Embed Size (px)
Citation preview

Stroke

Stroke
• Sudden in onset• Focal neurologic deficit• Involvement of the blood vessels

Temporal profiles of neurologic deficits that point to the underlying pathologic cause.
-Mayo Clinic

Types of Stroke

DIFFERENTIAL DIAGNOSIS
STROKE
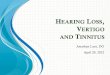
Ischemia, 85% Hemorrhage, 15%
Atherothrombotic Embolic Other
Clinical Types of Stroke in the PHILIPPINES61.39% Ischemic38.6% Hemorrhagic

Hemorrhagic Stroke
• Primary Intracerebral hemorrhage– Inside the brain– defective artery in the brain bursts– Bleed in the substance of the brain --. Basal ganglia (60%
recurrence) 10 % recurrence at the different lobes, 10% at the cerebellum, 10% recurrence a
– Secondary to hypertension• Subarchanoid Hemorrhage –
– Outside the brain– a blood vessel on the brain's surface ruptures and bleeds– annuerysm, AVM

Hemorrhagic Stroke• intracerebral > subarachnoid hemorrhage • Occur during stress or exertion• Focal deficits rapidly evolve • Confusion, coma or immediate death

Hemorrhagic Stroke
• Classic: sudden onset headache, vomiting, elevated BP
• Focal neurologic deficits that progress over minutes
• May present with agitation and lethargy but progresses to stupor or coma

Ischemic Stroke
• Thrombus forms and blocks blood flow in an artery bringing blood to part of the brain

Ischemic Stroke• Sudden onset of a non-convulsive, FND due to CVD
• Embolic strokes – Deficit reaches its peak almost at once– Reverses itself within a few hours or days
• Thrombotic strokes – Evolve more slowly over a period of several min/hrs and occasionally
days– Improve gradually over weeks or months
• Cerebral Hemorrhage– There is severe deficit of rapid but not necessarily instantaneous
onset

Ischemic Stroke: Thrombotic
• Local Origin of Clot• Usually develops at night during sleep• Symptoms perceived in the morning• Suspect in history of atherosclerosis,
hypercoaguable states and collagen vascular disorders

Thrombotic
• 1/3 of ischemic strokes, occlude large cerebral arteries (lCA, MCA, basilar), small penetrating arteries (lacunar strokes), cerebral veins, and venous sinuses.
• Symptoms evolve over minutes to hrs. • Often preceded by TIA in same territory
causing similar deficits.

Ischemic Stroke: Embolic
• Proximal origin of clot• Occurs at any time• Frequently during periods of vigorous activity• History of AF, valvular vegetations,
thromboembolism from MI, ulcerated plaques in carotid system
• Seizures in 20% of cases

Embolic
• 2/3 of ischemic strokes, from thrombus in heart, aortic arch, large cerebral artery or medium sized branches of brain a.
• In anterior circulation usually effect MCA , in posterior circulation usually effect branch point of basilar or PCA.
• Produce maximal neurological deficit at onset. • When TIAs precede, symptoms vary because
emboli lodges in different places.

Ischemic Stroke
• Classic: sudden onset of headache, vomiting, BP
• Focal neurological deficits progress over minutes
• May present with agitation & lethargy but progresses to stupor & coma
• Lacunar—small vessel disease

Diagnosis

Diagnose
• Clinical Presentation• Neuroimaging/neurosonology• Establish mechanism/s

Clinical Presentation
• WILL BE DISCUSSED BY ANOTHER TRIO

Neuroimaging/Neurosonology
• NeuroImaging• Cranial CT Scan – to differentiate infarct vs
hemorrhage• Timing of the test important when to do the
imaging• Cerebral Infarction 1st 6 hour normal• Bleeds abnormal at the start– Cranial MRI transmission weighted imaging
• Infarct early changes (DW1)• Diffusion-perfusion mismatch


• Neurosonology– Carotid Duplex Examination• Carotid Artery, Vertebral Artery, IMT (thickening)
– Stenosis• Obstruction– Transcranial Doppler Examination• Blood vessels inside the brain• Intracranial stenosis or occlusion
• non-invasive, can be repeated, accurate

Mechanism of stroke
• DISCUSSED ABOVE– HEMORRGAHIC, ISCHEMIC ETC

NIH Stroke Scale
• The National Institute of Health (NIH) stroke scale (NIHSS) is a standardized method used by physicians and other health care professionals to measure the level of impairment caused by a stroke.
• Assessment of whether or not the degree of disability caused by a given stroke merits treatment with tPA

NIH Stroke Scale
• The NIH stroke scale measures several aspects of brain function, including consciousness, vision, sensation, movement, speech, and language.
• A certain number of points are given for each impairment uncovered during a focused neurological examination.

NIH Stroke Scale
• A maximal score of 42 represents the most severe and devastating stroke. Current guidelines as of 2008 allow strokes with scores greater than 4 points to be treated with tPA.
• 0= no stroke• 1-4= minor stroke• 5-15= moderate stroke• 15-20= moderate/severe stroke• 21-42= severe stroke

NIH Stroke Scale• Level of
Consciousness (LOC)• 0-Alert• 1-Drowsy• 2-Stuporous• 3-Coma• • Best Gaze• 0-Normal• 1-Partial gaze palsy• 2-Forced deviation• • Best Motor Arm• 0-No drift• 1-Drift• 2-Can't resist gravity• 3-No effort against
gravity•
• LOC Answers Two Questions
• (Pt. asked two questions)
• 0-Answers correctly• 1-Answers one
correctly• 2-Answers none• • LOC Commands• (Patient given two
commands)• 0-Obeys both
correctly• 1-One correctly• 2-Incorrect• • Pupillary response• 0-Both react• 1-One reactive• 2-Neither reactive• • Best Visual• 0-No loss
• 1-Partial hemianopia• 2-Complete
hemianopia• • Facial Palsy• 0-Normal• 1-Minor• 2-Partial• 3-Complete• Best Motor Leg • 0-No drift• 1-Drift• 2-Can't resist gravity• 3-No effort against
gravity• • Plantar Reflex• 0-Normal• 1-Equivocal• 2-Extensor• 3-Bilaterally extensor•
• Limb Ataxia• 0-None• 1-Lower or upper• 2Both• • Sensory• 0-Normal• 1-Partial loss• 2-Dense loss• • Neglect• 0-None• 1-Partial• 2-Complete•
• Dysarthria• 0-Normal articulation• 1-Mild/moderate• 2-Near unintelligible
• • Best Language• 0-No aphasia• 1-Mild/moderate• 2-Severe• 3-Mute• • Change From
Previous Exam• same/better/worse• • Change From
Baseline• same/better/worse