Embed Size (px)
Citation preview
Stephen Clement M.D. CDE
Medical Director, Endocrine Services
Inova Fairfax Hospital

Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines


Case Study BH is a 67 y/o female with T2 DM for 15 years, treated with metformin and
glyburide
No self testing of BGs at home
A1C 8-9%
No microvascular complications
h/o MI, PTCA
Presents to community hospital with 10/10 substernal chest pain
ECG T wave inversions V1-V6
Cardiac Cath– severe multivessel disease, no occlusion

Case Study Questions: What intervention should she have for her multi-vessel disease?
Going forward, what are the goals for her diabetes and medical therapy for ASCVD based on recent Randomized Clinical Trials and Guidelines?
Outline RCTs/Clinical Guidelines
CABG vs. PTCA Trials
Glucose Control Studies:
UKPDS
ACCORD
CV Outcome Trials for new medications
How to Treat?

RCT/Clinical Practice Guideline Trends Retrospective studies are good for hypothesis generating, but suffer from..
o Bias from ascertainment of cases/controls, other biases
o Potential biases are a particular concern in comparative effectiveness research (i.e., confounding by indication)
Large multicenter randomized studies are still the Gold Standard
RCTs now often required for changing practice guidelines


American Diabetes AssociationClinical Practice Guidelines“Recommendations with an A rating are based on large well-designed
clinical trials or well-done meta-analyses. Generally, these recommendations have the best chance of improving outcomes when applied to the population to which they are appropriate.”
Diabetes Care 37, supplement 1, 2014

Case Study BH with T2DM Multi-vessel disease with acute coronary syndrome (unstable angina)
Prior RCTs: BARI, BARI 2D, CARDia, SYNTAX
? PCI with drug eluting stents vs. CABG?

FREEDOM STUDYFuture Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multi-vessel Disease
Diabetes with Multivessel Dz
Randomized to:
PCI with drug-eluting stents (serolimus or paxlitaxel) followed by abciximaband dual antiplatelet Rx, or
CABG
• Outcome: MACE

Kaplan–Meier Estimates of the Composite Primary Outcome and Death.
Farkouh ME et al. N Engl J Med 2012;367:2375-2384.

Freedom Study Conclusion: For patients with diabetes and advanced CAD, CABG was
superior to PCI in that it significantly reduced rate of death, MI, with a higher rate of stroke.

Case Study BH with T2DM Multi-vessel disease with acute coronary syndrome (unstable angina)?
Send for CABG
• What about her diabetes management?
What should her target A1C be?
Are there Rx’s (OHA, Insulin, incretin agonists) that confer better outcomes?


UKPDS – Myocardial Infarction
UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352(9131):837-853.
Risk Reduction 16% (0%-29%)
P=0.052
30
20
10
0
0 3 6 9 12 15
Years From Randomization
% o
f P
atie
nts
Wit
h a
n E
ven
t ConventionalIntensive
Fatal or Non-fatal MI, Sudden Death 573 of 3867 Patients (15%)

Myocardial Infarction Hazard Ratio(fatal or non-fatal MI or sudden death)
Intensive (SU/Ins) vs Conventional Glucose Control
HR (95%CI)
UKPDS 80. N Eng J Med 2008;359:1577–89
0.4
0.6
0.8
1.0
1.2
1.4
1997 1999 2001 2003 2005 2007
HR
MIHR=0.84p=0.052
HR=0.85p=0.014
Number of EventsCon: 168 212 239 271 296 319Int: 387 450 513 573 636 678
18
The ability to show a difference in a clinical trial depends upon:
The Hazard Rate of the outcome
The Effect Size of the intervention
The Exposure to the intervention
The Confounding therapies provided to the participants
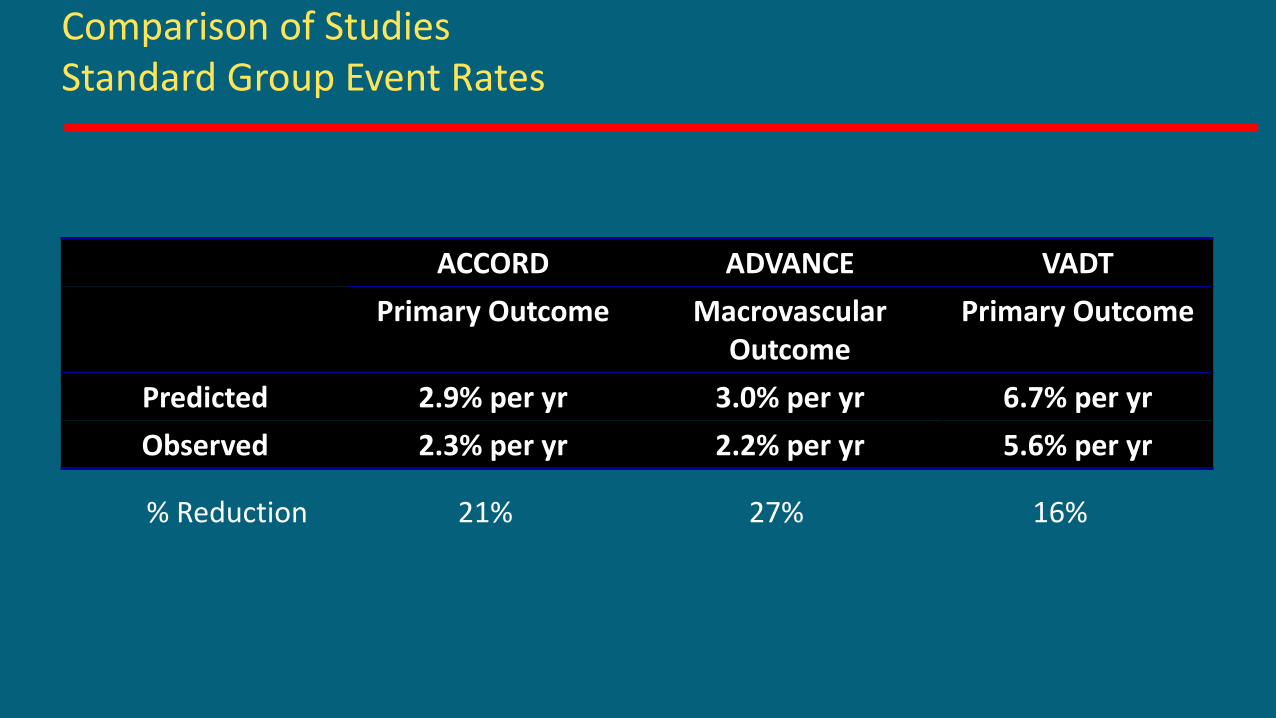
Comparison of StudiesStandard Group Event Rates
ACCORD ADVANCE VADT
Primary Outcome MacrovascularOutcome
Primary Outcome
Predicted 2.9% per yr 3.0% per yr 6.7% per yr
Observed 2.3% per yr 2.2% per yr 5.6% per yr
% Reduction 21% 27% 16%

ACCORD: Treatment Effects onGlucose Control
A1c
(%
)
Time (Years)
Standard therapy
Intensive therapy
6
9.0
8.5
8.0
7.5
7.0
6.5
6.0
00 1 2 3 4 5
ACCORD Study Group. N Engl J Med 2008;358:2545–59
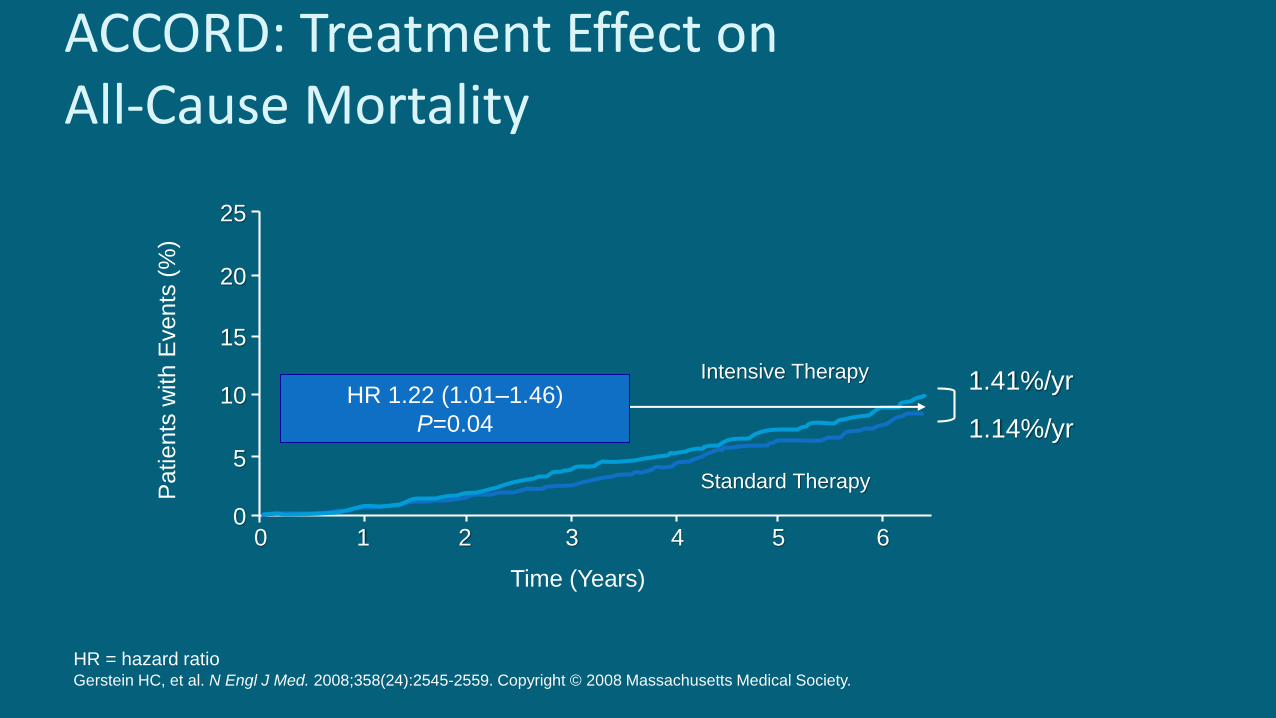
ACCORD: Treatment Effect onAll-Cause Mortality
Time (Years)
25
0
20
15
10
5
01 2 3 4 5 6
Standard Therapy
Intensive TherapyHR 1.22 (1.01–1.46)
P=0.04
1.41%/yr
1.14%/yr
Patients
with
Events
(%
)
HR = hazard ratioGerstein HC, et al. N Engl J Med. 2008;358(24):2545-2559. Copyright © 2008 Massachusetts Medical Society.

ACCORD: Deaths in Intensive vs Standard Glycemic Control Groups
National Heart, Lung, and Blood Institute. ACCORD Telebriefing Prepared Remarks. Bethesda, MD: NHLBI; February 6 2008.
Standard Glycemic Control Intensive Glycemic Control
Deaths, n 203 (11/1000/y) 257 (14/1000/y)
(0.011 /y) (0.014/y)
Median A1c 7.5% 6.4%

Risk of Death Over a Range of Average A1c
Riddle MC, et al. Diabetes Care. 2010;33(5):983-990. Copyright © 2010 by the American Diabetes Association.
Average A1c %
Adjusted log (HR) by Treatment StrategyRelative to standard at A1c of 6%
Standard strategy
6 8 97
Excess risk with intensive strategy vs standard occurred above A1c 7%
Intensive
strategy
1
0
–1
Steady increase of risk from 6% to 9% A1c with intensive strategy

Observations from ACCORD Investigators Many patients not able to adhere to complex oral/insulin regimens
The degree of “disarray” in the patient’s house predicted a major AE
Personal communication 2013
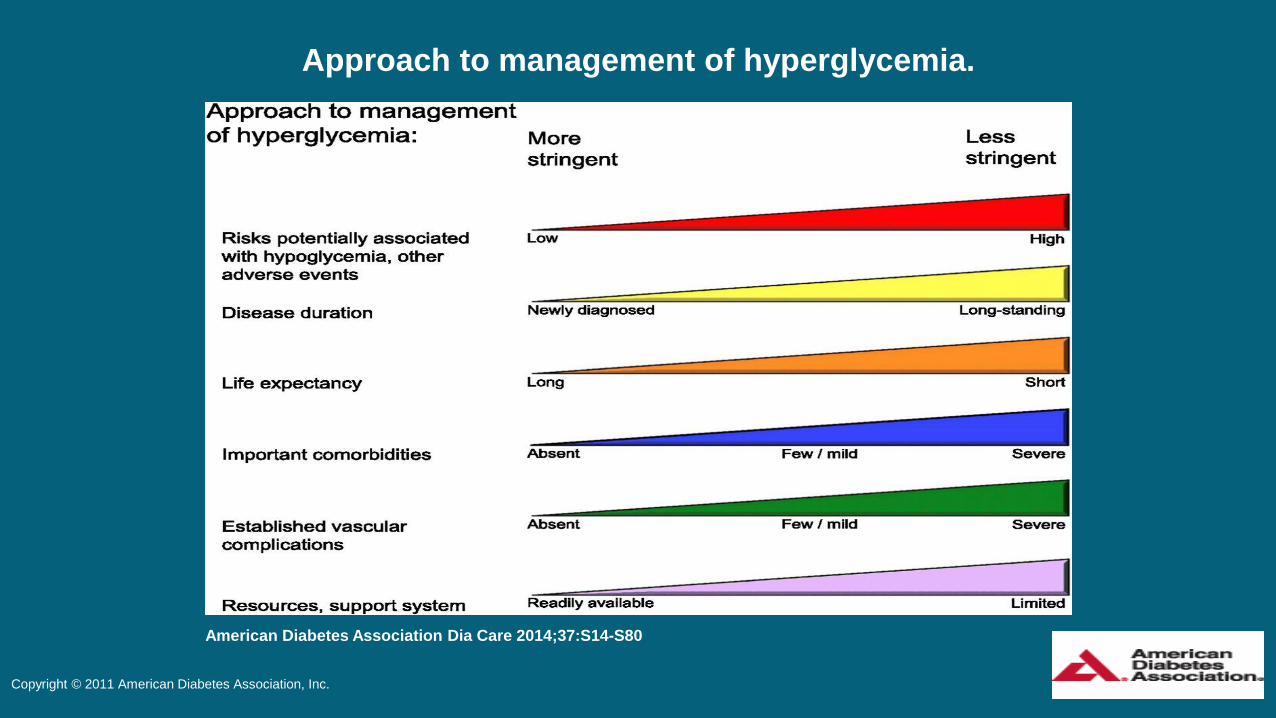
Approach to management of hyperglycemia.
American Diabetes Association Dia Care 2014;37:S14-S80
Copyright © 2011 American Diabetes Association, Inc.

Approach to management of hyperglycemia.
American Diabetes Association Dia Care 2014;37:S14-S80
Copyright © 2011 American Diabetes Association, Inc.
Goals should be individualized based on:
Duration of DM
Age/life expectancy
Comorbid conditions
Known CVD or advanced microvascular complications
Individual patient considerations
More or less stringent glycemic goals may be appropriate for individual patients

Outline RCTs/Clinical Guidelines
CABG vs. PTCA Trials
Glucose Control Studies:
UKPDS
ACCORD
CV Outcome Trials for new medications
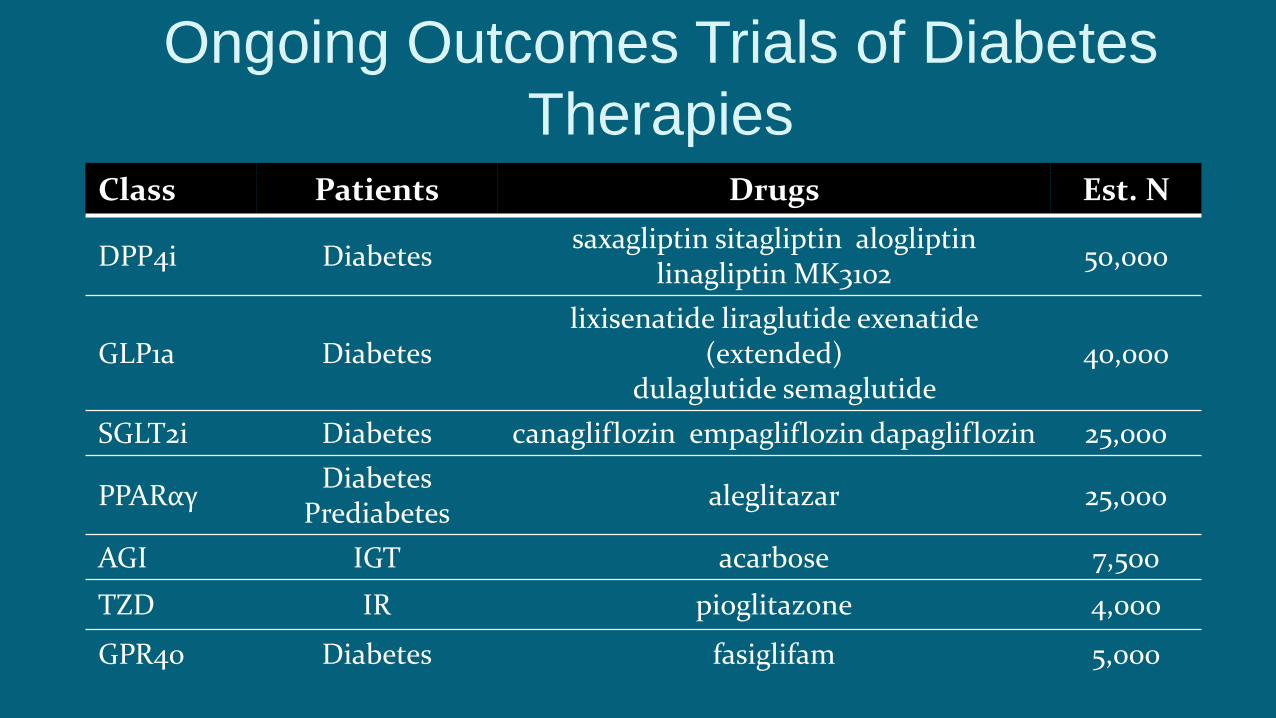
Ongoing Outcomes Trials of Diabetes
TherapiesClass Patients Drugs Est. N
DPP4i Diabetes saxagliptin sitagliptin alogliptin
linagliptin MK310250,000
GLP1a Diabeteslixisenatide liraglutide exenatide
(extended)dulaglutide semaglutide
40,000
SGLT2i Diabetes canagliflozin empagliflozin dapagliflozin 25,000
PPARαγDiabetes
Prediabetesaleglitazar 25,000
AGI IGT acarbose 7,500
TZD IR pioglitazone 4,000
GPR40 Diabetes fasiglifam 5,000
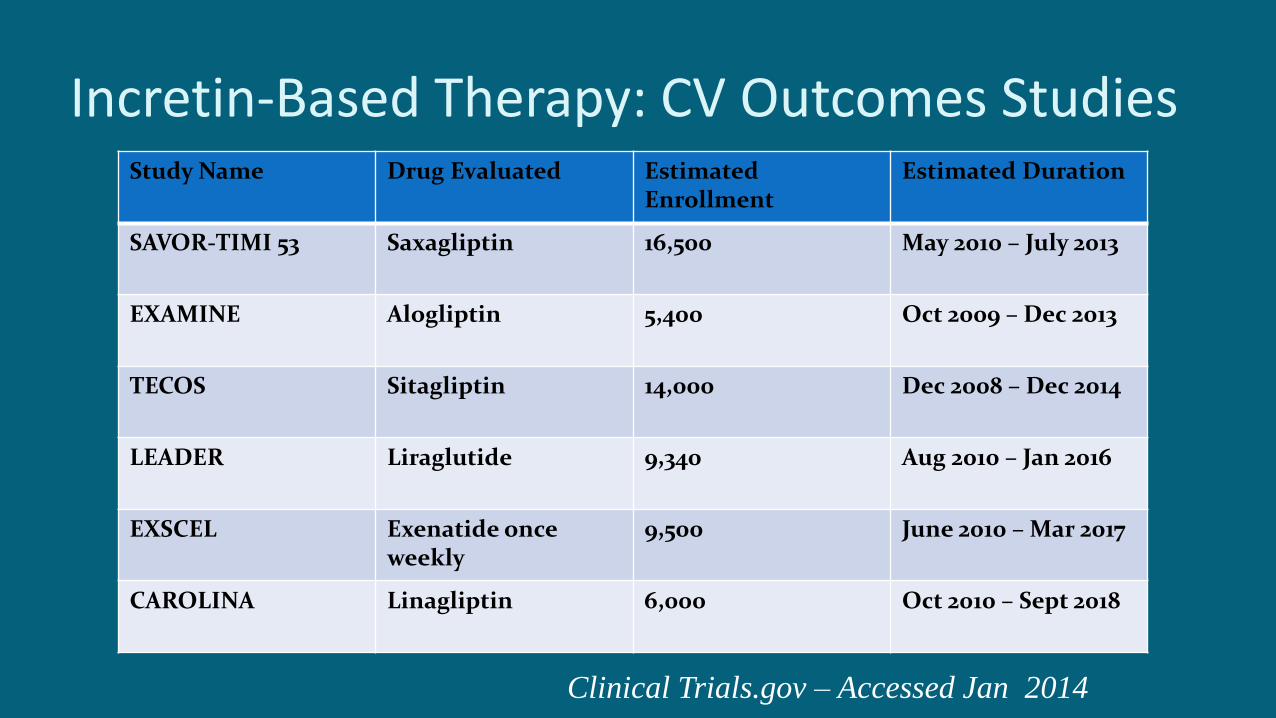
Incretin-Based Therapy: CV Outcomes Studies Study Name Drug Evaluated Estimated
EnrollmentEstimated Duration
SAVOR-TIMI 53 Saxagliptin 16,500 May 2010 – July 2013
EXAMINE Alogliptin 5,400 Oct 2009 – Dec 2013
TECOS Sitagliptin 14,000 Dec 2008 – Dec 2014
LEADER Liraglutide 9,340 Aug 2010 – Jan 2016
EXSCEL Exenatide onceweekly
9,500 June 2010 – Mar 2017
CAROLINA Linagliptin 6,000 Oct 2010 – Sept 2018
Clinical Trials.gov – Accessed Jan 2014

Approved SGLT-2 inhibitorsDrug Name Sponsor Trade Name
Empagliflozin Lilly Jardiance
Dapagliflozin BMS/AZ Farxiga
Canagliflozin J&J Invokana

NEJM 373:2117-28, 2015

Cardiovascular Outcomes and Death from Any Cause.
Zinman B et al. N Engl J Med 2015;373:2117-2128

Glycated Hemoglobin Levels.
Zinman B et al. N Engl J Med 2015;373:2117-2128

Conclusions
• Patients with type 2 diabetes at high risk for cardiovascular events who received empagliflozin, as compared with placebo, had a lower rate of the primary composite cardiovascular outcome and of death from any cause when the study drug was added to standard care.

Benefits/Limitations of SGLT-2 Inhibitors
Benefits: Lowers glucose in a glucose dependent fashion
Modest weight reduction
Effect is additive to metformin
? CV protection
Limitations: Safety

Posted 12/4/2015FDA.gov

How to Treat?

Initial drug monotherapy
Efficacy (! HbA1c)
Hypoglycemia
Weight
Side effects
Costs
Healthy eating, weight control, increased physical activity
Metformin
high
low risk
neutral/loss
GI / lactic acidosis
low
If needed to reach individualized HbA1c target after ~3 months, proceed to 2-drug combination (order not meant to denote any specific preference):
Metformin +
Metformin +
Metformin +
Metformin +
Metformin +
Efficacy (! HbA1c)
Hypoglycemia
Weight
Major side effect(s)
Costs
high
low risk
gain
edema, HF, fx’s‡
high
Thiazolidine- dione
intermediate
low risk
neutral
rare‡
high
DPP-4 Inhibitor
highest
high risk
gain
hypoglycemia‡
variable
Insulin (usually basal)
Two drug combinations*
Sulfonylurea†
+
Thiazolidine-dione
+
DPP-4 Inhibitor
+
GLP-1 receptor agonist
+
Insulin (usually basal)
+
Metformin +
Metformin +
Metformin +
Metformin +
Metformin +
TZD
DPP-4-i
GLP-1-RA
Insulin§
SU†
DPP-4-i
GLP-1-RA
Insulin§
SU† SU†
TZD TZD
TZD
DPP-4-i
Insulin§ Insulin§
If combination therapy that includes basal insulin has failed to achieve HbA1c target after 3-6 months, proceed to a more complex insulin strategy, usually in combination with 1-2 non-insulin agents:
Insulin# (multiple daily doses)
Three drug combinations
More complex insulin strategies
or
or
or
or
or
or
or
or
or
or
or
or GLP-1-RA
high
low risk
loss
GI‡
high
GLP-1 receptor agonist
Sulfonylurea†
high
moderate risk
gain
hypoglycemia‡
low
If needed to reach individualized HbA1c target after ~3 months, proceed to 3-drug combination (order not meant to denote any specific preference):
T2DM Antihyperglycemic Therapy: General RecommendationsDiabetes Care, Diabetologia 19 April 2012. [Epub ahead of print]

Initial drug monotherapy
Efficacy (! HbA1c)
Hypoglycemia
Weight
Side effects
Costs
Healthy eating, weight control, increased physical activity
Metformin
high
low risk
neutral/loss
GI / lactic acidosis
low
If needed to reach individualized HbA1c target after ~3 months, proceed to 2-drug combination (order not meant to denote any specific preference):
Metformin +
Metformin +
Metformin +
Metformin +
Metformin +
Efficacy (! HbA1c)
Hypoglycemia
Weight
Major side effect(s)
Costs
high
low risk
gain
edema, HF, fx’s‡
high
Thiazolidine- dione
intermediate
low risk
neutral
rare‡
high
DPP-4 Inhibitor
highest
high risk
gain
hypoglycemia‡
variable
Insulin (usually basal)
Two drug combinations*
Sulfonylurea†
+
Thiazolidine-dione
+
DPP-4 Inhibitor
+
GLP-1 receptor agonist
+
Insulin (usually basal)
+
Metformin +
Metformin +
Metformin +
Metformin +
Metformin +
TZD
DPP-4-i
GLP-1-RA
Insulin§
SU†
DPP-4-i
GLP-1-RA
Insulin§
SU† SU†
TZD TZD
TZD
DPP-4-i
Insulin§ Insulin§
If combination therapy that includes basal insulin has failed to achieve HbA1c target after 3-6 months, proceed to a more complex insulin strategy, usually in combination with 1-2 non-insulin agents:
Insulin# (multiple daily doses)
Three drug combinations
More complex insulin strategies
or
or
or
or
or
or
or
or
or
or
or
or GLP-1-RA
high
low risk
loss
GI‡
high
GLP-1 receptor agonist
Sulfonylurea†
high
moderate risk
gain
hypoglycemia‡
low
If needed to reach individualized HbA1c target after ~3 months, proceed to 3-drug combination (order not meant to denote any specific preference):
T2DM Antihyperglycemic Therapy: General RecommendationsADA/EASD Position Statement. Diabetes Care June 2012.

Cost for 30 Days Treatment DPP4 Inhibitors: $360-$404
SGLT-2 Inhibitors: $381-$443
GLP-1 Agonists: $300-$740

Minimizing Risk for Hypoglycemia with Insulin
Prescribe insulin that has physiologic action at the lowest possible dose
Patient education (when to eat, carry carbs, know symptoms)
Consider early use of insulin sparing medications (metformin, incretins, acarbose, ? SGLT-2 inhibitors)

Insulin and the Elderly
Interview and involve caregivers
Set realistic goals with patient and family
Facilitate roles of caregivers
Simplify regimen (next slide)
Halter F. Hypoglycemia in the Elderly, ADA Scientific Sessions June 2015
Elderly: Simplify Regimen Take basal insulin in the AM when caregivers are present
Have caregiver give insulin using vial and syringe
Check-mark when insulin is taken
Use pre-filled syringes
Take prandial insulin after meal
Have prepared meals
Re-assess what works
Medha Munshi, ADA Scientific Sessions, 2015
Conclusions RCTs play a greater role in our clinical decisions for diabetes care
Advances in pathophysiology have provided new targets for glucose management
Newer may not always be better
Individualize treatment goals
Start with low doses
Cost considerations
After metformin, individualize therapy

Questions??

Acknowledgements
My Former Team: GU Colleagues and coauthors
My new Team: GU and GW Chief Residents
Shirley Kalwaney MD
Madeline Erario MD
J.P. Verderese MD
Brian Hazen MD
Chappy Venkatasen MD
Hospitalists and Surgical Colleagues
Zobair Younossi MD








![Clement of Alexandria - Ryan Baumann · Clement of Alexandria Author Saint Clement [of Alexandria]](https://img.pdfslide.net/doc/110x75/5c4a7bb193f3c3245e261863/clement-of-alexandria-ryan-baumann-clement-of-alexandria-author-saint-clement.jpg)




















