Embed Size (px)
Citation preview

SF
InhcutletamotsepppssldpSs
PSWcpbstf
*†‡A
2
tretch-Related Myelopathyraser Henderson, MD,* Edward C. Benzel, MD,† and Alexander R. Vaccaro, MD‡
trfsisvfiwbattil
CCpiieoatlugmisdfl1(b
noetc
t is now widely accepted that stretch is a principal etiologicfactor in tethered cord syndrome. Pain, numbness, weak-
ess, pes cavus, scoliosis, and bowel and bladder dysfunctionave all been attributed to stretching injury of the spinalord.1-7 The degree or amount of traction on the conus med-llaris determines the age or onset of symptoms. Extensiveethering and severe stretching of the conus results in neuro-ogical disturbances in infancy, while a lesser degree of teth-ring often remains subclinical until adulthood, at whichime symptoms manifest in the setting of an acute event, suchs hyperflexion injury, or chronic process, such as develop-ent of ventral disc or osteophytes. Clinical manifestations
f tethered cord syndrome are most commonly referable tohe lumbosacral cord, but patients often exhibit neurologicaligns and symptoms originating from the cervical cord. Forxample, long tract involvement may lead to interscapularain, hand numbness, and poor coordination, as well as up-er extremity hyperreflexia. Quadriparesis has also been re-orted.9 This phenomenon supports the hypothesis that ten-ion within the spinal cord might be transmitted to remoteegments of the cord. It has been suggested that injury to thearge-diameter fibers of the corticospinal tracts occurs someistance from the actual tethering, and results in the clinicalicture of mixed upper and lower motor neuron deficits.8
ignificant spinal cord stretching has been observed in onetudy up to five segments from the site of tethering.
athology ofpinal Cord Stretch Injurye now understand the material properties and biome-
hanical behavior of spinal cord tissue under varioushysiological and pathological conditions. A growingody of evidence indicates that abnormal movement of thepine may result in increased strain and shear forces andhat these pathological forces can cause both diffuse andocal axonal injury within the spinal cord. The concept
Department of Neurosurgery, Georgetown University, Washington, DC.The Cleveland Clinic, Cleveland, OH.Thomas Jefferson University and the Rothman Institute, Philadelphia, PA.ddress reprint requests to Fraser Henderson, MD, Department of Neuro-
surgery, Georgetown University, Washington, DC. E-mail: hendersf@
(gunet.georgetown.edu.1040-7383/05/$-see front matter © 2005 Elsevier Inc. All rights reserved.doi:10.1053/j.semss.2005.01.007
hat increased mobility coupled with kyphotic deformityesults in spinal cord elongation and increased axial strainorces is well known.10,11 Even low-grade mechanicaltretching on neural tissues can have adverse effects. Dur-ng normal motion, large axial strains occur in the cervicalpinal cord.12 The white matter of the spinal cord can beiewed as an axial array of parallel fibers with individualbers demonstrating variable levels of crimping. As ahole, the cord is initially compliant to stretch, but itecomes progressively stiffer as the fibers straighten outnd bear tensile load.13 Rapid strains can exceed the ma-erial properties of the tissue and cause disruption andransient or permanent neurological injury. The degree ofnjury is related to the peak strain of the tissue and theoading rate.14
adaveric Studiesadaver studies of the cervical spine suggest that evenhysiological flexion of the cervical spine leads to stretch-
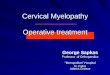
ng and the production of strain forces within the neurax-s.10 Flexion of the spinal column results in significantlongation of the spinal canal with concomitant stretchingf the spinal cord (Fig. 1). Physiological flexion of the headnd trunk in rhesus monkeys results in net movement ofhe spinal cord from the upper spine downward to theevel of C4 to 5, while net movement of the cord occurspward below this level.11 Net movement occurs to areater extent below C4 to 5, with only 1.6 mm of move-ent at C1 and 6 mm of movement at T3. Net movement
s small, but stretch is large, the amount of spinal cordtretch occurring at each level being proportional to theegree of flexion at the adjacent disc space. The amount ofexion is greatest at the cervicothoracic junction with a7.6-mm-length increase, and the local spinal cord strainstrain � increase in length, �/L, where L is the lengthefore stretching) reaches 24%.15
Normally, elongation of the spinal cord that occurs witheck flexion (and sometimes hyperextension) is distributedver the entire length of the spinal cord. However, with teth-ring of the spinal cord, the axial strain cannot be distributedhroughout the cord and is instead limited to the segment oford between the distracting force and the tethering point
Fig. 2).
ragtocotscsmswatt
SaSIsim
dkodpsvit
BFSAaLitiatedfo
acnrihis
BSIspscei
Fms
Fflt
Stretch-related myelopathy 3
The tethering action of the dentate ligaments may beesponsible for accentuating the effect of tensile cord stressnd exacerbating local tissue injury. Local spinal cord de-enerative changes are frequently identified adjacent tohickened dentate ligaments, suggesting that localizationf injurious mechanical forces at these levels may be asso-iated with the tethering effect of the ligaments.11,16 More-ver, dorsal displacement of the spinal cord as a result ofhe presence of ventral spondylotic bars may lead totretching of the dentate ligaments and tethering of theervical cord via the anterolaterally positioned nerve rootleeves. Repetitive microtrauma to these nerve root sleevesay lead to the progressive thickening that has been ob-
erved with age.16 Therefore, axial tension generatedithin the spinal cord during physiological motion may be
mplified at certain levels as a result of two separate fac-ors— overall spinal canal lengthening as well as the localethering effects of the dentate ligaments.
tretch Injury asCause of Cervicalpondylotic Myelopathy
nvestigators have attributed delayed progressive cervicalpondylotic myelopathy (CSM) to a combination of underly-ng structural kyphosis and abnormal or excessive cervical
otion.17,18
Dynamic lengthening of the cervical cord that occursuring neck flexion is magnified in patients with cervicalyphosis. Conversely, kinematic MRI studies have dem-nstrated that lengthening of the spinal cord also occursuring neck extension in some patients with fixed ky-hotic deformity of the cervical spine.19 In the setting oftatic cord compression and superimposed instability, cer-ical extension can also lead to aggravation of the cordmpingement and significant upper cervical cord elonga-
igure 1 The spinal cord undergoes significant stretch on routineexion of the cervical spine. Note the ruler before and after flexion;he spinal cord increases in length by 25%.
ion. d
iomechanicalactors in Cervicalpondylotic Myelopathy
bnormal or excessive motion of the cervical spine is stronglyssociated with clinical progression of CSM. Adams andogue performed a retrospective clinical review demonstrat-
ng that a cervical flexion/extension arc in excess of 40° washe most significant variable predicting poor clinical outcomen patients with CSM.20 Others have shown that patients withflexion/extension arc of greater than 60° following laminec-
omy were at increased risk for developing progressive my-lopathy.21,22 Conversely, elimination of excessive motionecreases pain and deficit: for example, a cervical collar af-ords relief to patients with cervical myeloradiculopathy sec-ndary to disc protrusion.23
Furthermore, the excellent long-term clinical results associ-ted with the elimination of abnormal cervical motion for CSMontrast with the poorer results following decompressive lami-ectomy alone. The largest series of patients undergoing ante-ior decompression and fusion for CSM demonstrated an 86%mprovement rate with no significant deterioration.24 Othersave also argued that elimination of movement by fusion and
nstrumentation is associated with more favorable clinical re-ults than decompression alone.25-34
iomechanical Models oftretch-Related Injury in CSM
n an attempt to explain the findings of histopathologicaltudies of CSM, Breig developed a mechanical model to ex-lain how a focal compressive force could result in wide-pread changes. His cadaveric models demonstrated thatompression forces acting ventrally on the cord, in the pres-nce of stenosis, created a pincer mechanism resulting inncreased axial tension in the cord and fissuring opposite the
igure 2 Tethering is the limitation of normal displacement or move-ent of a structure. The cord can be “tethered” by stenosis and other
pinal lesions, such as tumors, which limit the ability of the cord to
issipate the strain generated by flexion of the neck.
sssApprm
tssicspltoq
ESLEctpafsltrl
isvtm
HHTtsamiitmco
mrsc
lSarrotrdmiwdsdatnt
HSMtc
ha
dbi
dtap
jlufmtfidqaos
4 F. Henderson, E.C. Benzel, and A.R. Vaccaro
ide of compression. In this model the spinal cord is repre-ented as a viscoelastic cylinder, which compressed from theides exhibits net tissue creep to the free ends of the cylinder.s a result, tension forces were created perpendicular to thelane of compression. This model explains how ventral com-ression of the spinal cord in the presence of stenosis mightesult in stretch and shear injury to myelin and neural ele-ents.35
A mathematical model by Levine showed that flattening ofhe cord was not simply the result of ventral-dorsal compres-ion, but primarily a consequence of laterally directed ten-ion arising from the dentate ligaments which tighten in flex-on.36 He showed how a ventral spondylotic bar in CSMoupled with the tethering effects of dentate ligaments re-ulted in maximal stresses in the lateral funiculi. The modelrovides a possible explanation for the characteristic histo-
ogical findings in CSM in which there is relative sparing ofhe anterior and posterior funiculi. However, the importancef the dentate ligaments in the etiology of CSM remains inuestion.37
xperimentaltudies Involving theumbar and Sacral Cord
xperimental studies involving the lumbar and sacral cord ofats have demonstrated that acute tethering is very traumatico spinal cord tissue, particularly when stretching occurs re-eatedly.38 Spinal cord elongation is pronounced immedi-tely adjacent to the point of application of the tetheringorce. Under low levels of tension, the spinal cord demon-trates purely elastic behavior and returns to normal restingength. At greater tension, plastic deformation occurs. Por-ions of the spinal cord near the point of application of stretchemain elongated 7% over the original length, even after re-ease of tension.
Tethering in a guinea pig model of spinal cord stretchnjury results in significant delay and decreased amplitude ofomatosensory evoked potentials. EM shows potentially re-ersible histological changes, such as edema, destruction ofhe gray-white junction, axonal injury with loss of neurofila-ents, and evidence of myelin sheath damage.39
umanistopathological Studies
he axonal injury and edema seen in experimental models ofethered cord syndrome resembles spinal cord injury in amall group of elderly patients involved in motor vehicleccidents.40 Although the spinal cords were grossly intact,icroscopic examination revealed diffuse axonal disruption
n the deeper white matter of the lateral columns, particularlyn the corticospinal tracts, with only modest axonal disrup-ion in the ventral and dorsal columns. The localization ofyelin pallor and axonal injury in the corticospinal tracts in
ases of trauma is also similar to that noted in autopsy studies
f CSM patients41-44 and rheumatoid arthritis patients with ayelopathy due to basilar invagination.45 In the latter, axonaletraction balls and myelin pallor were interpreted to betretch-related, and there was no evidence of ischemichange.
Breig showed that the spinal cord can be tethered at anyevel by scarring, external compression, or spinal deformity.pinal cord deformation over a large disc herniation at thepex of a kyphosis can contribute to stretch and shear injuryemote from the locus of deformation.35 For example, neu-ological dysfunction of basilar invagination may be a resultf deformation and stretch injury of the neuraxis: deforma-ion of the medullospinal junction over the odontoid processesults in both local and remote neurological dysfunction—iplopia, dysphagia, dysarthria, vertigo, as well as sensori-otor deficits.46 While these effects may also be explained by
schemic injury, local ischemia has not been found.45 Patientsith Chiari malformations with deformity of the brainstemue to mild basilar invagination fail to improve with simpleuboccipital decompression if significant ventral medullaryeformity persists.47,48 Furthermore, disturbances of sleepnd alterations in central respiratory function have been at-ributed to medullary deformity secondary to basilar invagi-ation, and these disturbances have been reversed by correc-ion of ventral medullary deformity.49
istopathology ofpinal Cord Shear Injuryyelin edema and reactive axonal changes appear to be his-
opathological manifestations of stretch injury. Thesehanges are similar to diffuse axonal injury (DAI).
DAI is the most common brain injury resulting from bluntead trauma, and patient morbidity has been directly associ-ted with the extent of DAI.50,51
Recent studies of DAI have demonstrated that axons un-ergoing shear strain do not undergo immediate disruption,ut rather a nondestructive injury, and delayed axonal swell-
ng in internodal regions.52
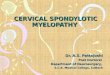
Axonal stretch at the time of injury results in axolemmalamage, disruption of axon transport and metabolism, andhe delayed formation of an “axon retraction ball” or reactivexonal swelling.53 (Fig. 3) This focal swelling is thought toresage secondary axotomy.54-57
The cell ultrastructural events proceeding from axonal in-ury have been well characterized.55 Axon cytoskeletal col-apse and rapid loss of the microtubular network appear tonderlie the observed impairment of axoplasmic transportollowing injury.58 Neurofilaments have been implicated in
aintenance of axon caliber, while microtubules are thoughto provide the mechanism for fast axonal transport. Neuro-lament compaction is thought to precede the cytoskeletalisappearance accompanying Wallerian degeneration. Auantitative analysis of injury-associated changes within thexoskeleton show evidence of injury throughout the lengthf the axon, but maximal changes in the midportion of thetretched nerve. Axons demonstrate enlargement of the para-
xonal space, compaction of neurofilaments, loss of microtu-
bmmi
pafaddsbdtcbd
pcfCadsim
mAmacc
RSISismwoc
cit
isitamlajtrcg
CSeaepvsseooa
R
Fblisto
Stretch-related myelopathy 5
ules, and reduction in axonal caliber. Collapse of neurofila-ents into tightly packed bundles in the center of the axonay precede secondary axotomy in nondisruptive stretch
njury of central nerves.58
Continued anterograde transport to the site of focal im-airment appears to result in localized ballooning of the axonnd formation of a reactive axon bulb or “Strich ball.” Withurther enlargement of the bulb, thinning of the overlyingxolemma and myelin sheath occurs. Eventually, anatomicisconnection occurs between axonal segments proximal andistal to the original site of injury. The overlying myelinheath is disrupted and then reforms to enclose the axonulb, while the distal axonal segment undergoes Wallerianegeneration. Meanwhile, the proximal axon bulb continueso expand due to continued anterograde transport of intra-ellular contents from the neuronal soma. In rodent studies,y 14 days, most reactive axons degenerate, become electronense, and are eventually phagocytized by microglia.Injury-associated changes in the axonal cytoskeleton are
receded by alterations in axolemmal permeability. In-reased calcium influx has been demonstrated in axons suf-ering stretch injury.59 Presumed loss of activity of the ecto-a-ATPase pump at sites of myelin disruption are thought tollow increased calcium influx into the myelin, possibly me-iating myelin dissociation and an increase in the periaxonalpace over a period of several hours. Increased calcium influxnto the injured axon may result in proteolysis of neurofila-
ents and dephosphorylation of neurofilament sidearms.59
In severe spinal cord injury, calcium-induced neurofila-entous degradation can be detected within 30 minutes.natomically, axons appear to be disrupted at sites of maxi-al tension. Large-caliber axons with a long intraaxial course
ppear to be more susceptible to tensile injury. Reactivehanges have been observed where axons change course,
igure 3 Electron micrograph of axon retraction balls. Retractionalls represent the accumulation of organelles within the axon fol-
owing a stretch injury. The accumulation appears to be the result ofnjury to the axolemma, loss of normal calcium gradient, and sub-equent clumping of neurofilaments and microtubules. Axon retrac-ion balls presage axotomy. (Color version of figure is availablenline.)
ross blood vessels, and decussate.60
elationship betweentretch-Related Myelopathy,
schemia, and Apoptosistretch injury renders axons more susceptible to secondarynjury from other processes, including ischemia and apopto-is.61 The role of ischemia in stretch-related injury is unclear:icroscopic studies have shown none of the changes oneould expect with ischemia, either in the microvasculaturer in the neuronal soma, axonal processes, or dendritic pro-esses.52,62
Iodoantipyrine studies have revealed no significanthanges in regional blood flow.62 Moreover, axons undergo-ng reactive change are frequently found surrounded by in-act neurons without any evidence of ischemia or injury.
Recent studies suggest that a significant portion of cell lossn chronic compression-related myelopathy is due to apopto-is.61 Cell loss occurs in spinal cord injury at both the time ofnjury and secondarily over a period lasting days to weeks. Athe injury epicenter, most cell death occurs through necrosisnd leads to active clearance of necrotic cell debris throughacrophage and microglial phagocytosis. White-matter cell
oss then continues through a longer segment of the cord forperiod of several weeks in a process called “secondary in-
ury.” A prominent role for apoptosis has been implicated inhis secondary cell loss following traumatic spinal cord inju-y.63-69 Animal studies have demonstrated that compressiveord injury leads to apoptosis of oligodendrocytes along de-enerating white-matter tracts.69
onclusionstretching of the deformed or tethered cord leads to the gen-ration of injurious tensile and shear forces in constituentxons. Strong support for the stretch-related theory of my-lopathy comes from an increased understanding of theathogenesis of spinal cord tethering, histological studies re-ealing reactive axonal injury in the spinal cord, and a moreophisticated understanding of the pathophysiology oftretch-related myelin and axonal injury. Stretch forces gen-rated within the spinal cord may be important factors notnly in the pathogenesis of tethered cord syndrome but alsother degenerative conditions and traumatic conditions suchs cervical spondylotic myelopathy and whiplash injury.
eferences1. Sostrin RD, Thompson JR, Roue SA, et al: Occult spinal dysraphism in
the geriatric patient. Radiology 125:165-169, 19772. Kaplan JO, Quencer RM: The occult tethered cord syndrome in the
adult. Radiology 137:387-391, 19803. Hoffman HJ, Hendrick EB, Humphreys RP: The tethered spinal cord:
its protean manifestations, diagnosis and surgical correction. ChildsBrain 2:145-155, 1976
4. Garceau JG: The filum terminale syndrome. J Bone Joint Surg Am35:711-716, 1953
5. Fitz CR, Nash DC: The tethered conus. Am J Neuroradiol 125:515-523,1975
6. Breig A: Overstretching of the spinal cord—a basic cause of symptoms
in cord disorders. J Biomech 3:7-9, 1970
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
6 F. Henderson, E.C. Benzel, and A.R. Vaccaro
7. Pierre-Kahn E, Lacombe J, Pichon J, et al: Intraspinal lipomas withspina bifida. J Neurosurg 65:756-761, 1986
8. Pang D, Wilberger JE: Tethered cord syndrome in adults. J Neurosurg57:32-47, 1982
9. Rogers HR, Long DM, Chou SN, et al: Lipomas of the spinal cord andthe cauda equina. J Neurosurg 34:349-354, 1971
0. Breig A, Turnbull I, Hassler O: Effects of mechanical stresses upon thecervical cord in cervical spondylosis: a study on fresh cadaver material.J Neurosurg 25:45-56, 1966
1. Smith CG: Changes in the length and position of the spinal cord withchanges in posture in the monkey. Radiology 66:259-266, 1956
2. Margulies S, Meaney DF, Bilston LB, et al: In vivo motion of the humancervical spinal cord during extension and flexion. Proceedings of theIRCOB Conference. Verona, Italy, 1992
3. Bilston LE, Thibault LE: The mechanical properties of the human cer-vical spinal cord in vitro. Ann Biomech Eng 24:67-74, 1996
4. Galbraith JA, Thibault LE, Matteson DR: Mechanical and electricalresponses in the giant squid axon to simple elongation. J Biomech Eng115:13-22, 1993
5. Reid JD: Effects of flexion extension movements on the head and spineupon the spinal cord and nerve roots. J Neurol Neurosurg Psychol23:214-222, 1960
6. Bedford PD, Bosanquet FD, Russell WR: Degeneration of the spinalcord associated with cervical spondylosis. Lancet 55-59, 1952
7. Sim FH, Svien HJ, Bickel WH, et al: Swan neck deformity followingextensive cervical laminectomy: a review of 21 cases. J Bone Joint SurgAm 56:564-580, 1974
8. Snow RB, Weiner RH: Cervical laminectomy and foraminotomy assurgical treatment of cervical spondylosis: a follow-up study with anal-ysis of failures. J Spinal Disord 6:245-251, 1993
9. Muhle C, Metzner J, Weinert D, et al: Kinematic imaging in surgicalmanagement of cervical disc disease, spondylosis and spondylotic my-elopathy. Acta Radiolog 40:146-153, 1999
0. Adams CBT, Logue V: The movement and contour of the spine inrelation to the neural complications of cervical spondylosis. Brain 94:569-586, 1971
1. Barnes MP, Saunders M: The effect of cervical mobility on the naturalhistory of cervical spondylotic myelopathy. J Neurol Neurosurg Psy-chol 47:17-20, 1985
2. Yonenobu K, Okada K, Fuji T, et al: Causes of neurological deteriora-tion following surgical treatment of cervical myelopathy. Spine 11:818-823, 1986
3. Campbell AMG, Phillips DG: Cervical disc lesions with neurologicdisorder. Br Med J 2:481-485, 1960
4. Eleraky MA, Llanos C, Sonntag VKHL: Cervical corpectomy: report of185 cases and review of the literature. J Neurosurg 90:35-41, 1999
5. Gonzalez-Feria L: The effect of surgical immobilization after laminec-tomy in the treatment of advanced cases of cervical myeloopathy. ActaNeurotic (Wien) 31:185-193, 1975
6. Ebersold MJ, Pare MC, Quast LM: Surgical treatment for cervical spon-dylitic myelopathy. J Neurosurg 82:745-751, 1995
7. Saunders RL, Bernini PM, Shireffs TGJ, et al: Central corpectomy forcervical spondylotic myelopathy: a consecutive series with long-termfollow-up evaluation. J Neurosurg 74:163-170, 1991
8. Zdeblick TA, Bohlmann HH: Cervical kyphosis and myelopathy: treat-ment by anterior corpectomy and strut grafting. J Bone Joint Surg Am71:170-182, 1989
9. Bernard TNJ, Whitecloud TSI: Cervical spondylotic myelopathy andmyeloradiculopathy: anterior decompression and stabilization with au-togenous fibular strut graft. Clin Orthop Rel Res 221:149-160, 1987
0. Seifert V, Stolke D: Multisegmental cervical spondylosis: treatment byspondylectomy, microsurgical decompression and osteosynthesis.Neurosurgery 29:498-503, 1991
1. Kojima T, Waga S, Kubo Y, et al: Anterior cervical vertebrectomy andinterbody fusion for multilevel spondylosis and ossification of the pos-terior longitudinal ligament. Neurosurgery 24:864-872, 1989
2. Maurer PK, Ellenbogen RG, Ecklund J, et al: Cervical spondylotic my-elopathy: treatment with posterior decompression and Luque rectangle
bone fusion. Neurosurgery 29:680-684, 19913. Kumar VGR, Rea GL, Mervis LJ, et al: Cervical spondylotic myelopathy:functional and radiographic long-term outcome after laminectomy andposterior fusion. Neurosurgery 44:000-000, 1999
4. Cusik JF, Steiner RE, Berns T: Total stabilization of the cervical spine inpatients with cervical spondylitic myelopathy. Neurosurgery 18491-18495, 1986
5. Breig A: Effects of pincer and clamping actions on the spinal cord, inAdverse Mechanical Tension in the Central Nervous System. New York,NY, Wiley, 1978, pp 61-83
6. Levine DN: The pathogenesis of cervical spondylotic myelopathy.J Neurol Neurosurg Psychol 62:334-340, 1997
7. Bishara SN: The posterior operation in treatment of cervical spondylo-sis with myelopathy: a long-term follow-up study. J Neurol NeurosurgPsychol 34:393-398, 1971
8. Tani S, Yamada S, Knighton RS: Extensibility of the lumbar and sacralcord: pathophysiology of the tethered spinal cord in cats. J Neurosurg66:116-123, 1987
9. Kocak A, Kilik A, Nurlu G, et al: A new model for tethered cord syn-drome: a biochemical, electrophysiological and electron microscopicstudy. Pediatr Neurosurg 34:120-126, 1997
0. Bunge RP, Puckett WR, Becerra JL, et al: Observations on the pathologyof human spinal cord injury. A review and classification of 22 new caseswith details from a case of chronic cord compression with extensivefocal demyelination, in Advances in Neurology, Vol. 59. New York, NY,Raven Press, 1993, pp 75-89
1. Ogino H, Tada K, Okada K, et al: Canal diameter, antero-posteriorcompression ratio, and spondylotic myelopathy of the cervical spine.Spine 8:1-15, 1983
2. Dastur DK, Wadia NH, Desai AD, et al: Medullospinal compression dueto atlantoaxial dislocation and sudden hematomyelia during decom-pression. Brain 88:897-927, 1965
3. Wadia NH: Myelopathy complicating congenital atlantoaxial disloca-tion. Brain 90:449-470, 1967
4. Nakano KK, C SW, Baker RA, et al: The cervical myelopathy associatedwith rheumatoid arthritis: analysis of 32 patients with two postmortemcases. Ann Neurol 3:144-151, 1978
5. Henderson FC, Geddes JF, Crockard HA: Neuropathology of the brain-stem and spinal cord in end stage rheumatoid arthritis: implications fortreatment. Ann Rheum Dis 52:629-637, 1993
6. Menezes AH, van Gilder JC, Clark CR, et al: Odontoid upward migra-tion in rheumatoid arthritis. J Neurosurg 63:500-509, 1985
7. Levy WJ, Mason L, Hahn JF: Chiari malformation presenting in adults:a surgical experience in 127 cases. Neurosurgery 12:377-390, 1983
8. Paul KS, Lye RH, Strange FA, et al: Arnold-Chiari malformation: reviewof 71 cases. J Neurosurg 58:137-183, 1983
9. Howard RS, Henderson FC, Hirsch NP, et al: Respiratory abnormalitiesdue to craniovertebral junction compression in rheumatoid disease.Ann Rheum Dis 53:134-136, 1994
0. Adams JH, Mitchell DE, Graham DI, et al: Diffuse brain damage ofintermediate impact type: its relationship to “primary brainstem dam-age” in head injury. Brain 100:487-502, 1977
1. Adams JH, Graham DI, Murray LS, et al: Diffuse axonal injury due tonon-missile injury in humans: an analysis of 45 cases. Ann Neurol12:557-563, 1982
2. Povlishok JT, Becker DP, Cheng CLY, et al: Axonal change in minorhead injury. J Neuropathol Exp Neurol 42:225-242, 1983
3. Erb DE, Povlishok JT: Axonal damage in severe traumatic brain injury:an experimental study in cat. Acta Neuropatholog 76:347-358, 1988
4. Povlishok JT: Traumatically induced axonal injury: pathogenesis andpathobiological implications. Brain Pathol 2:1-12, 1992
5. Christman CW, Grady MS, Walker SA, et al: Ultrastructural studies ofdiffuse axonal injury in humans. J Neurotrauma 11:173-186, 1994
6. Maxwell WL, Irvine A, Graham DI, et al: Focal axonal injury: the earlyresponse to stretch. J Neurocytol 20:157-164, 1991
7. Pettus EH, Povlishok JT: Characterization of a distinct set of intra-axonal ultrastructural changes associated with traumatically inducedalteration in axolemmal permeability. Brain Res 722:1-11, 1996
8. Jafari S, Maxwell WL, Neilson M, et al: Axonal cytoskeletal changes
after non-disruptive axonal injury. J Neurocytol 26:207-221, 1997
5
6
6
6
6
6
6
6
6
6
6
Stretch-related myelopathy 7
9. Maxwell WL, McGreath BJ, Graham DI, et al: Cytochemical evidencefor redistribution of membrane pump calcium-ATPase and ecto-Ca-ATPase activity and calcium influx into myelinated nerve fibers of theoptic nerve after stretch injury. J Neurocytol 24:925-942, 1995
0. Povlishok JT, Jenkins LW: Are the pathobiological changes evoked bytraumatic brain injury immediate and reversible? Brain Pathol 5:415-426, 1995
1. Yamaura I, Yone K, Nakahara S, et al: Mechanism of destructive patho-logic changes in the spinal cord under chronic mechanical compres-sion. Spine 27:21-26, 2002
2. Povlishok JT: Current concepts on axonal damage due to head injury.Proceedings of the 11th International Congress of Neuropathology,1991:749-753.
3. Majno G, Joris I: Apoptosis, oncosis, and necrosis: an overview of celldeath. Am J Pathol 146:3-15, 1995
4. Katoh K, Ikata T, Katoh S, et al: Induction and its spread of apoptosis
in rat spinal cord after mechanical trauma. Neurosci Lett 216:9-12,1996
5. Crowe MJ, Bresnahan JC, Shuman SL, et al: Apoptosis and delayeddegeneration after spinal cord injury in rats and monkeys. Nat Med3:73-76, 1997
6. Liu XZ, Up XM, Hun R, et al: Neuronal and glial apoptosis after trau-matic spinal cord injury. J Neurosci 17:5395-5406, 1997
7. Springer JE, Azbill RD, Knapp PE: Activation of the caspase-3 apoptoticcascade in traumatic spinal cord injury. Nat Med 5:943-946, 1999
8. Grossman SD, Rosenberg LJ, Wrathall JR: Temporal-spatial pattern ofacute neuronal and glial loss after spinal cord contusion. Exp Neurol168:273-282, 2001
9. Li GL, Brodin G, Farooque M, et al: Apoptosis and expression of Bcl-2after compression trauma to rat spinal cord. J Neuropathol Exp Neurol
55:280-289, 1996