Embed Size (px)
Citation preview
British Journal of Developmental Psychology (2015), 33, 106–122
© 2014 The British Psychological Society
www.wileyonlinelibrary.com
Step by step: A microgenetic study of thedevelopment of strategy choice in infancy
Sarah E. Berger1*, Brian Chin2, Sandeep Basra3 and Hannah Kim4
1Department of Psychology, College of Staten Island and The Graduate Center of the
City University of New York, USA2Department of Psychology, Stony Brook University, Stony Brook, New York, USA3Department of Psychology, University of Westminster, London, UK4Department of Psychology, The Graduate Center of the City University of NewYork, USA
To examine patterns of strategy choice and discovery during problem-solving of a novel
locomotor task, 13.5- and 18-month-old infants were placed at the top of a staircase and
encouraged to descend. Spontaneous stair descent strategy choices were documented
step by step and trial by trial to provide a microgenetic account of problem-solving in
action. Younger infants tended to begin each trial walking, were more likely to choose
walking with each successive step, and were more likely to lose their balance and have
to be rescued by an experimenter. Conversely, older infants tended to begin each trial
scooting, were more likely to choose scooting with each successive step, and were
more likely to use a handrail to augment balance on stairs. Documenting problem-
solving microgenetically across age groups revealed striking similarities between
younger infants’ strategy development and older children’s behaviour on more
traditionally cognitive tasks, including using alternative strategies, mapping prior
experiences with strategies to a novel task, and strengthening new strategies. As
cognitive resources are taxed during a challenging task, resources available for weighing
alternatives or inhibiting a well-used strategy are reduced. With increased motor
experience, infants can more easily consider alternative strategies and maintain those
solutions over the course of the trial.
The field of cognitive development has recently shifted its focus from describing
stage-based changes to exploring and understanding the mechanisms underlying
change (Adolph, Robinson, Young, & Gill-Alvarez, 2008; Lemaire, 2010; Siegler, 2007).One of the most fruitful approaches has been the microgenetic analysis of variability in
how school-aged children choose and execute strategies for solving problems. In these
studies, researchers make densely timed observations as children carry out a task,
successfully or not, typically in the context of math- or school-related skills (Bull, Espy,
& Wiebe, 2008; Lemaire & Lecacheur, 2011; Lemaire & Reder, 1999; Siegler, 2007;
Tunteler & Resing, 2002). Siegler’s ‘overlapping waves theory’ lays out the
expectations for the typical development of strategy use in contexts such as
preschoolers using simple tools and grade-schoolers solving arithmetic problems (e.g.,
*Correspondence should be addressed to Sarah E. Berger, Department of Psychology, College of Staten Island, 2800 Victory Blvd.,4S-108, Staten Island, NY 10314, USA (email: [email protected]).
DOI:10.1111/bjdp.12076
106

Chen & Siegler, 2000; Lemaire & Siegler, 1995). On this account, studying within-child
variability, rather than treating it as noise, is a powerful predictor of and tool for
understanding change (Siegler, 2007). Strategy development starts with the acquisition
of new strategies, improves as novices become able to map prior experiences to noveltasks, and culminates with the strengthening of newly acquired strategies (see Chen &
Siegler, 2000, for a review).
The mechanism for change, or what prompts children to move from less to more
efficient and successful strategies, is the automatization that comes from practice. As
cognitive resources that had previously been allocated to the monitoring of strategy
execution become available, they can be reallocated to make problem-solving more
efficient, such as searching for redundancies within existing strategies (Siegler, 2000).
Moreover, as practice increases familiarity with a problem, working memory resourcescan be reallocated to the exploration of alternative strategies (Shrager & Siegler, 1998).
Conversely, a decrease in processing resources in the elderly is associated with impaired
strategy use compared to younger adults, such as less efficient performance or poor
strategy choices (Lemaire, 2010).
One limitation to the typical measurement approaches for studying strategy choice
and problem-solving has been an emphasis on verbal and mathematical problems that,
while yielding rich behavioural data sets for older children, are generally unsuitable for use
with infants (Keen, 2011). As a result, our understanding of the process of strategyacquisition in infancy lacks the level of detail that we have with older children. One
domain in which infants provide as rich behavioural data sets as older children is
locomotor development. Indeed, studies of how infants solve locomotor problems have
revealed that experts in a posture can devise alternative strategies when they encounter
situations where their typical strategies are no longer appropriate. For example, expert
cruisers can bend at thewaist or cruise on their knees to use a low handrail (Berger, Chan,
& Adolph, 2014), and expert walkers choose to crawl so they can navigate squishy
surfaces (Joh & Adolph, 2006), scoot so they can navigate steep slopes (Adolph, 1997),and turn their bodies sideways to grab a handrail so they can navigate narrow bridges
(Berger & Adolph, 2003; Berger, Adolph, & Kavookjian, 2010; Berger, Adolph, & Lobo,
2005).
The overall goal of this studywas to better understand the process of strategy choice in
young infants. As such, our first aimwas to determinewhether infants’ patterns of strategy
discovery and selection followed the same trajectory as those observed in older children
and adults. We designed a locomotor task that could provide a context for observing
development in action, particularly the emergence of problem-solving skills. Specifically,we sought to microgenetically document infants’ spontaneous stair descent strategies.
Previouswork has focusedprimarily on establishing norms forwhen infants learn to climb
stairs (Frankenburg & Dodds, 1967; Gesell, 1934; McGraw & Breeze, 1941) or the social
structures that support infants as they learn to climb stairs (Berger, Theuring, & Adolph,
2007), but we know very little about how infants independently discover new strategies
for climbing stairs (Ulrich, Thelen,&Niles, 1990).Documenting infants’ strategies literally
from step to stepwould yield a high-density sample in real time and capture changewithin
and between trials (Siegler, 1996, 2002). Based on parent reports of how infants firstlearned to descend stairs (Berger et al., 2007), we expected to observe variability in
infants’ spontaneous stair descent when stairs were presented as a novel task that would
provide a differentiated description of children’s strategy choice (Chen & Siegler, 2000;
Siegler, 1996, 2002; Wilmut & Barnett, 2011). For example, in a sample of over 300
families, parents reported that infants typically descended stairs by crawling backwards,
Development of strategy choice 107
walking while holding a banister, or scooting down in a sitting position (Berger et al.,
2007). Moreover, parents reported being actively involved in teaching their infants to
climb stairs, including manoeuvering infants’ limbs into proper position to demonstrate
descent. Allowing infants to solve the novel problem of stair descent independently andwithout constraint would create a relatively naturalistic situation, generate behaviours to
make strategy evolution observable, and circumvent the problem of studying prob-
lem-solving in a pre-verbal population (Siegler, 1996, 1998; Ulrich et al., 1990).
Unlike most motor skills acquired in the first 2 years of life, stair descent carries an
element of risk. Infants are more likely to fall down stairs than any other age group
except elderly adults over the age of 65 (National SAFE KIDS Campaign, 2004; Young,
Torner, Schmitt, & Peek-Asa, 2011). Although infants fall frequently when learning to
cruise while holding onto furniture or walk on flat ground, they do not typically incurserious injury (Adolph et al., 2012; Sugar, Taylor, & Feldman, 1999). In contrast,
approximately 73,000 children between the ages of 6 months and 2 years were
injured on stairs or steps in 2009 (U.S. Consumer Product Safety Commission, 2010).
The extended period of locomotor experience that is required before infants can
coordinate different components of a plan into a strategy or devise alternative
strategies may explain the number of injuries associated with falls on stairs, despite
parents’ best efforts to teach their children safe descent strategies (Berger et al.,
2007). Understanding infants’ strategy choice in the context of stair descent wouldnot only enhance our basic understanding of the development of decision-making in
early childhood, but may offer some practical advice to caregivers about children’s
learning to use stairs.
Our second aim was to investigate the role of expertise in strategy choice as a way to
gain insight into change mechanisms. To do so, we documented 13.5- and 18-month-old
infants’ spontaneous navigation strategies for stair descent when they were placed at
the top of a staircase and encouraged to make their way to a caregiver waiting at the
bottom. This design allowed us to investigate emerging solutions at multiple time scales:Step by step, trial by trial, and between age groups (Adolph, Robinson, et al., 2008;
Badaly & Adolph, 2008; Siegler, 1996). The stair descent task required infants to
generate a goal (reaching a parent at the bottom of a staircase), sequence the steps
necessary to obtain the goal (possibly devising alternative descent strategies for balance
control), and continually monitor their progress towards the goal (to maintain balance).
Each of these task components places a heavy demand on cognitive resources (Carrico,
2013). Moreover, younger infants would have little walking experience and little to no
stair descent experience, so for them, the motor demands of the task would also taxattentional resources (Berger, 2004, 2010; Woollacott & Shumway-Cook, 2002). To
lower their centre of gravity and increase control of balance, infants could theoretically
choose alternative descent strategies such as scooting down on their bottoms facing
forward or backing down stairs. However, despite the increased biomechanical stability
associated with these alternative descent strategies, they are not initially found in
infants’ locomotor repertoires (Adolph, Eppler, & Gibson, 1993). Infants who lack stair
descent experience simply may not perceive these strategies as possibilities for action
until they have amassed sufficient practice navigating stairs with their novice descentskills (e.g., Gibson et al., 1987; Kretch & Adolph, 2013). Examining patterns of infants’
choices and errors on the stair descent task speaks to the role of processing resources in
the development of problem-solving in infancy.
108 Sarah E. Berger et al.

Method
A subset of this data (n = 19) was collected as part of a larger study examining thedevelopment of 13-month-old infants’ ability to inhibit. In the original study, infants
descended a staircase several times before being encouraged to switch to a new staircase.
Primary outcome measures focused on the differences between pre- and post-switch
behaviours. Only data from the pre-switch trials were included in this data set. Data from
the remaining participants (thirteen 13.5-month-olds and seventeen 18-month-olds) were
collected specifically and uniquely for the current study.
Participants
Thirty-two 13.5-month-old infants (16 boys;M = 13 months, 10 days; SD = 13 days) and
seventeen 18-month-old infants (seven boys; M = 18 months, 1 day; SD = 7 days)
participated in this study. The criterion for participation was being able to walk 10 feet
(3.05 m) across the room independently without stopping or falling. We chose
13 months as the age for the younger group because at that age, most infants have
minimal to no stair descent experience and because pilot testing confirmed that stair
descent was a challenging motor task that elicited rich motor behaviours for that agegroup (Berger, 2010; Berger et al., 2007). We chose 18 months as the age for the older
group because in a previous survey of over 700 families about their infants’ navigation of
stairs, most infants had learned to descend stairs between 17 and 20 months (Berger
et al., 2007). Families were recruited via a purchased commercial mailing list. All infants
were healthy and born at term. The sample was approximately 1/3 White, 1/3 Hispanic,
and 1/3 other, including parents who refused to report; was primarily of middle-class
socio-economic status; and lived in the New York City metropolitan area. An
experimenter interviewed parents about infants’ crawling, walking, stair-climbing, andhandrail experience (see Table 1). Interviewers used a strict protocol of probe questions
regarding dates of events (Berger et al., 2007). Parents used ‘baby books’ or calendars to
augment theirmemories formilestone dates. Families received a small thank-you gift and a
diploma for participating.
Staircase apparatus
The experimental apparatus (see Figure 1) was a 54-cm-high wooden staircase with fivesteps down to the floor (step height = 14.29 cm) and custom-built low handrails
(21.27 cm from the step) on both sides that came to approximately hip height on an
average toddler. The top step (42 cm2)waswider than the other four (19 cmdeep) so that
participantswouldhave room tomanoeuver if theywanted to change or explore positions
before descending. Four poles at the corners (34.29 cm high) of the top step were
available to provide support for balance while standing or shifting body postures before
stair descent. All steps and risers of the staircase were carpeted.
Procedure
All participants completed five trials. At the start of each trial, an experimenter placed
infants close to the centre of the platform, 15–20 cm from the edge. On each trial, infants
descended the stairs to a caregiverwhowaited at the bottom. Parents called to their babies
from the foot of the stairs and offered words of encouragement, but did not provide
Development of strategy choice 109
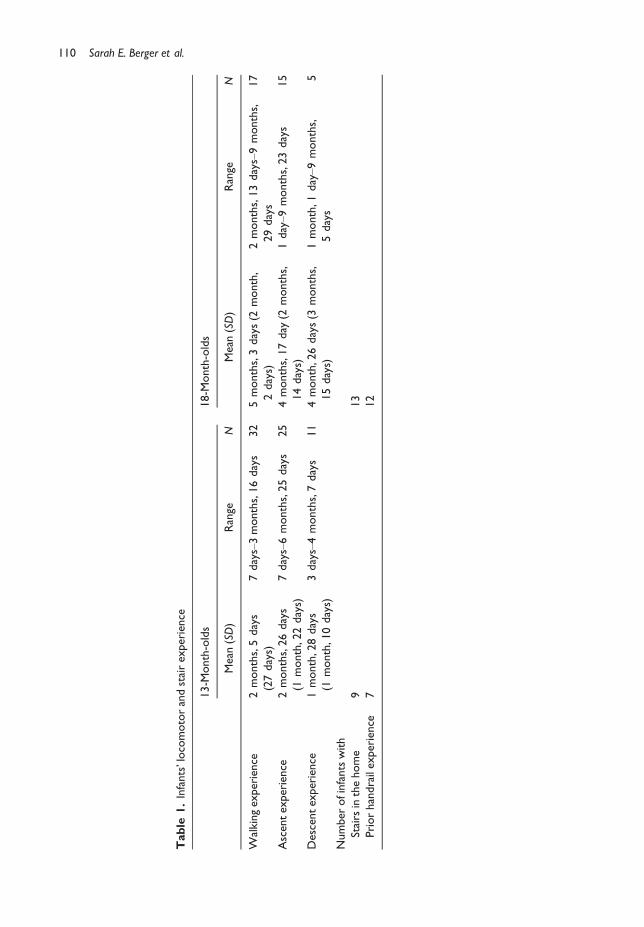
Table
1.Infants’locomotorandstairexperience
13-M
onth-olds
18-M
onth-olds
Mean
(SD)
Range
NMean
(SD)
Range
N
Walkingexperience
2months,5days
(27days)
7days–3months,16days
32
5months,3days(2
month,
2days)
2months,13days–9months,
29days
17
Ascentexperience
2months,26days
(1month,22days)
7days–6months,25days
25
4months,17day
(2months,
14days)
1day–9
months,23days
15
Descentexperience
1month,28days
(1month,10days)
3days–4months,7days
11
4month,26days(3
months,
15days)
1month,1
day–9
months,
5days
5
Numberofinfantswith
Stairs
inthehome
913
Priorhandrailexperience
712
110 Sarah E. Berger et al.
instruction on how to descend. A highly trained experimenter spotted the infants by
following alongside them to ensure their safety, but did not otherwise help the infants
with descent. The experimenter held their hands near the infants to spot them, but did not
touch them unless they started to fall. The session was videotaped with a single camerathat captured each trial with a point of viewof slightly above and facing the participants as
they descended the stairs. Sessions lasted 30 min.
Results
Data codingData from each test session were coded from videotape using OpenSHAPA, a
computerized video coding system (now Datavyu, datavyu.org; Sanderson et al., 1994).
Toddlers contributed five trials each, yielding 245 total trials for coding (160 from 13.5-
month-olds and 85 from 18-month-olds). A primary coder coded all outcome measures
from video. To ensure inter-rater reliability, a second coder independently coded 25% of
all outcome measures. Inter-rater agreement ranged from 0.98 to 1.0, and p-values for all
Cohen’s kappa coefficients <.01.
Variability in descent strategies
Coders documented all strategies infants spontaneously used to descend the staircase.
Infants descended the stairs in three ways: Walking if they walked down the stairs,
scooting if they bumped down the stairs on their bottoms, and backing if they moved
backwards on hands and knees down the stairs. Infants could perform more than one
descent strategy on each trial. A 5 (trial) 9 5 (step of the staircase [top step to bottom
step]) 9 2 (age group) repeated-measures ANOVA, with trial and step number aswithin-subjects factors and age group as a between-subjects factor, revealed no effect of
trial on the frequency that infants walked down the stairs, but did show main effects for
step of the staircase and for age, F(1, 47) = 4.62, p < .04 and F(1, 47) = 6.47, p < .02,
respectively, and a significant quadratic effect of step, F(1, 47) = 8.81, p < .01, with
(a) (b) (c)
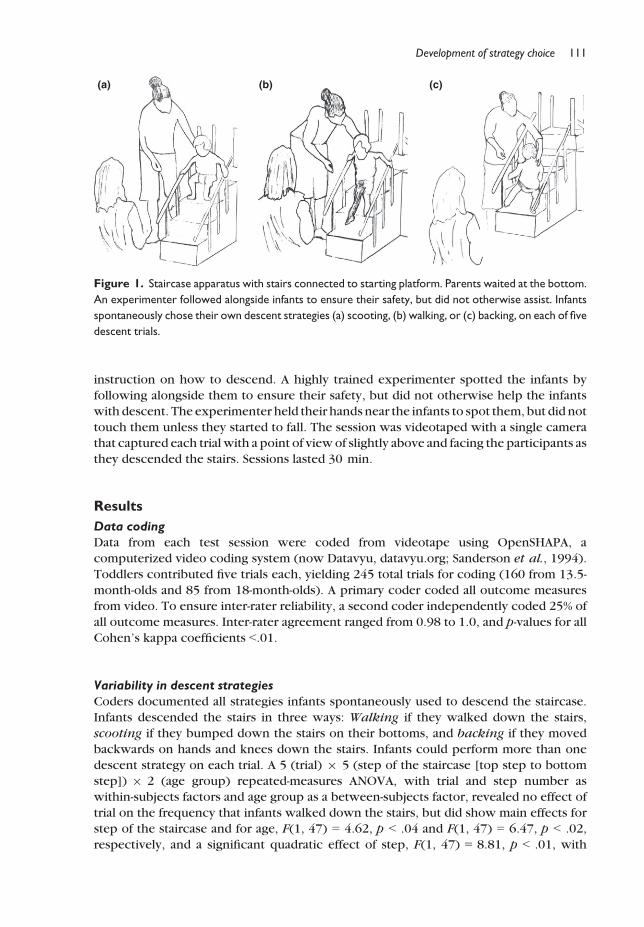
Figure 1. Staircase apparatus with stairs connected to starting platform. Parents waited at the bottom.
An experimenter followed alongside infants to ensure their safety, but did not otherwise assist. Infants
spontaneously chose their own descent strategies (a) scooting, (b) walking, or (c) backing, on each of five
descent trials.
Development of strategy choice 111
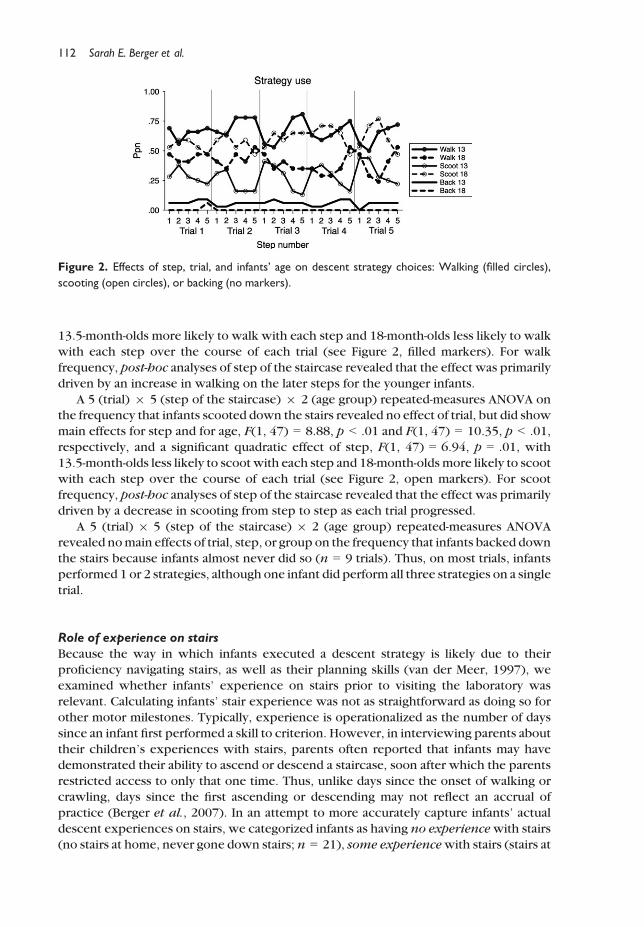
13.5-month-olds more likely to walk with each step and 18-month-olds less likely to walk
with each step over the course of each trial (see Figure 2, filled markers). For walk
frequency, post-hoc analyses of step of the staircase revealed that the effect was primarily
driven by an increase in walking on the later steps for the younger infants.
A 5 (trial) 9 5 (step of the staircase) 9 2 (age group) repeated-measures ANOVA onthe frequency that infants scooted down the stairs revealed no effect of trial, but did show
main effects for step and for age, F(1, 47) = 8.88, p < .01 and F(1, 47) = 10.35, p < .01,
respectively, and a significant quadratic effect of step, F(1, 47) = 6.94, p = .01, with
13.5-month-olds less likely to scoot with each step and 18-month-oldsmore likely to scoot
with each step over the course of each trial (see Figure 2, open markers). For scoot
frequency, post-hoc analyses of step of the staircase revealed that the effect was primarily
driven by a decrease in scooting from step to step as each trial progressed.
A 5 (trial) 9 5 (step of the staircase) 9 2 (age group) repeated-measures ANOVArevealed nomain effects of trial, step, or group on the frequency that infants backed down
the stairs because infants almost never did so (n = 9 trials). Thus, on most trials, infants
performed 1 or 2 strategies, although one infant did perform all three strategies on a single
trial.
Role of experience on stairs
Because the way in which infants executed a descent strategy is likely due to theirproficiency navigating stairs, as well as their planning skills (van der Meer, 1997), we
examined whether infants’ experience on stairs prior to visiting the laboratory was
relevant. Calculating infants’ stair experience was not as straightforward as doing so for
other motor milestones. Typically, experience is operationalized as the number of days
since an infant first performed a skill to criterion. However, in interviewing parents about
their children’s experiences with stairs, parents often reported that infants may have
demonstrated their ability to ascend or descend a staircase, soon after which the parents
restricted access to only that one time. Thus, unlike days since the onset of walking orcrawling, days since the first ascending or descending may not reflect an accrual of
practice (Berger et al., 2007). In an attempt to more accurately capture infants’ actual
descent experiences on stairs, we categorized infants as having no experiencewith stairs
(no stairs at home, never gone down stairs; n = 21), some experiencewith stairs (stairs at
Figure 2. Effects of step, trial, and infants’ age on descent strategy choices: Walking (filled circles),
scooting (open circles), or backing (no markers).
112 Sarah E. Berger et al.

home, but never gone down, n = 12; or no stairs at home, but has gone down, n = 5), or
full experience with stairs (stairs at home, has gone down stairs; n = 11).
Using handrails
Light touches of a handrail can augment balance and provide postural support (Barela,
Jeka, & Clark, 1999; Chen, Metcalfe, Chang, Jeka, & Clark, 2008; Metcalfe & Clark, 2000),
and experiencedwalkers can use handrails as a tool for balance control during locomotion
(Berger & Adolph, 2003; Berger et al., 2005). We coded whether infants touched the
handrail during stair descent. A 5 (trial) 9 2 (age group) 9 4 (experience on stairs)
repeated-measures ANOVA on the proportion of trials that infants used the handrail
revealed a significant main effect for age, with 18-month-olds using the handrail on 92% oftrials and 13.5-month-olds using the handrail on only 57% of trials, F(1, 42) = 9.57,
p < .01.
Using the experimenter
Coders documented the ways that the experimenter interacted with the infants as they
descended the stairs.We counted rescueswhether the experimenter had to touch infants
to prevent them from falling as they descended. A 5 (trial) 9 5 (step) 9 2 (agegroup) 9 4 (experience on stairs) repeated-measures ANOVA on the proportion of trials
that the experimenter rescued the infants revealed main effects for step, F(1, 42) = 6.54,
p < .02, age group, F(1, 42) = 33.30, p < .01, and a step by age group interaction, F(1,
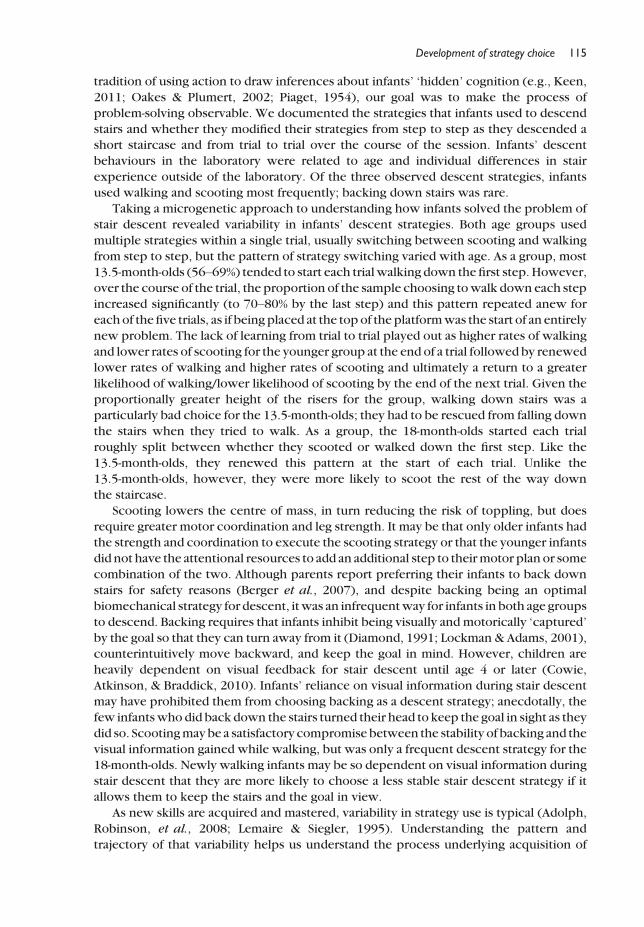
42) = 5.66, p < .03. 13.5-month-olds had to be rescued significantly more often than
18-month-olds, particularly at the end of each trial (see Figure 3, open and filled triangle
markers).
We also coded whether infants used the experimenter to augment balance if they
touched or grabbed the experimenter after they had left the starting platform. A 5(trial) 9 5 (step) 9 2 (age group) 9 4 (experience on stairs) repeated-measures ANOVA
on the proportion of trials that infants used the experimenter for support revealed a main
effect only for experience on stairs, F(3, 42) = 3.06, p < .04 (see Figure 4a). Post-hoc
analyses revealed that infants with the least experience (no stair descent experience, no
Figure 3. Effects of step, trial, and infants’ age on the role of the experimenter: Used by infants to
augment balance (circle markers), having to rescue infants when they started to fall (triangle markers), or
not involved beyond spotting the infants (square markers).
Development of strategy choice 113
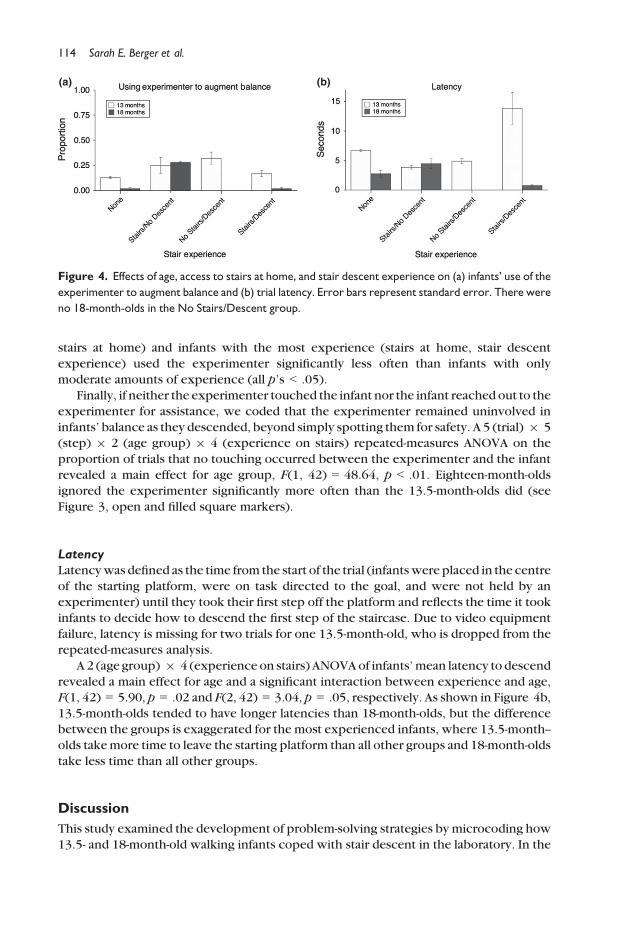
stairs at home) and infants with the most experience (stairs at home, stair descent
experience) used the experimenter significantly less often than infants with only
moderate amounts of experience (all p’s < .05).
Finally, if neither the experimenter touched the infant nor the infant reached out to the
experimenter for assistance, we coded that the experimenter remained uninvolved in
infants’ balance as they descended, beyond simply spotting them for safety. A 5 (trial) 9 5(step) 9 2 (age group) 9 4 (experience on stairs) repeated-measures ANOVA on the
proportion of trials that no touching occurred between the experimenter and the infant
revealed a main effect for age group, F(1, 42) = 48.64, p < .01. Eighteen-month-olds
ignored the experimenter significantly more often than the 13.5-month-olds did (see
Figure 3, open and filled square markers).
LatencyLatencywas defined as the time from the start of the trial (infantswere placed in the centre
of the starting platform, were on task directed to the goal, and were not held by an
experimenter) until they took their first step off the platform and reflects the time it took
infants to decide how to descend the first step of the staircase. Due to video equipment
failure, latency is missing for two trials for one 13.5-month-old, who is dropped from the
repeated-measures analysis.
A 2 (age group) 9 4 (experience on stairs) ANOVAof infants’mean latency to descend
revealed a main effect for age and a significant interaction between experience and age,F(1, 42) = 5.90, p = .02 and F(2, 42) = 3.04, p = .05, respectively. As shown in Figure 4b,
13.5-month-olds tended to have longer latencies than 18-month-olds, but the difference
between the groups is exaggerated for the most experienced infants, where 13.5-month--
olds takemore time to leave the starting platform than all other groups and 18-month-olds
take less time than all other groups.
Discussion
This study examined the development of problem-solving strategies by microcoding how
13.5- and 18-month-old walking infants coped with stair descent in the laboratory. In the
(a) (b)
Figure 4. Effects of age, access to stairs at home, and stair descent experience on (a) infants’ use of the
experimenter to augment balance and (b) trial latency. Error bars represent standard error. There were
no 18-month-olds in the No Stairs/Descent group.
114 Sarah E. Berger et al.
tradition of using action to draw inferences about infants’ ‘hidden’ cognition (e.g., Keen,
2011; Oakes & Plumert, 2002; Piaget, 1954), our goal was to make the process of
problem-solving observable. We documented the strategies that infants used to descend
stairs and whether they modified their strategies from step to step as they descended ashort staircase and from trial to trial over the course of the session. Infants’ descent
behaviours in the laboratory were related to age and individual differences in stair
experience outside of the laboratory. Of the three observed descent strategies, infants
used walking and scooting most frequently; backing down stairs was rare.
Taking a microgenetic approach to understanding how infants solved the problem of
stair descent revealed variability in infants’ descent strategies. Both age groups used
multiple strategies within a single trial, usually switching between scooting and walking
from step to step, but the pattern of strategy switching varied with age. As a group, most13.5-month-olds (56–69%) tended to start each trialwalking down the first step. However,
over the course of the trial, the proportion of the sample choosing towalk down each step
increased significantly (to 70–80% by the last step) and this pattern repeated anew for
eachof the five trials, as if beingplaced at the topof the platformwas the start of an entirely
new problem. The lack of learning from trial to trial played out as higher rates of walking
and lower rates of scooting for the younger group at the end of a trial followedby renewed
lower rates of walking and higher rates of scooting and ultimately a return to a greater
likelihood of walking/lower likelihood of scooting by the end of the next trial. Given theproportionally greater height of the risers for the group, walking down stairs was a
particularly bad choice for the 13.5-month-olds; they had to be rescued from falling down
the stairs when they tried to walk. As a group, the 18-month-olds started each trial
roughly split between whether they scooted or walked down the first step. Like the
13.5-month-olds, they renewed this pattern at the start of each trial. Unlike the
13.5-month-olds, however, they were more likely to scoot the rest of the way down
the staircase.
Scooting lowers the centre of mass, in turn reducing the risk of toppling, but doesrequire greater motor coordination and leg strength. It may be that only older infants had
the strength and coordination to execute the scooting strategy or that the younger infants
did not have the attentional resources to add an additional step to theirmotor plan or some
combination of the two. Although parents report preferring their infants to back down
stairs for safety reasons (Berger et al., 2007), and despite backing being an optimal
biomechanical strategy for descent, itwas an infrequentway for infants in both age groups
to descend. Backing requires that infants inhibit being visually and motorically ‘captured’
by the goal so that they can turn away from it (Diamond, 1991; Lockman & Adams, 2001),counterintuitively move backward, and keep the goal in mind. However, children are
heavily dependent on visual feedback for stair descent until age 4 or later (Cowie,
Atkinson, & Braddick, 2010). Infants’ reliance on visual information during stair descent
may have prohibited them from choosing backing as a descent strategy; anecdotally, the
few infantswho did back down the stairs turned their head to keep the goal in sight as they
did so. Scootingmaybe a satisfactory compromise between the stability of backing and the
visual information gained while walking, but was only a frequent descent strategy for the
18-month-olds. Newly walking infants may be so dependent on visual information duringstair descent that they are more likely to choose a less stable stair descent strategy if it
allows them to keep the stairs and the goal in view.
As new skills are acquired and mastered, variability in strategy use is typical (Adolph,
Robinson, et al., 2008; Lemaire & Siegler, 1995). Understanding the pattern and
trajectory of that variability helps us understand the process underlying acquisition of
Development of strategy choice 115
problem-solving skills. In this study, scooting down stairs and using the handrail were
alternative descent strategies that provided increased stability for toddlers. However, new
walkers can be reluctant to switch to alternative locomotor strategies, even when
continuing towalkmeans bumping a head on a low entrance or trying to squeeze throughan impossibly narrow space (Berger, 2010; Berger & Scher, 2012; Brownell, Zerwas, &
Ramani, 2007; Comalli & Adolph, 2013). In this case, for the few 13.5-month-olds who
came up with the strategy of scooting at the start of the trial, maintaining that posture for
the duration of the trial was difficult. In addition, the younger infants did not incorporate
an external object into their action plan, with only around half of the group using the
handrail, and almost none reaching out to the experimenter for help. The overlapping
waves model of adaptive strategy choice would predict that with increased experience,
the use of alternative strategies should increase (Lemaire & Siegler, 1995; Siegler, 2005).Indeed, the 18-month-olds, who on average had more walking and descent experience
than the 13.5-month-olds, maintained the alternative descent strategy of scooting for a
greater proportion of each trial and almost all used the handrail for support (they did not
use the experimenter for help, either, but that was because they used the handrail
instead). Moreover, infants with moderate amounts of experience reached out to the
experimenter during descent more often than infants with no descent experience at all
prior to participating in the study. Augmenting balance with an adult may serve as an
alternative descent strategy available to infants with minimal experience on stairs that isless sophisticated than handrail use, but possibly reflecting prior experience in which an
adult taught infants to descend.
A possible explanation for the observed pattern of strategy shifts could be the
tendency of younger children to demonstrate ‘utilization deficiencies’ (Clerc & Miller,
2013; Gaultney, Kipp, & Kirk, 2005; Schneider, Kron, Hunnerkopf, & Krajewski, 2004).
Utilization deficiencies were first identified by Miller (1990) as part of the normal
progression of strategy development in which a strategy is used properly and
spontaneously, but to no benefit. In keeping with the tradition of studying utilizationdeficiencies microgenetically (Coyle & Bjorklund, 1996; Schwenck, Bjorklund, &
Schneider, 2007), we documented 13-month-olds’ tendency to switch to walking at later
steps on a trial and the increased likelihood that they required rescue on those later steps.
This patternwas parallel to the utilization deficiencies seen in tasks that traditionally study
memory, selective attention, organization, and reading comprehension (Bjorklund, Coyle,
& Gaultney, 1992; Gaultney, 1995; Gaultney et al., 2005; Miller, 1994). Consistent with
Miller’s account of strategy development, 18-month-olds did not show evidence of
utilization deficiencies – upon switching to a scooting strategy, they experienced thebenefits that the younger infants did not – most likely due to their increased locomotor
experience and greater pool of attentional resources.
Taken together, infants’ sequence of behaviours suggests that their exploration largely
focused on how to approach the 1st step of the staircase, rather than on the creation of a
detailed plan for navigating the staircase from top to bottom. For example, 13-month-olds
typically started out with a good descent strategy, but soon switched to a bad one, with
rescues happening primarily later in the trial. It is unlikely that this would be part of a
general navigation plan given how effortful and taxing it is for new walkers to switchbetween postures (Berger, 2010) and how aversive they find being rescued from a fall
(e.g., Adolph, 2000; Berger et al., 2005; Franchak & Adolph, 2012). Moreover, the
18-month-olds were essentially at chance in their choice of strategy on the first step, but
consistently switched to a more efficient strategy for subsequent steps. If they were
planning ahead from the platform, we might expect consistency in strategy choice from
116 Sarah E. Berger et al.
the initial step, rather than settling on it eventually. Thus, it appears as though infants’
planning happened online as they faced the challenge of each new step, rather than at the
start of a sequence of planned movements.
Individual differences in experience descending stairs also shed light onto thedevelopment of problem-solving. One of the hallmarks of expertise is understandingwhat
information is relevant to the task at hand and how to use that information effectively
(Adolph, Karasik, & Tamis-LeMonda, 2010; Tamis-LeMonda et al., 2008). Infants in both
age groups who had the most experience descending stairs – having stairs at home and
having descended stairs prior to visiting the laboratory – approached the problem of
descent differently than infants withminimal descent experience. However, as with their
choice of descent strategies, approach differed by age. Experienced 18-month-olds
recognized the problem and quickly came up with a solution – they left the startingplatform in a fraction of the time of all other groups. In contrast, experienced
13-month-olds took significantly longer to plan their descent strategy compared to all
other groups. Their expertise gave them thewherewithal to recognize that they needed to
plan their solution, but they were slower and more deliberate than the older infants in
carrying out the plan. Both experienced groups’ exploratory behaviour suggested that
they recognized stair descent as a novel problem and that their solution to this problem
drew on their unique and specific experiences (van der Meer, 1997; Ulrich et al., 1990).
Adaptive locomotion involves both motor proficiency and higher level cognitiveabilities (Berger & Adolph, 2003). Our microgenetic coding of strategy use, exploratory
behaviour, and success on the task reflected elements of planning and decision-making
associated with problem-solving. However, our measure of experience was admittedly a
crude way to capture proficiency. For stair descent in particular, with only parent reports
of the first day that infants performed the skill to criteria to go on, experience may be
harder tomeasure than othermotormilestones because of the inextricable role of parents
creating constraints and opportunities for practice. The finding that our rudimentary
measure of experience predicted one strategy suggests that it may be fruitful for futurework to delve further into the role of proficiency with either biomechanical measure-
ments or prospective documentation of stair experience. Previous work has shown that
measures of locomotor proficiency predict individual differences when the locomotor
task pushes infants to the limits of their abilities (Berger & Adolph, 2003). Our measure of
experience may not have been sensitive enough to tease apart the contributions of skill
and cognitive ability for all strategy choices, but a more precise measure may reveal a
greater role of experience.
The development of strategy use has typically focused on older children learning tosolve cognitive or reasoning tasks and has taken advantage of participants’ verbal abilities
to respond toquestions or provide commentary on their actions (e.g., Chen&Klahr, 1999;
although Adolph, 1997; andMcCarty, Clifton, &Collard, 1999; are some exceptions). One
drawback has been the unsuitability of thesemethods for usewith pre-verbal populations.
In contrast, our approach to studying locomotor problem-solving has the advantage of
documenting strategy use and decision-making in a younger population that is otherwise
unable to comment on their own actions. We see striking parallels between infants’
behaviour in this locomotor problem-solving task and older children’s behaviour onmore‘cognitive’ tasks. For example,we got a glimpse of the first phase of strategy development,
the acquisition of new strategies, with the appearance of new locomotor descent
strategies in the repertoire of younger infants, and saw the utilization of new strategies in
full force by the older infants. The second phase of strategy development ismapping prior
experiences with strategies to the novel task. In this case, we observed the infants with
Development of strategy choice 117

prior stair experience treating the laboratory task differently from theway infants with no
or minimal experience treated the task. Finally, we observed phase three of strategy
development, strengthening the newly acquired strategy. Over the course of several
months spent acquiring relevant walking and stair descent experience, the older infantsreified the more effective solutions to the problem of stair descent. Within each trial, we
observed a mix of an initial failing to rely on newly acquired strategies, but then the
strengthening of the usage of those strategies for the 18-month-olds.
These findings may be useful for parents whose children are learning to climb stairs.
Previous work has shown that although infants’ may have locomotor expertise across a
variety of terrains in one posture, they need to attain that expertise all over again upon the
acquisition of a new posture (e.g., Adolph, 1997, 2000; Berger, 2010). Likewise, in this
study, experienced walkers solved the novel problem of stair descent more effectivelythan novice walkers. Parents’ attempts to teach new, motorically safe, but cognitively
challenging descent strategies to new walkers as they learn to descend stairs would be
ineffective before infants have attained sufficient motor and cognitive proficiency.
Parents’ vigilance upon the onset of infants’ acquisition of stair descent is crucial,
particularly for new walkers.
Previous work has documented variability in locomotor strategies from trial to trial as
new skills were acquired or revealed the repertoire of strategies available to experts
(Adolph, 1997; Berger et al., 2005). Documenting descent strategy on a step-by-step basisin this study has helped to provide a new level of precision in understanding the process of
acquiring the expertise required for successful strategy choice. As cognitive resources are
taxed during a challenging task, performing the task itself may reduce the resources
available for weighing alternatives or inhibiting an often-used strategy. On each trial,
younger infants entertained an alternative,more stable strategy for descent (scooting), but
often reverted to their typical locomotor strategy of walking before the end of the trial.
During each new trial, they considered again the possibility of using a better, safer
strategy, but themotor difficulty of stair descent combinedwith the cognitive demands ofentertaining alternative plans of action may have overtaxed their resources. In contrast,
the older infants who did not have to attend so closely to the motor demands of descent
could more easily consider alternative strategies, including switching to scooting and
using a handrail, and maintain those solutions over the course of a trial.
In sum, documenting within- and between-trial problem-solving at both microgenetic
and cross-sectional levels in a locomotor task yielded a rich behavioural data set and
helped to chart the process of becoming increasingly proficient and efficient in strategy
choice and use. Studying learning in action demonstrated that stair descent requiresproblem-solving strategies similar to those previously observed in other forms of adaptive
locomotion, as well as in tasks more broadly construed as cognitive (Berger, 2010; Berger
& Adolph, 2007; Carrico, 2013).
Acknowledgements
Wegratefully acknowledgeDr. LanaKarasik and themembers of the ChildDevelopment Lab at
the College of Staten Island for their constructive feedback on earlier drafts of this manuscript.
A portion of this research was supported by PSC-CUNY Research Grant 40-175 to Sarah E.
Berger, Department of Psychology, the College of Staten Island, and theGraduate Center of the
City University of New York. A portion of this data was presented at the Seventeenth
International Conference on Infant Studies, Baltimore, MD, 2010.We thankMohamedHussein
for his help with data coding and the line drawings.
118 Sarah E. Berger et al.
References
Adolph, K. E. (1997). Learning in the development of infant locomotion.Monographs of the Society
for Research in Child Development, 62(3), 1–158.Adolph, K. E. (2000). Specificity of learning: Why infants fall over a veritable cliff. Psychological
Science, 11, 290–295. doi:10.1111/1467-9280.00258Adolph, K. E., Cole,W. G., Komati, M., Garciaguirre, J. S., Badaly, D., Lingeman, J. M., . . . Sotsky, R. B.
(2012). Howdo you learn towalk? Thousands of steps and dozens of falls per day. Psychological
Science, 23, 1387–1394. doi:10.1177/0956797612446346Adolph, K. E., Eppler, M. A., & Gibson, E. J. (1993). Crawling versus walking infants’ perception of
affordances for locomotion over sloping. Child Development, 64, 1158–1174. doi:10.1111/j.1467-8624.1993.tb04193.x
Adolph,K. E., Karasik, L. B., &Tamis-LeMonda, C. S. (2010). Using social information to guide action:
Infants’ locomotion over slippery slopes. Neural Networks, 23, 1033–1042. doi:10.1016/j.neunet.2010.08.012
Adolph, K. E., Robinson, S. R., Young, J. W., & Gill-Alvarez, F. (2008). What is the shape of
developmental change? Psychological Review, 115, 527–543. doi:10.1037/0033-295X.115.3.527
Badaly, D., & Adolph, K. E. (2008). Beyond the average: Walking infants take steps longer than their
leg length. Infant Behavior andDevelopment, 31, 554–558. doi:10.1016/j.infbeh.2007.12.010Barela, J., Jeka, J. J., & Clark, J. (1999). The developmental use of somatosensory information during
the acquisition of independent upright stance. Infant Behavior andDevelopment, 22, 89–104.doi:10.1016/S0163-6383(99)80007-1
Berger, S. E. (2004). Demands on finite cognitive capacity cause infants’ perseverative errors.
Infancy, 5, 217–238. doi:10.1207/s15327078in0502_7Berger, S. E. (2010). Locomotor expertise predicts infants’ perseveration errors. Developmental
Psychology, 46, 326–336. doi:10.1037/a0018285Berger, S. E., & Adolph, K. E. (2003). Infants use handrails as tools in a locomotor task.
Developmental Psychology, 39, 594–605. doi:10.1037/0012-1649.39.3.594Berger, S. E., & Adolph, K. E. (2007). Learning and development in infant locomotion. In C. von
Hofsten & K. Rosander (Eds.), From action to cognition (pp. 237–255). Amsterdam, the
Netherlands: Elsevier.
Berger, S. E., Adolph, K. E., & Kavookjian, A. E. (2010). Bridging the gap: Solving spatial means–endsrelations in a locomotor task. Child Development, 81, 1367–1375. doi:10.1111/j.1467-8624.2010.01478.x
Berger, S. E., Adolph, K. E., & Lobo, S. A. (2005). Out of the toolbox: Toddlers differentiate wobbly
and wooden handrails. Child Development, 76, 1294–1307. doi:10.1111/j.1467-8624.2005.00851.x
Berger, S. E., Chan, G., & Adolph, K. E. (2014). What cruising infants understand about support for
locomotion. Infancy, 19, 117–137. doi:10.1111/infa.12042Berger, S. E., & Scher, A. (2012). What is the role of sleep in toddlers’ motor learning? Poster
presented at the Eighteenth Biennial International Conference on Infant Studies, Minneapolis,
MN.
Berger, S. E., Theuring, C.,&Adolph,K. E. (2007).Howandwhen infants learn to climb stairs. Infant
Behavior and Development, 30, 36–49. doi:10.1016/j.infbeh.2006.11.002Bjorklund, D. F., Coyle, T. R., & Gaultney, J. F. (1992). Developmental differences in the acquisition
and maintenance of an organizational strategy: Evidence for the utilization deficiency
hypothesis. Journal of Experimental Child Psychology, 54, 434–448. doi:10.1016/0022-0965(92)90029-6
Brownell, C. A., Zerwas, S., & Ramani, G. B. (2007). “So big”: The development of body
self-awareness in toddlers. Child Development, 78, 1426–1440. doi:10.1111/j.1467-8624.2007.01075.x
Development of strategy choice 119
Bull, R., Espy, K. A., & Wiebe, S. A. (2008). Short-term memory, working memory, and executive
functioning in preschoolers: Longitudinal predictors of mathematical achievement at age
7 years. Developmental Neuropsychology, 33, 205–228. doi:10.1080/87565640801982312Carrico, R. L. (2013). Attention andmultistep problem solving in 24-month-old children. Journal of
Cognition and Development, 14, 529–545. doi:10.1080/15248372.2012.689388Chen, Z., & Klahr, D. (1999). All other things being equal: Acquisition and transfer of the control of
variables strategy. Child Development, 70, 1098–1120. doi:10.1111/1467-8624.00081Chen, L. C., Metcalfe, J. S., Chang, T. Y., Jeka, J. J., & Clark, J. E. (2008). The development of infant
upright posture: Sway less or sway differently? Experimental Brain Research, 186, 293–303.doi:10.1007/s00221-007-1236-1
Chen, Z., & Siegler, R. S. (2000). Across the great divide: Bridging the gap between understanding of
toddlers’ and older children’s thinking. Monographs of the Society for Research in Child
Development, 65(1), 1–96.Clerc, J., & Miller, P. H. (2013). Utilization deficiencies and transfer of strategies in preschoolers.
Cognitive Development, 28, 76–93. doi:10.1016/j.cogdev.2012.09.003Comalli, D. M., & Adolph, K. E. (2013). Stop, drop, and crawl: Infants select locomotor strategies
based on overhead clearance. Poster presented at Society for Research in Child Development,
Seattle, WA.
Cowie, D., Atkinson, J., & Braddick, O. (2010). Development of visual control in stepping down.
Journal of Experimental Brain Research, 202, 181–188. doi:10.1007/s00221-009-2125-6Coyle, T. R., & Bjorklund, D. F. (1996). The development of strategic memory: A modified
microgenetic assessment of utilization deficiencies. Cognitive Development, 11, 295–314.doi:10.1016/S0885-2014(96)90006-4
Diamond, A. (1991). Neuropsychological insights in themeaning of object concept development. In
S. Carey & R. Gelman (Eds.), The epigenesis of mind (pp. 67–110). Hillsdale, NJ: Erlbaum.
Franchak, J.M.,&Adolph,K. E. (2012).What infants knowandwhat theydo: Perceiving possibilities
for walking through openings. Developmental Psychology, 48, 1254–1261. doi:10.1037/
a0027530
Frankenburg, W. K., & Dodds, J. B. (1967). The Denver developmental screening test. Journal of
Pediatrics, 71, 181–191. doi:10.1016/S0022-3476(67)80070-2Gaultney, J. F. (1995). The effect of prior knowledge and metacognition on the acquisition of a
reading comprehension strategy. Journal of Experimental Child Psychology, 59, 142–163.doi:10.1006/jecp.1995.1006
Gaultney, J. F., Kipp, K., & Kirk, G. (2005). Utilization deficiency and working memory capacity in
adult memory performance: Not just for children anymore. Cognitive Development, 20, 205–213. doi:10.1016/j.cogdev.2005.02.001
Gesell, A. (1934). Infant behavior: Its genesis and growth. New York, NY: Greenwood Press.
Gibson, E. J., Riccio, G., Schmuckler, M. A., Stoffregen, T. A., Rosenberg, D., & Taormina, J. (1987).
Detection of the traversability of surfaces by crawling and walking infants. Journal of
Experimental Psychology: Human Perception and Performance, 13, 533–544. doi:10.1037/0096-1523.13.4.533
Joh, A. S., & Adolph, K. E. (2006). Learning from falling. Child Development, 77, 89–102. doi:10.1111/j.1467-8624.2006.00858.x
Keen, R. (2011). The development of problem solving in young children: A critical cognitive skill.
Annual Review of Psychology, 62, 1–21. doi:10.1146/annurev.psych.031809.130730Kretch, K. S., & Adolph, K. E. (2013). Cliff or step? Posture-specific learning at the edge of a drop-off.
Child Development, 84, 226–240. doi:10.1111/j.1467-8624.2012.01842.xLemaire, P. (2010). Cognitive strategy variations during aging. Current Directions in Psychological
Science, 19, 363–369. doi:10.1177/0963721410390354Lemaire, P., & Lecacheur, M. (2011). Age-related changes in children’s executive functions and
strategy selection: A study in computational estimation. Cognitive Development, 26, 282–294.doi:10.1016/j.cogdev.2011.01.002
120 Sarah E. Berger et al.
Lemaire, P., & Reder, L. (1999). What affects strategy selection in arithmetic? The example of parity
and five effects on product verification. Memory & Cognition, 27, 364–382. doi:10.3758/BF03211420
Lemaire, P., & Siegler, R. S. (1995). Four aspects of strategic change: Contributions to children’s
learning of multiplication. Journal of Experimental Psychology: General, 124, 83–97. doi:10.1037/0096-3445.124.1.83
Lockman, J. J., & Adams, C. D. (2001). Going around transparent and grid-like barriers: Detour ability
as a perception-action skill.Developmental Science, 4, 463–471. doi:10.1111/1467-7687.00188McCarty, M. E., Clifton, R. K., & Collard, R. R. (1999). Problem solving in infancy: The emergence of
an action plan. Developmental Psychology, 35, 1091–1101. doi:10.1037/0012-1649.35.4.1091McGraw, M. B., & Breeze, K. W. (1941). Quantitative studies in the development of erect
locomotion. Child Development, 12, 267–303.Metcalfe, J. S., & Clark, J. E. (2000). Sensory information affords exploration of posture in newly
walking infants and toddlers. Infant Behavior & Development, 23, 391–405. doi:10.1016/S0163-6383(01)00054-6
Miller, P. H. (1990). The development of strategies of selective attention. In D. F. Bjorklund (Ed.),
Children’s strategies: Contemporary views of cognitive development (pp. 157–184). Hillsdale,NJ: Erlbaum.
Miller, P. H. (1994). Individual differences in children’s strategy behaviors: Utilization deficiencies.
Learning and Individual Differences, 6, 285–307. doi:10.1016/1041-6080(94)90019-1National SAFE KIDS Campaign (2004). Falls fact sheet. Retrieved from http://www.preventinjury.
org/PDFs/FALLS.pdf
Oakes, L. M., & Plumert, J. M. (2002). Variability in thirteen-month-old infants’ touching patterns in
the sequential-touching task. Infant Behavior and Development, 25, 529–549. doi:10.1016/S0163-6383(02)00149-2
Piaget, J. (1954). The construction of reality in the child. New York, NY: Free Press.
Sanderson, P. M., Scott, J. J. P., Johnston, T., Mainzer, J., Watanabe, L. M., & James, J. M. (1994).
MacSHAPA and the enterprise of Exploratory Sequential Data Analysis (ESDA). International
Journal of Human-Computer Studies, 41, 633–681.Schneider, W., Kron, V., Hunnerkopf, M., & Krajewski, K. (2004). The development of young
children’s memory strategies: First findings from the Wurzburg Longitudinal Memory Study.
Journal of Experimental Child Psychology, 88, 193–209. doi:10.1016/j.jecp.2004.02.004Schwenck, C., Bjorklund, D. F., & Schneider, W. (2007). Factors influencing the incidence of
utilization deficiencies and other patterns of recall/strategy-use relations in a strategic memory
task. Child Development, 78, 1771–1787. doi:10.1111/j.1467-8624.2007.01090.xShrager, J., & Siegler, R. S. (1998). SCADS: A model of children’s strategy choices and strategy
discoveries. Psychological Science, 9, 405–410. doi:10.1111/1467-9280.00076Siegler, R. S. (1996).Emergingminds: The process of change in children’s thinking. NewYork, NY:
Oxford University Press.
Siegler, R. S. (1998). Children’s thinking (3rd ed.). Upper Saddle River, NJ: Prentice Hall.
Siegler, R. S. (2000). The rebirth of children’s learning. Child Development, 71 (1), 26–35. doi:10.1111/1467-8624.00115
Siegler, R. S. (2002). Microgenetic studies of self-explanation. In N. Granott & J. Parziale (Eds.),
Microdevelopment: Transition processes in development and learning (pp. 31–58). NewYork, NY: Cambridge University Press.
Siegler, R. S. (2005). Children’s learning. American Psychologist, 60, 769–778. doi:10.1037/0003-066X.60.8.769
Siegler, R. S. (2007). Cognitive variability. Developmental Science, 10, 104–109. doi:10.1111/j.1467-7687.2007.00571.x
Sugar, N. F., Taylor, J. A., & Feldman, K.W. (1999). Bruises in infants and toddlers: Those who don’t
cruise rarely bruise. Archives of Pediatrics and Adolescent Medicine, 153, 399–403. doi:10.1001/archpedi.153.4.399
Development of strategy choice 121

Tamis-LeMonda, C. S., Adolph, K. E., Lobo, S. A., Karasik, L. B., Ishak, S., & Dimitropoulou, K. A.
(2008). When infants take mothers’ advice: 18-month-olds integrate perceptual and social
information to guide motor action. Developmental Psychology, 44, 734–746. doi:10.1037/0012-1649.44.3.734
Tunteler, E., &Resing,W.C.M. (2002). Spontaneous analogic transfer in 4-year-olds: Amicrogenetic
study. Journal of Experimental Child Psychology, 83, 149–166. doi:10.1016/S0022-0965(02)00125-X
Ulrich, B. D., Thelen, E., & Niles, D. (1990). Perceptual determinants of action: Stair-climbing
choices of infants and toddlers. Advances in Motor Development Research, 3, 1–15.U.S. Consumer Product Safety Commission (2010).National electronic injury surveillance system
(NEISS). Retrieved from http://www.cpsc.gov/library/neiss.html
van der Meer, A. L. (1997). Visual guidance of passing under a barrier. Early Development and
Parenting, 6, 149–158.Wilmut, K., & Barnett, A. L. (2011). Locomotor behaviour of children while navigating through
apertures. Experimental Brain Research, 210, 185–194. doi:10.1007/s00221-011-2614-2Woollacott, M., & Shumway-Cook, A. (2002). Attention and the control of posture and gait: A review
of an emerging area of research.Gait & Posture, 16, 1–14. doi:10.1016/S0966-6362(01)00156-4Young, T., Torner, J., Schmitt, K., & Peek-Asa, C. (2011). Fall injury report (2002–2009 Iowa State
Trauma Registry Data). Des Moines, IA: Iowa Department of Public Health.
Received 21 April 2014; revised version received 13 November 2014
122 Sarah E. Berger et al.