Embed Size (px)
Citation preview
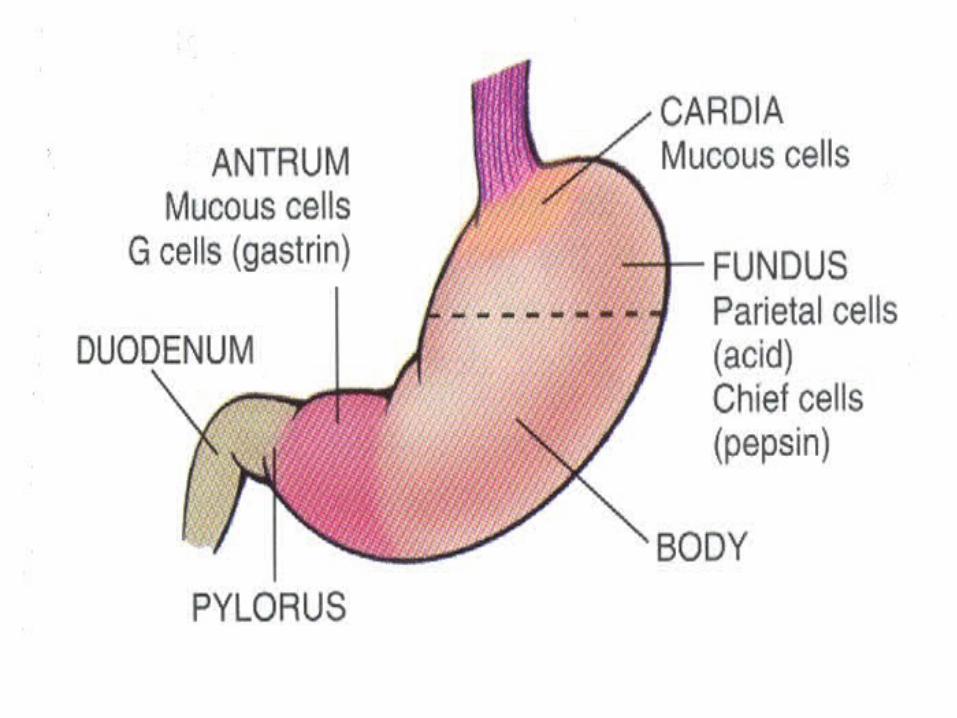
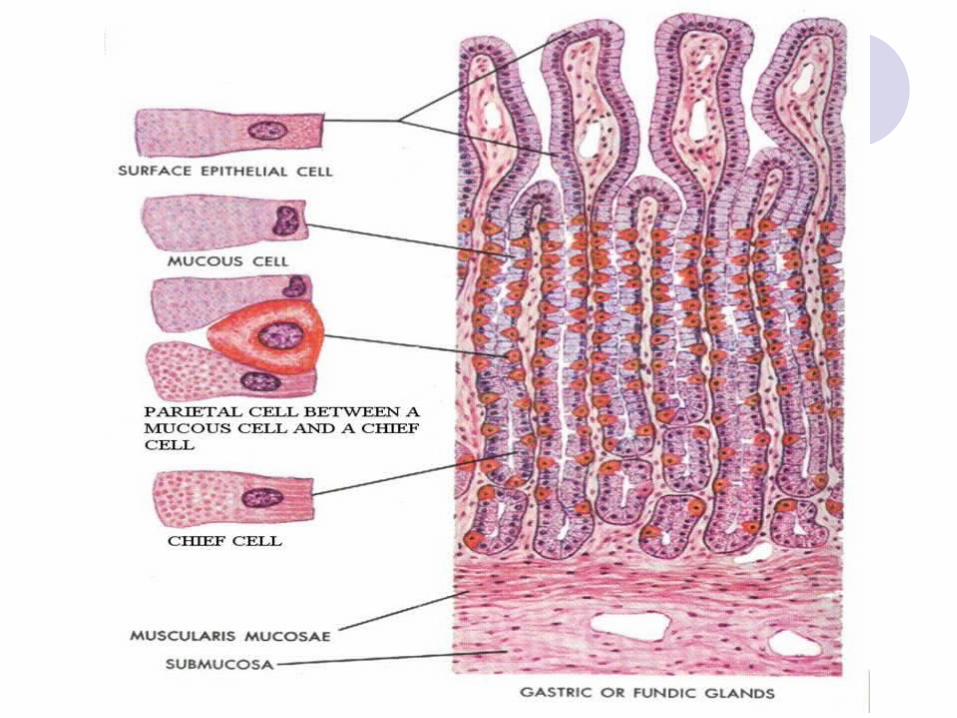
STOMACH Cell types:
Mucosal surface & foveolae: Surface foveolar cells - secrete mucous
Mucous neck cells - progenitor cells Glands:
Mucous cells - secrete mucous & pepsinogen II
Parietal cells - secrete HCl & IFChief cells - secrete pepsinogen I & IIEndocrine cells - secrete peptide & amine
hormones
• Congenital Anomalies
CONGENITAL ANOMALIES
Diaphragmatic Hernia:
Defect in diaphragm, away from esophageal hiatus
Portions of stomach & SI herniate pulmonary hypoplasia & respiratory impairment
CONGENITAL ANOMALIES
Heterotopic rests:
Location: Anywhere in the GITMC: Pancreatic & gastricS/S: Usually asymptomatic but may cause
ulceration
CONGENITAL ANOMALIES
Congenital Hypertrophic Pyloric Stenosis:CHiPs
M > F (3:1), 1 in 200 infant males, multifactorial inheritance
Cause: Hypertrophy & hyperplasia of circular muscle of pylorus
regurgitation, projectile non- bilious vomiting commences at 2 - 6 wks of age
May be due to defective autonomic regulation Dx: Visible peristalsis & palpable mass in RUQ Tx: Pyloromyotomy is curative

ACUTE GASTRITIS
Other Causes:
Ingestion of strong acids or alkaliCa chemotxRadiationIschemia & shockNGTs
- Reduced mucosal blood flow - Direct damage to mucosal epithelium
ACUTE GASTRITIS
Clinically:
Asymptomatic to epigastric pain of varying severity, up to acute abdomen w/ hematemesis & shock
major cause of massive hematemesis (esp. alcoholics)
Common in those who take daily aspirin for RA
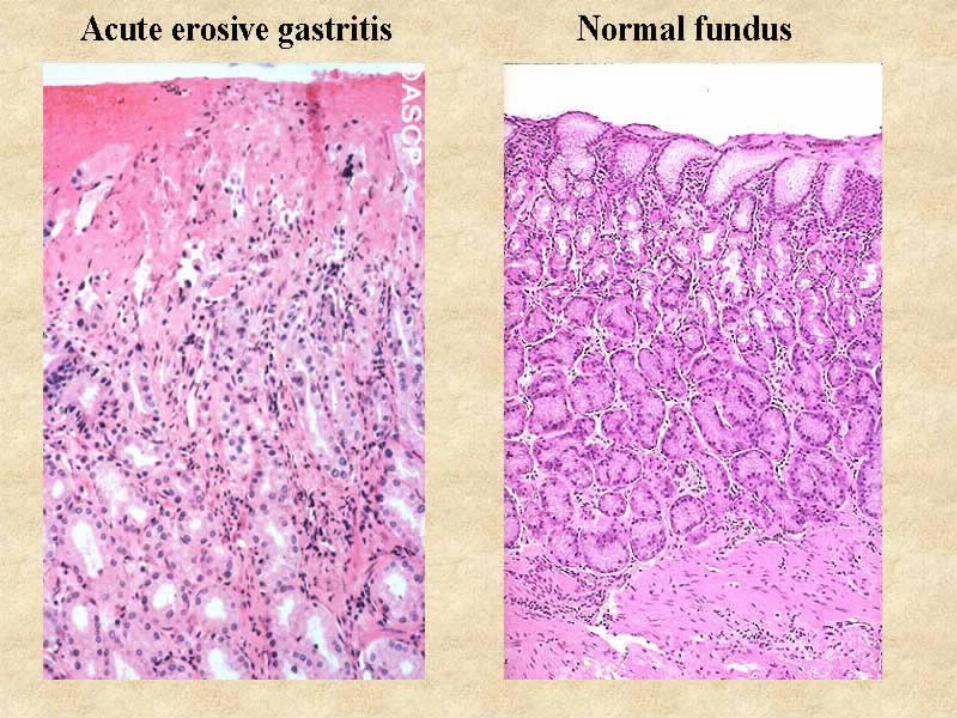
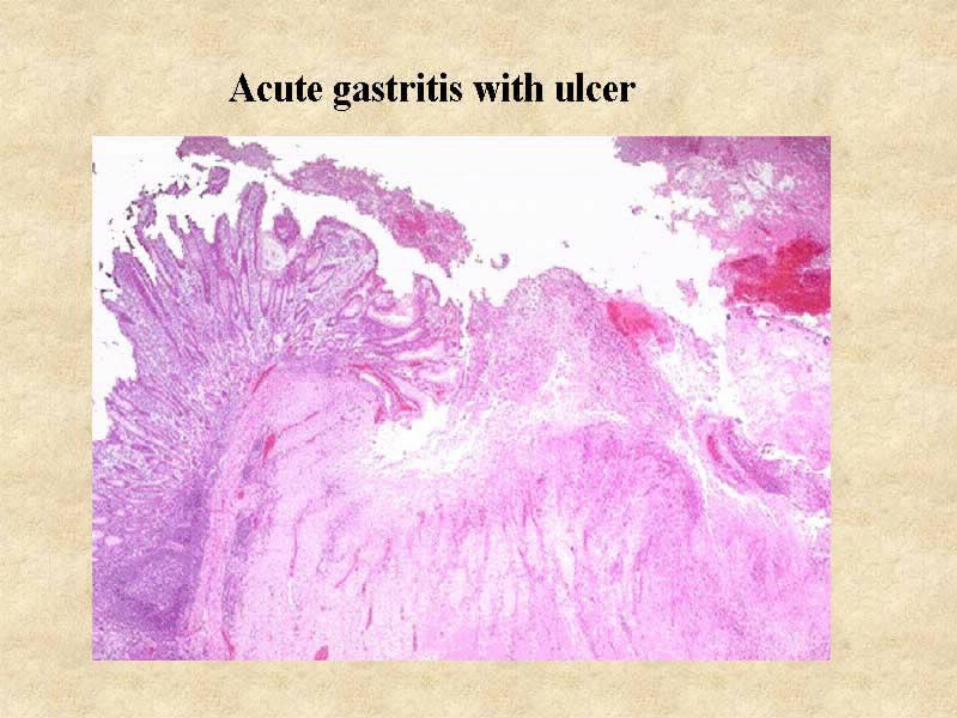
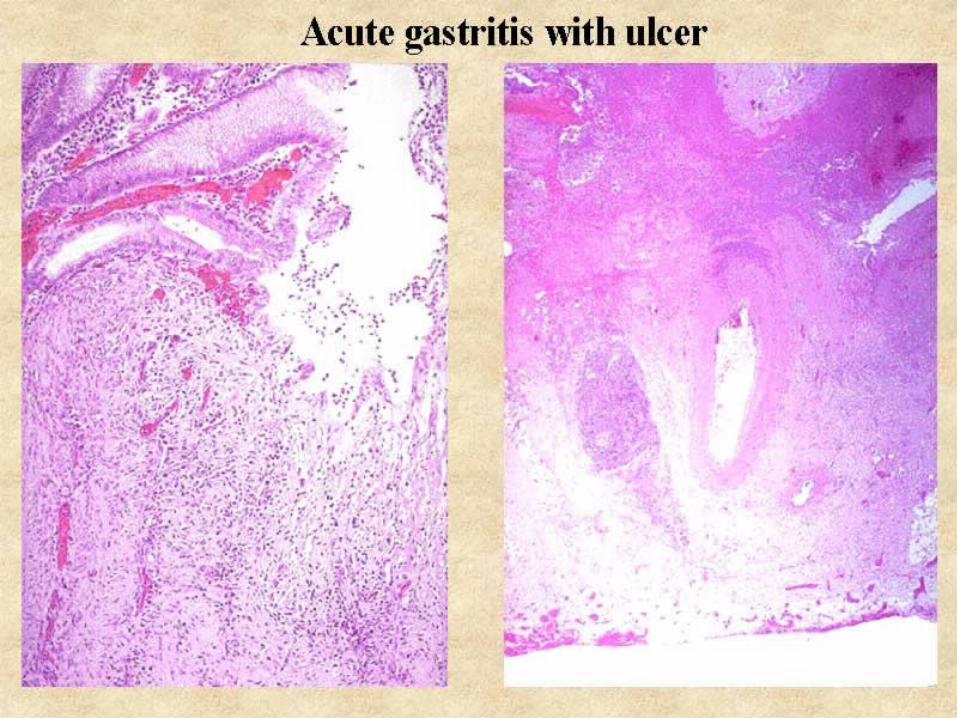
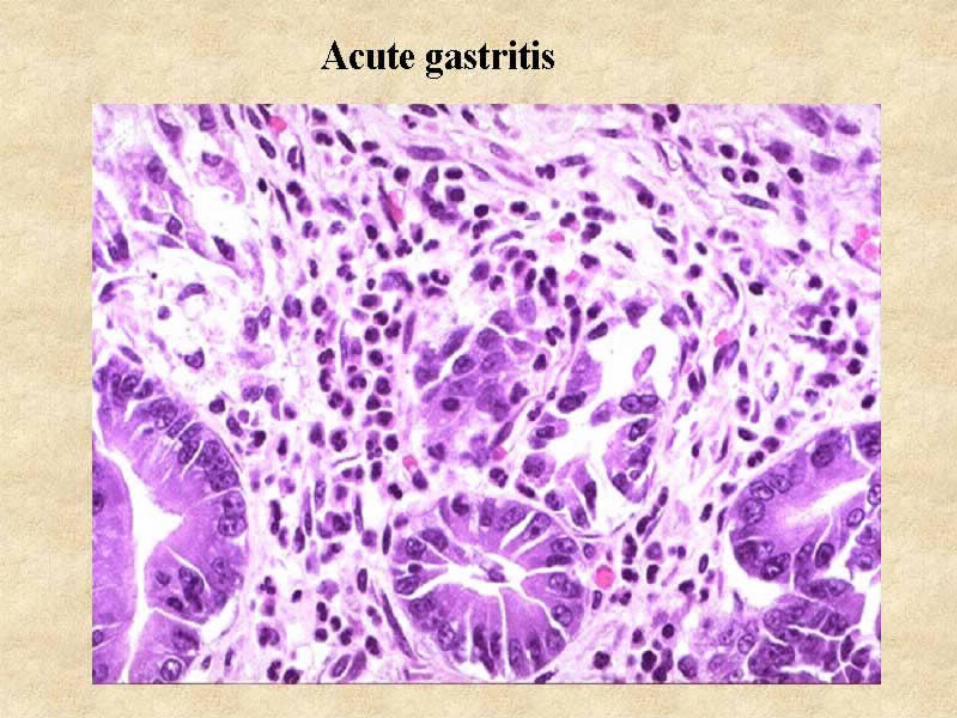
ACUTE GASTRITIS
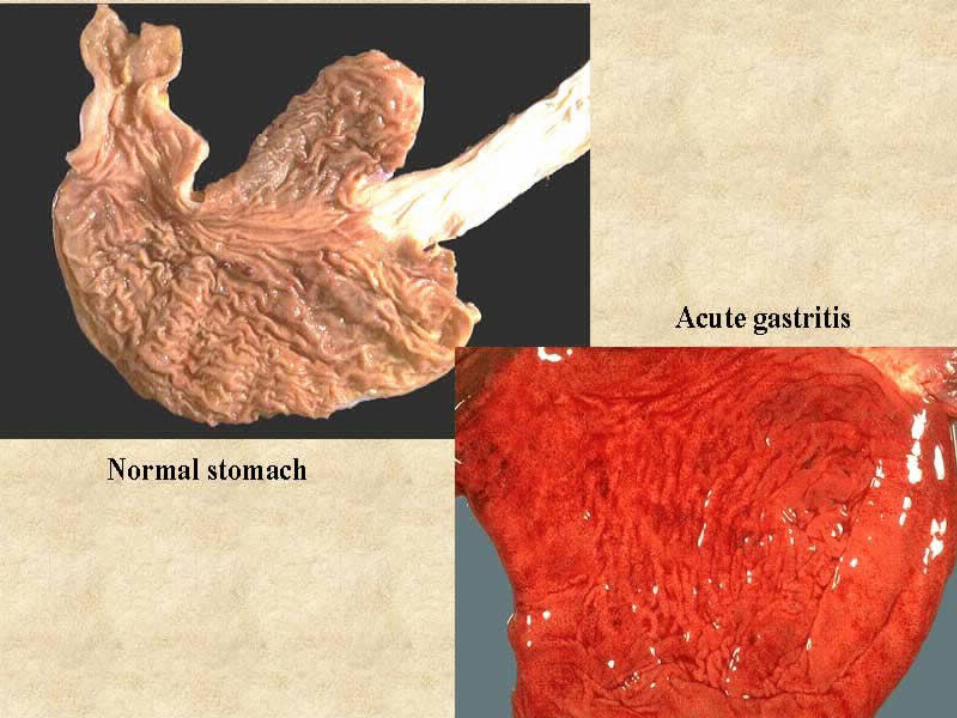
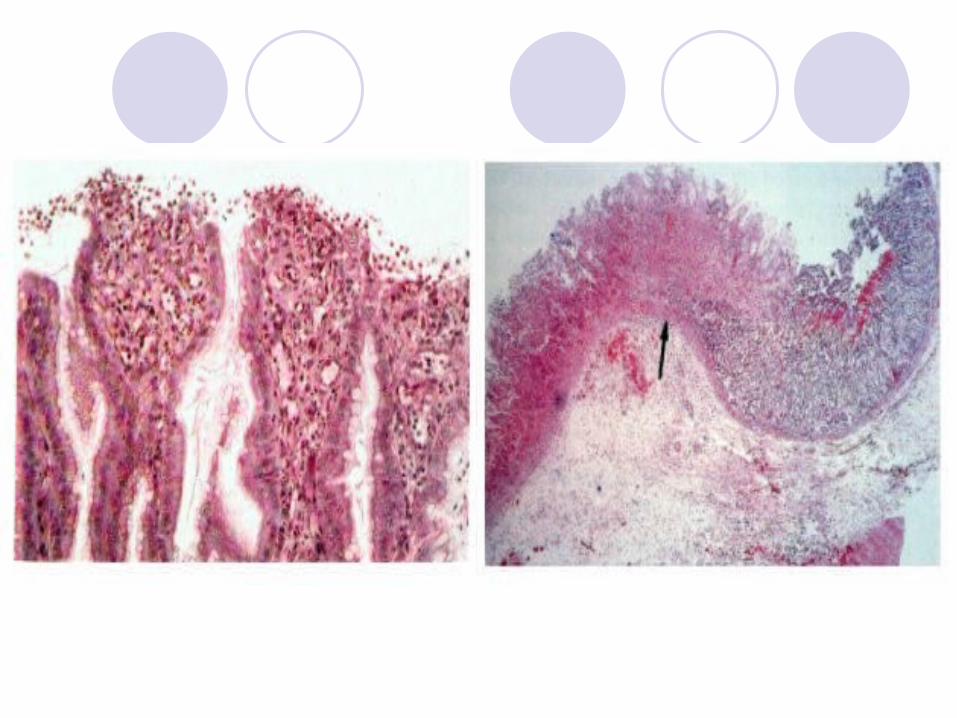
Morphology:
Mucosal edema & congestion, PMN infiltration (milder cases)
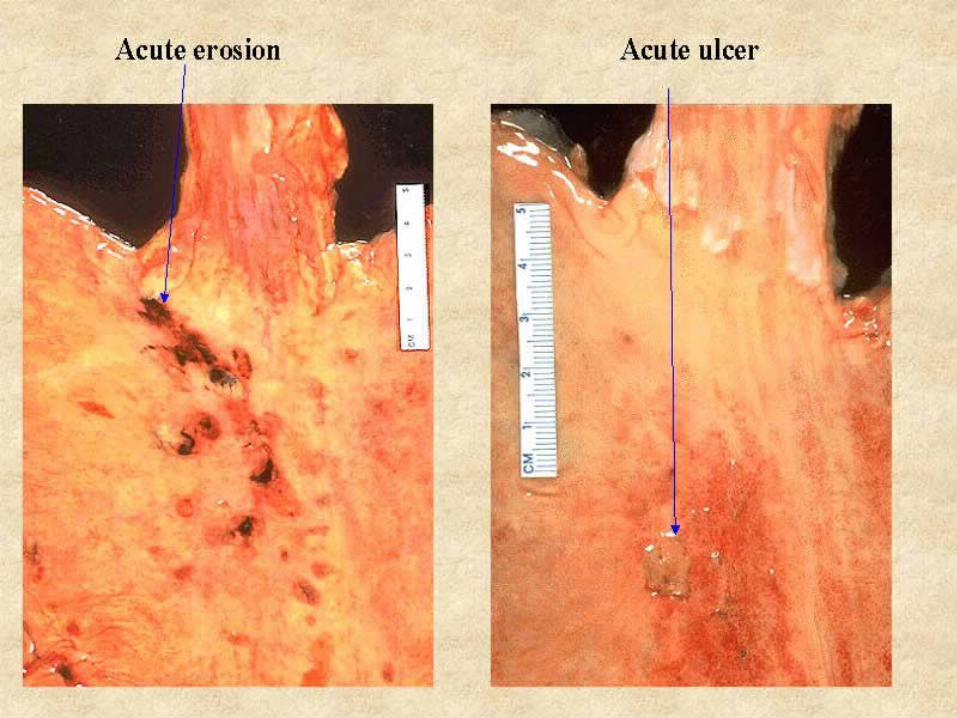
Erosions (not deeper than muscularis mucosa) & hges (acute erosive gastritis)
/ dysplasia
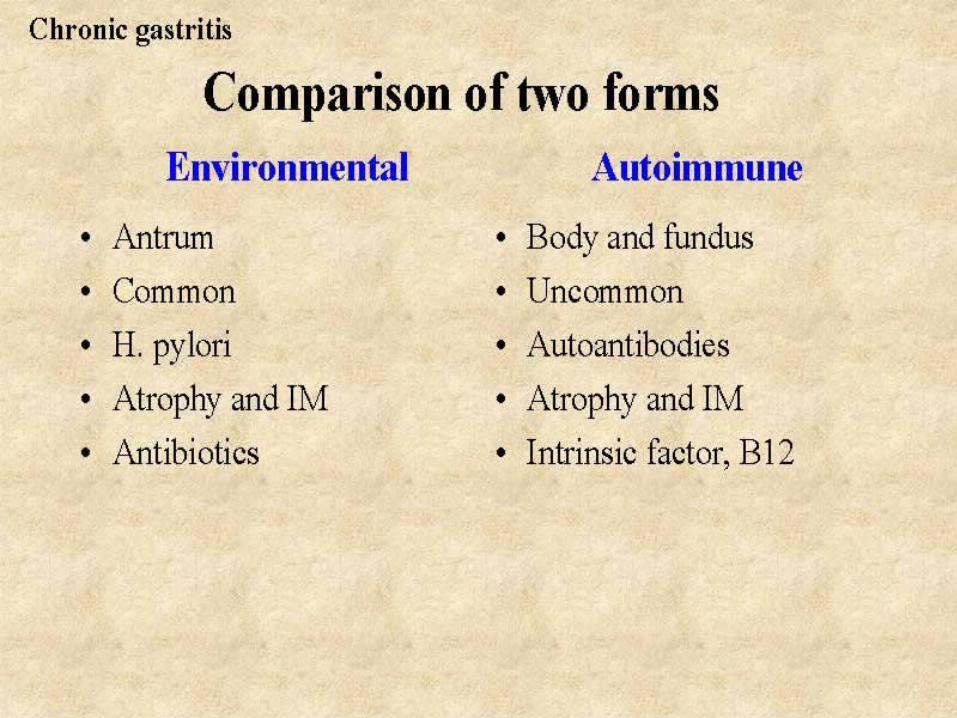
CHRONIC GASTRITIS
Pathogenesis:
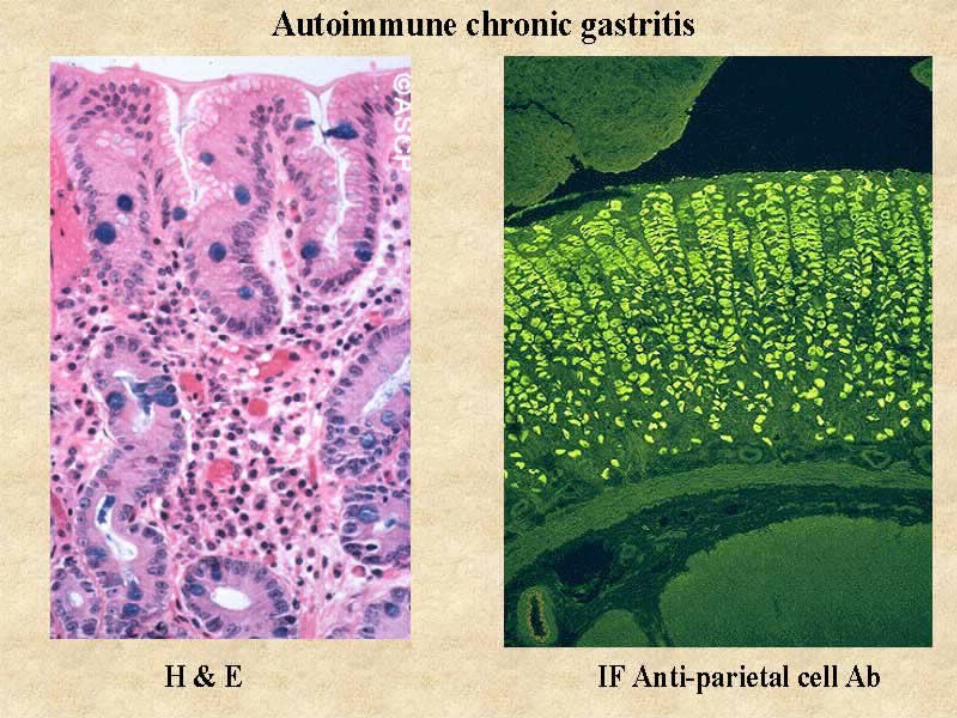
Autoimmune: Abs to parietal cells parietal cell destruction ( HCl & IF)
Environmental: Chronic infection by H. pylori Alcohol, tobacco, radiation, bile reflux, Crohn’s
disease, uremia, gastric atony
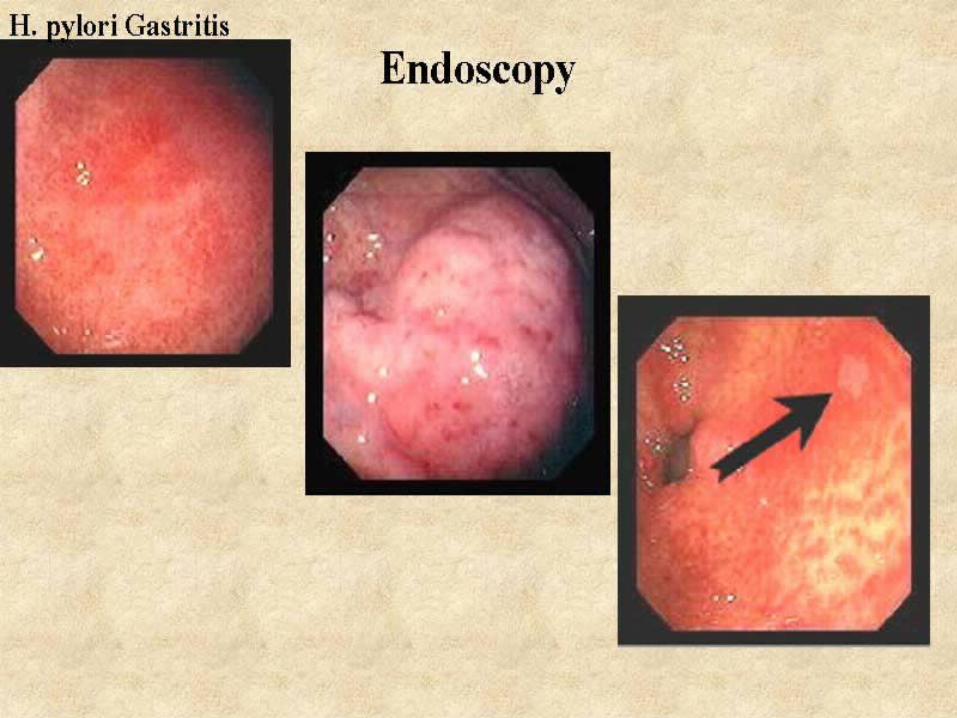
CHRONIC GASTRITIS
Gross:Red mucosa (thickened or flattened)
Autoimmune fundus & body H pylori antrum & bodyBile reflux antrum
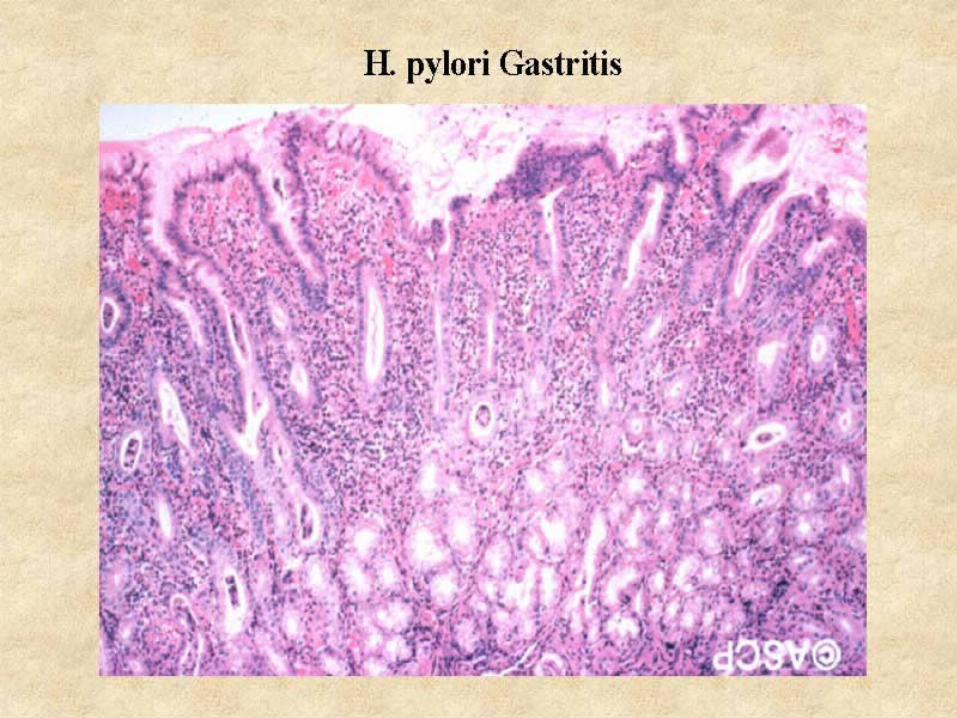
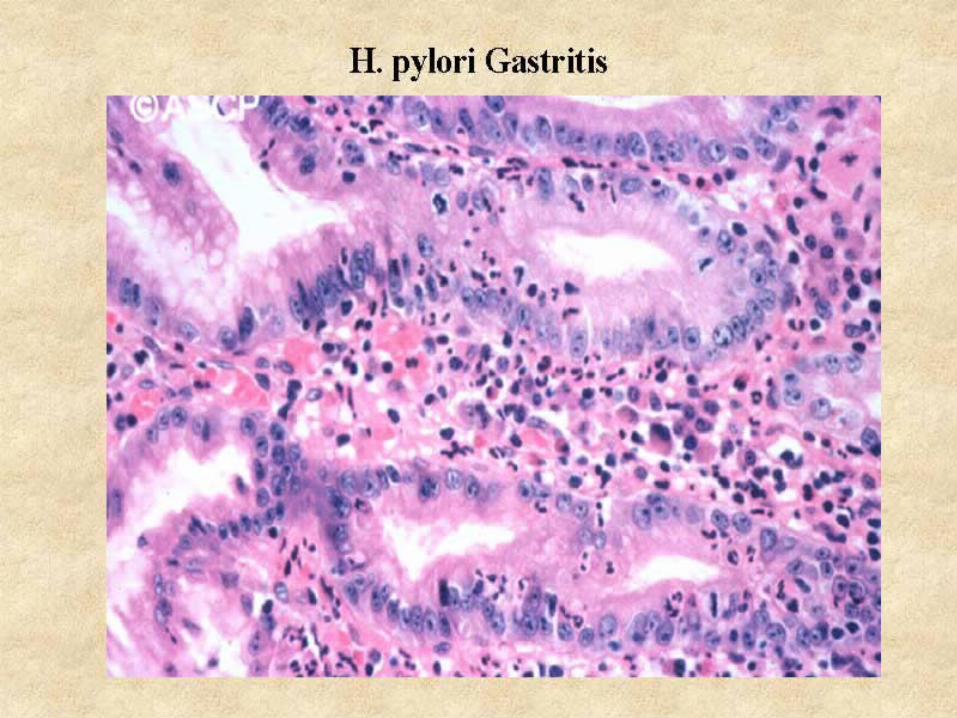
CHRONIC GASTRITIS
Histology:
Lympho & plasma cell infiltrates in LP (superficial or involving entire mucosal thickness)
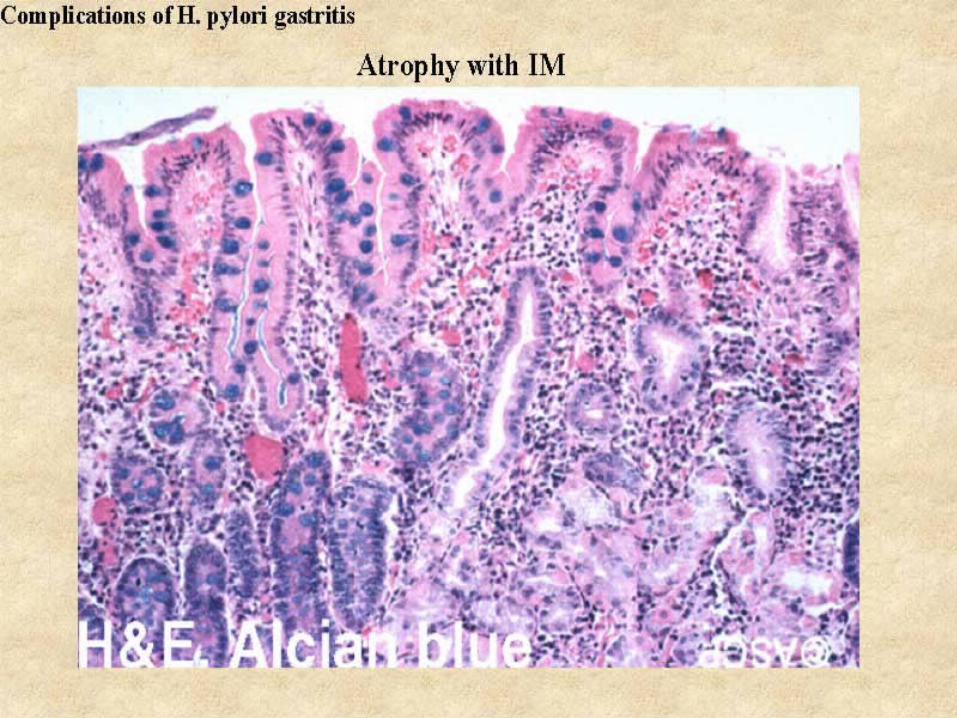
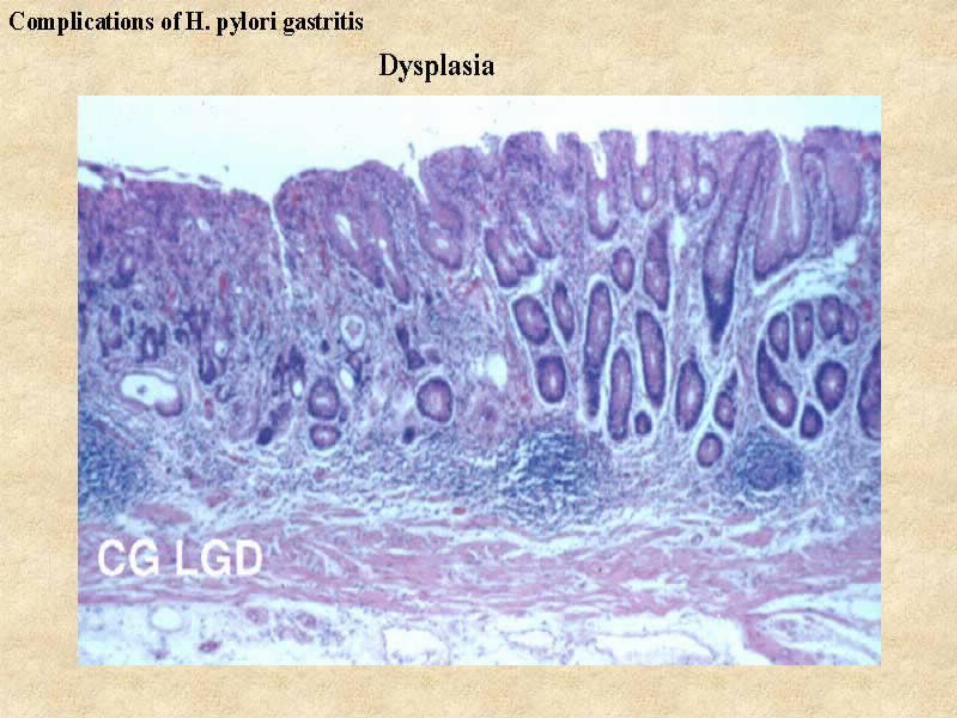
Others:
Regenerative atypia Intestinal metaplasia Atrophy Dysplasia
CHRONIC GASTRITIS
Clinical: Mild abdominal discomfort, nausea,
vomiting, hypochlorhydria
Autoimmune gastritis: Hypo- / a- chlorhydria, hypergastrinemia, ~
10% overt PA, long-term risk of Ca is 2-4%
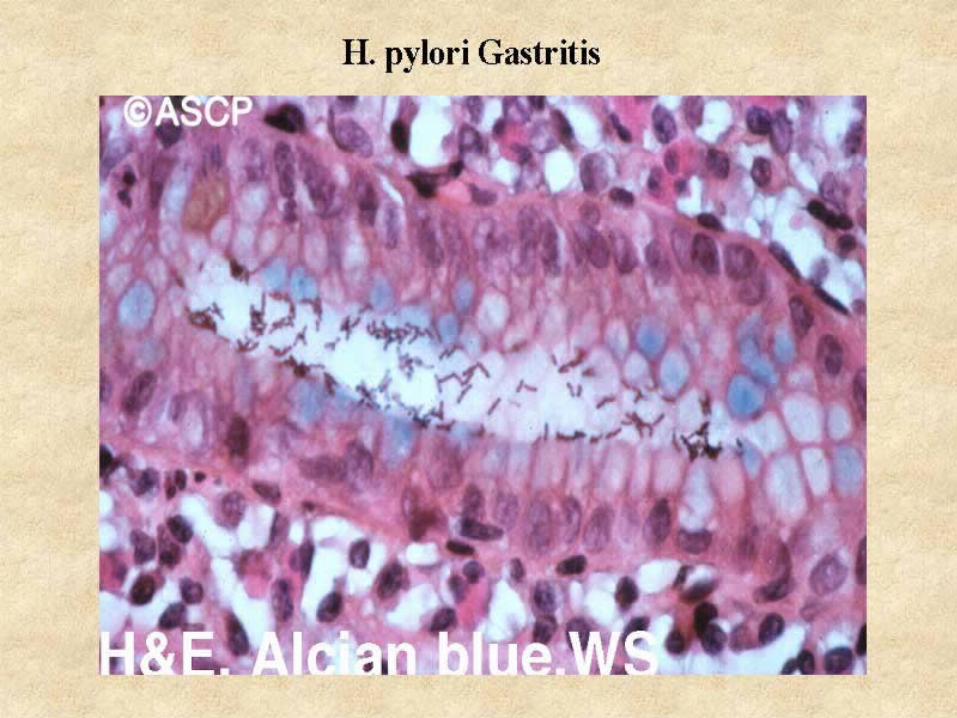
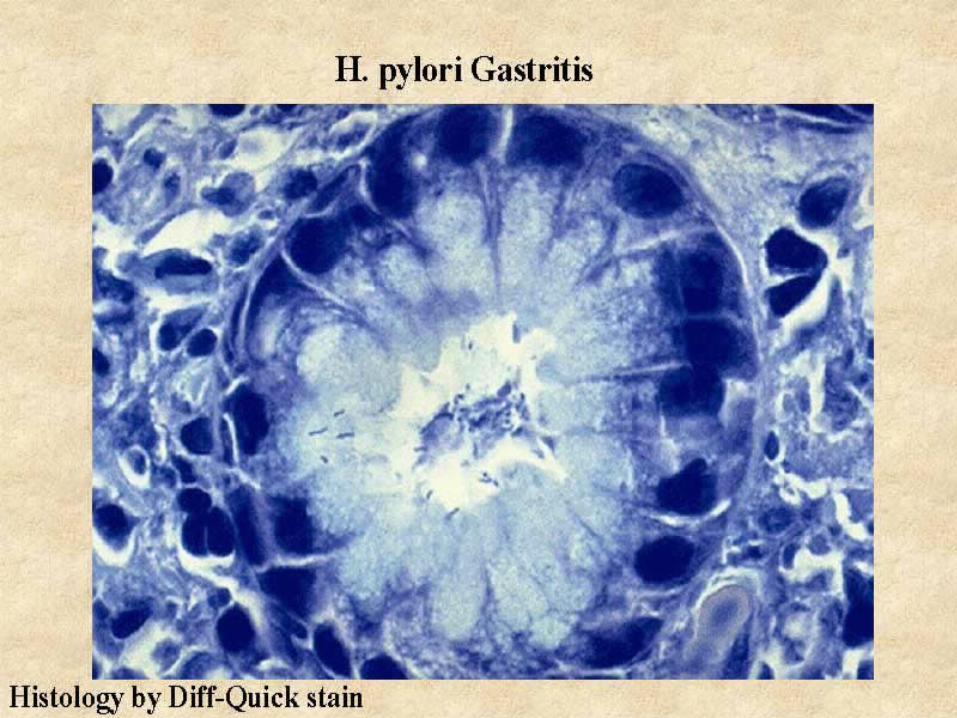
Helicobacter pylori
~ 50% of asymptomatic American adults > 50 yrs are infected
Dx: CLO test
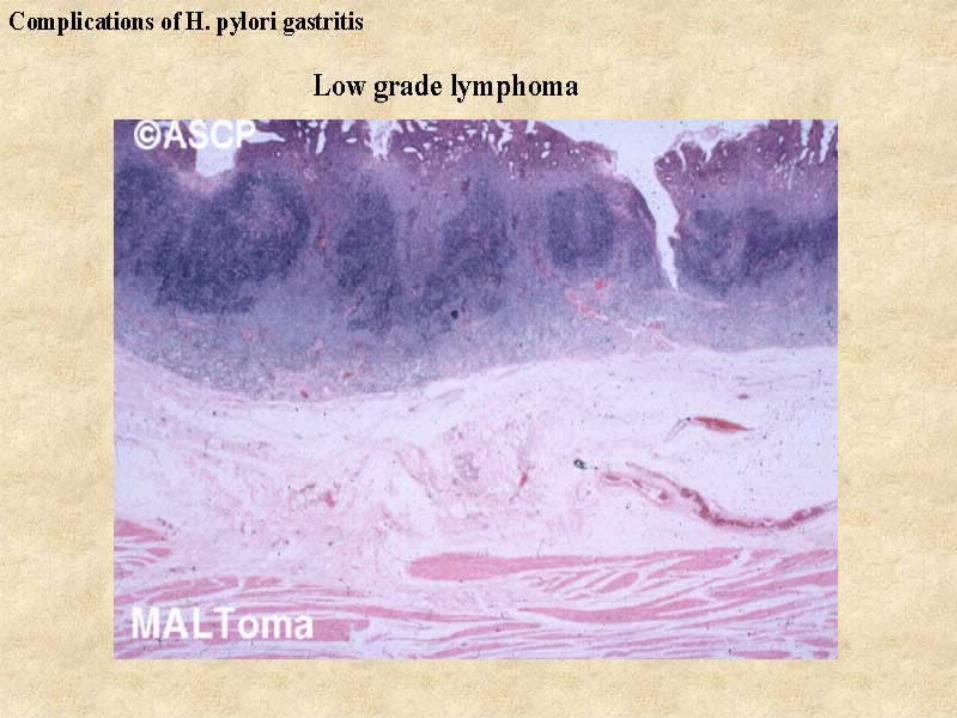
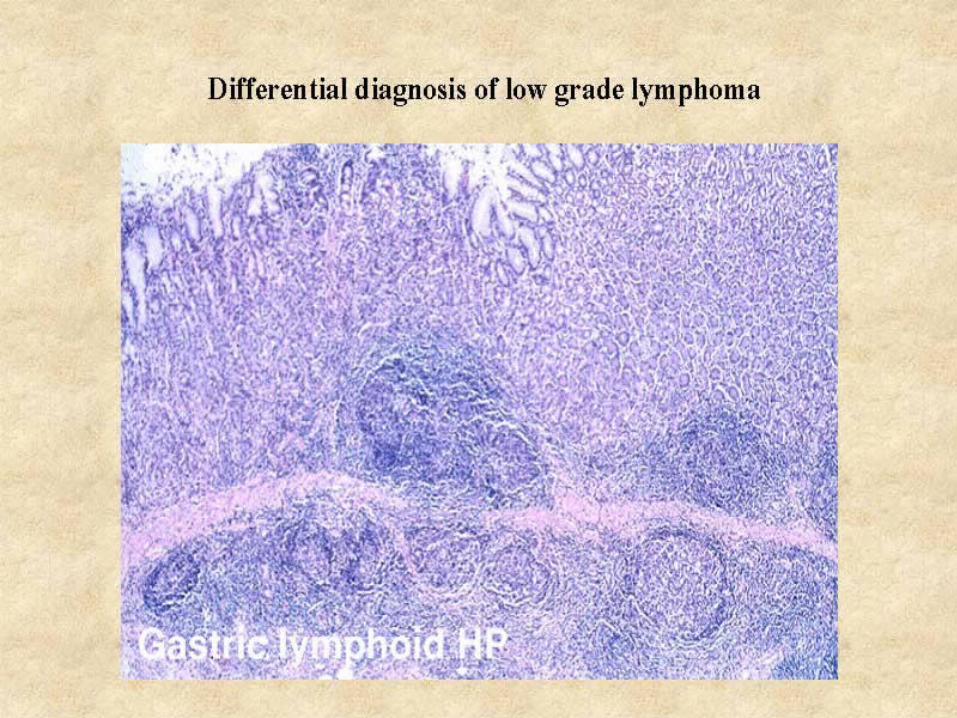
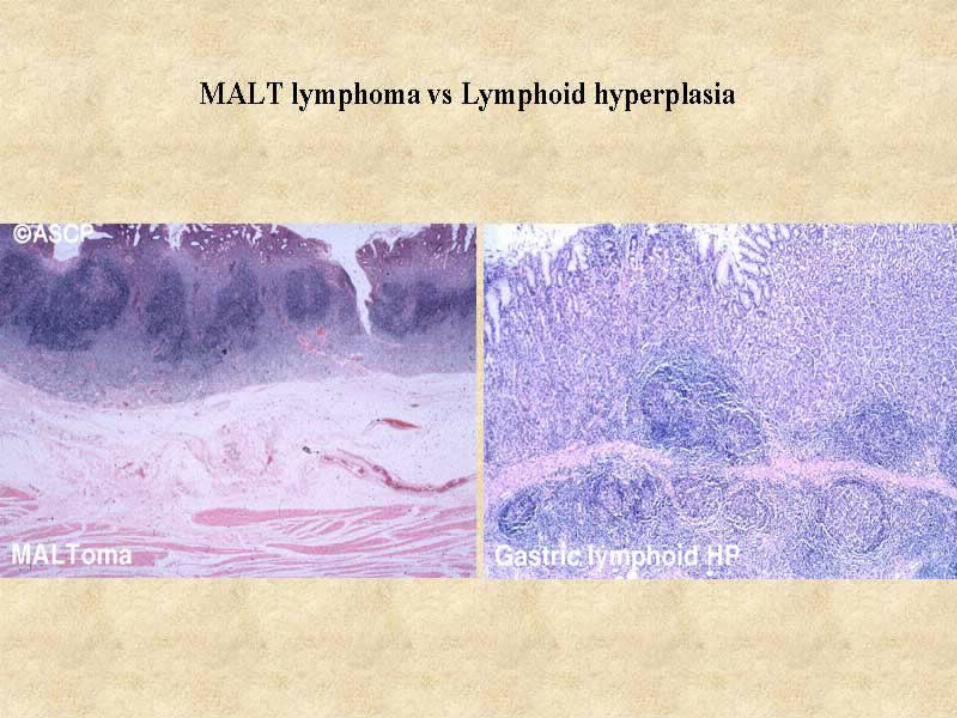
Diseases Association:
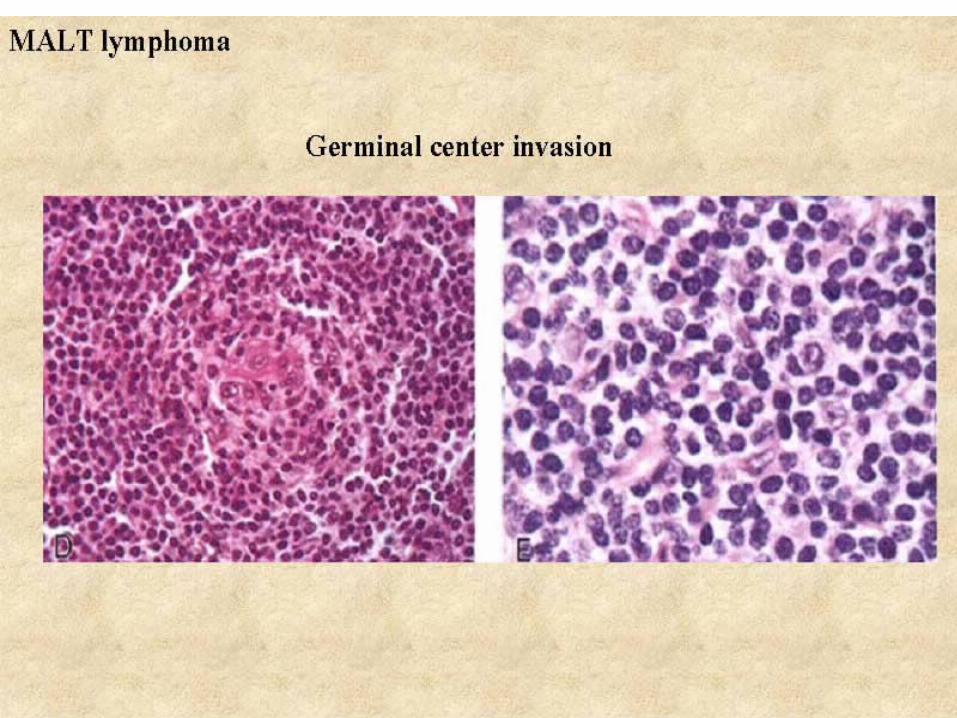
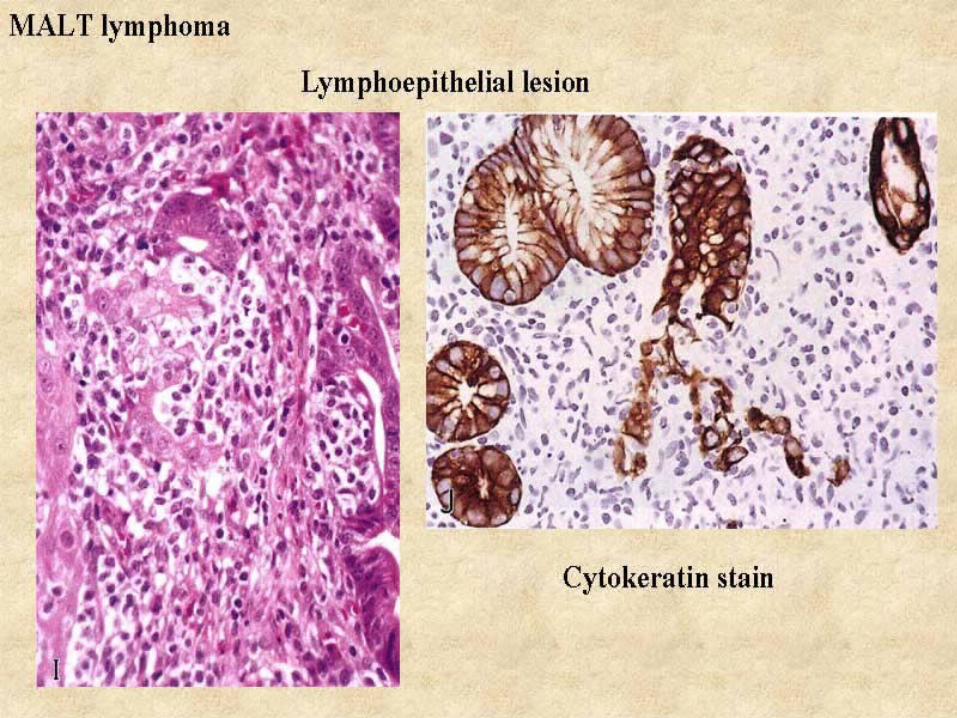
Chronic gastritis PUD Gastric ca/ lymphoma
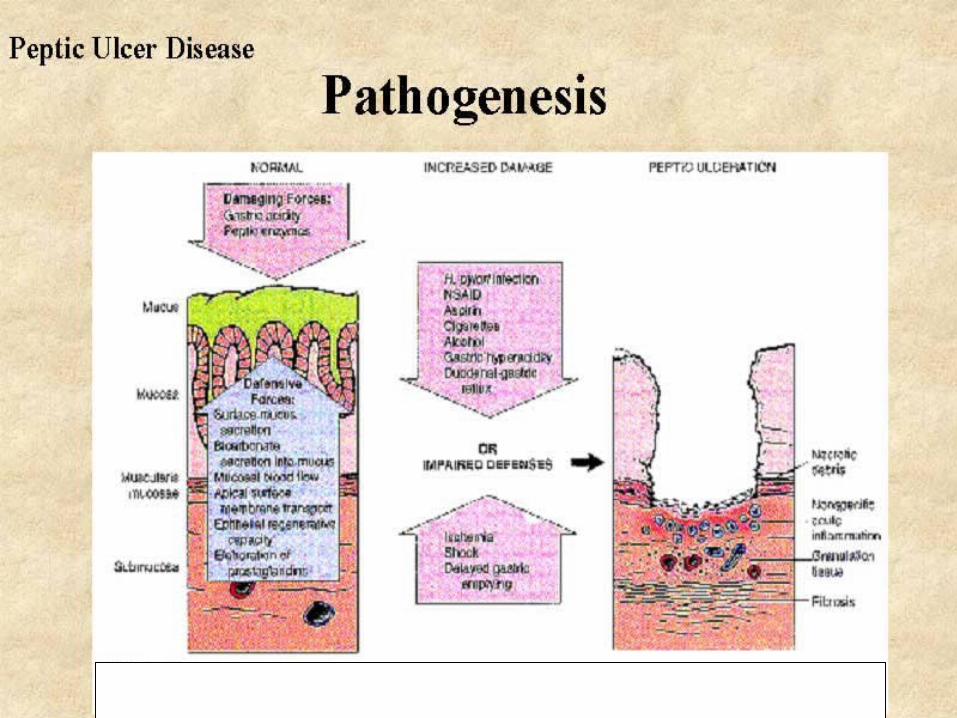
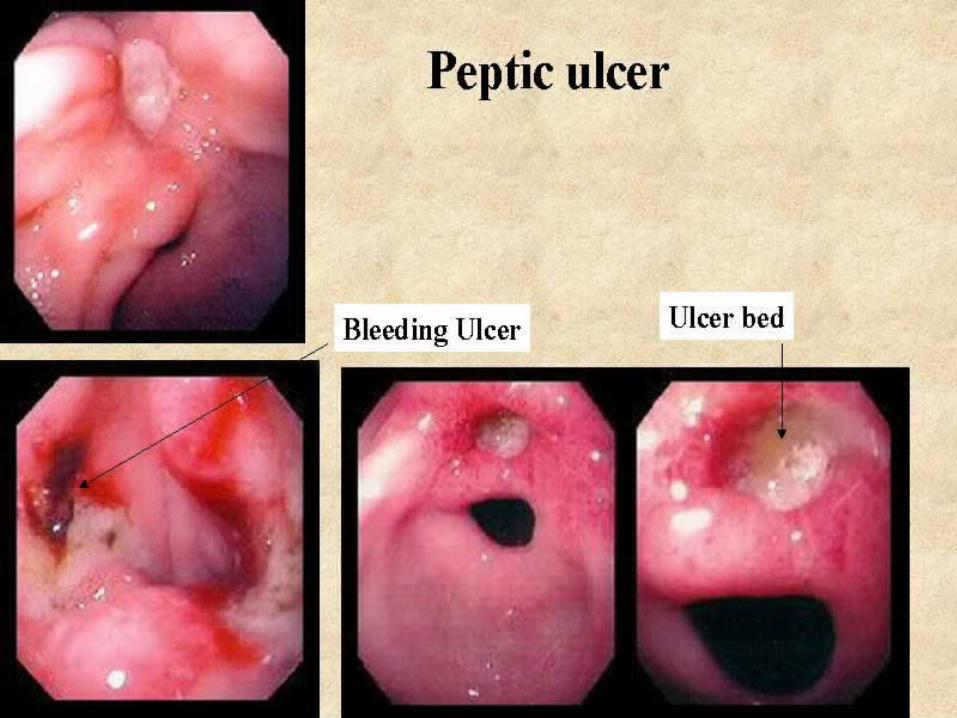
PEPTIC ULCERS
Usually solitary ~ 0.6 - 4 cm MC: duodenum & antrum Ratio of duodenal: gastric PU is ~ 4 : 1~ 4 M Americans have PU Life-time incidence in USA is 10% for men
& 4% for women
PEPTIC ULCERS
Clinical:
Epigastric pain 1-3 hrs PC & worse at night; nausea; vomiting; belching, weight loss
Complications:
Hemorrhage - 25% of ulcer deaths
Perforation - ~ 2/3 of ulcer deaths
Obstruction - causes severe crampy abdominal pain
Malignant transformation extremely rare
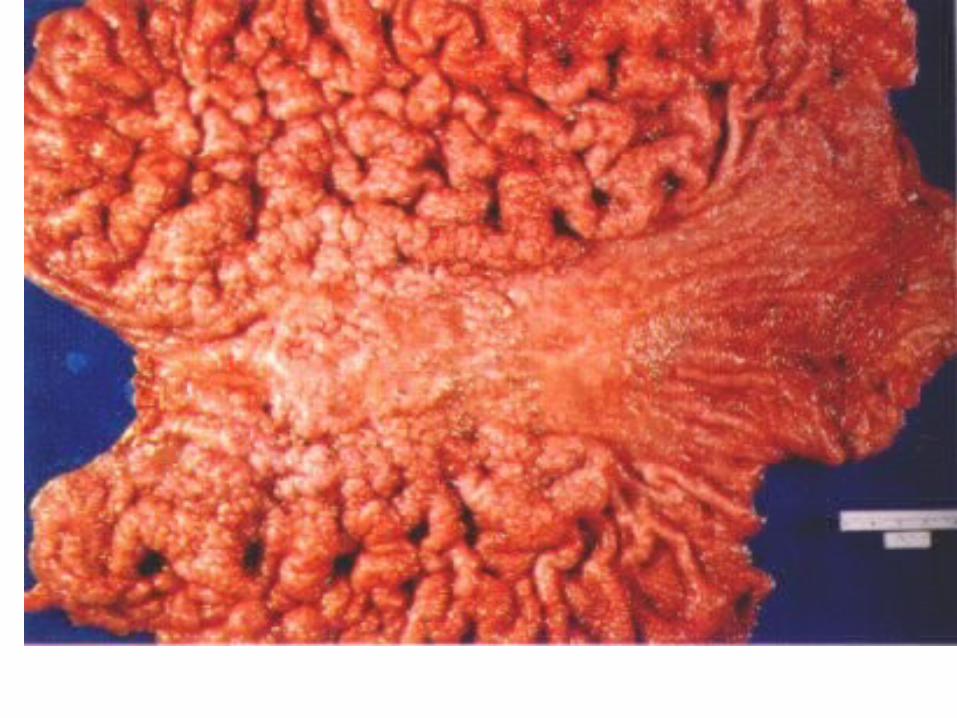
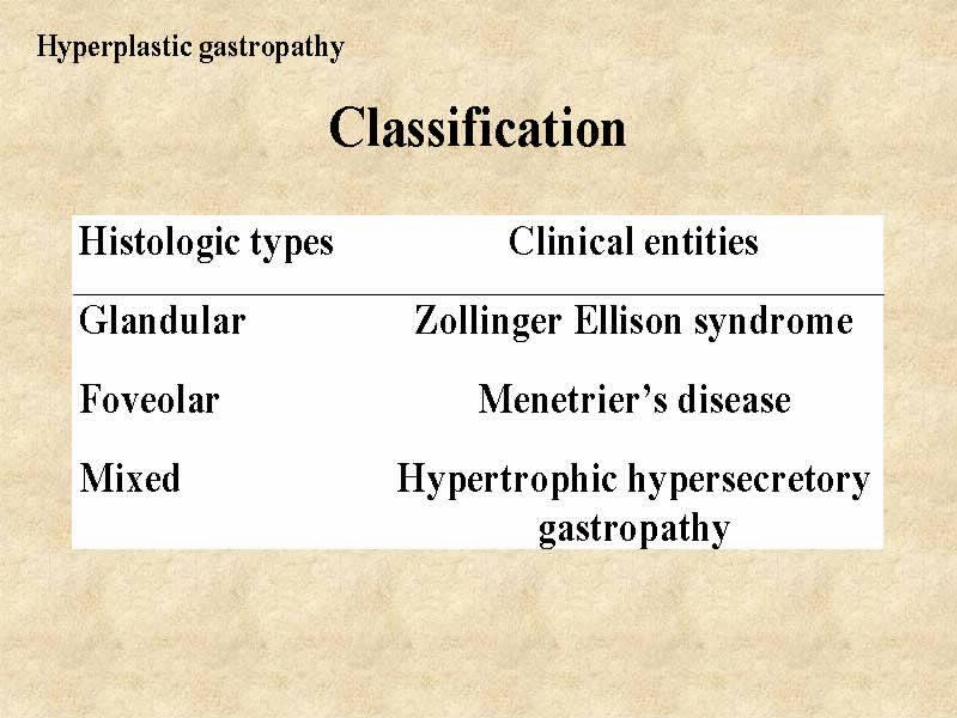
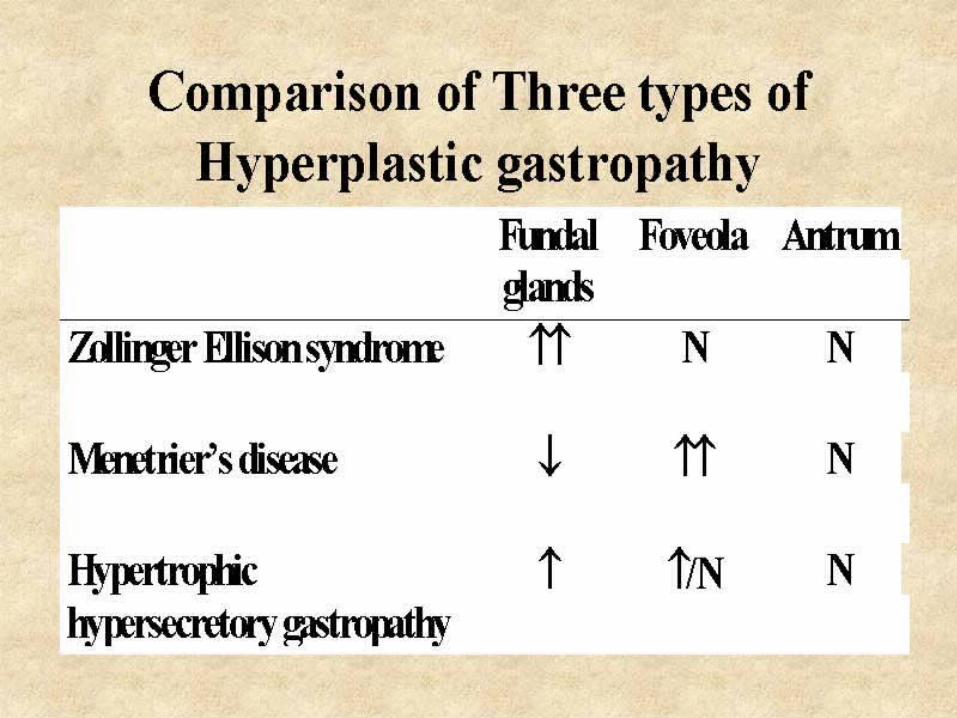
HYPERTROPHIC GASTROPATHTY
Zollinger-Ellison Syndrome:
Hypertrophic rugal folds Parietal cell hyperplasia Peptic ulcers Markedly elevated serum gastrin levels Caused by a gastrin secreting tumor
(gastrinoma) Pancreas is the usual primary site
HYPERTROPHIC GASTROPATHY
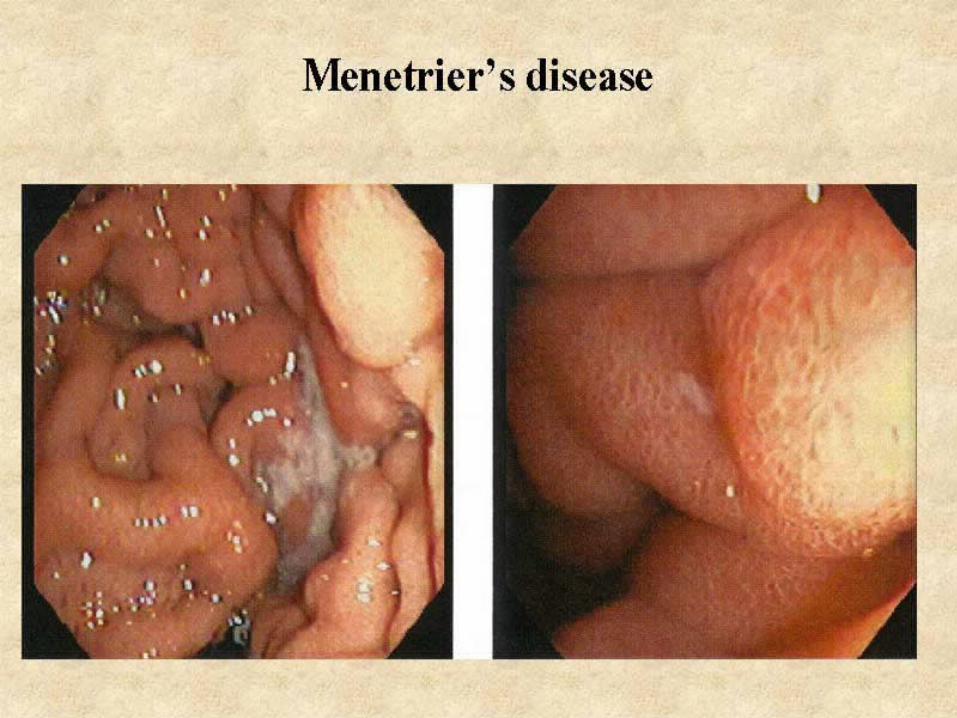
Menetrier’s disease:
Affects men in 4th to 6th decades Epigastric pain, anorexia, vomitting, wt. loss &
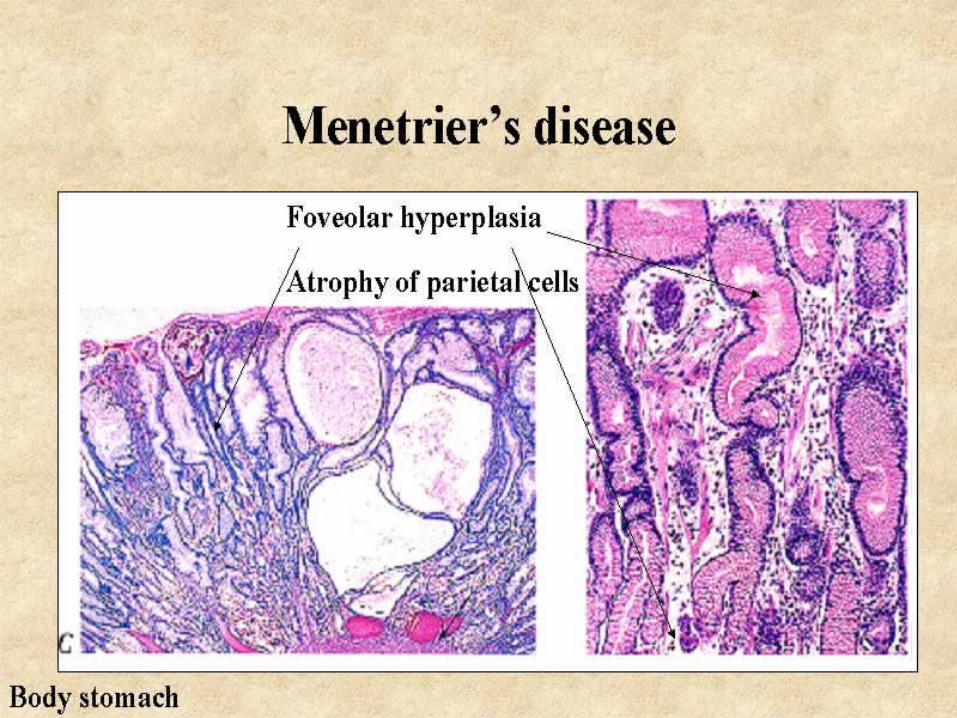
peripheral edema Diffuse rugal hypertrophy Marked foveolar hyperplasia, smooth muscle
proliferation in LP, glandular atrophy Hypochlorhydria Protein-losing enteropathy
GASTRIC POLYPS
Mucosal masses projecting above level of surrounding mucosa
> 90% non-neoplastic polyps - no malignant potential
Hyperplastic polyps: MC type of gastric polyp Small sessile polyps May be multiple No dysplasia no malignant potential
GASTRIC POLYPS (CONT.)
Adenomatous polyps (Adenomas): May be sessile or pedunculated Usually solitary May reach 3-4 cm in dia Contain proliferating dysplastic epithelium Are true neoplasms Up to 40% contain a focus of ca at time of biopsy Patients with autoimmune gastritis or colonic polyposis Syndromes have an increased incidence Gastric polyps need to be biopsied
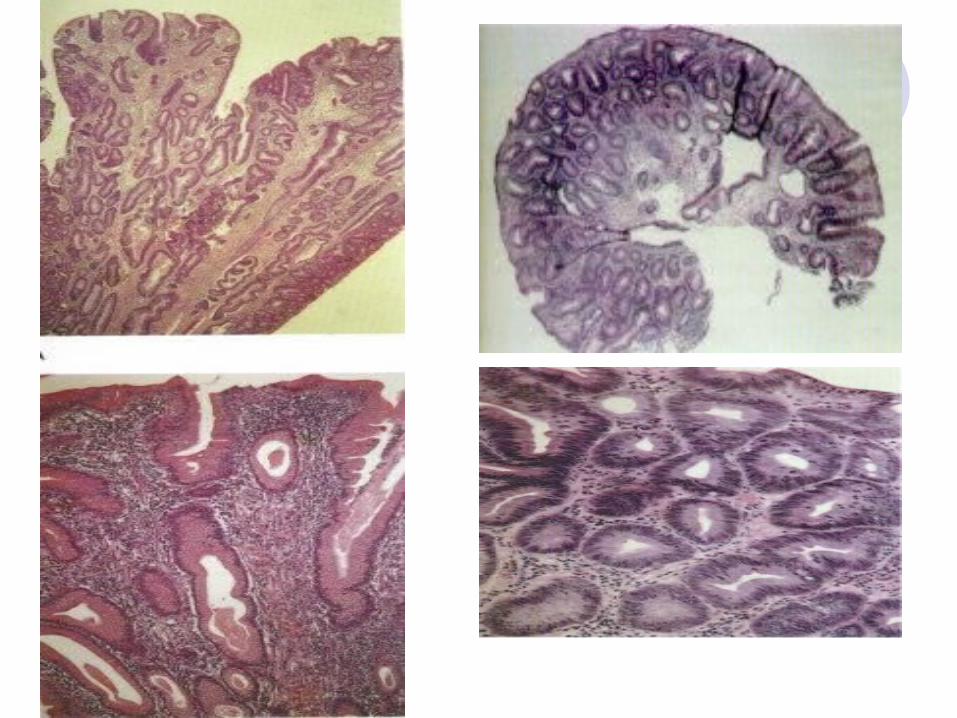
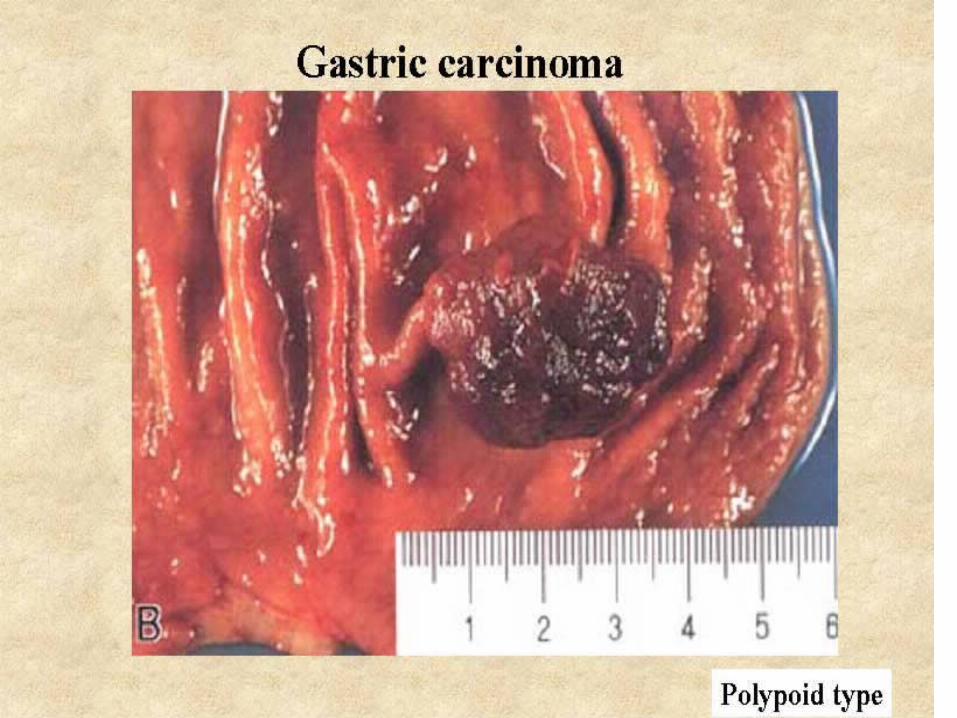
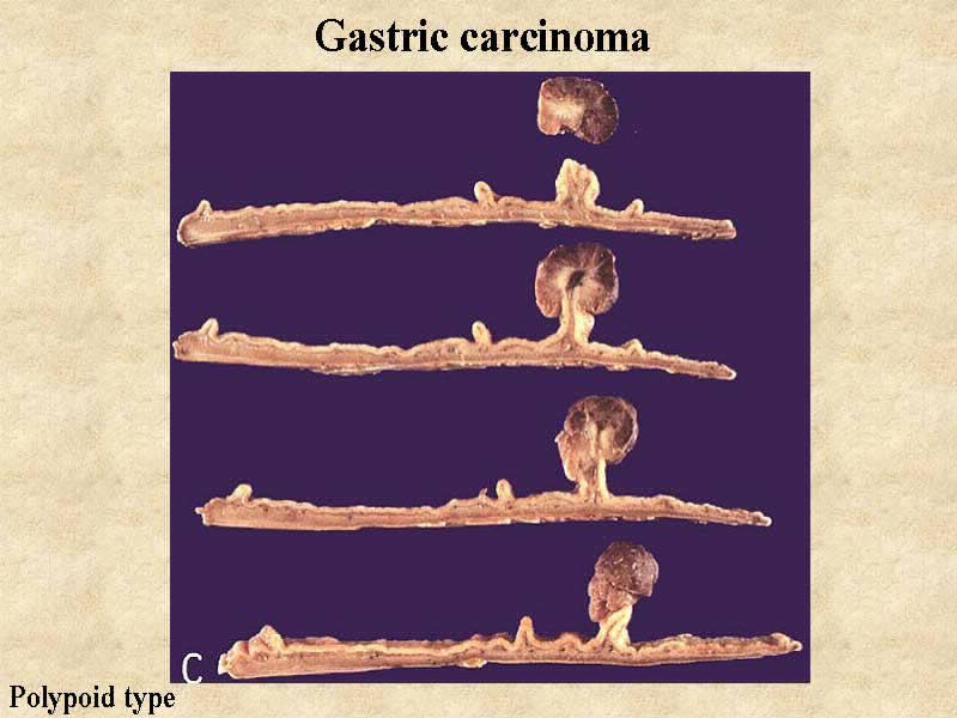
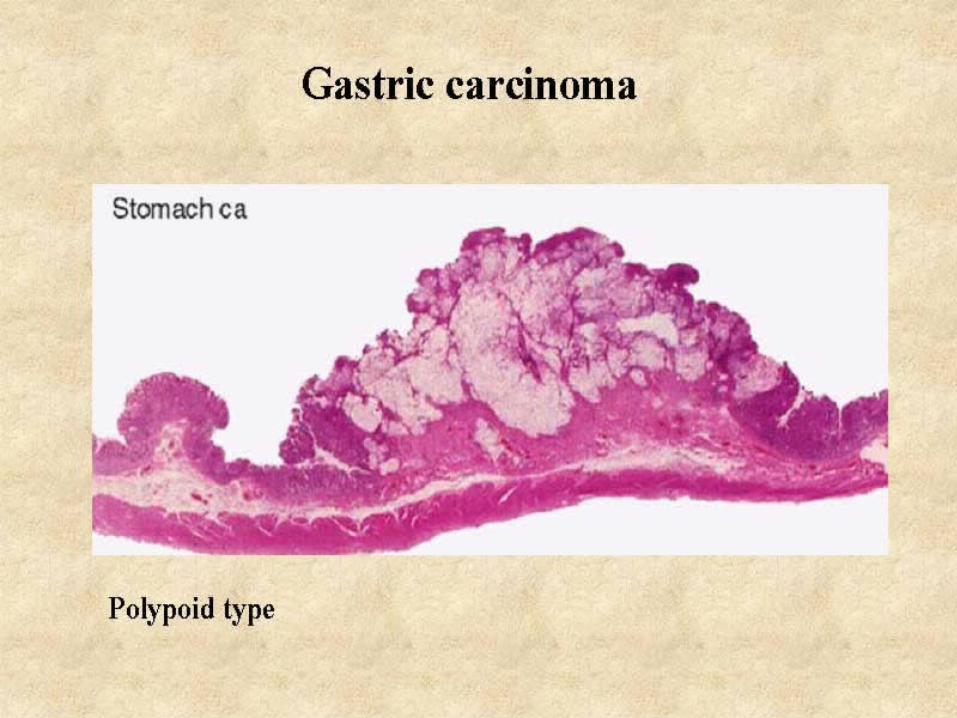
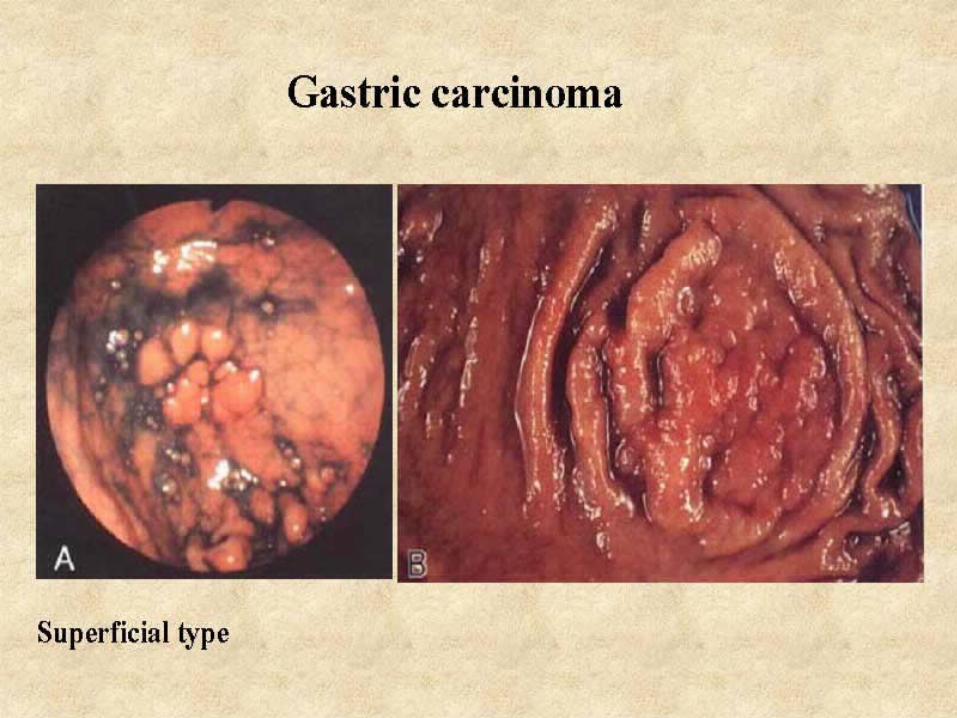
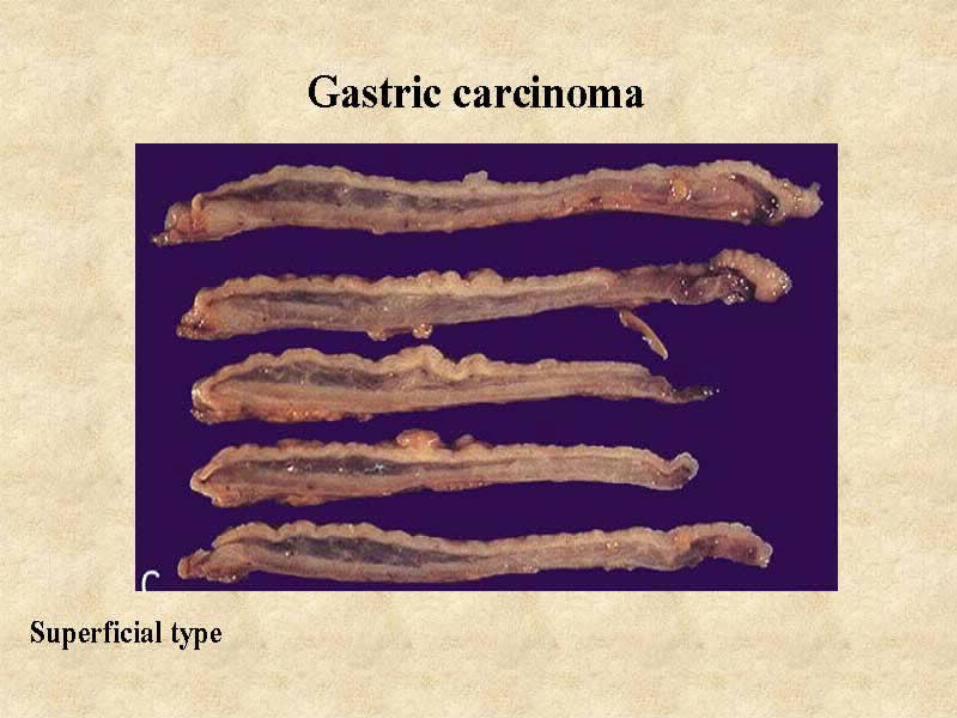
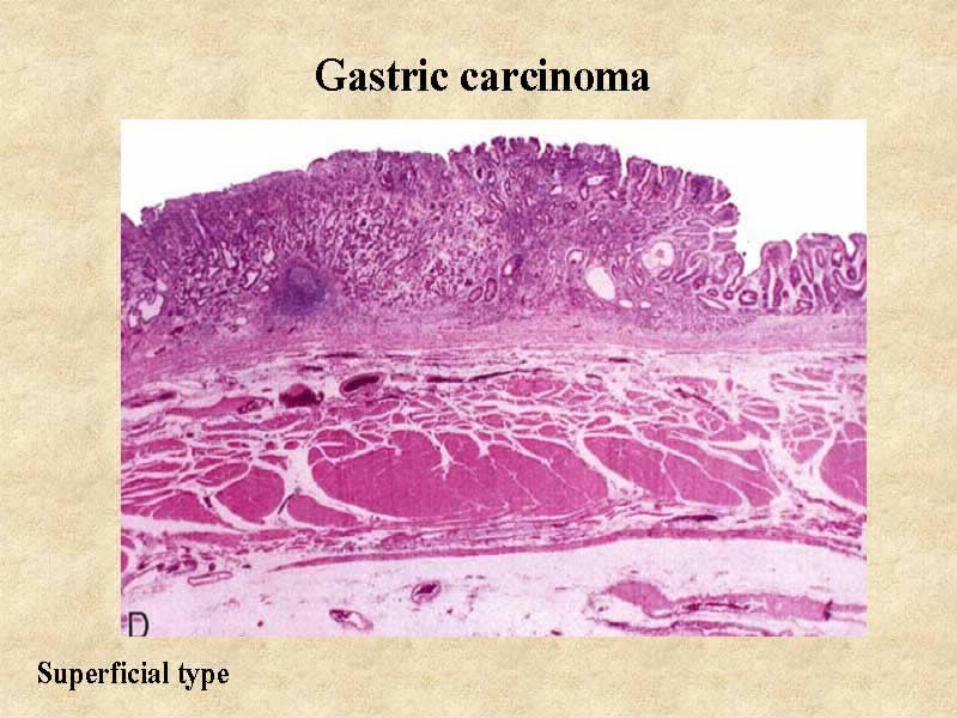
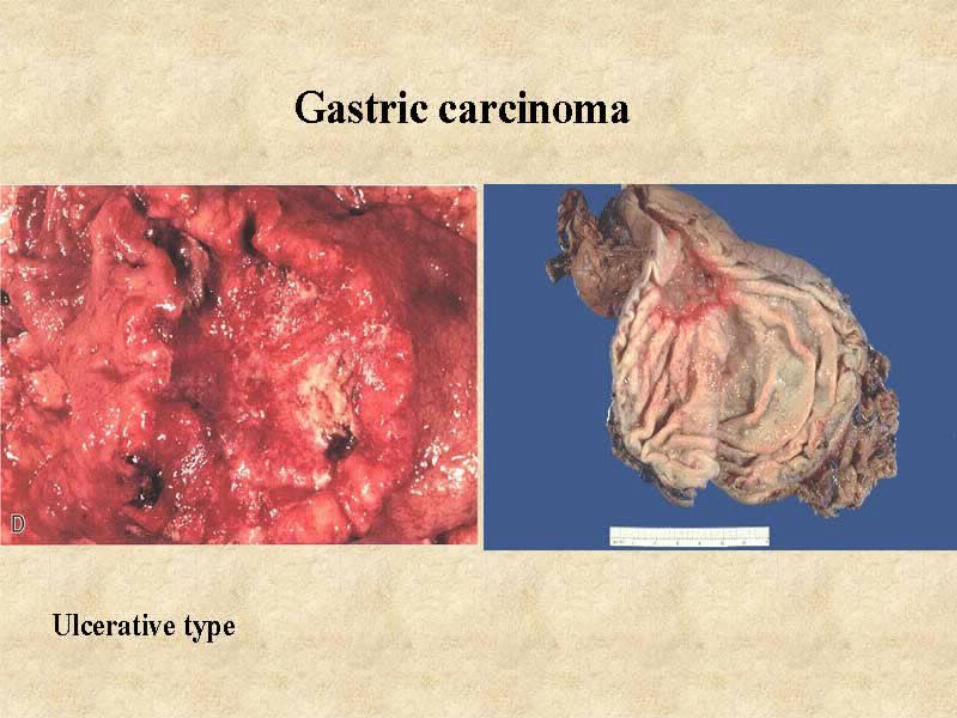
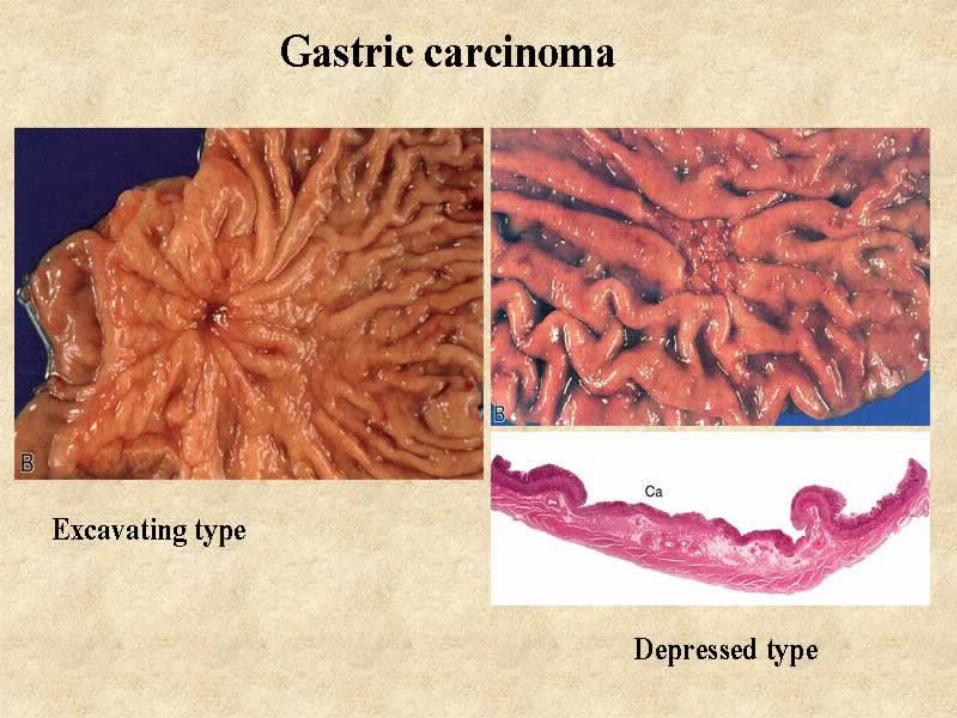
GASTRIC CARCINOMA
Worldwide distribution variableUS 2.5% of all Ca deaths5-6 fold decline in incidence over last 70
yrs (for unknown reasons)
GASTRIC CARCINOMA Classification:
According to Depth of invasion: Early Gastric Ca:
Confined to mucosa & submucosa Very good prognosis - ~ 90% 5-year survival, even w/
limited LN spread Advanced Gastric Ca:
Extended beyond submucosa Spread by local invasion, lymphatics, blood (to liver,
lungs & bone) Virchow node Bilateral ovarian metastases - Krukenberg Poor prognosis (<15% 5-year survival)
GASTRIC CARCINOMA Classification:
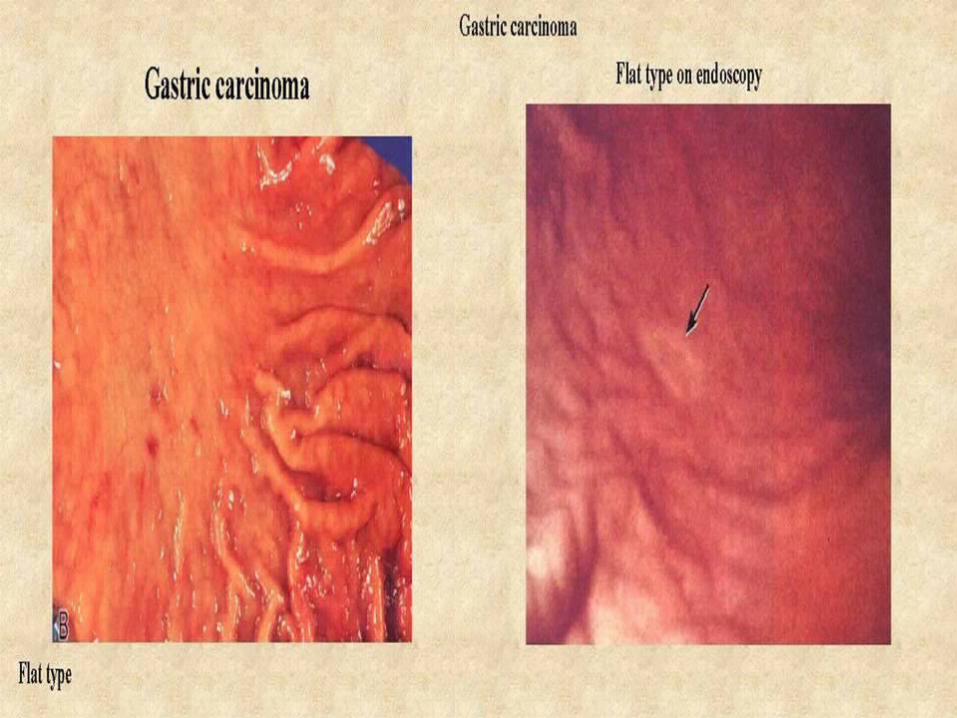
According to Gross Pattern: Exophytic Flat/depressed Excavated (ulcerative)
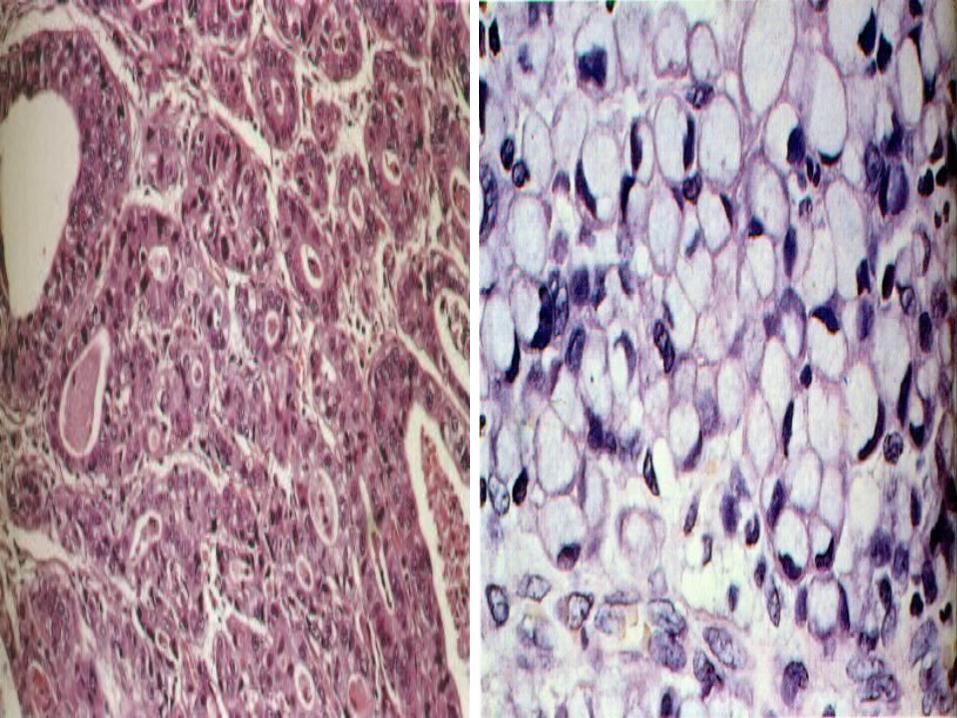
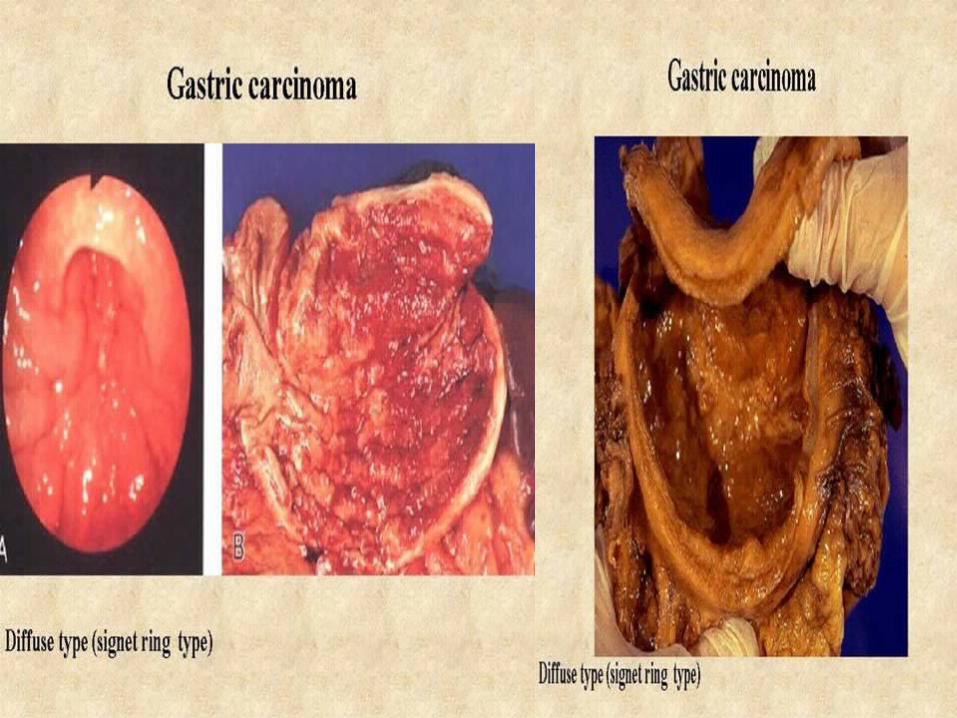
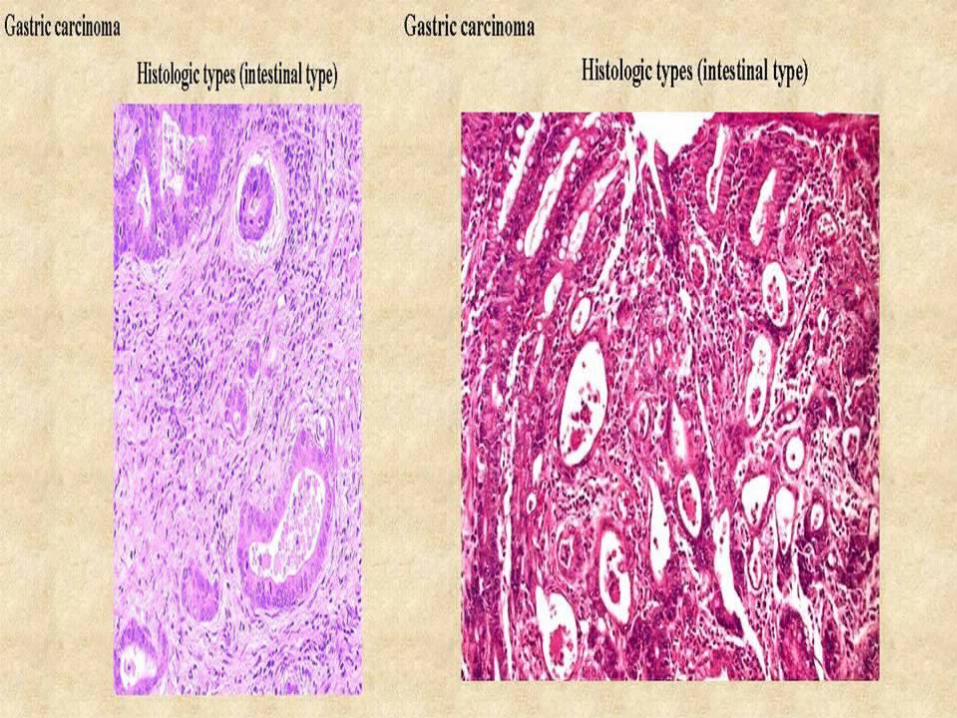
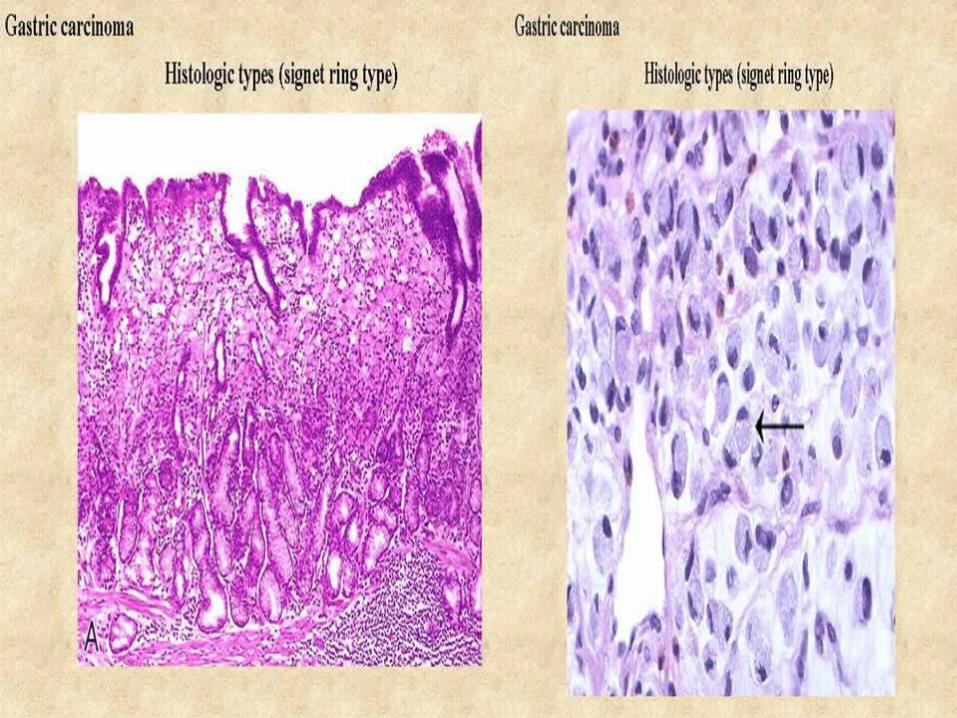
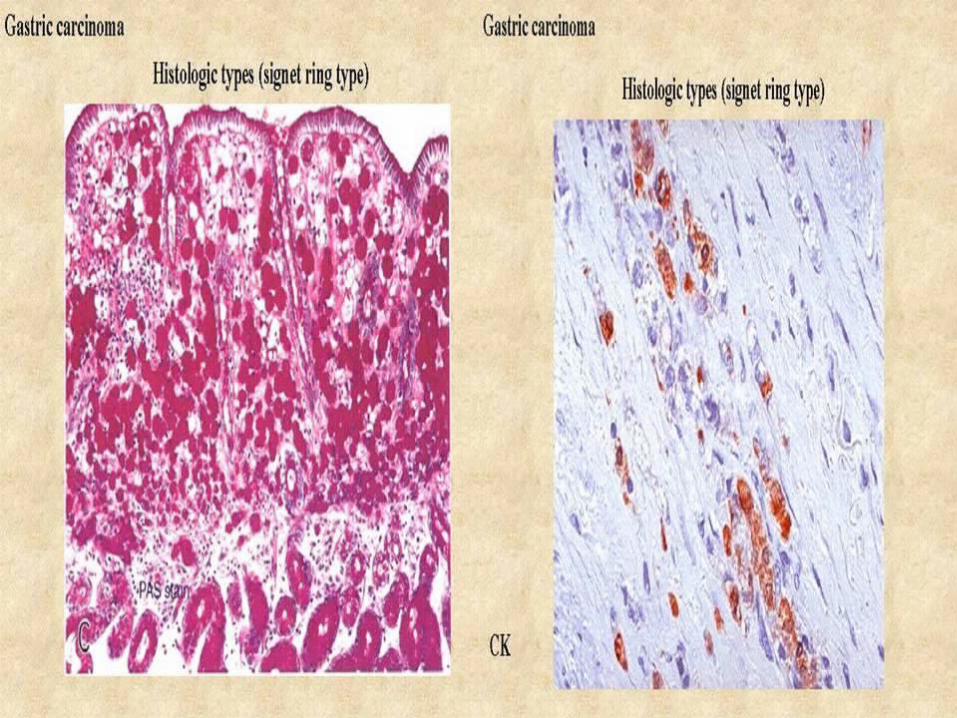
According to Histologic Pattern:Intestinal type, glandular, expansile Diffuse type, “signet ring cell”, infiltrating
(linitis plastica)
GASTRIC CARCINOMA Classification: Pathologic stage is the most important
prognostic indicator
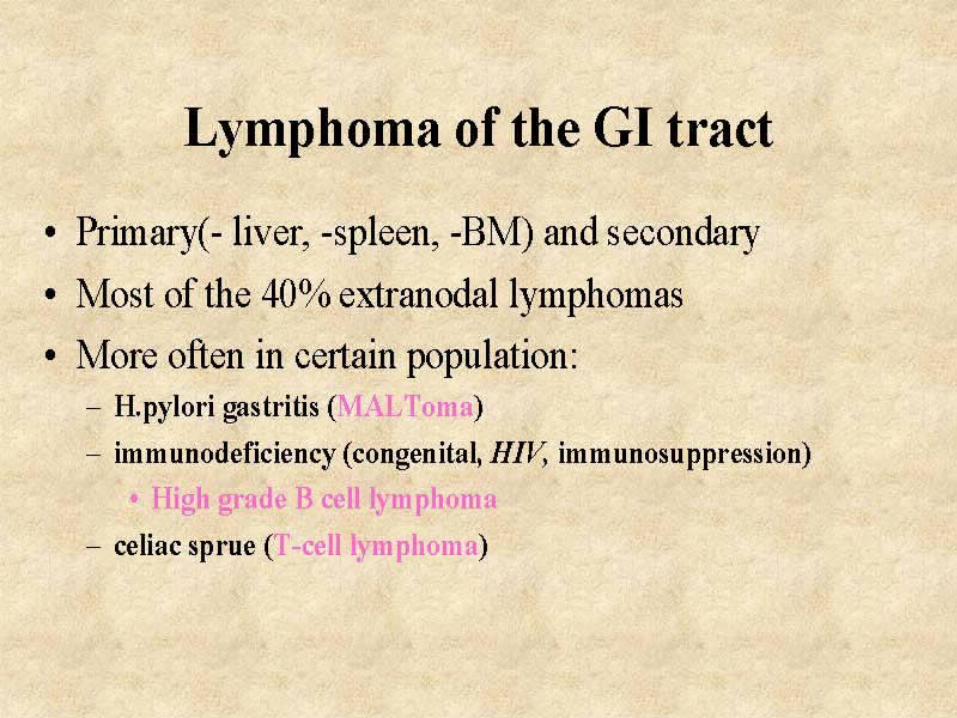
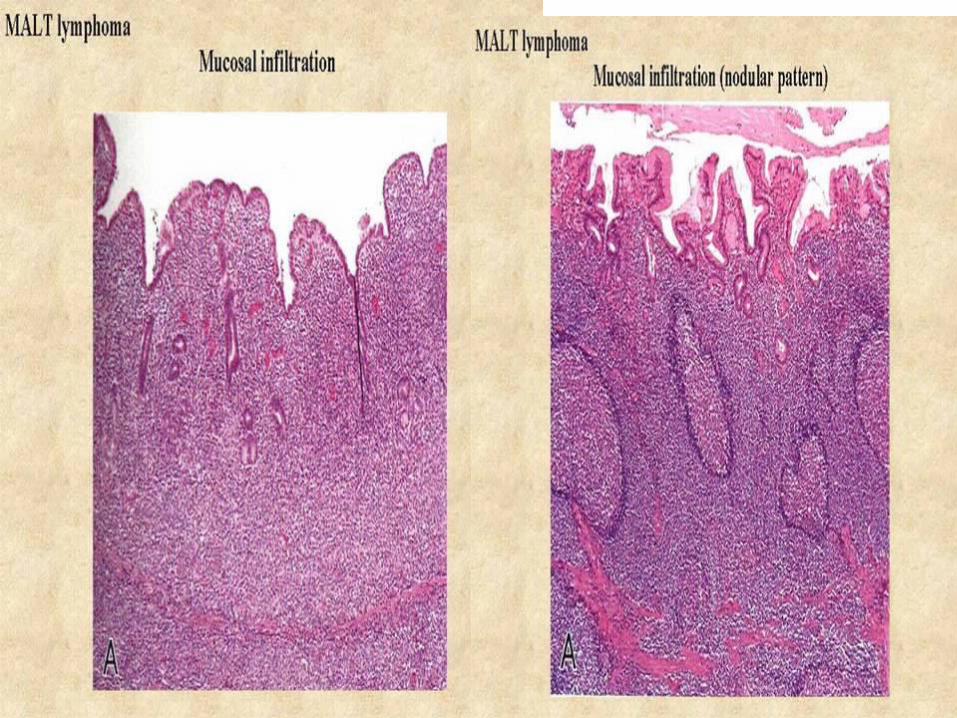
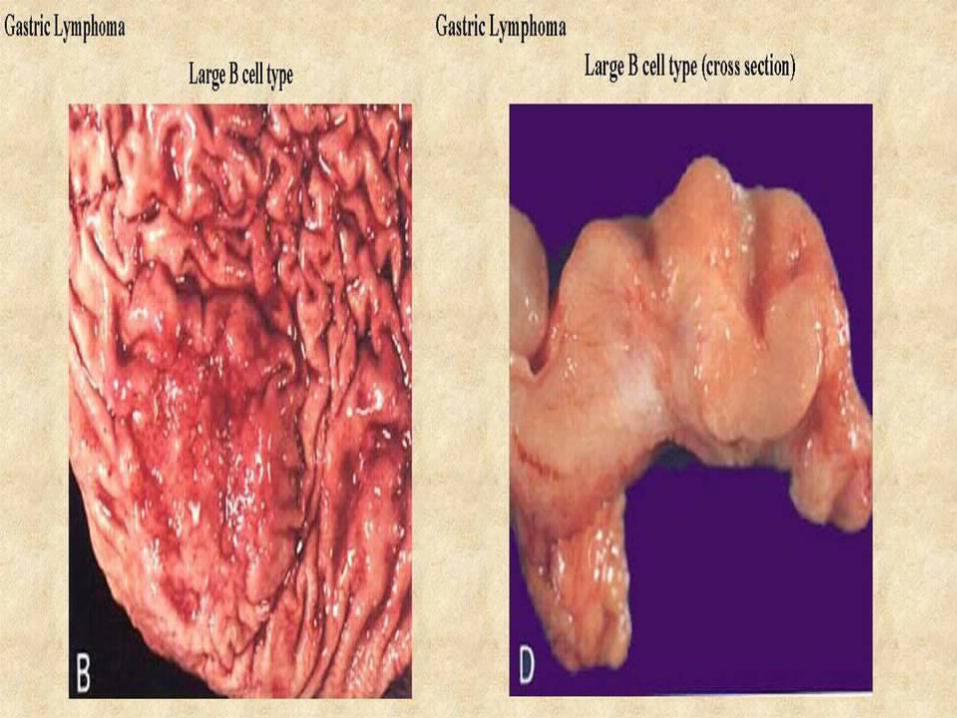
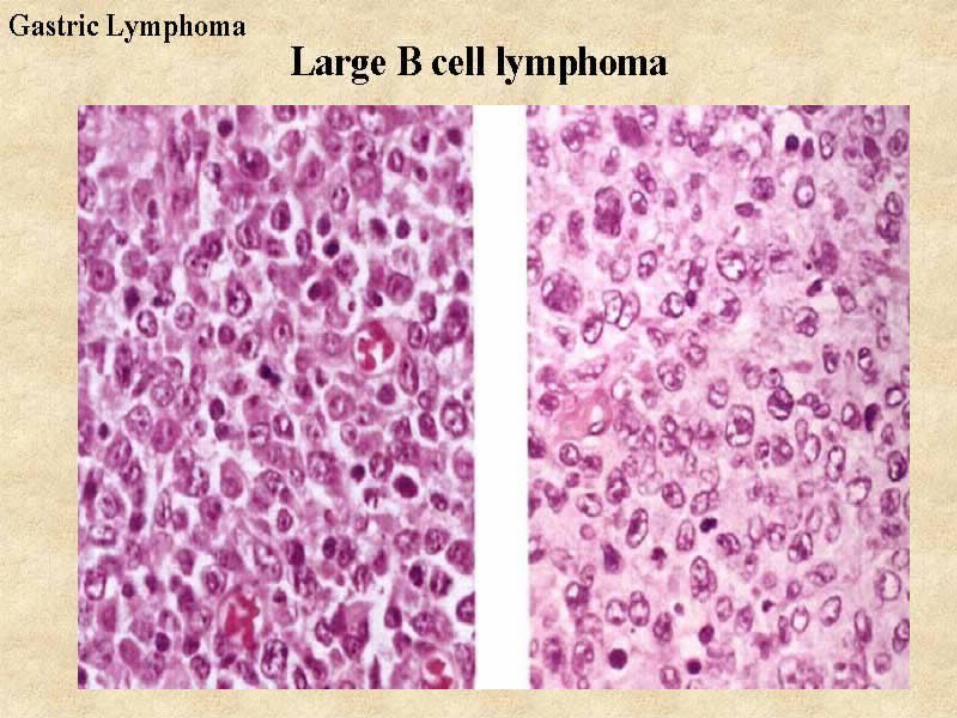
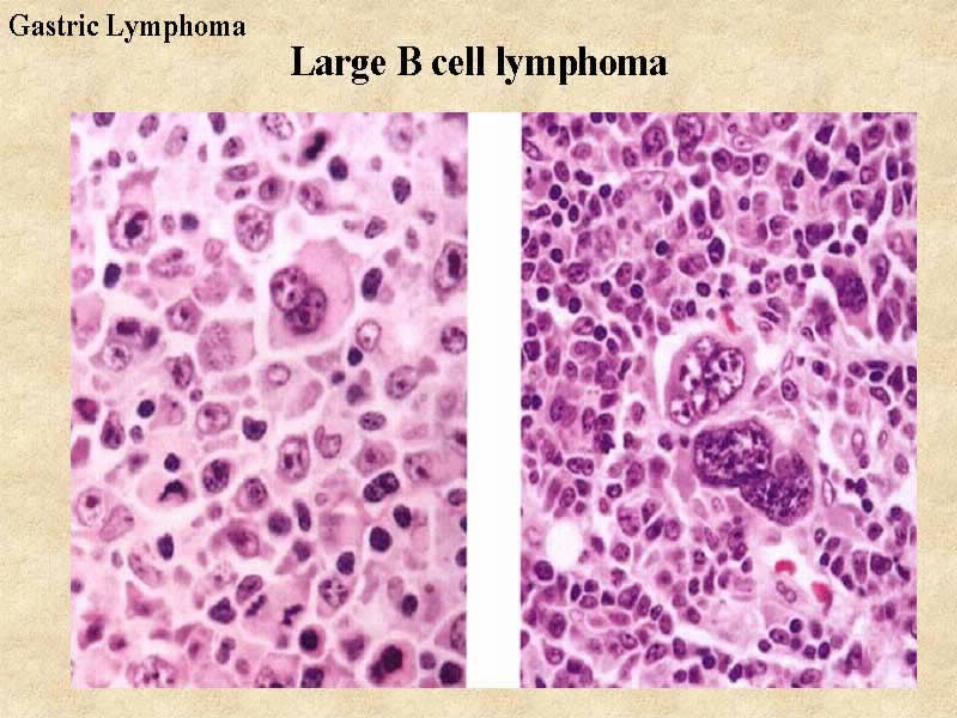
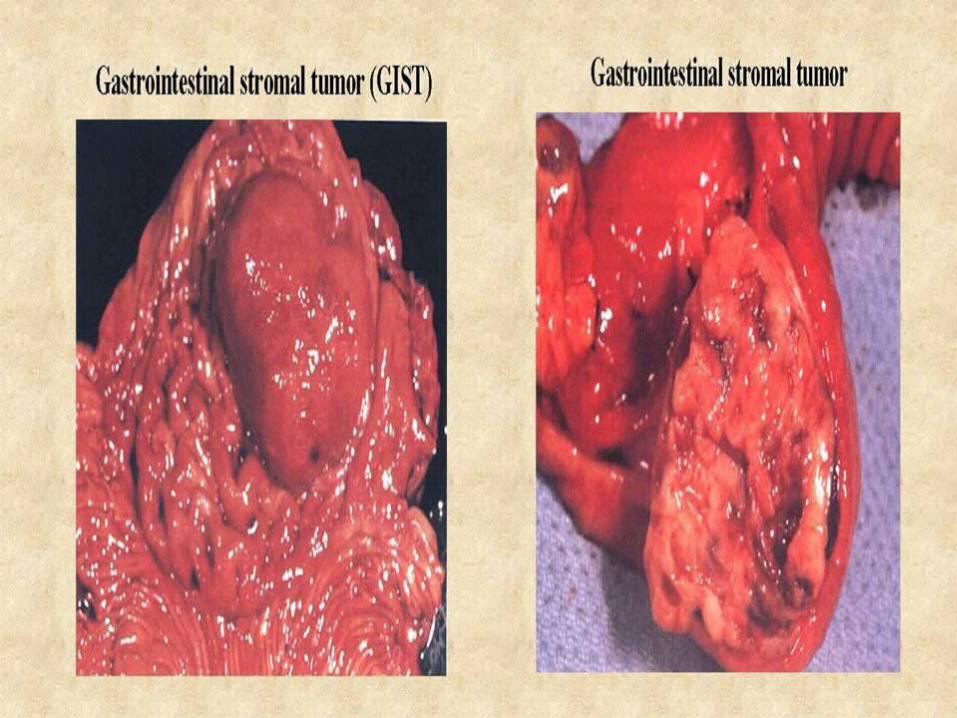
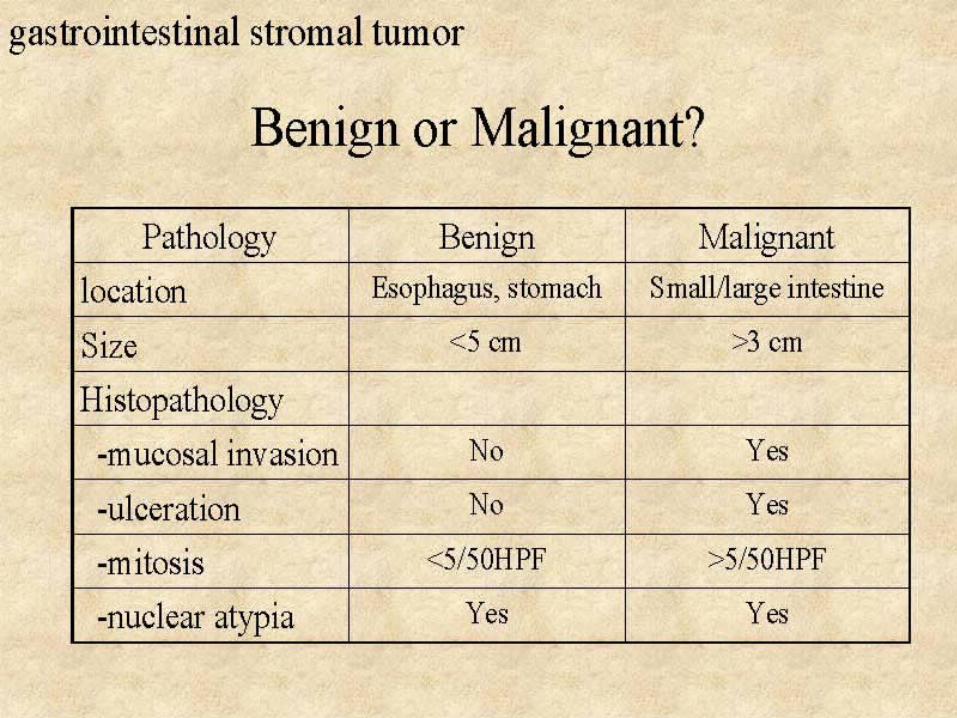
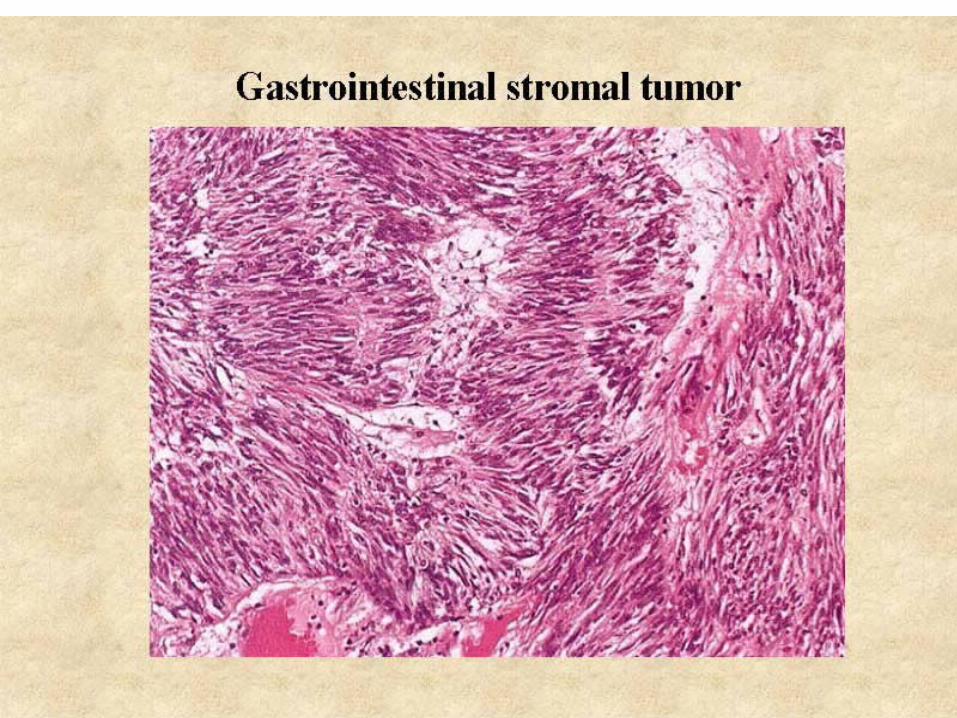
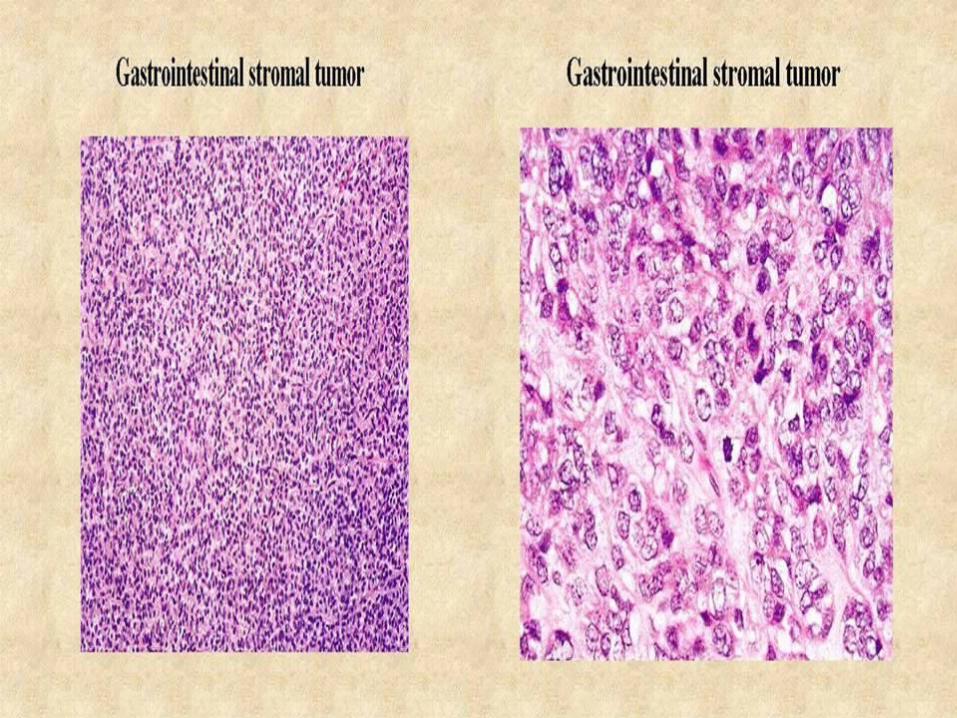
Less Common Gastric Tumors:Lymphomas (~ 5%) Stromal tumors (~ 2%) Carcinoid tumors (rare)
GASTRIC CARCINOMA
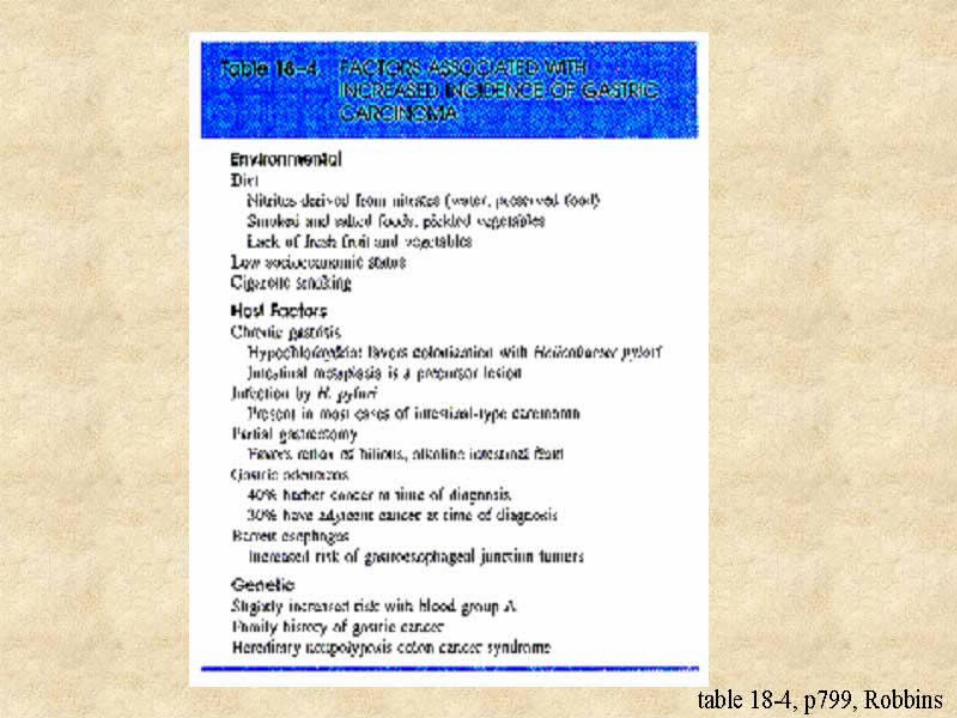
Risk Factors: Diet: Nitrites (food preservatives), smoked &
salted foods, deficiency of fresh fruits & vegetables
Host Factors: chronic gastritis (autoimmune & H. pylori), adenomatous polyps, partial gastrectomy
Genetic Factors: only ~ 4% of patient’s w/ gastric CA have a family Hx
![Lymphocytic gastRitis - Termedia surface and foveolar epithelial cells [1, 2, 3]. Those lymphocytes are usually round and small [2]. Inside the cells, there is a clear halo, nuclei](https://img.pdfslide.net/doc/110x75/5f7f3b8c0deed929a5772a94/lymphocytic-gastritis-termedia-surface-and-foveolar-epithelial-cells-1-2-3.jpg)