Embed Size (px)
Citation preview

Sternberg-Reed Cells in the Peripheral Blood
of Patients with Hodgkin’s Disease
By BaavriiA A. BOURONCLE
With the technical assistance of Rosemary Mann
I T IS well known that Hodgkin’s disease can originate in lymph nodes,spleen, liver and other organs of the reticuloendothelial system. From there
it spreads throughout the body by local invasion, by lymphatic dissemination,
and by hematogenous dissemination.
The possibility of the hematogenous dissemination of Hodgkin’s disease was
first suggested by Dorothy Reed’ in her classic description of the morbid
pathology of Hodgkin’s disease in 1902: “These giant cells occur in great
numbers in the large lymph sinuses of the gland and occasionally occur in
blood vessels.” In 1926, Jeanselme and Marchal2 reported Sternberg-Reed cell
emboli observed within blood vessels in biopsied and postmortem organs of a
patient who had died from Hodgkin’s disease. In addition, these giant cells
were described as being frequent in perivascular locations and in some sections
appeared to be passing through a vessel into the parenchyma.
These early observations support the possibility of hematogenous dissemina-
tion of Hodgkin’s disease. However, the presence of Sternberg-Reed cells in
routine peripheral blood smears is a rare occurrence and only 8 isolated cases
have been reported in the world’s literature.31#{176} Among 890 patients studied
in our institution, Sternberg-Reed cells were found in the routine peripheral
blood examinations in only 2 patients with advanced generalized disease.
In this report, we present the results of our search for Sternberg-Reed cells
in the smears of leukocyte concentrates in 135 patients with confirmed diag-
noses of Hodgkin’s disease. We also report our comparative observations of
leukocyte concentrates in the splenic vein and splenic artery of 3 splenecto-
mized patients who had Hodgkin’s disease.
MATERIALS AND METHODS
Method of Study
Among the numeroims miiethods described for the demonstration of cancer cells in the
circulating blood, we chose a simple. but not quantitative, method which is a modification of
the silicone flotation technique of Seal.” This method takes advantage of the differences in
the specific gravity of the various cells.
Dow-Corning Silicone 555 an(l 710 are blended to achieve 5 ml. of solution of a specific
gravity 1.075. Five ml. of fresh heparinized blood is carefully layered above the silicone
From the Department of Medicine, Ohio State University, Columbus, Ohio.
This investigation was supported by Public Health Service Research Grants CA-06196-
OJA1 and CA-06196-02 from the National Cancer Institute.
First submitted June 2, 1965; accepted for publication Aug. 2, 1965.
BERTHA A. BOURONCLE, M.D.: Associate Professor, Department of Medicine, Ohio State
University, Columbus, Ohio.
544
BLOOD, VOL. 27, No. 4 (APRIL), 1966
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom

STERNBERG-R.EED CELLS 545
solution and the tube centrifuged at 1500 rpm for 15 minutes. The Stemberg-Reed cells,
being lighter than 1.075, conic to lie on the surface of the silicone and form a distinct buffycoat which is easily aspirated with a fine Pasteur pipette. Smears are prepared, giving
special care to achieving readily visible edges and are stained with Wright’s stain. Scanning
of 10 slides for each blood sample is carried out by an expert technician. Suspicious cells are
marked on the slide with a mnicrolocator and are then personally examined and photo-
graphed by the author.
Several tests were first employed to determine the effectiveness of the above technic: (1)
Ascites tumor cells were obtained from the abdominal cavity of an infected mouse and
“seeded” in normal human blood. This saniple was processed following our technic. The
ascites tumor cells were present in stained smears in proportionate numbers to the “seeded”
cells. ( 2 ) Areas grossi� involved with Hodgkin’s disease from fresh lymiiph nodes, obtained at
stmrgerv. were scra1)ed and mixed with compatible blood from normal individtmals and then
samples were processed following the described silicone technic. Sternberg-Reed cells were
found in the stained smears proportionally to the amount of the scraped material of the
Hodgkin’s lymph node mixed with the normal blood. From the results of the above 2
experiments. we concluded that our technic is effective in isolating Sternberg-Reed or similar
cells.
Material
Employing the described silicone technic we have examined, for the past 4 years, the
peripheral blood of 135 patients who had confirmed pathologic diagnoses of Hodgkin’s
disease. During this 4-year period of observation, from 1 to 49 determinations were done on
individimal patients during the course of their illness. The total number of determinations
performed was 1060. Seventy-eight patients were males and 57 were females. The age
range was from 8 to 91 years. A group of 50 healthy individuals were used as normal
controls. Another control group consisted of 22 patients with proved diagnoses of lvmpho-
sarcoma.
In each of 3 patients with Hodgkin’s disease who underwent splenectomy for secondary
hypersplenism, 3 samples were obtained at the timime of surgery. The first sample was
obtained from the splenic artery, the second sample from the splenic vein, and the third
sample from the splenic vein after manual squeezing of the spleen by the surgeon. A total of
15 ml. of blood was obtained per sample and was divided into 3 tubes. Ten slides were
made from each tube and reviewed for the presence of Sternberg-Reed cells. A similar
experiment was carried out in three splenectomized control patients; in 1 the diagnosis was
hereditary spherocytosis, and in the other 2 it was idiopathic thrombocytopenia purpura.
RESULTS
Peripheral Blood Studies
The results of our study have demonstrated that in leukocyte concentrate
slides from patients with Hodgkin’s disease a marked increase in monocytes is
present. Many of them are large and young forms, and some have vacuoles.
Such increase in monocytes is more pronounced during the periods of activity
or in the advanced stages of their disease. This finding confirms our observa-
tions in routine peripheral white blood cell differential counts from patients
with Hodgkin’s disease.
In addition to the usual normal cells seen on the routine differential slides,
other cells were found, which are rarely or never found in routine blood
smears. We have arbitrarily classified these cells in 3 groups:
1. Atypical celLs which are rarely found in routine slides but are found in
low number in leukocyte concentrates of normal subjects.
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom

546 I3ERTIJA A. BOURONCLE
2. Abnormal cells which are not found in either routine slides or leukocyte
concentrates of normal subjects.
3. Neoplastic cells of the Sternberg-Reed type which are only found in
patients with Hodgkin’s disease.
Among the atypical cells we found:
a. Atypical mononuclear cells which stand out because of their dark blue,
strongly basophilic cytoplasm. They frequently have a clear perinuclear area
near the nucleus. The chromatin structure of the nucleus can be either coarse
or delicate. Nucleoli are usually distinguished. They most likely represent
altered monocytes. We have found these cells in the slides prepared from
normal subjects hut in greater numbers in patients with Hodgkin’s disease
(Fig. 1).
h. Cells in niitosis ��‘ere very rarely observed in the leukocyte concentrate
slides of our normal control subjects, but they were more frequently found in
patients with Hodgkin’s disease. These mitotic cells were at different stages of
mitosis, and they seem to belong to the atypical mononuclear cells ( Fig. 2).
c. Small hinucleated cells were also found occasionally in the normal huffy
coat; they were numerous and very frequently found in the huffy coat from
Patients with Hodgkin’s disease ( Fig. 3).d. Nuclei of nlegakaryocytes of different sizes and shapes were found fre-
(lilently in the leukocytes concentrates of normal subjects, sometimes sur-rounded by normal platelets. However, intact megakaryocytes were rare. On
the contrary, in patients with Hodgkin’s disease, numerous intact megakaryo-
cytes were found, in some patients as many as 2 or 3 per oil immersion field
( Fig. 4 ). The high incidence of megakaryocytes in leukocyte concentrates has
been reported recently in patients with carcinoma.’�
C . Hi.stiocytes, also described as macrophages or reticnlimm cells, were found
in very small numbers in the leukocyte concentrates of some of the normal
subjects, being found more frequently in patients with Hodgkin’s disease. They
appeared as large cells with abundant cytoplasm, which is pale gray-blue with
a delicate edge, so that the cell membrane is difficult to discern, giving the
appearance of a veil. The cytoplasm contained vacuoles of various sizes, gran-
tiles, cellular debris, phagocytosed red cells, white cells or platelets. The nucle-
us is oval, kidney shaped or round. The nuclear strimcture has a honey-comb
appearance and stains to a light purple color (Fig. 5).
f. Endothelial celLi, often arranged in small clusters surrounded by a large
field of cytoplasm of grayish-blue color, were seldom found in leukocyte con-
centrates of normal subjects; however, they were seen in patients with Hodg-
kin’s disease.
We found that patients with Hodgkin’s disease present other abnormal cells
which are not present in either routine slides or leukocyte concentrates of
normal subjects. They include:
a. Large atypical mononuclear cells are 2 to 4 times larger than a normal
monocyte having large nuclei, with irregular structure and one or several
nucleoli and hasophilic cytoplasm (Fig. 6).
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom

srEnNBEI�(;-1�EED CELLS 547
� -�--- ----I.-- �-. -._-�---
C�. . � �
,.‘ � � w’ 2
ti. � !
� � S. �
� �
� ..
*.‘ ‘iiPlate 1.-Leukocyte concentrates of peripheral blood of patients with Hodgkin’s
disease. Fig. 1: Atypical miiononuclear cell. Fig. 2: Cell in mitosis (mnetaphase)
probably ami atypical miiomionuclear cell. Fig. .3: Small binucleated cell. Fig. 4: Intact
mnegakam’�ocvte. Fig. .5: Histiocvte. Fig. 6: Large atypical rnommonimclear cell. Fig.
�: Large atypical mononuclear cell with minineroims cvtoplasmnic �‘acimoles. Fig. 8:
Large atypical binucleated cell. Reduced 20 P�’ cent from mnagmiificatiom� 2400 x
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom

548 BERTHA A. BOURONCLE
1). Large atypical nicnonuclear celLs with numerous vacitoles ( Fig. 7).
c. Large atypical binucleated cells, some of which are elongated with the
same cytoplasmic and nuclear characteristics of the cells described above ( Fig.
8).
These three groups of abnormal cells resemble pathologically altered retic-
ulu.m cells, and morphologically we can recognize the characteristics of the
transitional stages of reticulum cells.
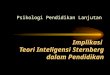
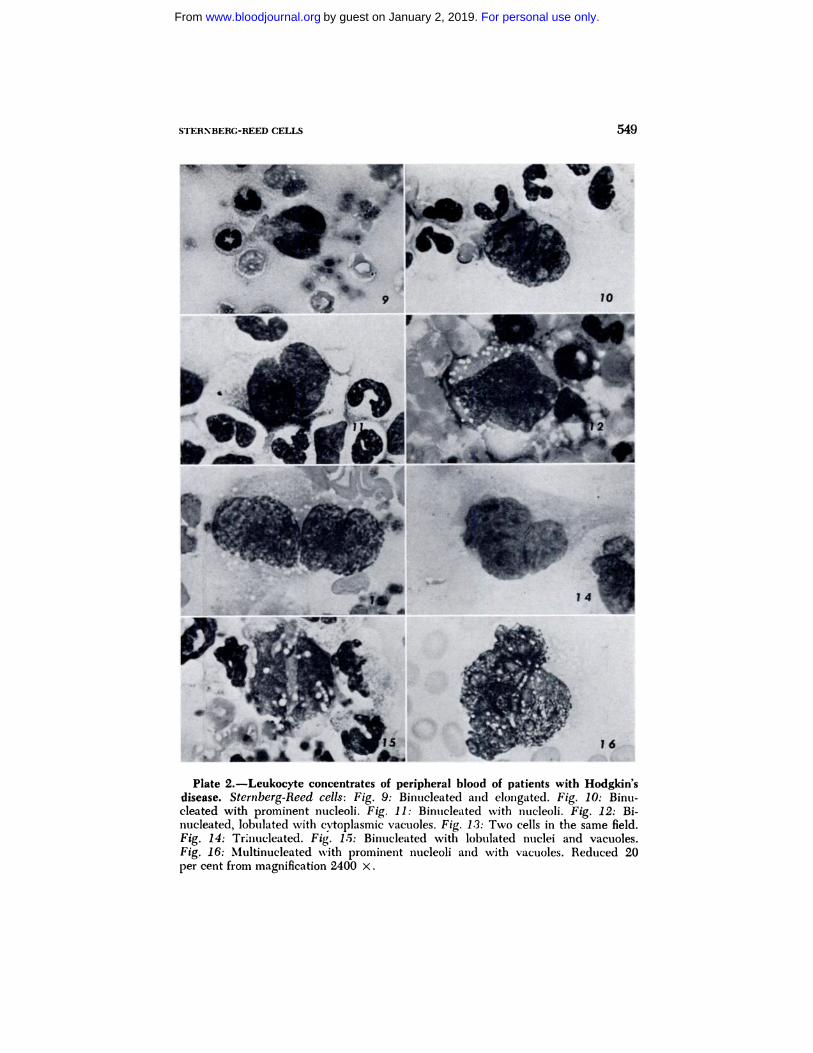
The next group consisted of definitely neoplastic cells and was found only in
the leukocyte concentrates of patients with Hodgkin’s disease. They are differ-
ent morphologic variations of typical Sternberg-Reed cells. Some of them are
as large as 50 microns in diameter. They are mono, binucleate or multinu-
cleated. The nucleus is large, sometimes showing lobulations; the nuclear
chromatin is of variable thickness and staining. The nucleoli are very large,
irregular in shape, and usually deeply stained ( Figs. 9-16).
Among the 135 patients with Hodgkin’s disease s’�died, 85 (63 per cent)
had negative leukocyte concentrates for abnormal cells or Sternherg-Reed
cells. Fifty (37 per cent) were positive. Of this latter group, 25 patients (18.5
per cent ) of the total number of patients studied showed the presence of
typical Sternberg-Reed cells sometime during the course of their illness.
The abnormal cells described were found mainly during the time of activity
of Hodgkin’s disease, but occasionally large atypical hinucleate and large
atypical mononuclear cells were found during the time of clinical remission.
Stemberg-Reed cells were found only in patients showing generalized and
advanced stages of their Hodgkin’s disease. In 18 patients, these cells were
found from 4 months to 1 day prior to death. However, 4 patients in whom
Sternberg-Reed cells were found in the peripheral blood still responded to
therapy and obtained further remissions of 1#{189}to 3 years duration. Three
patients who had Stemberg-Reed cells in their leukocyte concentrates are still
alive and responding to therapy.
We have also observed that the presence of Stemberg-Reed cells has l)cen
more frequently associated with the involvement of abdominal organs by
Hodgkin’s disease.
Splenic Studies
Of interest are the results of our observations in leukocyte concentrates from
samples obtained at the time of splenectomy on 3 patients with Hodgkin’s
disease. Patient 1 was in an advanced stage of Hodgkin’s disease at the time of
surgery, and patients 2 and 3 developed secondary hemolytic anemia while
they were in earlier stages of their disease.
Patient 1 illustrates the results of our splenic studies. We found that after
careful scanning of 10 slides prepared from each of 3 samples, no Sternberg-
Reed cells were found in the first blood sample obtained from the splenic
artery, and only 1 large atypical binucleate cell was seen. In the second
sample, obtained from the splenic vein, 12 abnormal cells and 5 Stemberg-
Reed cells were found. In the third sample, obtained from the splenic vein
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom
15
#{149}1
STERNBERC-REED CELLS 549
Plate 2.-Leukocyte concentrates of peripheral blood of patients with Hodgkin’sdisease. Sternberg-Reed cells: Fig. 9: Bimiucleated and elomigated. Fig. 10: Binu-cleated with prominent nucleoli. Fig. 11: Binucleated with nucleoli. Fig. 12: Bi-
nucleated, lobulated with c�toplasmic vacuoles. Fig. 1.3: Two cells in the same field.
Fig. 14: Trinucleated. Fig. 15: Binucleated with lobulated nuclei and vacuoles.
Fig. 16: Multinucleated with prominent nucleoli and with vacuoles. Reduced 20
per cent from magnification 2400 x.
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom

550 BERThA A. BOURONCLE
after manual squeezing of the spleen by the surgeon, 21 abnormal cells and 12
Stemberg-Reed cells were detected ( Figs. 17-24). Leukocyte concentrates
from peripheral blood, obtained before surgery, revealed the presence of only
1 large binucleated cell. The day after surgery 2 binucleated cells and 1 large
atypical mononuclear cell with vacuoles were found; no Stemberg-Reed cells
were seen.
Pathologic examination of the spleen revealed gross infiltration by Hodgkins
disease. The spleen weight was 919 Gm. Microscopic examination of the spleen
revealed generalized infiltration by Hodgkin’s disease ( Fig. 25).
Special search for the presence of Sternberg-Reed cells in the capillary
vessels of the spleen revealed that many of the sinusoidal vessels of the spleen
contained large atypical reticulum cells which may possibly represent Stern-
berg-Reed cells.
Similar studies done on patient 2 revealed neither abnormal cells nor Stern-
berg-Reed cells in either the splenic artery or the splenic vein samples. In the
samples obtained after mechanical squeezing of the spleen, 22 abnormal cells
and 4 Stemberg-Reed cells were present. Patient 3 showed no abnormal cells
present in the sample obtained from the splenic artery, and 10 abnormal cells
were found equally divided between the splenic vein samples obtained directly
and after squeezing of the spleen.
As control studies, similar splenic samples were obtained in 3 splenecto-
mized patients, 2 of idiopathic thrombocytopenic purpura and 1 of hereditary
spherocytosis. No abnormal cells or Stemberg-Reed cells were found in either
the splenic artery or splenic vein samples obtained before and after manual
s(�ueezing of the spleen. The only occasional large cells found had the morpho-
logic characteristics of histiocytes. Similar cells were also found in the splenic
studies of the splenectomized patients with Hodgkin’s disease ( Fig. 5).
Dis�ussiox
The presence of Stemberg-Reed cells in routine smears of patients with
Hodgkin’s disease is extremely rare. In numerous periodic observations of a
total of 890 patients in our institution, over the past 15 years, such cells were
found only on 2 occasions, or 0.2 per cent. In the world’s literature, only 8
isolated cases have been reported.�’
The presence of Sternberg-Reed cells in routine needle bone marrow aspira-
tions is also rare. In our institution Sternberg-Reed cells have been found in
routine examinations of the bone marrow in 43 of 890 patients studied, or 4.8
per cent. These findings agree with other reports.2’2’ This is probably due to
the scattered focal lesions which may not be aspirated by the sternal needle
and also because the specific lesions in the hone marrow tend to have much
fibrous tissue, making their aspiration more difficult. This explains the practi-
cally constant finding of Hodgkin’s invasion of bone marrow in fatal autopsy
cases.--
The periodic examination of the leukocyte concentrates in 135 patients with
Hodgkin’s disease, conducted over the past 4 years in our laboratory, has
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom

STERNBERC-REED CELLS
I, 23r -�
1”
551
Plate 3.-Leukocyte concentrate of splenic vein samples from patients with Hodg-kin’s disease. Sternberg-Reed cells: Fig. 1 7: Two cells in same field. Fig. 18: Cellwith indented nucleous and cvtoplasmic vacuoles. Fig. 19: Cell with cvtoplasmicvacuoles. Fig. 20: Mononuclear cell with prominent large nucleoli and cvtoplasmic
vacuoles. Fig. 21: Mononuclear cell with large nucleoims and promninemit miucleoli. Fig.
22: Multinucleated. Fig. 23: Multilobulated. Fig. 24: Binucleated with irregular
cvtoplasmic membrane and vacuoles. Magnification for Fig. 17 redtmced 20 per cent
from 2000 X; magnification for Figs 18-24 reduced 20 per cent from 2400 x.
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom

Fig. 25.-Patient 1. Microphotograph of spleen showing areas of infiltration byHodgkin’s disease. Magnification 318 X.
552 BERTHA A. BOURONCLE
revealed the presence of abnormal cells in 50 patients, or 37 per cent. Of this
group, 25 ( 18.5 per cent) also revealed the presence of typical Sternberg-Reed
cells sometime during the course of their illness. A few reports of similar
results in small numbers of patients have been published.8”3”4
The cells we have classified and described previously as abnormal cells
resemble morphologically transitional forms from reticuloendothelial cells. In
previous studies we have supported the view that Sternberg-Reed cells derive
from the reticuloendothelial system, and we have described transitional forms
in electron microscopy observations of lymph nodes of patients with Hodgkin’s
disease.’5 This view is generally accepted.m�m4
The abnormal or transitional cells were found mainly during the time of
activity of Hodgkin’s disease, but on some occasions they were also present
during periods of clinical remission. The Sternberg-Reed cells were found only
in patients with generalized advanced stages of Hodgkin’s disease. In 17 of the
25 patients, these cells were found from 4 months to 1 day prior to death.
However, 7 patients still responded to therapy and obtained further remissions
of from 1#{189}to 3 years duration. Three of the 7 obtained even longer remissions
since they are still alive and continuing to respond to therapy. Consequently,
the presence of Stemberg-Reed cells in the peripheral blood must be consid-
ered as indicating an advanced stage of the disease but not necessarily predict-
ing an immediately fatal outcome.
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom

STERNBERG-REED CELLS 553
In spite of the fact that the technic employed in our study was qualitative,
the incidence of abnormal or transitional cells and Sternberg-Reed cells has
been as high as 40 cells per total number on periodic observations per each
individual patient and from 1 to as many as 30 cells per 5 ml. sample per
individual patient. It is then apparent that the total Sternberg-Reed cells and
transitional cells in the peripheral blood must, at times, be quite high.
Both the abnormal or transitional cells and the typical Sternberg-Reed cells
were found individually isolated in the leukocyte concentrate smears, in con-
trast to cancer cells which are usually found in clusters. The viability of the
exfoliated cells and the ability to overcome the patient’s defenses to form
metastases were not studied.
In some patients who responded to therapy, the Sternberg-Reed cells disap-
l)eared from the peripheral blood. However, this has occurred in some in-stances despite any objective evidence of a remission. It is also important to
emphasize that in our group of 135 patients, 85 (63 per cent) gave negative
findings. Nineteen of the negative patients had far-advanced disease, and they
did not clearly differ in terms of clinical or laboratory findings from the similar
positive group. In some of them, even determinations obtained immediately
prior to death were negative.
It is possible to hypothesize that in patients with active Hodgkin’s disease
Sternberg-Reed cells, transitional cells, other abnormal cells and monocytes are
stimulated in their production from cells of the reticuloendothelial system, in
the lymph nodes, spleen, liver and other organs of the reticuloendothelial
system. The stimulating agent which initiates this process is presently un-
known. However, the production of these various cells from the reticuloendo-
thelial system seems to increase simultaneously. These cells gain entry into the
general circulation. The reason the number of Sternberg-Reed cells is very
small and frequently absent in the peripheral blood is that their large size
militates against their remaining in circulation. They are presumably filtered
by the capillaries of the lungs. Only those cells which escape the first filtering
effect of the capillaries would be found transiently in the peripheral blood. The
concept of a filtering action by the lungs of large cellular elements which may
gain entrance into the general circulation is one which was suggested by
Aschoff23 and applied by Kiyono to the explanation of the low histiocyte count
in arterial blood.24 Simpson25 has demonstrated this same phenomenon to be
true for macrophages in experimental studies done in rabbits. The monocytes,
due to their smaller size, are able to circulate in the peripheral blood and are
found to be markedly increased during the active or advanced stages of Hodg-
kin’s disease.
This hypothesis is further supported by our studies on the incidence of
Stemberg-Reed cells and abnormal or transitional cells in the three splenec-
tomized patients with Hodgkin’s disease. Samples of circulating blood ob-
tained at the time of surgery showed no Sternberg-Reed cells in the samples
obtained from the splenic artery. However, they were present in the samples
obtained from the splenic vein, and in greater number in the samples obtained
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom

554 BER’rIIA A. BOURONCLE
from the splenic vein after manual squeezing of the spleen. Because of the
distribution of the circulation of the spleen, it is possible that the Sternberg-
Reed cells and transitional cells, after they have reached the spleen or after
they are produced in the spleen, find easier access to the circulation. This
might also explain the higher incidence of Sternberg-Reed cells in the periph-
eral blood of patients who had abdominal involvement with Hodgkin’s
disease. In view of their higher circulating number more cells are able to
escape the effect of the capillary filtration. The microscopic study of the path-
ologic sections of the spleen from these patients confirmed the presence of
large atypical reticulum cells inside the splenic veins.
It should be emphasized that the search for Sternberg-Reed cells in the
leukocyte concentrates of patients with Hodgkin’s disease is essentially a re-
search technic and should not he considered as a screening test for Hodgkin’s
disease or a definite prognostic test.
SUMMATIY
Our observations of 135 patients indicate that 37 per cent of those suffering
from Hodgkin’s disease exhibit abnormal cells in the leukocyte concentrates of
the peripheral blood during the course of their illness. Typical Sternberg-Reed
cells were found in 18.5 per cent of patients and were present only in the
advanced stages of generalized Hodgkin’s disease.
The presence of Sternberg-Ileed cells in the peripheral blood indicates an
advanced stage of the disease l)ut does not necessarily predict an immediately
fatal outcome.
Comparative studies, searching for Sternberg-Reed cells in the splenic circu-
lation, showed no Sternberg-Reed cells to he present in the splenic arteries of
patients with Hodgkin’s disease; but numerous Sternberg-Reed cells were pres-
ent in the splenic vein, particularly after mechanical squeezing of the spleen.
A possible hypothesis is given to support the evidence for the circulation of
Sternberg-Reed cells and an explanation for their lower incidence in the pe-
ripheral blood.
Our observations support the hematogenous metastasis of Hodgkin’s disease.
SUMMARIO IN INTERLINCUA
Nostre observationes in 135 patientes indica que 37 pro centa del casos de
morbo de Hodgkin es characterisate durante Ic curso clinic per cellulas
anormal in le concentratos leucocytic dcl sanguine peripheric. Typic cellulas
de Steriiberg-Reed esseva trovate in 18,5 pro cento del patientes e esseva
presente solmente in le stadios avantiate de generalisate morbo de Hodgkin.
Le presentia de cellulas de Sternberg-Reed in Ic sanguine peripheric indica
tin stadio avantiate del morbo sed non predice necessarimente un imminente
exito mortal.
Studios comparative, cercante cellulas de Sternberg-Reed in Ic circulation
splenic, revelava nulle tales in Ic arterias splenic de patientes con morbo de
Hodgkin, sed numerose cellulas de Sternberg-Reed esseva presente in le vena
splenic, particularmente post compression mechanic del splen.
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom
STERNBERC-REED CELLS 555
Es formulate un hvpothese in supporto del evidentia pm Ic circulation de
cellulas de Sternberg-Reed e un explication pro br plus basse incidentia in Ic
sangtmine peripheric.
Nostre observationes supporta le conception del metastase hematogene de
morbo de Hodgkin.
ACKNOWLEDGMENTS
We are grateful to Doctors Charles A. Doami and Jacob \V. Old for their suggestions ammd
review of this manuscript.
REFERENCES
1. Reed, D. \I.: On the pathological
changes in Hodgkin’s disease, with
especial reference to its relation to
tuberculosis. Johns Hopkins Hosp.
Rep. 10:133-196. 1902.
2. jeanselme, E.. and Marchal, C. : Corn-
mnentaires sur Un cas de maladie de
Hodgkin a evolution aigii#{233}. Diss
#{233}mi�ination Par la voie sanguine
d’emiibolies a celhmles de Sternberg.
Reaction de Bordet-Wassenuan oscil-
lante, Ann. Med. 20: 1-26, 1926.
:3. Isaacs. R.: Hodgkin’s disease. Med. Cliii.
N. Amer. 28:201-213, 1944.
4. Ludmiian, H.. and Spear. P. W.: Reed-
Sternberg cells in the peripheral
blood. Report of case of Hodgkin’s
disease. Blood 12: 189-192. 1957.
5. Varadi, S.: Reed-Sternherg cells in the
peripheral blood amid bone-marrow in
Hodgkin’s disease. Brit. Med. j.
1:1239-1243, 1960.
6. Chrob#{225}k,L., and Hor#{225}c#{232}k,J.: Maligmil
lvmfogranulomii s n#{225}lezem neohvyk-
l�’ch btmn#{233}kv perifernI krvi. Casop.
l#{233}k.#{232}esk. 99:1305-1308, 1960.
7. Keiser, V. C.: Tumorzellausschwemmi-
numng bei malignen Tumiioren des lymu-
phatishen rmnd reticul#{228}ren Systems.
Acta Haemat. 23:29-46, 1960.
8. Lib#{225}nsk�’. J.. Bedn#{225}�. B., and Buzek, J.:Sternberg cells (Reed cells) in periph-
eral blood in a patient with Hodg-
kin’s disease. Neoplasmu 9:411-428,
1962.
9. Reves del Pozo. E.: Hallazgo de celulas
Sternberg-Reed en la medula osea en
cuatro casos de enfermedad de Hodg-
kin. Arch. Peruanos Pat. Clin. 14:173-
202, 1960.
10. Scheerer. P. P.. Pierre, R. V.. Schwartz,
D. L.. and Linmnan, J. W.: Reed-Sternberg-cell leukemia and lactic aci-
dosis. New Emmg. J. NIe(l. 270:274-278.
1964.
1 1. Seal, S. H.: Silicomie flotation: A Simnl)le
quantitative method for the isolationof free-floating cancer cells from the
blood. Cancer 12:590-595, 1959.
12. Flimnie, R., West. J. T.. Malmgren. R. A..
and Chu, E. A. : Qimamititative observa-
tions of circulating niegakaryocytes in
the blood of patients with cancer.
New Eng. J. Med. 270:111-117. 1964.
13. Marchal. C.. Perles, S., Fertakis, A.. amid
Cool. V. : Les niigrations sanguines des
cellules (IC Sternberg dans la maladie
de Hodgkin ( leuco-concentration).
Scm. Hop. Paris 38:568-571, 1962.
14. Stoflerg. A. NI. M.: The significance of
the letmkocyte concentrate in the
demonstration of tumiiotmr cells in the
blood. Acta Haeniat. 29:65-79. 1963.
15. Frajola. W. J.. Creider. M. 11.. Boo-
roncle, B. A., iifl(l Doami. C. A. : Elec-
tron niicroscopv of lymph miodes of
patients with Hodgkin’s disease and
allied (lisor(lers. Proc. 6th Intern.
Congr. Hemiiatol.. 1956. pp 231-238.16. Doan, C. A.. and Wisemuan, B. K.: The
muonocvte. muonocvtosis and muonocvtic
letmkosis: A clinical and pathologicalstudy. Anmi. Imit.Med. 8:383-416. 1934.
17. Moeschlin. S.. Schwarz. E.. amid Wamig.
H.: Die Hodgkinzellen als Tmmmorzel-
len. Schweiz. Med. Wschr. 80:1103-
1112. 1950.
18. Hoffmanmi, C. T.. and Rottino, A.: Phase
microscopy studies of Hodgkin’s dis-
ease lymph nodes in relation to histo-
genesis of the Sternbcrg-Reed cell.
Blood 5:74-78, 1950.
19. Petrakis, N. L.. Bostick, W. L.. amid Sie-
gel. B. V.: The deoxyribonucleic acid
(DNA) content of Sternberg-Reed
cells. J. Nat. Cancer Inst. 22:551-554
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom

556 BERTHA A. BOURONCLE
1959.20. Limarzi, L. R., and Paul, J. T.: Sternal
marrow studies in Hodgkin’s disease.
A review of the literature and a reportof thirty-five cases. Amer. J. Clin.Path. 19:929-961, 1949.
21. Bayrd. E. C., Paulson, C. S., and Har-
graves, M. M.: Hodgkin’s specific cellsin bone niarrow aspirations. A brief
review and report of two cases. Blood
9:46-56, 1953.22. Hashimoto, M., and Hanazato, Y.:
Study on bone marrow of autopsy
cases in Hodgkin’s disease. J. Kyu.
Hem. Soc. 11:193-208, 1961.
23. Aschoff, L.: Em Beitrag zur Lehre vonden Makrophagen auf grund von un-
tersuchungen von Dr. Kiyono. Ver-handl. d. Deutsch. Path. Geselsch., 16Tagnung, 1913.
24. Aschoff, L., and Kiyono, K.: Zur Frageder grossen Mononuklearen. Folia
Haemat. 15:149-150, 1913.
25. Simpson, M. E.: The experimental pro-
duction of macrophages in the circula-
ting blood. J. Med. Res. 43:77-144,
1922.
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom

1966 27: 544-556
BERTHA A. BOURONCLE and Rosemary Mann DiseaseSternberg-Reed Cells in the Peripheral Blood of Patients with Hodgkin's
http://www.bloodjournal.org/content/27/4/544.full.htmlUpdated information and services can be found at:
Articles on similar topics can be found in the following Blood collections
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of
For personal use only.on January 2, 2019. by guest www.bloodjournal.orgFrom