Embed Size (px)
Citation preview
Stereotactic Ablative Radiation (SABR) for Hepato-biliary
Malignancies
Supriya Sastri Associate Professor, Radiation Oncology
ACTREC, Tata Memorial Centre
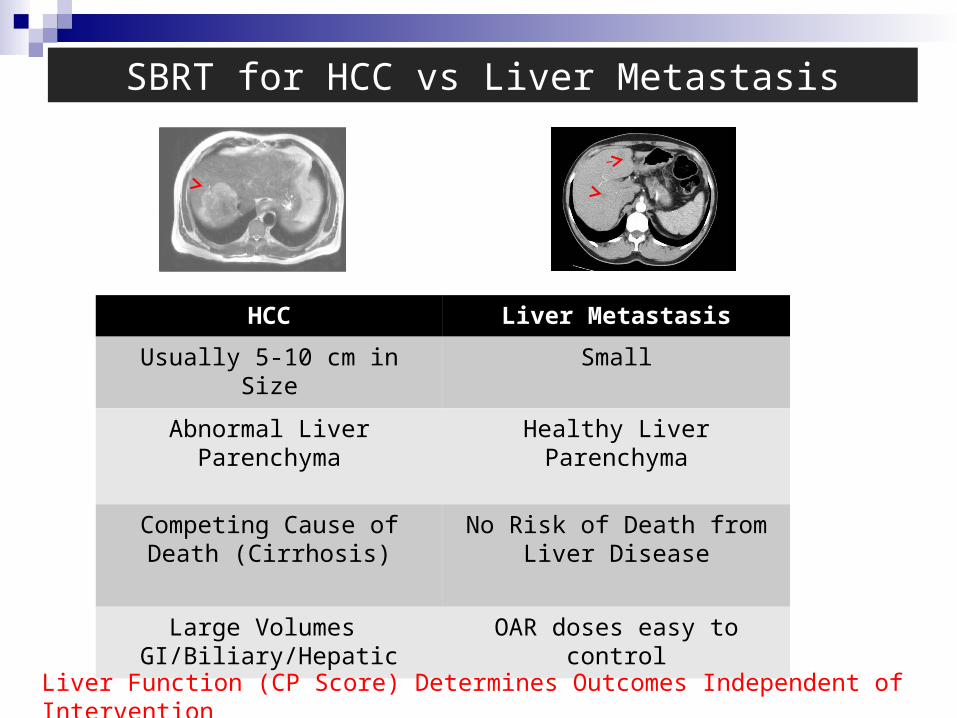
SBRT for HCC vs Liver Metastasis
HCC Liver Metastasis
Usually 5-10 cm in Size Small
Abnormal Liver Parenchyma Healthy Liver Parenchyma
Competing Cause of Death (Cirrhosis)
No Risk of Death from Liver Disease
Large Volumes GI/Biliary/Hepatic
OAR doses easy to control
Liver Function (CP Score) Determines Outcomes Independent of Intervention
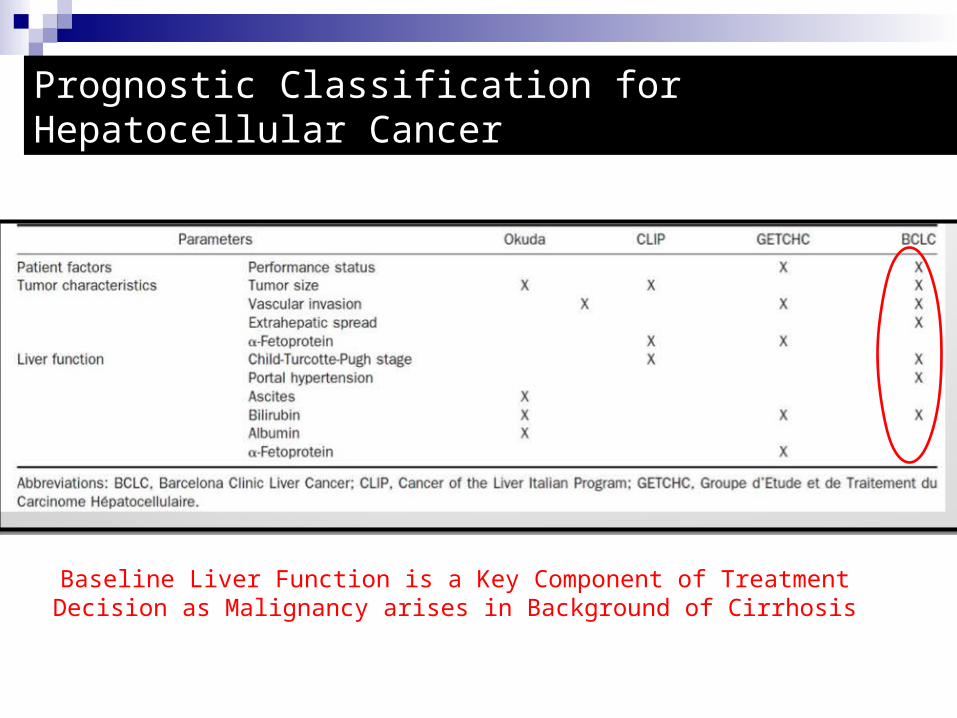
Prognostic Classification for Hepatocellular Cancer
Baseline Liver Function is a Key Component of Treatment Decision as Malignancy arises in Background of Cirrhosis
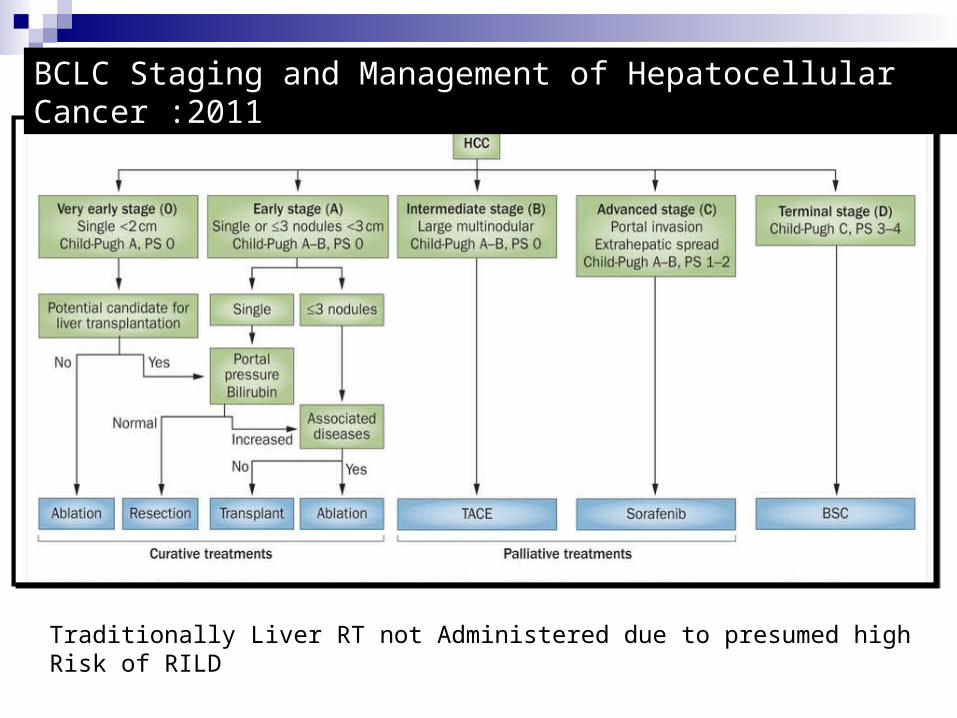
BCLC Staging and Management of Hepatocellular Cancer :2011
Traditionally Liver RT not Administered due to presumed high Risk of RILD
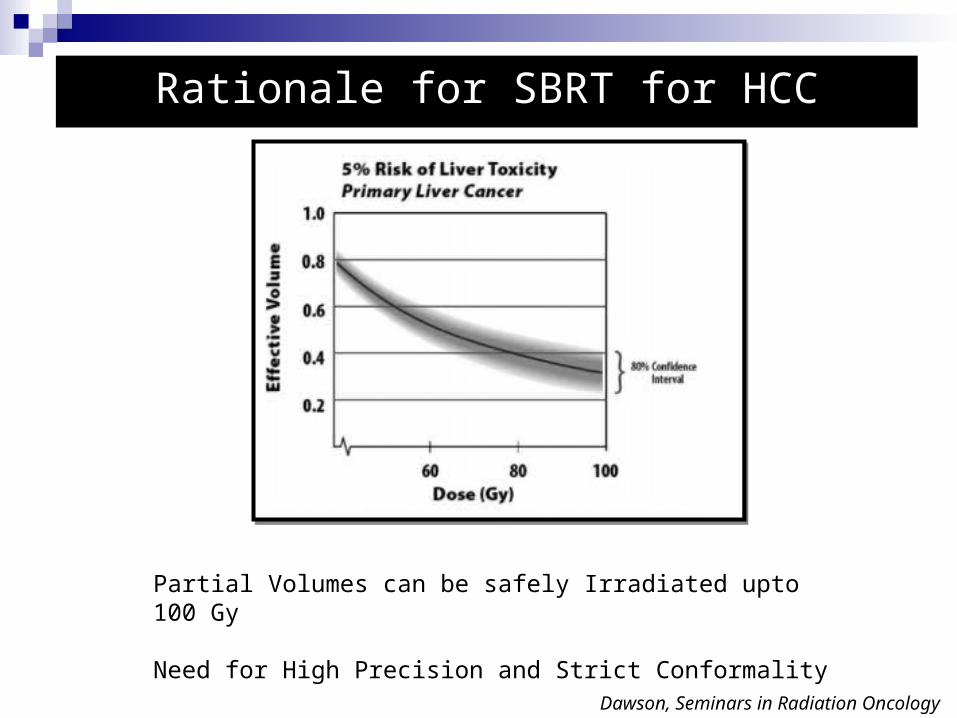
Rationale for SBRT for HCC
Partial Volumes can be safely Irradiated upto 100 Gy
Need for High Precision and Strict Conformality
Dawson, Seminars in Radiation Oncology
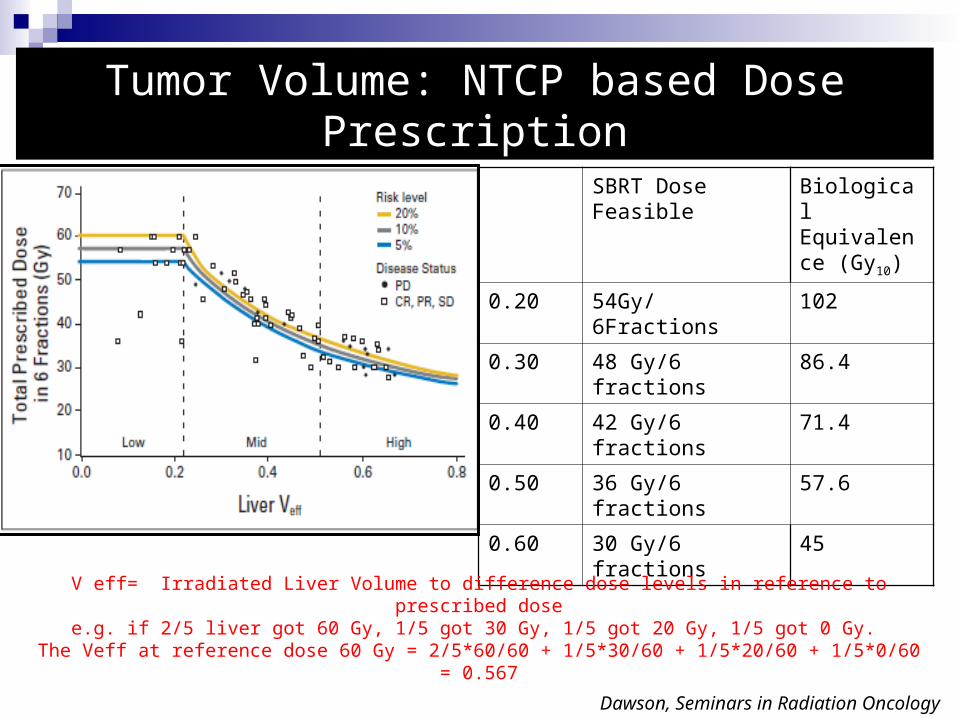
Tumor Volume: NTCP based Dose Prescription
SBRT Dose Feasible
Biological Equivalence (Gy10)
0.20 54Gy/6Fractions 102
0.30 48 Gy/6 fractions 86.4
0.40 42 Gy/6 fractions 71.4
0.50 36 Gy/6 fractions 57.6
0.60 30 Gy/6 fractions 45
Dawson, Seminars in Radiation Oncology
V eff= Irradiated Liver Volume to difference dose levels in reference to prescribed dosee.g. if 2/5 liver got 60 Gy, 1/5 got 30 Gy, 1/5 got 20 Gy, 1/5 got 0 Gy.
The Veff at reference dose 60 Gy = 2/5*60/60 + 1/5*30/60 + 1/5*20/60 + 1/5*0/60 = 0.567
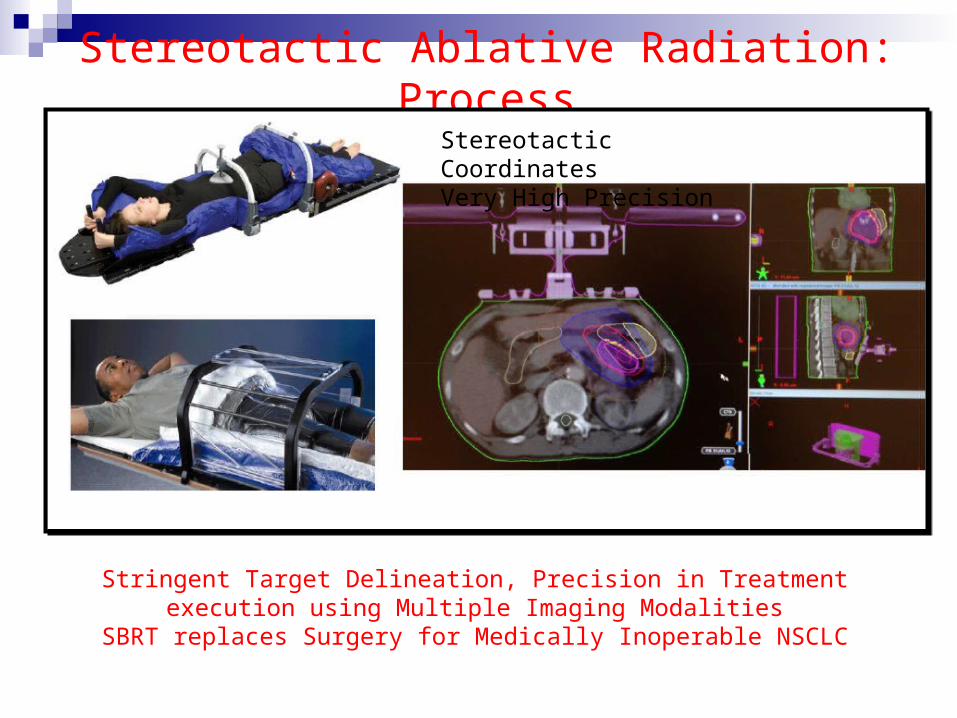
Stereotactic Ablative Radiation: Process
Stringent Target Delineation, Precision in Treatment execution using Multiple Imaging Modalities
SBRT replaces Surgery for Medically Inoperable NSCLC
Stereotactic CoordinatesVery High Precision
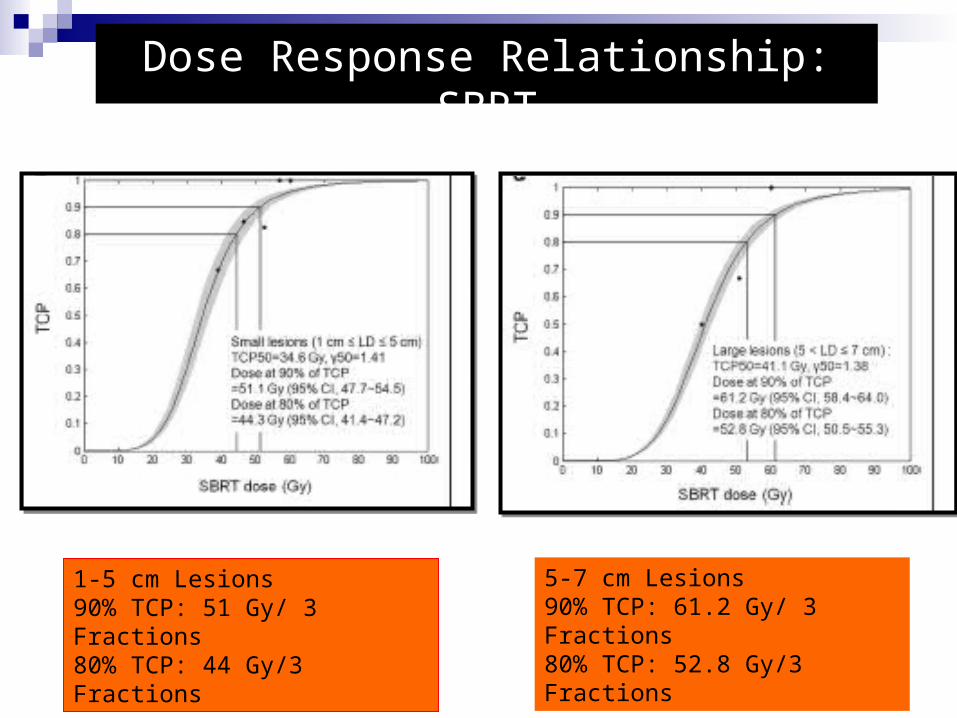
Dose Response Relationship: SBRT
1-5 cm Lesions 90% TCP: 51 Gy/ 3 Fractions80% TCP: 44 Gy/3 Fractions
5-7 cm Lesions 90% TCP: 61.2 Gy/ 3 Fractions80% TCP: 52.8 Gy/3 Fractions
•SBRT : Medically Inoperable
•SBRT : as bridge to transplant
•SBRT: TACE Failures/ Portal Vein Thrombosis
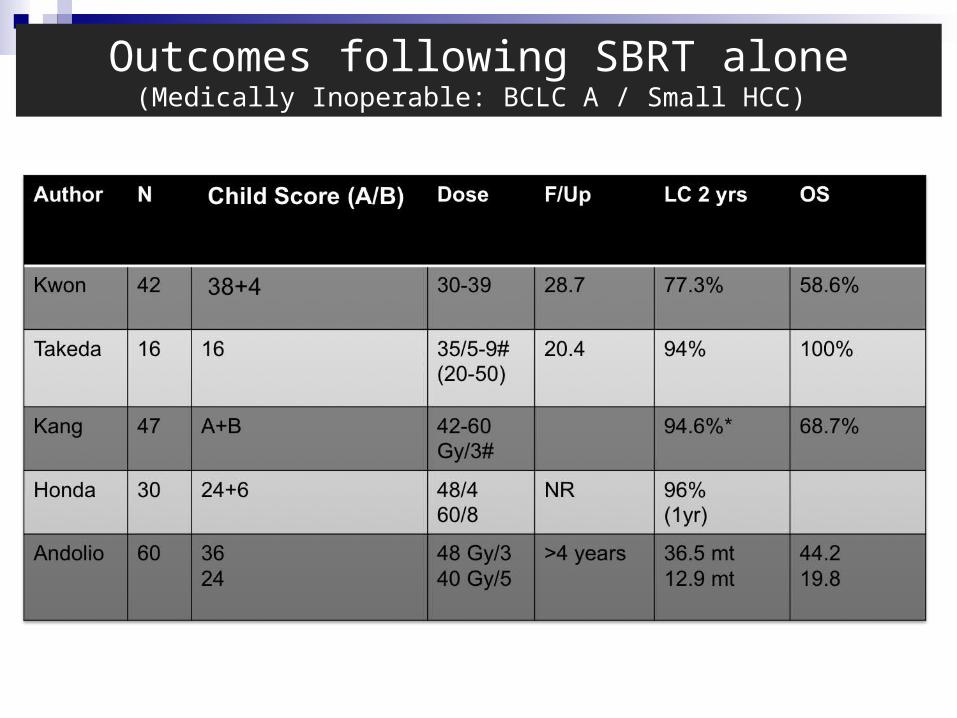
Outcomes following SBRT alone(Medically Inoperable: BCLC A / Small HCC)
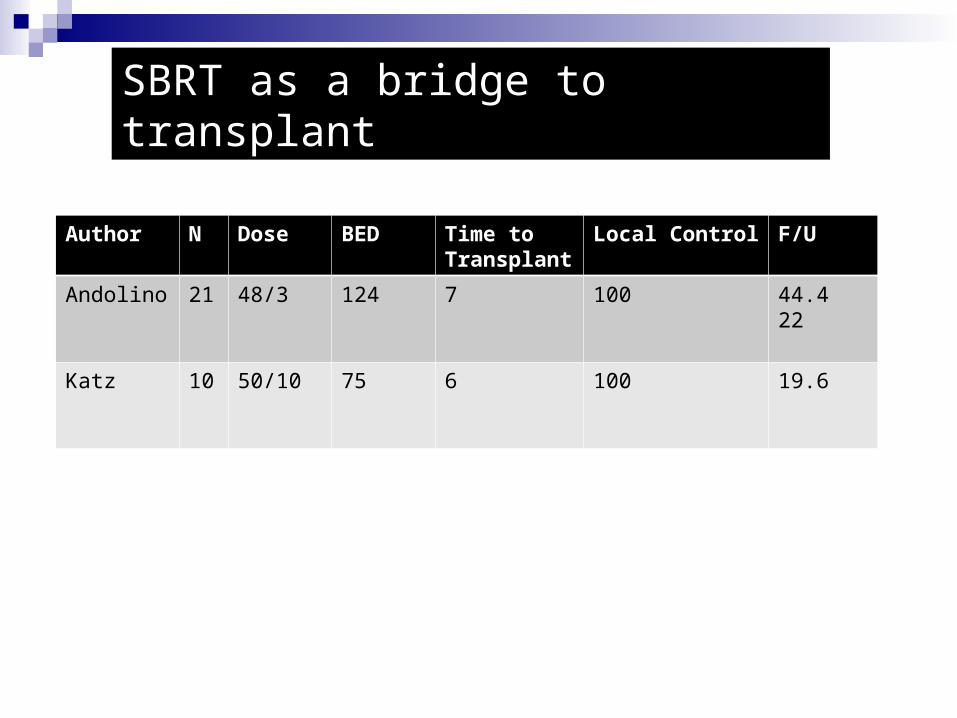
SBRT as a bridge to transplant
Author N Dose BED Time to Transplant
Local Control F/U
Andolino 21 48/3 124 7 100 44.422
Katz 10 50/10 75 6 100 19.6
Author N Child PVT Dose F/UP CR%, PR
%
Survival
*Choi 15
5
A
B
4 PVT 18pat:10x5Gy
2pat: 5x10Gy
23 20
60
22
Méndez 6
2
A
B
3
2 PTV
3-5 x 5-12.5Gy 12.9 NRP 22.1
Tse 31 A/B Yes 36 Gy (24-54 Gy) 26 mths 86% 24
Seo 34
4
A
B
NRP 33-57Gy
40-44 Gy
15 3
61
32
Andolino 36 A
B
NRP A:3x12-16 Gy
B: 5x8Gy
27 30
40
20.4
Cardenes 17 A
B
NRP 48/3
40/5
100% (1yr)
Bujold 102 A 56 (TVT) 6 x 4-9 Gy 31 11 17
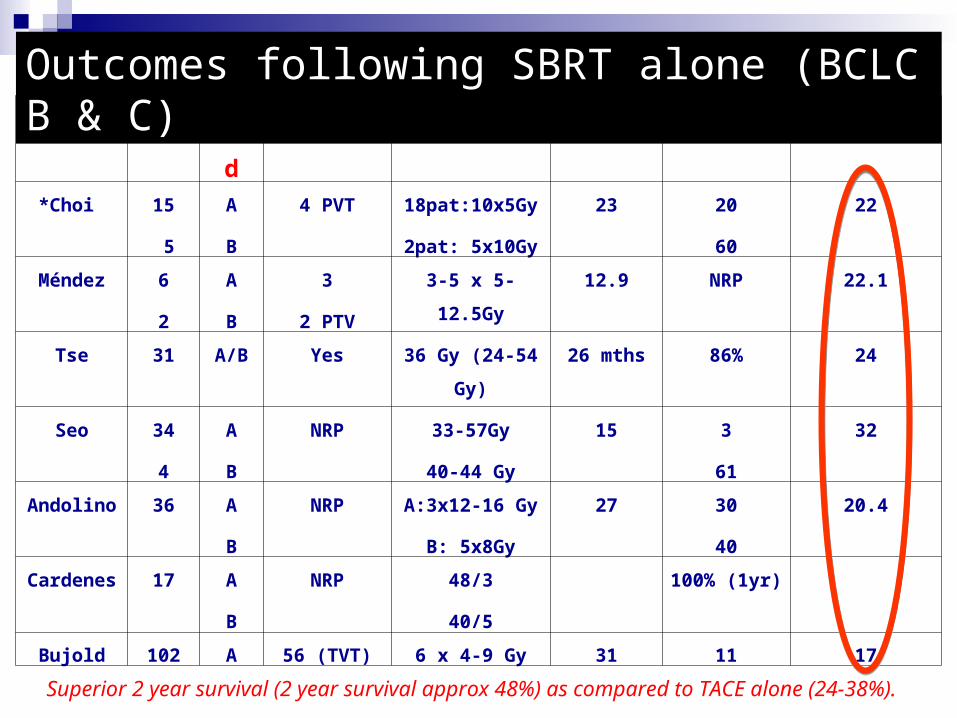
Outcomes following SBRT alone (BCLC B & C)
Superior 2 year survival (2 year survival approx 48%) as compared to TACE alone (24-38%).
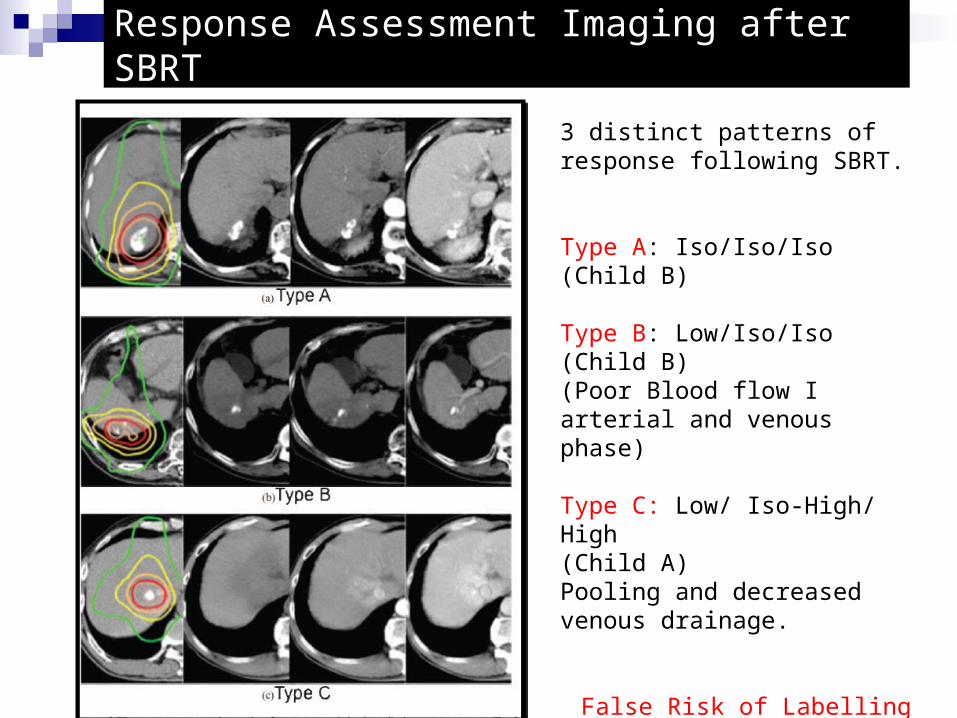
Response Assessment Imaging after SBRT
3 distinct patterns of response following SBRT.
Type A: Iso/Iso/Iso (Child B)
Type B: Low/Iso/Iso (Child B)(Poor Blood flow I arterial and venous phase)
Type C: Low/ Iso-High/ High (Child A)Pooling and decreased venous drainage.
False Risk of Labelling Pseudoprogression
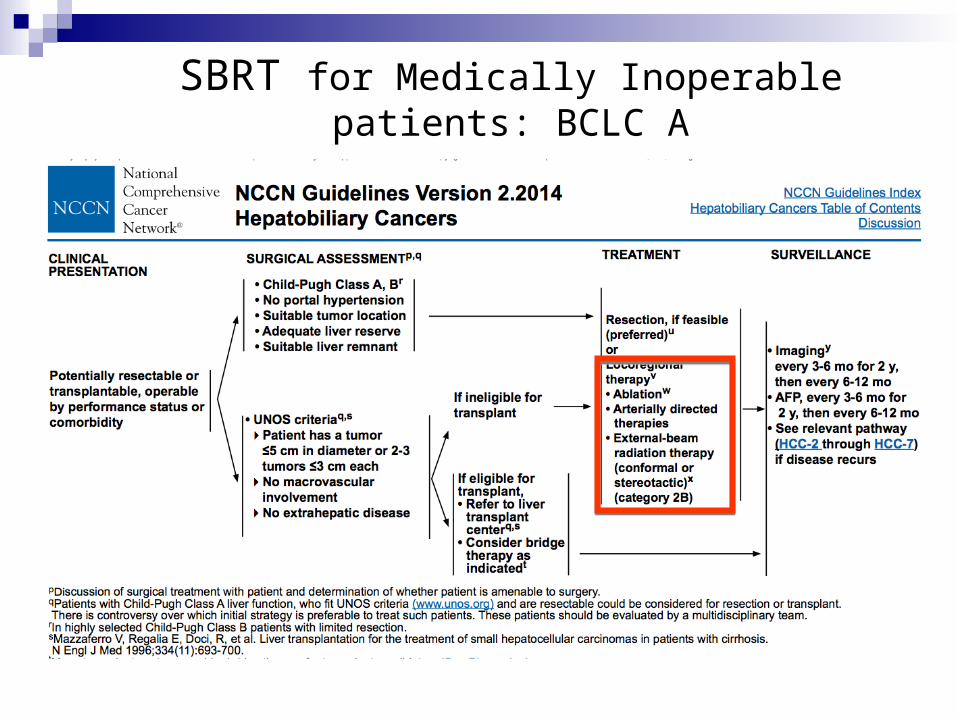
SBRT for Medically Inoperable patients: BCLC A
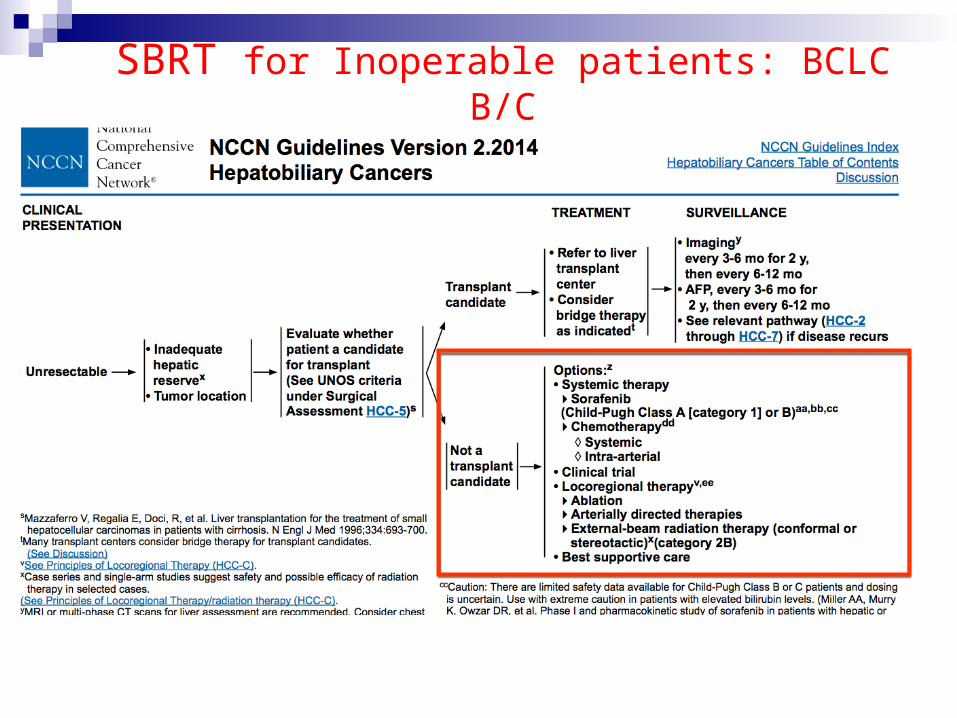
SBRT for Inoperable patients: BCLC B/C
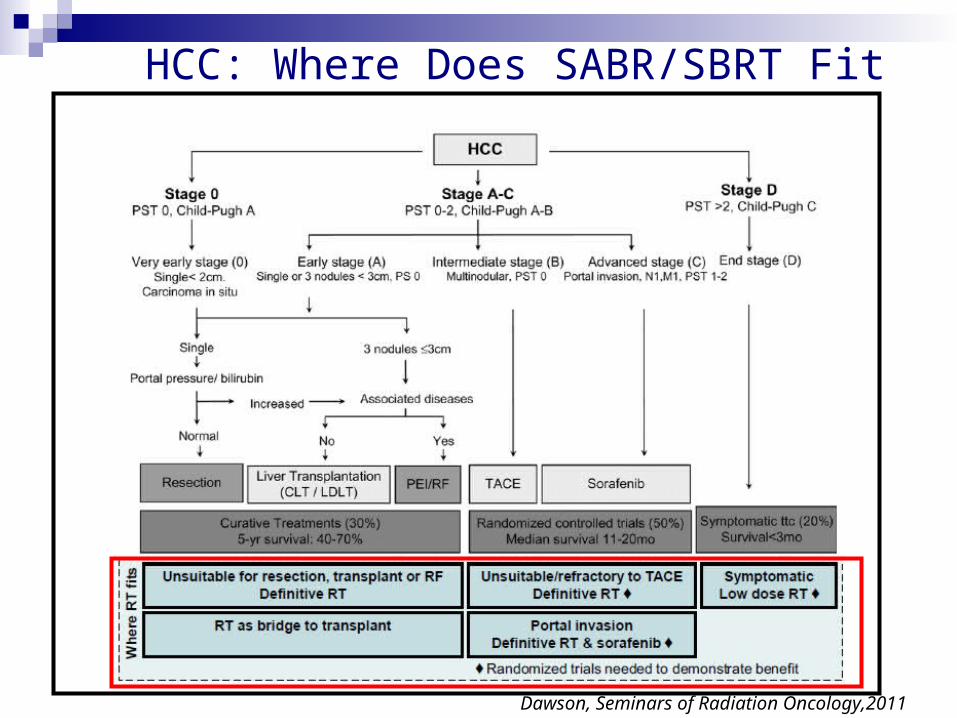
Dawson, Seminars of Radiation Oncology,2011
HCC: Where Does SABR/SBRT Fit In?
SBRT as a part of Multimodality Management of HCC
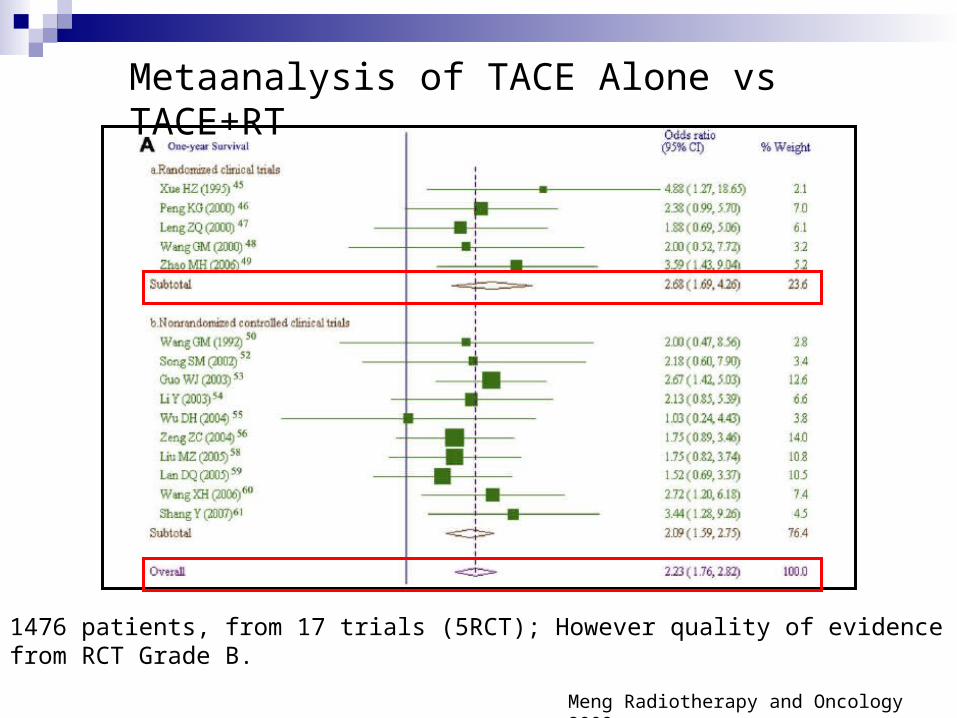
Metaanalysis of TACE Alone vs TACE+RT
1476 patients, from 17 trials (5RCT); However quality of evidence from RCT Grade B.
Meng Radiotherapy and Oncology 2009
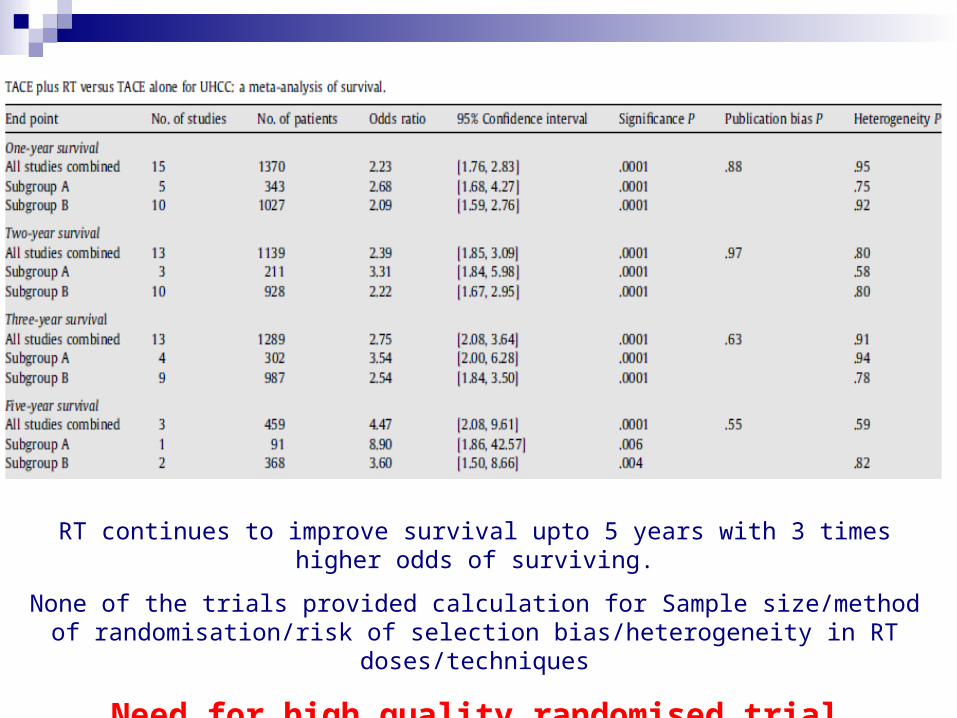
RT continues to improve survival upto 5 years with 3 times higher odds of surviving.
None of the trials provided calculation for Sample size/method of randomisation/risk of selection bias/heterogeneity in RT doses/techniques
Need for high quality randomised trial
Integrated Phase II/ III RCT of DEBTACE/alone or with SBRT for
unresectable HCC
Initiated in ACTREC/TMH 2014,Funded through DAECTC/ Varian
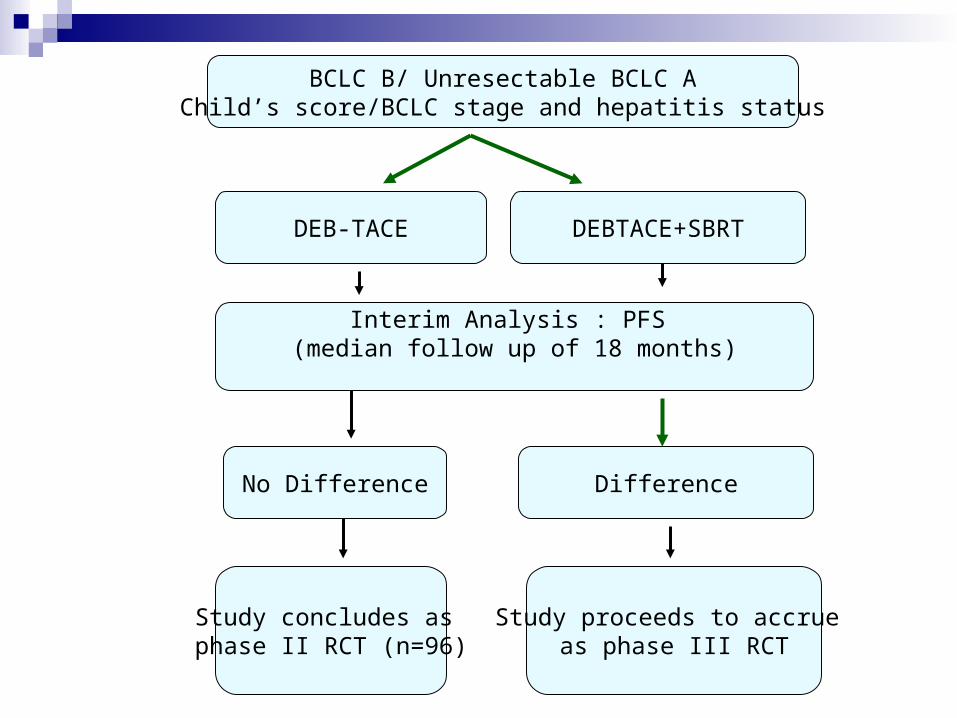
BCLC B/ Unresectable BCLC AChild’s score/BCLC stage and hepatitis status
DEB-TACE DEBTACE+SBRT
Interim Analysis : PFS (median follow up of 18 months)
No Difference Difference
Study concludes as phase II RCT (n=96)
Study proceeds to accrue as phase III RCT
Phase III RCT of TACE vs SBRT for unresectable HCC
International Atomic Energy Association Sponsored and Funded Study
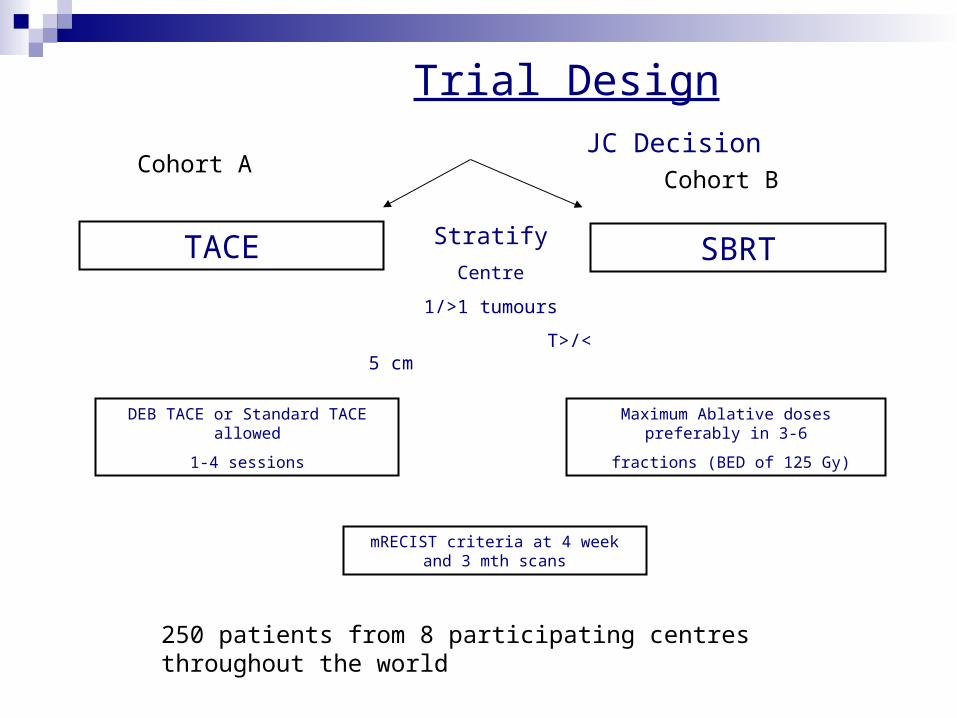
Trial Design JC Decision
TACE SBRTStratify
Centre
1/>1 tumours
T>/< 5 cm
Cohort ACohort B
DEB TACE or Standard TACE allowed
1-4 sessions
Maximum Ablative doses preferably in 3-6
fractions (BED of 125 Gy)
mRECIST criteria at 4 week and 3 mth scans
250 patients from 8 participating centres throughout the world
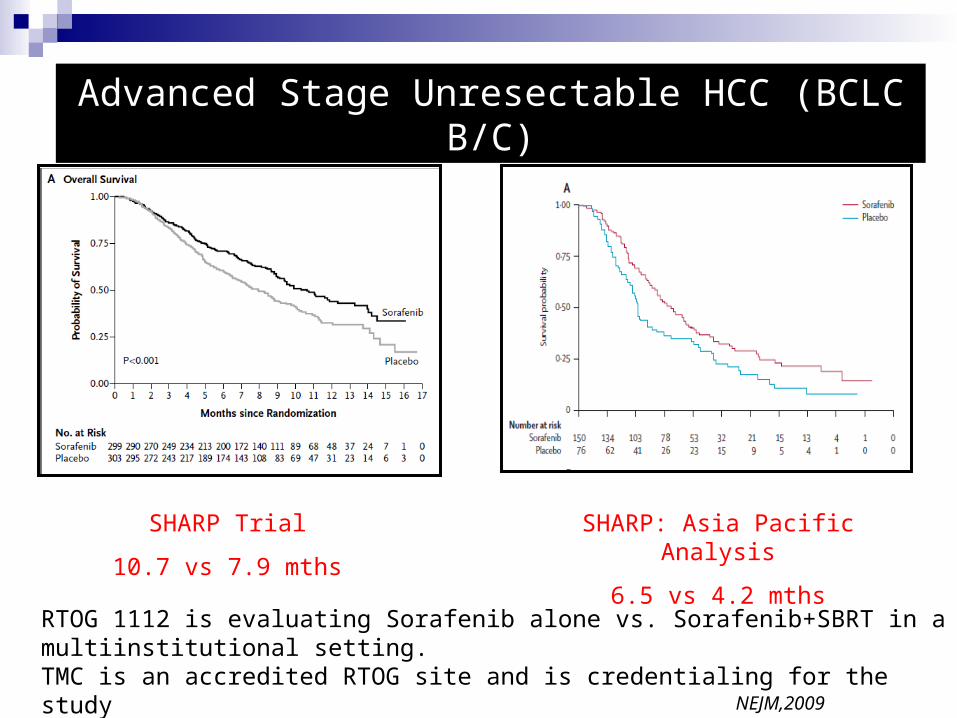
Advanced Stage Unresectable HCC (BCLC B/C)
SHARP Trial
10.7 vs 7.9 mths
SHARP: Asia Pacific Analysis
6.5 vs 4.2 mths
NEJM,2009
RTOG 1112 is evaluating Sorafenib alone vs. Sorafenib+SBRT in a multiinstitutional setting. TMC is an accredited RTOG site and is credentialing for the study
Summary : HCC
Very Encouraging Phase II Data for use of SBRT for HCC. Low Grade III/IV toxicity.
3 Key Randomized Trials will provide the proof for / against use of SBRT in BCLC stage B and C patients.
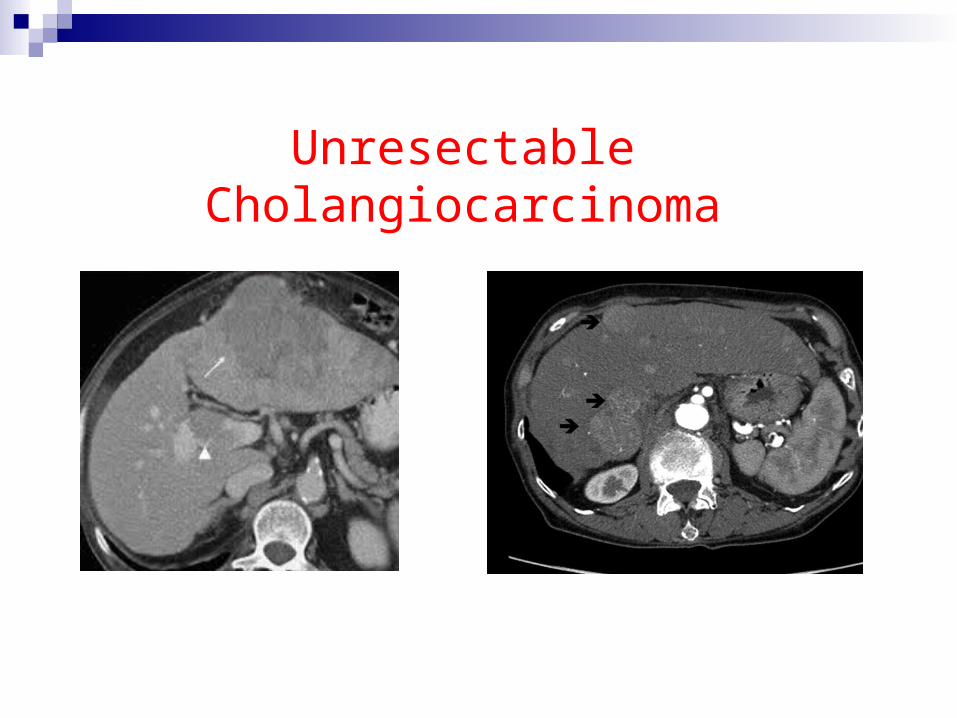
Unresectable Cholangiocarcinoma
For unresectable cholangiocarcinomas, systemic chemotherapy improves survival (8 months vs. 4 months; ABC -01).
Use of doublet chemotherapy is superior to single agent chemotherapy. ( 11.7 vs 8 mths; ABC -02).
ABC-02 had 60% patients with CCA of which 75% had metastasis at presentation.
OAS improved with doublet for entire cohort, however for CCA the overall HR was insignificant
Background
Rationale for RT for cholangiocarcinomas
After upfront resection: Isolated LR 58% (Mayo Clinic)
NACRT prior to liver transplantation: 42% patients had cPR.
Definitive Chemoradiation: Of 52% with progression 74% were local.
Best Results with SBRT combined with systemic chemotherapy (33-35 months)
However SBRT may pose risk of higher toxicity in perihilar location (biliary strictures/cholangitis/ GI toxicity) hence high dose fractionated approach may be more appropriate
Rea DJ,Ann Surg. 2005; Jarnagin WR, Cancer 2003; Kim JK, Abdom Imaging 2003; de Castro SM, J Gastrointest Surg 2004; Crane CH Int. J. Radiation Oncology Biol. Phys.,2002;Alden ME Int J Radiat Oncol Biol Phys 1994;
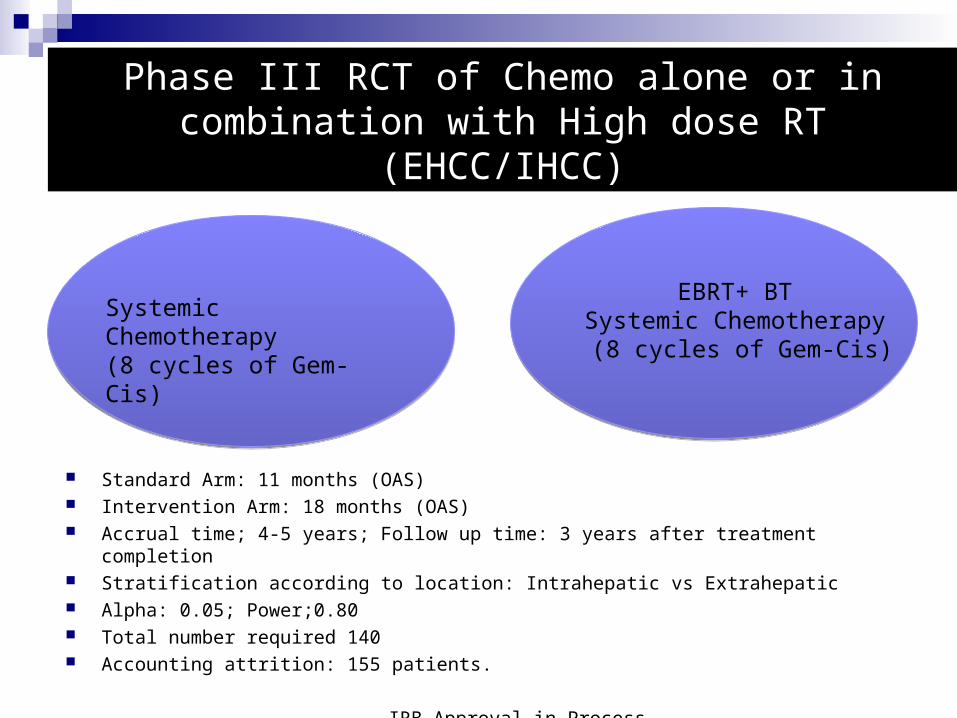
Phase III RCT of Chemo alone or in combination with High dose RT (EHCC/IHCC)
Standard Arm: 11 months (OAS) Intervention Arm: 18 months (OAS) Accrual time; 4-5 years; Follow up time: 3 years after treatment completion Stratification according to location: Intrahepatic vs Extrahepatic Alpha: 0.05; Power;0.80 Total number required 140 Accounting attrition: 155 patients.
IRB Approval in Process
Systemic Chemotherapy (8 cycles of Gem-Cis)
EBRT+ BT Systemic Chemotherapy
(8 cycles of Gem-Cis)
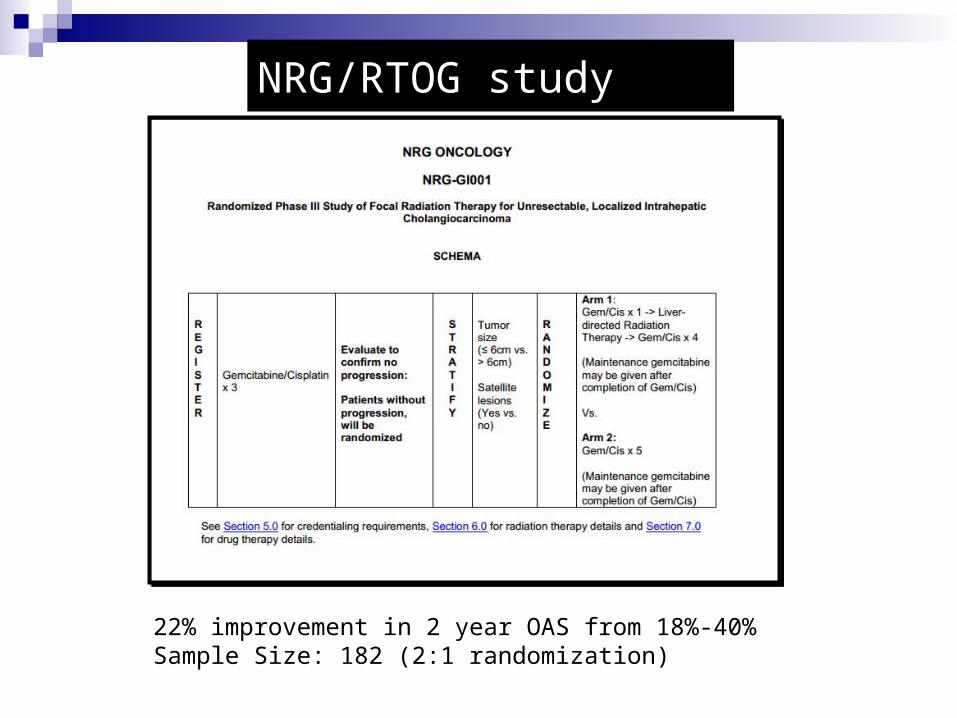
NRG/RTOG study
22% improvement in 2 year OAS from 18%-40%Sample Size: 182 (2:1 randomization)


![Stereotactic Ablative Body Radiation Therapy (SABR): A Resource€¦ · the recommendations detailed in the NPSA report ‘Towards Safety in Radiotherapy’ [1]. In particular the](https://img.pdfslide.net/doc/110x75/5f1cdaf36d3823431859a3cb/stereotactic-ablative-body-radiation-therapy-sabr-a-resource-the-recommendations.jpg)