.11–13 To determine whether differentiationr fusion of transplanted cells with recipient hepato-ytes was responsible for the human albumin-positiveells, a highly sensitive genomic DNA multiplex poly-erase chain reaction capable of detecting a single
opy of mouse B2M gene among 100,000 copies ofuman B2M gene25 was set up, and human B2M-orted cells were amplified by polymerase chain reac-
igure 2. Transplanted donor cells engraft recipient liver and differentiosttransplantation of MSCs (MSC-Tx). Human B2M-sorted cells (hB2nd (C) verified for their human origin by genomic DNA polymerase chainescued by MSC transplantation (enzyme-linked immunosorbent assay
ion to detect the presence of human and mouse r
Downloaded for Anonymous User (n/a) at National Yang-Ming UniverFor personal use only. No other uses without permission. Cop
enomic DNA. In all 3 independent FACS samples, theresence of human DNA was consistently found in thebsence of mouse DNA (Figure 2C), indicating that theells were human in origin. While our data do notefinitively exclude the occurrence of cell fusionvents, they nevertheless show that human MSCs canifferentiate into hepatocytes independent of cell fu-ion. To further show the functionality of differenti-ted cells, sera fractionated from the peripheral bloodf rescued animals were quantified for the concentra-ion of human albumin by enzyme-linked immunosor-ent assay (Figure 2D). The results show that donor-erived hepatocytes were capable of secreting humanlbumin into the serum.
To evaluate the degree of recovery of the recipient liver,e performed 60% partial hepatectomy on recipient ani-als that were rescued from FHF at 4 weeks after trans-
lantation of MSCs. Animals were killed at 3 weeksostoperation, and approximately two thirds of the tis-ue mass removed was regained through compensatoryrowth (not shown), indicating that the livers of MSC-
to hepatocytes. (A) FACS for human B2M-expressing cells at 4 weeksere (B) analyzed for expression of liver marker genes by Western blot
ion. (D) Detection of human albumin in the peripheral blood of recipientsn � SD of 3 determinations).
ate inM�) wreact
escued mice were extensively regenerated.
sity from ClinicalKey.com by Elsevier on April 16, 2020.yright ©2020. Elsevier Inc. All rights reserved.

BA
SIC–LIV
ER,
PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
2116 KUO ET AL GASTROENTEROLOGY Vol. 134, No. 7
Downloaded for Anonymous User (n/a) at National Yang-Ming University from ClinicalKey.com by Elsevier on April 16, 2020.For personal use only. No other uses without permission. Copyright ©2020. Elsevier Inc. All rights reserved.

r01cBcatAfadn
srcTtsmv
mPrfeatWoWbtlipdhsFg
lcazdns(ssmisadta(o
pffbdootsw
MoseCraraaro
4FvC��M�
BA
SIC–L
IVER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
June 2008 MSC THERAPY FOR HEPATIC FAILURE 2117
Engraftment frequencies of transplanted donor cells inecipient liver at 4 weeks posttransplantation (4.2% �.88%) is in line with reports in the literature that only%–3% of the host liver is readily repopulated by donorells following a single session of cell transplantation.31
y 3 months posttransplantation, human B2M-positiveells were below the sensitivity of detection, and thus wedapted a real-time genomic DNA polymerase chain reac-ion–based approach previously reported in the literature.32
lthough human cells were detectable by this approach,requencies were estimated to be 0.001%–0.01% in the livert both 3 and 6 months posttransplantation, conceivablyue to the dilution of donor-derived cells as a result oformal tissue turnover.
MSCs Possess Greater Resistance toOxidative StressWe initially hypothesized that MDHs may offer
pontaneous functional support and expedite recovery ofecipient animals but, on the contrary, rescuing frequen-ies were vastly enhanced by transplantation of MSCs.he ability to rescue recipient animals in such a short
ime, together with the reduced cell dose requirement,uggests that rescue of FHF by MSCs was not primarily
ediated by differentiation of transplanted cells but in-olved other mechanisms.
The hepatotoxic effects of CCl4 are dependent on itsetabolic activation in the liver by the cytochrome
450 – dependent monooxygenase system to reactive freeadicals.33,34 Transplanted cells must withstand the un-avorable microenvironment to endow their therapeuticffects. Given that MSCs do not exhibit cytochrome P450ctivity, the supplementation of CCl4 under in vitro cul-ure would not recapitulate the in vivo oxidative effects.
e assessed the effect of oxidative stress on the survivalf MDHs and MSCs using a potent oxidant, paraquat.hile the viability of MDHs was seemingly less affected
y paraquat-induced oxidative stress under short-termreatment, MSCs exhibited greater resistance under pro-onged treatment and the difference in viability becamencreasingly evident with increasing concentrations ofaraquat (Figure 3A). The differential resistance to oxi-ative stress was further confirmed by treatment withydrogen peroxide (Figure 3B) and by directly generatinguperoxide anions under in vitro culture (Supplementaryigure 3A; see supplementary material online at www.astrojournal.org).
™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™igure 3. MSCs are more resistant to oxidative stress than MDHs. Eiability of MSCs and MDHs (mean � SD of 3 determinations). (C) BasauZnSOD, copper/zinc superoxide dismutase; MnSOD, manganese suChange in expression of antiapoptotic genes (D) Bcl-2 and (E) Bcl-xLSD of 3 determinations). (F) Changes in reduced glutathione/oxidize
DHs at 24 hours after administration of 0.28 mL CCl4/kg (mean � SD
.05 was considered significant. *Statistical significance (D–F).Downloaded for Anonymous User (n/a) at National Yang-Ming UniverFor personal use only. No other uses without permission. Cop
The prominent resistance to oxidative stress was be-ieved to be attributed to enhanced reactive oxygen spe-ies (ROS)-scavenging potentials of MSCs over MDHs,nd we investigated the expression of antioxidative en-ymes in these cells. While basal expression of mitochon-rial-specific manganese superoxide dismutase was sig-ificantly higher in MDHs, the cytosolic copper/zincuperoxide dismutase was found to be higher in MSCsFigure 3C), suggesting that MSCs have an inherentlytronger potential to scavenge ROS entering the cytosolicpace from the microenvironment. Another possible
echanism conferring resistance to environmental stresss mediated through antiapoptotic programs. Indeed, re-ults in Figure 3D and E show that expression of anti-poptotic genes Bcl-2 and Bcl-xL, respectively, was moreramatically up-regulated in MSCs than in MDHs. Fur-hermore, expression of the downstream target Akt waslso up-regulated in MSCs but down-regulated in MDHsSupplementary Figure 3B; see supplementary materialnline at www.gastrojournal.org).
The greater resistance to oxidative stress and the su-erior scavenging potentials of MSCs suggest a possibleaster clearance of ROS in the recipient animal. There-ore, we investigated the change in oxidative stress in vivoy measuring the ratio of reduced glutathione to oxi-ized glutathione, where a decrease in reduced glutathi-ne/oxidized glutathione ratio indicates an increase inxidative stress. Indeed, mice that underwent transplan-ation with MSCs showed a faster reduction of oxidativetress in vivo than mice that underwent transplantationith MDHs (Figure 3F).
MSC Transplantation Enhances Repopulationof Endogenous Liver CellsTo further explore whether transplantation of
SCs protected endogenous hepatocytes from necrosisr promoted regeneration of the liver, we compared liverections from mice that underwent transplantation withither cell type and were killed at different times afterCl4 administration. Histologic evaluations of MDH-
ecipient livers at 3 days (60% � 4.8% necrosis; Figure 4And Supplementary Figure 4A; see supplementary mate-ial online at www.gastrojournal.org) and 6 days afterdministration of CCl4 (63% � 2.7% necrosis; Figure 4And Supplementary Figure 4B; see supplementary mate-ial online at www.gastrojournal.org) showed little signsf regeneration of the necrotized regions. On the other
™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™of exogenous oxidant (A) paraquat and (B) hydrogen peroxide on theression of antioxidative enzymes in MSCs and MDHs by Western blot.ide dismutase; GAPDH, glyceraldehyde-3-phosphate dehydrogenase.Cs and MDHs in the presence of exogenous oxidant paraquat (meantathione ratio in mice that underwent transplantation with MSCs anddeterminations). Statistical analysis was performed by paired t test; P
™™™ffectl exp
peroxin MSd gluof 3
sity from ClinicalKey.com by Elsevier on April 16, 2020.yright ©2020. Elsevier Inc. All rights reserved.

Ftd(CEw
BA
SIC–LIV
ER,
PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
2118 KUO ET AL GASTROENTEROLOGY Vol. 134, No. 7
igure 4. Transplantation of MSCs rescues endogenous hepatocytes. (A) Mean percentage of necrosis in the liver of recipient mice that underwentransplantation with MSCs and MDHs at 3 and 6 days after CCl4 administration (mean � SD of 10 determinations). (B) Change in the number ofonor-derived cells in the liver of recipient mice that underwent transplantation with MSCs and MDHs at 3, 5, and 7 days after CCl4 administration
mean � SD of 3 determinations). Bromodeoxyuridine incorporation in the liver of (C) MSC recipients and (D) MDH recipients at 3 and 5 days afterCl4 administration (red arrowheads, QuantumDot-labeled donor cells; blue, nuclei staining; brown nuclei, bromodeoxyuridine-labeled cells). (E)ffect of MSC and MDH coculture on the proliferation of hepatocytes after paraquat treatment (mean � SD of 3 determinations). Statistical analysis
as performed by paired t test; P � .05 was considered significant. *Statistical significance (A,B,E).Downloaded for Anonymous User (n/a) at National Yang-Ming University from ClinicalKey.com by Elsevier on April 16, 2020.For personal use only. No other uses without permission. Copyright ©2020. Elsevier Inc. All rights reserved.

httSoo4sod
l(t3Rwi7al�wtFwhMwstsmwfciprhbfp2
StatcM
di
ntatiFtprrFvtmopoeudiMsvww
ptotpuswf1entsia
1bfwoweprad
BA
SIC–L
IVER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
June 2008 MSC THERAPY FOR HEPATIC FAILURE 2119
and, necrosis of the MSC recipient liver was comparableo that of MDH recipient liver at 3 days after adminis-ration of CCl4 (63% � 4.3% necrosis; Figure 4A andupplementary Figure 4C; see supplementary materialnline at www.gastrojournal.org). Significant restorationf the necrotized tissue was observed by day 6 (31% �.1% necrosis; Figure 4A and Supplementary Figure 4D;ee supplementary material online at www.gastrojournal.rg), suggesting that MSCs enhanced repopulation by en-ogenous cells.
To further explore the fate of transplanted cells, weabeled MSCs and MDHs with fluorescent nanocrystalsQuantumDot; Invitrogen, Carlsbad, CA) and comparedhe absolute number of label-positive cells in the liver at, 5, and 7 days after administration of CCl4 by FACS.esults showed that approximately 10.5 � 103 MSCsere present within the recipient liver on day 3 and
ncreased to 24.5 � 103 and 67.0 � 103 by day 5 and day, respectively (Figure 4B). In comparison, only 5.5 � 103
nd 5.4 � 103 label-positive MDHs were detected in theiver at day 3 and day 5, respectively, and were reduced to
500 cells by day 7 (Figure 4B). These findings correlatedell with the differential resistance of MSCs and MDHs
o oxidative stress (Figure 3A and E and Supplementaryigure 3A and B; see supplementary material online atww.gastrojournal.org). Also consistent with the en-anced animal survival, intravenously transplantedSCs showed a greater number of label-positive cellsithin the recipient liver (Supplementary Figure 4E; see
upplementary material online at www.gastrojournal.org)han intrasplenic transplantation (Figure 4B). Immuno-taining for bromodeoxyuridine incorporation in these
ice showed that numerous proliferating hepatocytesere present in the liver of MSC recipients by day 3 and
urther increased by day 5 (Figure 4C, brown nuclei). Inontrast, there was a paucity of proliferating hepatocytesn MDH recipients (Figure 4D, brown nuclei). Trans-lanted QuantumDot-labeled MSCs (Figure 4C, red ar-owheads) were found localized among the proliferatingepatocytes (Figure 4C). Also consistent with the above,iochemical tests showed improved recovery of liverunctions by transplantation of MSCs over MDHs andlacebo controls, and complete recovery was achieved byweeks posttransplantation (Table 1).To explore the possible role of a paracrine effect, NOD-
CID mice– derived hepatocytes were subjected to oxida-ive stress followed by the addition of MDHs and MSCss coculture at 24 hours after treatment. Consistent withhe above, viability and proliferation of primary hepato-ytes were significantly increased by coculturing with
SCs compared with MDHs (Figure 4E).
DiscussionUsing a murine model of lethal chemically in-
uced FHF, we investigated various parameters govern-
ng the success and efficacy of using MSCs as an alter- tDownloaded for Anonymous User (n/a) at National Yang-Ming UniverFor personal use only. No other uses without permission. Cop
ative cell source to hepatocyte transplantation forreatment of liver disease. Our data show that MDHs are
potential alternative transplantable cell source for thereatment of FHF. However, transplantation of MSCsmproved the rescuing efficiency compared with MDHs.urther enhancements were accomplished by systemicransplantation compared with the intrasplenic ap-roach commonly used clinically. Although donor-de-ived hepatocytes were detected in the recipients, theeduced cell requirement and the rapidity of rescue fromHF suggest that MSC-mediated therapeutic effects in-olved mechanisms other than functional complementa-ion from direct differentiation. MSCs were found to be
ore resistant to ROS and resulted in faster reduction ofxidative stress in recipient mice. In addition, MSCsrominently stimulated hepatocyte proliferation afterxidative insult, suggesting a possible role for paracrineffects. The significance of adopting a lethal hepatic fail-re model is that it parallels more closely the clinicalemand for alternative or bridging therapies while wait-
ng for donor organs. In addition, transplantation ofSCs after establishment of extensive liver injury in this
tudy mimics the realistic time frame for medical inter-ention, such as in the case of acetaminophen overdosehere patients are typically admitted to the hospitalithin 24 hours.To date, only a few clinical studies of hepatocyte trans-
lantation for treatment of FHF have been reported inhe literature with limited degrees of success.29,30,35,36 Inne study, only 3 of 7 patients recovered from transplan-ation of fetal hepatocytes29 and, in another, survival wasrolonged between 12 and 52 days in 3 of 5 patients whonderwent transplantation with hepatocytes.30 In thesetudies, 109 to 1010 total cells were used. In our study, itas found that a single systemic transplantation of as
ew as 1.4 � 106 MSCs/kg body wt, approximating 1 �08 cells for an average adult body weight of 70 kg,ffectively rescued all recipient mice from FHF. Althoughot investigated in this study, it is conceivable that theherapeutic effects can be further enhanced by multipleessions of cell infusion, which may be required for treat-ng patients who are delayed in reporting to the hospitalnd have sustained prolonged liver injury.
Following a single session of cell transplantation, only%–3% of the normal rodent liver is repopulated readilyy donor cells.31 Our finding of donor cell engraftmentrequencies at 4 weeks post-transplantation was in lineith those previously reported. Although differentiationf some of the transplanted donor cells into hepatocytesas detected, consistent with those reported by Sato
t al26 and Aurich et al,27 the combined findings ofredominant repopulation by murine cells, the superiorescuing potential of MSCs over MDHs, as well as thebility to rescue FHF in such a short period suggest thatifferentiation of donor cells into hepatocytes was not
he primary attribute.sity from ClinicalKey.com by Elsevier on April 16, 2020.yright ©2020. Elsevier Inc. All rights reserved.

attcatacRcdssasfapr
ntteorbmfcuaietetssMaacpb
pAsibhfut
lhcuiaMcaaahrbtFp
ct1
1
1
1
1
1
BA
SIC–LIV
ER,
PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
2120 KUO ET AL GASTROENTEROLOGY Vol. 134, No. 7
A number of factors may be conceived to confer ther-peutic advantages on MSCs over predifferentiated hepa-ocytes, but survival of transplanted cells is a prerequisiteo the endowment of any regenerative effects that theells may possess. Like various other hepatotoxins, hep-totoxicity of CCl4 is mediated by oxidative damagehrough metabolic activation, producing free radicalsnd leading to lipid peroxidation, DNA damage, andellular death.33,34,37,38 The generation of high levels ofOS by CCl4 not only results in tissue damages butontinues to exert effects on the transplanted cells. Ourata showing superior resistance of MSCs to oxidativetress in vitro and in vivo seems to find support fromtudies reporting the persistence of MSCs in patientsfter myeloablation39 and is coherent with the recipienturvival curves. Although conferment of resistance wasound, principally, through the up-regulation of anti-poptotic and cell survival signals, the higher basal ex-ression of cytosolic superoxide dismutases suggests aole of MSCs in protecting against oxidative insults.
Our findings that MSCs enhanced repopulation ofecrotized tissue by endogenous cells rather than pro-ected cells from necrosis, as well as that in vitro cocul-ure with MSCs more significantly promoted the prolif-ration and regeneration of murine hepatocytes afterxidative injury, suggest a role for paracrine effects in theescue of FHF. All cells are known to secrete variousioactive molecules, and it has been documented thatultipotent MSCs synthesize a wide variety of growth
actors and cytokines, exerting a paracrine effect on localellular dynamics.40,41 Such trophic effects include stim-lation of revascularization, leading to measurable ther-peutic benefits in animal models of stroke, myocardialnfarction, and renal failure, irrespective of direct differ-ntiation of transplanted cells into lineages of the respec-ive tissues.42,43 Such trophic effects are also conceived tonhance endogenous cell proliferation and revasculariza-ion of the liver in our model. As cells proceed toward apecific lineage phenotype, the quantity and array ofecreted bioactive factors change,41 and it is likely that
DHs have reduced production of stimulatory factorsnd increased production of molecules primarily associ-ted with liver functioning. The contribution of para-rine effects is further supported by a recent study re-orting the therapeutic benefit of using MSC-derivediomolecules for treatment of acute liver injury.44
Earlier studies have reported that transplanted hemato-oietic stem cells are capable of repopulating the liver.45
lthough functional recovery of the liver was achieved inelected animal models of inherited metabolic liver disease,t was later shown that the effect was mediated by fusionetween the transplanted donor cells and the recipientepatocytes,12,13 and it remains undetermined whether the
requency of such events is sufficient for realistic clinicalse. In addition, diseases resulting from extensive damage
o the liver, such as chemical- or viral-induced hepatitis, mayDownloaded for Anonymous User (n/a) at National Yang-Ming UniverFor personal use only. No other uses without permission. Cop
ack viable cells for fusion events to take place. On the otherand, MSCs are extrahepatic stem cells that are easily ac-essible from a variety of postnatal tissues and can contrib-te to liver regeneration, which makes MSCs an outstand-
ng source for transplantation and offers a novel therapy forcute liver diseases. However, it remains to be seen whetherSC transplantation will be effective for treatment of
hronic liver diseases of different etiologies. It could benticipated that the paracrine effects of MSCs may alsopply to chronic conditions that are induced by drugs orlcohol, but less could be speculated of its application inepatitis arising from viral infections. Although it has beeneported by Oyagi et al that liver fibrosis could be reducedy MSC transplantation,46 suggesting potential applica-ions of MSCs in the treatment of chronic liver diseases.urther efforts are required to explore the effect of variousarameters in different disease models.
Supplementary Data
Note: To access the supplementary material ac-ompanying this article, visit the online version of Gas-roenterology at www.gastrojournal.org, and at doi:10.053/j.gastro.2008.03.015.
References
1. Keeffe EB. Liver transplantation: current status and novel ap-proaches to liver replacement. Gastroenterology 2001;120:749–762.
2. Lee LA. Advances in hepatocyte transplantation: a myth becomesreality. J Clin Invest 2001;108:367–369.
3. Ott M, Schmidt HH, Cichon G, et al. Emerging therapies in hepa-tology: liver-directed gene transfer and hepatocyte transplanta-tion. Cells Tissues Organs 2000;167:81–87.
4. Kawashita Y, Guha C, Yamanouchi K, et al. Liver repopulation: anew concept of hepatocyte transplantation. Surg Today 2005;35:705–710.
5. Rajvanshi P, Kerr A, Bhargava KK, et al. Efficacy and safety ofrepeated hepatocyte transplantation for significant liver repopu-lation in rodents. Gastroenterology 1996;111:1092–1102.
6. Fox IJ, Roy-Chowdhury J. Hepatocyte transplantation. J Hepatol2004;40:878–886.
7. Lloyd TD, Orr S, Skett P, et al. Cryopreservation of hepatocytes: areview of current methods for banking. Cell Tissue Bank 2003;4:3–15.
8. Petersen BE, Bowen WC, Patrene KD, et al. Bone marrow as apotential source of hepatic oval cells. Science 1999;284:1168–1170.
9. Theise ND, Nimmakayalu M, Gardner R, et al. Liver from bonemarrow in humans. Hepatology 2000;32:11–16.
0. Alison MR, Poulsom R, Jeffery R, et al. Hepatocytes from non-hepatic adult stem cells. Nature 2000;406:257.
1. Terada N, Hamazaki T, Oka M, et al. Bone marrow cells adopt thephenotype of other cells by spontaneous cell fusion. Nature2002;416:542–545.
2. Wang X, Willenbring H, Akkari Y, et al. Cell fusion is the principalsource of bone-marrow-derived hepatocytes. Nature 2003;422:897–901.
3. Vassilopoulos G, Wang PR, Russell DW. Transplanted bone mar-row regenerates liver by cell fusion. Nature 2003;422:901–904.
4. El-Badri NS, Maheshwari A, Sanberg PR. Mesenchymal stem
cells in autoimmune disease. Stem Cells Dev 2004;13:463–72.sity from ClinicalKey.com by Elsevier on April 16, 2020.yright ©2020. Elsevier Inc. All rights reserved.

1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
CG1
9i(m
BA
SIC–L
IVER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
June 2008 MSC THERAPY FOR HEPATIC FAILURE 2121
5. Ringden O, Uzunel M, Rasmusson I, et al. Mesenchymal stemcells for treatment of therapy-resistant graft-versus-host disease.Transplantation 2006;81:1390–1397.
6. Bunnell BA, Deng W, Robinson CM, et al. Potential application formesenchymal stem cells in the treatment of cardiovascular dis-eases. Can J Physiol Pharmacol 2005;83:529–539.
7. Minguell JJ, Erices A. Mesenchymal stem cells and the treatmentof cardiac disease. Exp Biol Med 2006;231:39–49.
8. McTaggart SJ, Atkinson K. Mesenchymal stem cells: immunobi-ology and therapeutic potential in kidney disease. Nephrology2007;12:44–52.
9. Pittenger MF, Mackay AM, Beck SC, et al. Multilineage potentialof adult human mesenchymal stem cells. Science 1999;284:143–147.
0. Lee OK, Kuo TK, Chen WM, et al. Isolation of multipotent mes-enchymal stem cells from umbilical cord blood. Blood 2004;103:1669–1675.
1. Sottile V, Halleux C, Bassilana F, et al. Stem cell characteristicsof human trabecular bone-derived cells. Bone 2002;30:699–704.
2. De Bari C, Dell’Accio F, Tylzanowski P, et al. Multipotent mesen-chymal stem cells from adult human synovial membrane. ArthritisRheum 2001;44:1928–1942.
3. Zuk PA, Zhu M, Ashjian P, et al. Human adipose tissue is asource of multipotent stem cells. Mol Biol Cell 2002;13:4279–4295.
4. Lee KD, Kuo TK, Whang-Peng J, et al. In vitro hepatic differenti-ation of human mesenchymal stem cells. Hepatology 2004;40:1275–1284.
5. Chou SH, Kuo TK, Liu M, et al. In utero transplantation of humanbone marrow-derived multipotent mesenchymal stem cells inmice. J Orthop Res 2006;24:301–312.
6. Sato Y, Araki H, Kato J, et al. Human mesenchymal stem cellsxenografted directly to rat liver are differentiated into humanhepatocytes without fusion. Blood 2005;106:756–763.
7. Aurich I, Mueller LP, Aurich H, et al. Functional integration ofhepatocytes derived from human mesenchymal stem cells intomouse livers. Gut 2007;56:405–415.
8. Lee OK, Ko YC, Kuo TK, et al. Fluvastatin and lovastatin but notpravastatin induce neuroglial differentiation in human mesenchy-mal stem cells. J Cell Biochem 2004;93:917–928.
9. Habibullah CM, Syed IH, Qamar A, et al. Human fetal hepatocytetransplantation in patients with fulminant hepatic failure. Trans-plantation 1994;58:951–952.
0. Bilir BM, Guinette D, Karrer F, et al. Hepatocyte transplantation inacute liver failure. Liver Transpl 2000;6:32–40.
1. Malhi H, Gupta S. Hepatocyte transplantation: new horizons andchallenges. J Hepatobiliary Pancreat Surg 2001;8:40–50.
2. Lee RH, Hsu SC, Munoz J, et al. A subset of human rapidlyself-renewing marrow stromal cells preferentially engraft in mice.Blood 2006;107:2153–2161.
3. Slater TF, Cheeseman KH, Ingold KU. Carbon tetrachloride toxic-ity as a model for studying free-radical mediated liver injury.Philos Trans R Soc Lond B Biol Sci 1985;311:633–645.
4. Noguchi T, Fong KL, Lai EK, et al. Specificity of a phenobarbital-
induced cytochrome P-450 for metabolism of carbon tetrachlo-Downloaded for Anonymous User (n/a) at National Yang-Ming UniverFor personal use only. No other uses without permission. Cop
ride to the trichloromethyl radical. Biochem Pharmacol1982;31:615–624.
5. Strom SC, Fisher RA, Thompson MT, et al. Hepatocyte transplan-tation as a bridge to orthotopic liver transplantation in terminalliver failure. Transplantation 1997;63:559–5569.
6. Fisher RA, Bu D, Thompson M, et al. Defining hepatocellularchimerism in a liver failure patient bridged with hepatocyte infu-sion. Transplantation 2000;69:303–307.
7. Ahmad FF, Cowan DL, Sun AY. Detection of free radical formationin various tissues after acute carbon tetrachloride administrationin gerbil. Life Sci 1987;41:2469–2475.
8. Natarajan SK, Thomas S, Ramamoorthy P, et al. Oxidative stressin the development of liver cirrhosis: a comparison of two differ-ent experimental models. J Gastroenterol Hepatol 2006;21:947–957.
9. Rieger K, Marinets O, Fietz T, et al. Mesenchymal stem cellsremain of host origin even a long time after allogeneic peripheralblood stem cell or bone marrow transplantation. Exp Hematol2005;33:605–611.
0. Haynesworth SE, Baber MA, Caplan AI. Cytokine expression byhuman marrow-derived mesenchymal progenitor cells in vitro:effects of dexamethasone and IL-1 alpha. J Cell Physiol 1996;166:585–592.
1. Caplan AI, Dennis JE. Mesenchymal stem cells as trophic medi-ators. J Cell Biochem 2006;98:1076–1084.
2. Tang YL, Zhao Q, Qin X, et al. Paracrine action enhances theeffects of autologous mesenchymal stem cell transplantation onvascular regeneration in rat model of myocardial infarction. AnnThorac Surg 2005;80:229–236.
3. Togel F, Hu Z, Weiss K, et al. Administered mesenchymal stemcells protect against ischemic acute renal failure through differ-entiation-independent mechanisms. Am J Physiol Renal Physiol2005;289:F31–F42.
4. Parekkadan B, van Poll D, Suganuma K, et al. Mesenchymal stemcell-derived molecules reverse fulminant hepatic failure. PLosOne 2007;2:e941.
5. Lagasse E, Connors H, Al-Dhalimy M, et al. Purified hematopoi-etic stem cells can differentiate into hepatocytes in vivo. Nat Med2000;6:1229–1234.
6. Oyagi S, Hirose M, Kojima M, et al. Therapeutic effect of trans-planting HGF-treated bone marrow mesenchymal cells. J Hepatol2006;44:742–748.
Received May 11, 2007. Accepted March 6, 2008.Address requests for reprints to: Oscar K. Lee, MD, PhD, Institute of
linical Medicine, National Yang-Ming University and Taipei Veteranseneral Hospital, 201, Sec 2, Shi-Pai Road, Beitou District, Taipei1221, Taiwan. e-mail: [email protected]; fax: (886) 2-28757657.Supported by the National Science Council, Taiwan (grants NSC
5-2745-B-075-002-MY3 and NSC 95-2314-B-075-014-MY2), by thentramural grant from the Taipei Veterans General Hospital, Taiwangrant V96S4-026), and by the Liver Disease Prevention and Treat-
ent Research Foundation, Taiwan.
The authors report that no conflicts of interest exist.sity from ClinicalKey.com by Elsevier on April 16, 2020.yright ©2020. Elsevier Inc. All rights reserved.

mpdfvocfeIAcbptcdcitu
wsrt
sdrmusapi
C
tm3tS
2scwptp�rbusFss
(pscbFnfGBvfvwC
�socwm7pmtcmE1hPpc
2121.e1 KUO ET AL GASTROENTEROLOGY Vol. 134, No. 7
Supplementary Materials and Methods
Cell Isolation and CultureThe isolation and characterization of mesenchy-
al stem cells (MSCs) from bone marrow was as reportedreviously.1,2 Briefly, human bone marrow was aspirateduring fracture surgeries from normal donors with in-ormed consent, and approval from the institutional re-iew board of the Taipei Veterans General Hospital wasbtained before commencement of the study. Mononu-lear cells were obtained by negative immunoselectionollowed by density gradient centrifugation and plated inxpansion medium. Expansion medium consists ofscove’s modified Dulbecco’s medium (IMDM; Sigma-ldrich, St Louis, MO) and 10% fetal bovine serum (Hy-lone, Logan, UT) supplemented with 10 ng/mL fibro-last growth factor– basic (Sigma-Aldrich), 100 Uenicillin, 1000 U streptomycin, and 2 mmol/L L-glu-amine (Sigma-Aldrich). MSCs used in this study werelonally derived, and their immunophenotype as well asifferentiation potentials into osteoblasts, adipocytes,hondrocytes, and hepatocytes were previously character-zed and reported.3 For generation of MSC-derived hepa-ocytes, hepatic induction was performed for 3 weekssing the 2-step protocol that we previously reported.3
Cell TransplantationCell transplantations and surgical procedures
ere performed under 3% isoflurane inhalation anesthe-ia. Direct intrasplenic injections were made after lapa-otomy, and systemic transplantations were made percu-aneously via the tail vein.
Partial HepatectomyFor partial hepatectomy, an upper midline inci-
ion was made from the xiphoid inferiorly and the ab-ominal cavity exposed with an Alm retractor. The ante-ior lobes to be resected were gently lifted with a
oistened cotton swab, and a silk suture was placednder the lobe proximal to the origin. The ends of theuture were tied over the lobe near the inferior vena cava,nd the lobe was resected just distal to the suture. Therocedure was performed for the anterior lobes, resulting
n approximately 60% hepatectomy.
Cell Labeling With QuantumDotsCells were labeled with QTracker585 (Invitrogen,
arlsbad, CA) as per the manufacturer’s instructions.
Preparation of Liver Cell SuspensionCells were prepared as reported previously.4 Liver
issues were minced in collagenase buffer containing 3g/mL collagenase (Sigma-Aldrich) for 40 minutes at
7oC under gentle agitation. Cells were collected by cen-rifugation, resuspended in FACS buffer (BD Biosciences,
an Jose, CA), and successively passed through 23- and WDownloaded for Anonymous User (n/a) at National Yang-Ming UniverFor personal use only. No other uses without permission. Cop
6-gauge needles and a 40-�m cell strainer (BD Bio-ciences) to yield a single cell suspension, and red bloodells were removed by ACK lysing buffer. Cell viabilitiesere �93% by trypan blue dye exclusion, and total cellsroduced from each liver were �5 � 107. For flow cy-ometry and fluorescence-activated cell sorting, cells sus-ensions were incubated with biotinylated anti-human2-microglobulin antibodies for 30 minutes at 4oC,
insed with phosphate-buffered saline, and then incu-ated with streptavidin-QDot585 conjugates for 30 min-tes at 4oC. Cells were rinsed with phosphate-bufferedaline and resuspended in FACS buffer (BD Biosciences,landers, NJ) and analyzed by FACSCalibur (BD Bio-ciences) for flow cytometry or by FACSAria for cellorting (BD Biosciences).
Total RNA Isolation and Real-Time Reverse-Transcription Polymerase Chain ReactionTotal RNA was extracted from cells using RNeasy
Qiagen, Chatsworth, CA), and reverse transcription waserformed using BD Sprint PowerScript (BD Bio-ciences). For real-time reverse-transcription polymerasehain reaction (PCR), complementary DNA was analyzedy ABI 7700 Sequence Detector (Applied Biosystems,oster City, CA). The amount of target template wasormalized by the housekeeping gene GAPDH. Primers
or GAPDH are forward CCAGGTGGTCTCCTCT-ACTTC and reverse GTGGTCGTTGAGGGCAATG; forcl-2 are forward GGCTGGGATGCCTTTGTG and re-erse CAGCCAGGAGAAATCAAACAGA; for Bcl-xL areorward CAGAGCTTTGAACAGGTAGTGAATG and re-erse TCTCAGCTTTCCACGCACAGT; for Akt are for-ard CTTCTATGGCGCTGAGATTGTG and reverseCCGGTACACCACGTTCTTC.
Western Blot AnalysisProtein concentration was determined and 20 –25
g of protein was separated on 12% sodium dodecylulfate/polyacrylamide gel electrophoresis and blottednto a polyvinylidene difluoride membrane (GE Health-are Bio-Sciences, Piscataway, NJ). Nonspecific bindingsere blocked by 3% skim milk in TBST buffer (50mol/L Tris-HCl, 150 mmol/L NaCl, 0.1% Tween 20, pH
.4). The membrane was sequentially hybridized with therimary antibody (copper/zinc superoxide dismutase andanganese superoxide dismutase, 1:5000, Upstate Bio-
echnology, Charlottesville, VA; catalase, 1:3000, Calbio-hem, San Diego, CA; GAPDH, 1:5000, Chemicon, Te-ecula, CA; albumin, 1:4000, Abcam, Cambridge,
ngland; cytokeratin-18, 1:4000, Abcam; �1-antitrypsin,:2000, Abcam; glutamine synthetase, 1:2000, Abcam;epatocyte nuclear factor 4, 1:2000, Abcam; cytochrome450 2C8/9/12/19, 1:4000, Abcam) and with horseradisheroxidase– conjugated secondary antibody (GE Health-are Bio-Sciences) at room temperature for 1 hour.
ashes were performed between incubations. Protein
sity from ClinicalKey.com by Elsevier on April 16, 2020.yright ©2020. Elsevier Inc. All rights reserved.

ic
d3(tbbAatSl
wcwttBHbma2bwhbtjstw
bhctamsGAsDgv
ba
latnrppwpgeTpaGC
e�ImmoriaMaeiwattp�wvhcmaMts
June 2008 MSC THERAPY FOR HEPATIC FAILURE 2121.e2
ntensity was determined with enhanced chemilumines-ence reagent (PerkinElmer, Wellesley, MA).
Histologic and Immunofluorescence AnalysisTissues were fixed in 3.7% formaldehyde, dehy-
rated, embedded in paraffin blocks, and sectioned at– 4 �m. For histology, sections were stained with H&ESigma-Aldrich). For immunofluorescence staining, sec-ions were blocked with 5% goat serum in phosphate-uffered saline (Sigma-Aldrich) and sequentially incu-ated with mouse anti-human albumin antibody (Sigma-ldrich) and with Cy3-conjugated goat anti-mousentibody (Sigma-Aldrich). Washes were performed be-ween incubations. Imaging was performed with thePOT RT Imaging System (Diagnostic Instruments, Ster-
ing Heights, MI) under an epifluorescence microscope.
Bromodeoxyuridine Incorporation andImmunohistochemical AnalysisBromodeoxyuridine (BrdU) dissolved in saline
as injected into mice intraperitoneally at 12 hours afterell transplantation. BrdU was injected at 50 mg/kg bodyt twice daily up to the time the mice were killed. Liver
issues were embedded in OCT compound and cryosec-ioned at 4 –5 �m. For immunohistochemical staining ofrdU, endogenous peroxidase activity was blocked with2O2 for 10 minutes at 37oC and rinsed with phosphate-
uffered saline. DNA was denatured in 2N HCl for 30inutes at 37oC, rinsed with phosphate-buffered saline,
nd then enzymatically pretreated with 0.1% trypsin for0 minutes at 37oC. Tissues were blocked for nonspecificinding by 5% goat serum in PBS and then incubatedith anti-BrdU antibody (1:1000; Sigma-Aldrich) for 2ours at 37oC, followed by biotinylated secondary anti-ody (1:1000; Sigma-Aldrich) for 40 minutes at roomemperature and with avidin/horseradish peroxidase con-ugate for 30 minutes at room temperature. Positivelytained cells were detected using 3,3=-diaminobenzidineetrahydrochloride substrate (Sigma-Aldrich). Imagingas performed with the SPOT RT Imaging System.
Genomic DNA PCRGenomic DNA was extracted from cells isolated
y fluorescence-activated cell sorting for expression ofuman �2-microglobulin using the Illustra tissue andells genomicPrep kit (GE Healthcare Bio-Sciences) as perhe manufacturer’s instructions. Total cellular DNA wasnalyzed by PCR for human- and mouse-specific �2-icroglobulin using a published method.5 Primers that
pecifically amplify human �2-microglobulin (forward:TGTCTGGGTTTCATCCATC, reverse: GGCAGGCAT-CTCATCTTTT) were selected based on the published
equence and were shown to amplify human, not mouse,NA. Primers that specifically amplify mouse �2-micro-
lobulin (forward: AGACTTTGGGGGAAGCAGAT, re-
erse: CAGTCTCAGTGGGGGTGAAT) were selected aDownloaded for Anonymous User (n/a) at National Yang-Ming UniverFor personal use only. No other uses without permission. Cop
ased on the published sequence and were shown tomplify mouse, not human, DNA.
Estimation of Cell Frequencies by Real-TimePCRFrequencies of human cells in recipient mouse
iver were estimated using a published method.6 Themount of DNA was first determined by absorbance andhen by real-time PCR for the mouse albumin gene toormalized genomic DNA. PCR assays were performed ineactions containing SYBR Green PCR Master Mix (Ap-lied Biosystems), 900 nmol/L of forward and reverserimers, and 200 ng of target template. Standard curvesere generated by serially diluting human genomic DNArepared from MSCs into samples containing 200 ng ofenomic DNA from mouse liver and bone marrow. Prim-rs for mouse DNA (forward: GAAAACCAGGCGAC-ATCTCC, reverse: TGCACACTTCCTGGTCCTCA) am-lify a specific intron sequence of the single copy serumlbumin gene. Primers for human DNA (forward: CAT-GTGAAACCCCGTCTCTA, reverse: GCCTCAGCCTC-CGAGTAG) amplify human Alu repetitive sequence.
Exogenous Oxidative Stress and Cell ViabilityAssayTo assay for cell viability in the presence of exog-
nous oxidative stress, MSCs and MDHs were seeded at 4103 cells/well in 96-well plates and serum deprived in
MDM for 2 days before the assay. Paraquat was supple-ented in IMDM at concentrations between 1 and 4mol/L, and paraquat-containing medium was replaced
n a daily basis. Cell viability was assay using MTSeagent (Promega, Madison, WI) as per manufacturer’snstructions at 0 to 5 days posttreatment with paraquat,nd readings were measured at 490 nm on a Bio-Radodel 680 microplate reader (Hercules, CA). MTS re-
gent only served as blank control, and results werexpressed as relative viability to day 0. For cell viabilitiesn the presence of hydrogen peroxide, hydrogen peroxideas added into IMDM at concentrations between 100nd 800 �mol/L and replaced daily. For cell viabilities inhe presence of superoxide anions, cells were cultured inhe presence of xanthine oxidase and xanthine was sup-lemented into medium at concentrations between 100mol/L and 1 mmol/L for 30 minutes. Cell viabilitiesere determined as described previously. For hepatocyte
iability under coculture, 2 � 105 normal NOD-SCIDepatocytes were seeded in the lower level of Transwellhambers in IMDM. On day 0, paraquat was supple-ented into IMDM at a final concentration of 4 mmol/L;
t 24 hours after addition of paraquat, 1 � 105 MDHs orSCs preseeded in Transwell chambers were placed into
he well containing paraquat-treated hepatocytes for sub-equent coculturing. An empty Transwell chamber served
s non-cocultured control. Viability and proliferation ofsity from ClinicalKey.com by Elsevier on April 16, 2020.yright ©2020. Elsevier Inc. All rights reserved.

Na
2gRm
2dtitwrraBw
wHm
1
2
3
4
5
6
2121.e3 KUO ET AL GASTROENTEROLOGY Vol. 134, No. 7
OD-SCID hepatocytes were determined by MTS assay,nd results were expressed as relative viabilities to day 0.
In Vivo Reduced Glutathione/OxidizedGlutathione AssayWhole blood was collected from the animals at
4-hour intervals, and reduced glutathione and oxidizedlutathione levels were determined using the GSH/GSSGatio Assay Kit (Calbiochem, San Diego, CA) as per theanufacturer’s instructions.
Albumin Enzyme-Linked Immunosorbent AssayEach well of a microtiter plate was coated with
00 �L of human albumin-specific antibody (Sigma-Al-rich) at 0.2 �g/mL for 1 hour at 37oC and washed 3imes with PBS-T. Samples were applied to the wells andncubated for 1 hour at room temperature and washed 3imes with PBS-T. Subsequently, wells were incubatedith detection antibody at 0.2 �g/mL for 30 minutes at
oom temperature and washed 3 times with PBS-T. Tet-amethylbenzidine substrate was added into each wellnd allowed to develop for 30 minutes and read on aio-Rad Model 680 microplate reader. Concentrations
ere determined against the standard curve.Downloaded for Anonymous User (n/a) at National Yang-Ming UniverFor personal use only. No other uses without permission. Cop
Image Analysis
Image analysis and the percentages of necrosisere measured using ImageJ (National Institutes ofealth). Data are presented as mean � SD of 10 deter-inations.
References
. Lee OK, Kuo TK, Chen WM, et al. Isolation of multipotent mesen-chymal stem cells from umbilical cord blood. Blood 2004;103:1669–1675.
. Lee OK, Ko YC, Kuo TK, et al. Fluvastatin and lovastatin but notpravastatin induce neuroglial differentiation in human mesenchy-mal stem cells. J Cell Biochem 2004;93:917–928.
. Lee KD, Kuo TK, Whang-Peng J, et al. In vitro hepatic differentiationof human mesenchymal stem cells. Hepatology 2004;40:1275–1284.
. Lazaro CA, Croager EJ, Mitchell C, et al. Establishment, character-ization, and long-term maintenance of cultures of human fetalhepatocytes. Hepatology 2003;38:1095–1106.
. Chou SH, Kuo TK, Liu M, et al. In utero transplantation of humanbone marrow-derived multipotent mesenchymal stem cells inmice. J Orthop Res 2006;24:301–312.
. Lee RH, Hsu SC, Munoz J, et al. A subset of human rapidlyself-renewing marrow stromal cells preferentially engraft in mice.
Blood 2006;107:2153–2161.sity from ClinicalKey.com by Elsevier on April 16, 2020.yright ©2020. Elsevier Inc. All rights reserved.


























![Mesenchymal Stem Cell Transplantation for Liver Cell Failure ...with liver cell failure. Amazingly, Okumoto et al. [21] reported that the level of stem cell factor was markedly decreased](https://img.pdfslide.net/doc/110x75/60c3e0c47b592f07ab7956cc/mesenchymal-stem-cell-transplantation-for-liver-cell-failure-with-liver-cell.jpg)