Embed Size (px)
Citation preview
Laser and IPL Physics and Safety ‘Core of Knowledge’ – Laser/IPL light generation & characteristics (Unit 1)
Page 1 of 40 Copyright 2020 Online Laser Training Ltd. Updated: July 2020 UK 3
Student Resource
Physics and Safety Core of Knowledge –
Course Workbook 3
Laser & Intense Light Source Radiation - TissueInteraction
Authors:
Dr Godfrey Town Ph.D.
Patti Owens RN, BSN, MHA, CMLSO, CNOR

Laser and IPL Physics and Safety ‘Core of Knowledge’ – Laser/IPL light generation & characteristics (Unit 1)
Page 2 of 40 Copyright 2020 Online Laser Training Ltd. Updated: July 2020 UK 3
Dear Colleague,
Lasers and Intense Pulsed Light (IPL) Physics and Safety ‘Core of Knowledge’ – Unit 3: Laser &Intense Light Source radiation - tissue Interaction
The course is intended for aestheticians, beauty therapists, nurses, nurse practitioners, doctors,dentists and other personnel intending to use powerful lasers and IPL systems to performenergy-based treatments in cosmetic skin therapy. It is also suitable for healthcareprofessionals wishing to understand the safety controls and compliance necessary for the useof these devices for the treatment of disease, disorder or injury in all specialities includingOBGYN, ENT, orthopaedics, dental, etc.
This learning programme provides you with the necessary basic knowledge about light-basedtherapy and shares with you over 20 years of experience in light-based technology safety andskin therapy science. It will help you to offer “best practice” to your patients or clients andextend your ability to use light-based technology more effectively.
Upon completion, you will receive a professional Certificate of Achievement under theauthority of Dr Godfrey Town an RPA 2000 certified Laser Protection Adviser (Certificate No:L00159 dated 1st May 2018) that you can provide to your employer, insurer, CQC or localauthority responsible for regulating / licensing users of lasers and IPL devices confirming thatyou have successfully completed a recognised Laser and IPL Physics and Safety “Core ofKnowledge” course.
In addition, the course is worth 30 CPD learning credits (which is equivalent to a notional 30hours of learning) accredited by The CPD Accreditation Group and is approved by the BritishMedical Laser Association in the United Kingdom, The Royal Australasian College of GeneralPractitioners and Radiation Health, Queensland, Australia.
I hope that you will enjoy the course,
Dr Godfrey Town PhDInternational Course Director
Patti Owens RN, BSN, MHA, CMLSO, CNORCo-Author

Laser and IPL Physics and Safety ‘Core of Knowledge’ – Laser/IPL light generation & characteristics (Unit 1)
Page 3 of 40 Copyright 2020 Online Laser Training Ltd. Updated: July 2020 UK 3
TABLE OF CONTENTS
ABOUT THE AUTHORS 4
INTRODUCTION 5
COURSE OVERVIEW 5LASER & IPL SAFETY TRAINING 5BENEFITS ACHIEVEMENTS & FEEDBACK 5TRAINING FACULTY 6DISCLAIMER 6COURSE OBJECTIVES: 7
LASER & INTENSE LIGHT SOURCE RADIATION - TISSUE INTERACTION 8
INTERACTIONS OF LIGHT WITH TISSUE 8TISSUE TARGETS 11CHROMOPHORES AND SELECTIVE PHOTOTHERMOLYSIS 11LASER & INTENSE LIGHT SOURCE OUTPUT SPECTRUM 12HEATING EFFECTS AND THE THERMAL RELAXATION TIME (TRT) 12SPOT SIZE ON TISSUE 13
THERAPEUTIC TISSUE EFFECT 14
PHOTOTHERMAL EFFECT 14PHOTOABLATIVE EFFECT 15PHOTOACOUSTIC (ELECTROMECHANICAL) EFFECTS 15PHOTOCHEMICAL EFFECTS 16PHOTO DYNAMIC THERAPY (PDT) 16PHOTOBIOMODULATION (PBM) 18POPULAR COSMETIC LASER AND INTENSE LIGHT SOURCE TREATMENTS 21HAIR REMOVAL WITH IPL DEVICES AND LASERS 21SKIN PHOTO-REJUVENATION 22Ablative Skin Resurfacing (ASR) 23Fractional Photothermolysis (FP) 24Fractional Photothermolysis (FP) 25Non-ablative dermal remodelling (NDR) 25TATTOO REMOVAL 26PIGMENTED LESION TREATMENTS 28VASCULAR LESION TREATMENTS 31ACNE 32OTHER COSMETIC TREATMENTS 34LASER SURGERY IN DISEASE, DISORDER AND INJURY 35OBGYN 35ENT 35ORTHOPAEDICS 36OPHTHALMIC LASERS 36TREATMENT-RELATED SIDE EFFECTS 37SIDE EFFECTS AND COMPLICATIONS IN COSMETIC TREATMENTS 37PARADOXICAL HAIR GROWTH 38FINDING THE THERAPEUTIC WINDOW FOR SUCCESSFUL OUTCOMES 39

Laser and IPL Physics and Safety ‘Core of Knowledge’ – Laser/IPL light generation & characteristics (Unit 1)
Page 4 of 40 Copyright 2020 Online Laser Training Ltd. Updated: July 2020 UK 3
About the authorsCourse Director Dr Godfrey Town Ph.D.Dr Town Ph.D. is a UK registered clinical technologist and scientist specialising in the comparative measurementof IPL and laser devices. He is a regular invited speaker at international aesthetic laser meetings and haspublished scientific and clinical papers in international peer-reviewed journals on the use of laser and intensepulsed light (IPL) devices.
For five years, he was an owner-manager of a successful UK private laser & IPL clinic in the UK. As an RPA2000Certificated Laser Protection Adviser (LPA), his LPA consultancy has supported over 300 private medical and dentalpractices, clinics, salons and spas using more than 350 laser and IPL devices for whom he has also providedapplications and accredited ‘Core of Knowledge’ training, clinical protocol, regulatory and safety proceduresupport.
He has authored over twenty-five peer-reviewed studies and journal articles on laser and IPL use and writtencomprehensive laser hair removal and skin rejuvenation training manuals and book chapters and has directlyassisted in the staff training and commissioning of numerous laser skin care clinics.
He is engaged with national and international agencies in order to identify, design and formulate necessaryregulations and standards for lasers and light-based devices. His area of work as an Expert Witness embracescosmetic laser injuries, negligence in laser surgery and laser accidents.
Dr Town’s Professional Affiliations include: Senior Research Fellow, Ph.D., Department of Dermatology, Aalborg University
Hospital, Aalborg, Denmarksince 2019
ANSI SSC-3 Laser safety standards sub-committee since 2014 Cardiff University Bond Solon Expert Witness Certificate holder since 2013 Committee Member: EPL/076 Optical radiation safety and laser equipment;
IEC TC/76 WG4 Safety of medical laser equipment; CPL/61/1 ‘Liaison Expert EPL/76’Safety of household and similar electrical appliances; and IEC TC61 WG30 Beautytherapy appliances for household and commercial use
since 2010
Fellow of American Society for Laser Medicine and Surgery (ASLMS) since 2003 Member of British Medical Laser Association (BMLA) since 2002 Registered Clinical Technologist (RCT-IPEM) since 2002 Member of European Society for Laser Dermatology (ESLD) since 2001
A full C.V. and comprehensive bibliography is available at: www.godfreytown.com
Patricia Owens RN, BSN, MHA, CMLSO, CNOR, Course Co-AuthorPatti Owens provides consultation services in aesthetic and medical safety programs and in-officemanagement services for a variety of laser companies and professional organizations. Patti is an activemember on the ANSI Z136.3 committee where she has been appointed as the acting secretary for thepast 3 years.
Patti has published numerous articles in the field of laser surgery and aesthetics. Her co-authored bookwith Pamela Hill, Milady’s Aesthetician Series, Laser and Light Therapy, was published in 2009 by CengageLearning.
A full C.V. and comprehensive biography is available at www.aestheticmedconsulting.com

Laser and IPL Physics and Safety ‘Core of Knowledge’ – Laser/IPL light generation & characteristics (Unit 1)
Page 5 of 40 Copyright 2020 Online Laser Training Ltd. Updated: July 2020 UK 3
IntroductionCourse Overview
Laser and IPL Physics and Safety ‘Core of Knowledge’ is a collaboration of the current evidencebased and consensus based practices listed in the CENELEC Technical Report CLC/TR 50448:2005: ‘Guide to levels of competence required in laser safety’ [1], International ElectricalTechnical Commission Technical Report IEC/TR 60825-8:2006 Edition 2: ‘Safety of laserproducts: Guidelines for the safe use of laser beams on humans’ [2], MHRA document ‘Lasers,intense light source systems and LEDs - Guidance for Safe Use in medical, surgical, dental andaesthetic practices’ September 2015 [3], Essential Standards Regarding Class 3B and Class 4Lasers and Intense Light Sources in Non-surgical Applications October 2016 – published by theBritish Medical Laser Association [4] and the recommended practices published in the‘American National Standard for Safe Use of Lasers in Health Care Z136.3 2011 edition’ [5]
This e-learning course is designed to provide approximately 30 hours of training at Level 4 fortherapists and healthcare professionals intending to provide laser and/or intense pulsed lightservices in registered establishments. It is worth 30 CPD credits (awarded by The CPD Group)for completion of the course. In addition, it is designed to provide Laser Safety Supervisors /Laser Safety Officers and IPL Safety Supervisors with the necessary laser and IPL physics andsafety training to enable them to carry out the duties required of them under currentlegislation.
The Core of Knowledge contained in this course includes that recommended in the MHRAdocument Lasers, intense light source systems and LEDs - Guidance for Safe Use in medical,surgical, dental and aesthetic practices September 2015[3].
Participants are also encouraged to read the Reference Guide to Consent for Examination orTreatment (second edition) and Information to Assist in Amending Consent Forms published bythe UK Department of Health at:http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_103643
Laser & IPL Safety Training
With the rapidly increasing popularity of intense pulsed light sources and the inclusion of thesedevices in current legislation covering licensed establishments, this course has been expandedbeyond the content of the UK MHRA document to provide appropriate, relevant and necessaryinformation to support users in the safe operation of these non-laser intense light systems.
Benefits Achievements & Feedback
The attendee will benefit from the course by being better informed about the safe use of lasersand intense pulsed light devices in their delivery of patient/client-centred care. Participantscompleting this course will meet the requirements of the recommended BMLA EssentialStandards in respect of adequate training as a Laser Protection Supervisor (LPS) [4].

Laser and IPL Physics and Safety ‘Core of Knowledge’ – Laser/IPL light generation & characteristics (Unit 1)
Page 6 of 40 Copyright 2020 Online Laser Training Ltd. Updated: July 2020 UK 3
The achievements of the learner will be assessed through completion of Multiple-ChoiceQuestionnaires (MCQs) at the end of each Unit of learning to qualify for nationally recognisedCPD credits.
Feedback on the content, quality of presentation, level of course fees and suggestions forimprovements will be recorded on the Feedback Form at the end of the course and analysedfor reference in improving subsequent courses.
Financial Interest: This course is run on a ‘for-profit’ basis.
Correspondence please contact: Dr Godfrey Town: [email protected]
Training Faculty
Dr Godfrey Town PhD, RPA2000 Certificated Laser Protection Adviser
Patti Owens RN, BSN, MHA, CMLSO, CNOR, Co-Author
Anita Clarkson, Beauty Therapist Trainer
Basics Physics and Safety Core of Knowledge Training includes the following topics:
Unit 1: Laser/intense light generation and characteristicsUnit 2: Hazards and risks from equipment and laser/IPL beamsUnit 3: Laser & Intense Light Source radiation - tissue InteractionUnit 4: Relevant legislation and safety standards
Disclaimer
Online Laser Training Ltd provides information for educational purposes only; it is not intended toprovide medical or legal advice or for any of its’ users. The information provided in this e-learning is nota guarantee of compliance with regional or national regulations and non-regulatory controls.
Aesthetic practice and regulatory information may change quickly, and information contained shouldnot be relied on as the benchmark document pertaining to all laser and IPL devices and all aestheticprocedures. It is mandatory that the Laser Safety Officer and Laser User review the manufacturer’sprocedure manual concerning each laser device along with receiving the appropriate education andhands-on training before attempting to treat an aesthetic patient. Policies and procedures willconcurrently need to be established along with a viable laser and IPL safety programme. You agree thatby using this resource that the limitations of liability set out in this disclaimer are reasonable and willprotect and indemnify Online Laser Training Ltd and its officers, employees, agents, successors andassigns.
Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 7 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
COURSE OBJECTIVES:UNIT 3 TITLE: Understand Laser & Intense Light Source Radiation -Tissue Interaction
LEARNING OUTCOMES ASSESSMENT CRITERIAAt the end of this Unit, the learner should be able to:1. Explain what happens to the eye, skin and other body tissue when exposed to IPL/laser.
1.1 Describe what “Photothermal” means.1.2 Explain “Thermal Relaxation Time (TRT)”.1.3 Describe why TRT is important.1.4 Explain how tissue interaction takes place in tattoo removal.1.5 Explain the terms “ablative” and “non-ablative” in relation to fractional laser1.6 Explain the advantages of fractional non-ablative laser treatment over ablative treatment1.7 Describe one example of photochemical tissue interaction.
2. Explain suitability of wavelengths and pulse structures.2.1 Explain which wavelengths are best for hair removal.2.2 Explain which wavelengths are best for vascular treatments.2.3 Explain which wavelengths are best for pigmentation treatments.2.4 Explain which wavelengths stimulate porphyrin and affect Acne Vulgaris.2.5 Explain the relationship between pulse duration and size of tissue target.2.6 Explain which wavelengths and pulse durations are best for surgical incision / ablation.
3. Explain tissue targets (chromophores, penetration depth, etc.).3.1 Name the 3 main chromophores in skin.3.2 Describe which optical wavelengths penetrate tissue most deeply.3.3 Describe the main chromophores in surgical incision / ablation.
4. Describe laser & intense light source output spectrum and relevance of beam size andshape.
4.1 Identify the typical output spectrum (wavelength range) of an IPL.4.2 Identify the typical output spectrum (wavelength range) of an LED4.3 Describe two advantages of a large spot size laser or IPL.4.4 Explain the benefit of a small spot size laser.
5. Explain common laser and intense light source treatments.5.1 Give an explanation of hair growth delay caused by laser and IPL.5.2 Explain how light-based stimulation of hair growth is believed to work.5.3 Describe how laser/IPL is used to remove pigmented blemishes.5.4 Describe how laser/IPL is used to remove vascular blemishes.5.5 Explain the likely mechanisms of acne reduction using laser/IPL.5.6 Explain how Lasers can reduce fine lines and wrinkles.
6. Understand the principal laser/IPL-related potential adverse effects on eye and skin.6.1 Identify the 3 parts of the eye most at risk from laser/IPL exposure6.2 Describe the most common treatment-related side effect on skin.6.3 Identify five other adverse effects on skin from laser/IPL exposure.

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 8 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Laser & Intense Light Source Radiation - Tissue InteractionKnowledge of light interaction with tissue provides an explanation for observed therapeuticefficacy and treatment related side effects learned in the surgical and dermatologic findingsof scientific and clinical research. The first section of this review of tissue effects focuses onestablished theories and provides a basic understanding of light-tissue interaction. Thissection will also concentrate on its implications for light-based therapy with an emphasis onphoto-thermal, photo-acoustic, photo-ablative and photo-biomodulation or photo-chemicaleffects.
To understand the biological effect of light penetration or transfer of optical radiation withinskin, its location and the absorption depth into the tissue is strongly dependent on thewavelength of the light. The mechanisms by which optical radiation induces tissue damageare similar for all biological systems and may involve photo-thermal, photo-chemical,electro-mechanical and photo-ablative processes. Photo-thermal - heats the target Photo-acoustic (electro-mechanical) - shatters the target Photo-chemical - chemically alters the target Photo-ablative - explosively removes the target
Interactions of Light with TissueThere are 4 distinct characteristics of optical light as the energy comes in contact with theskin.
Figure 1: Diagrammatic representation of incident radiation on human skin illustrating regular reflectance atthe surface, forward scattering, absorption, and transmission. (Illustration courtesy of T. Igarashi, ColumbiaState University, USA)

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 9 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Tissues are certainly not ideal optical media. They are not homogeneous and the skin, fattytissues, muscle, cartilage, nerves and blood-filled capillaries all contribute to the laser andlight characteristics. In the human skin, depending on the wavelength, a laser beam canreflect, scatter, absorb and/or transmit into the epidermal and dermal skin layers [Figure 1].
Reflection occurs when the laser comes in contact with a curved or shiny flat surface, suchas instrument, mirrors and jewellery. Since the stratum corneum of the epidermis iscomposed of flat shiny skin cells, a reflection of around 3% can occur.
Scattering of light off of skin structures is a physical phenomenon influencing lightpropagation in biological tissue. Forward scattering involves the interaction of light as itbounces off of the epidermal and dermal structures. Depending on the wavelength, thescattering of the energy can be changed by the amount of melanin in the skin. With shortervisible wavelengths, the scattering is higher with less tissue penetration. At the longerwavelengths (red and near infra-red) where the light is absorbed less by melanin, there isdecreased optical scatter and the beam is more penetrating into the skin. Therefore, thegreater the scattering, the less depth of penetration due to more absorption.
Due to limited melanin absorption of the Nd:YAG laser (1064 nm), there is up to 30%backscatter towards the user, the highest amongst popular visible and near infra-red lasers.With the CO2 and Erbium YAG lasers, there is limited forward scatter, and no backscatterdue to its energy being absorbed within the intracellular water in the epidermis.
The transmission of light through tissue is the ability to pass through tissue until the laserradiant energy comes in contact with its target chromophore. Transmission of light is used inhealthcare to measure vital sign parameters such as blood oxygenation content in vivo anddrug concentration levels. For increasing photon energy density, the biophysical effect ofphoton interactions increases from photochemical (wavelength dependent) to photothermal(heat dependent) to photomechanical (ablation).
Anderson and Parrish described light incident on the surface of the skin as always partiallyreflected with 4-7% of the photon light energy from 250 nm - 3000 nm directly reflectedirrespective of skin colour. The remaining 93–96% of energy is transmitted into the skin. Thistransmitted energy is absorbed or scattered, determined by the absorption and thescattering coefficients or re-emitted back into the environment. When wavelengths of lightare absorbed by a specific component of the skin, there will be a precise biological effect[Figure 2].
Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 10 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
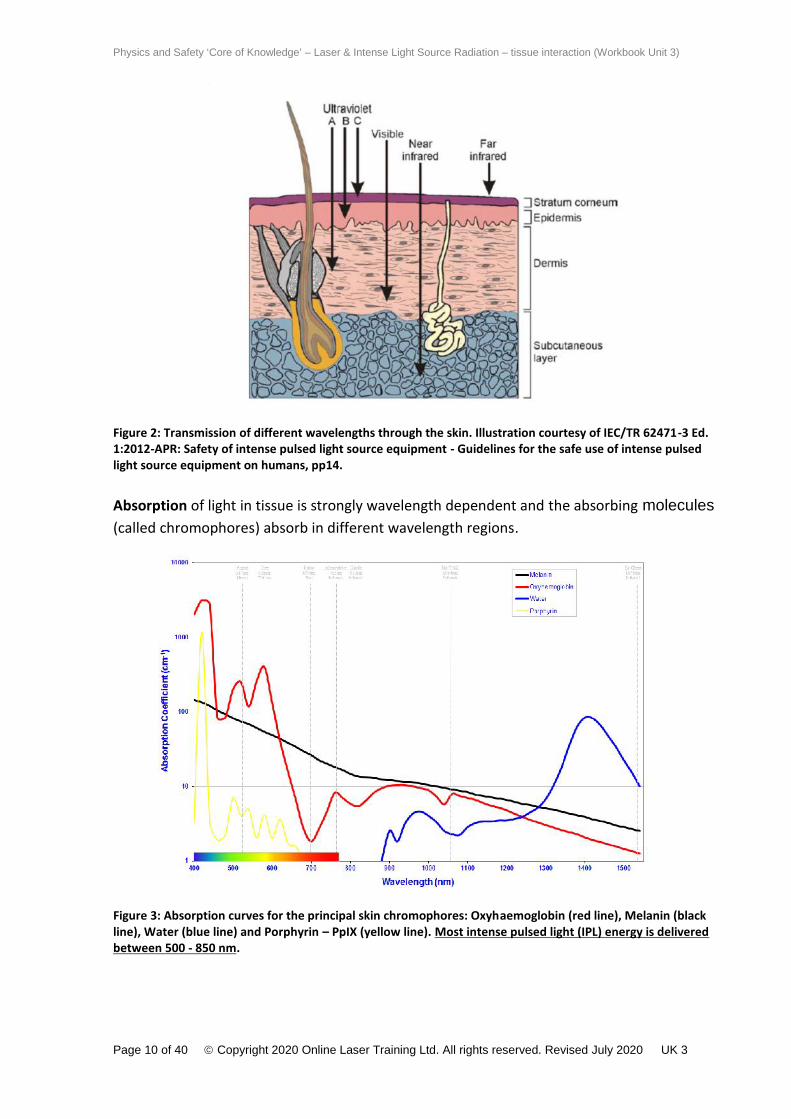
Figure 2: Transmission of different wavelengths through the skin. Illustration courtesy of IEC/TR 62471-3 Ed.1:2012-APR: Safety of intense pulsed light source equipment - Guidelines for the safe use of intense pulsedlight source equipment on humans, pp14.
Absorption of light in tissue is strongly wavelength dependent and the absorbing molecules(called chromophores) absorb in different wavelength regions.
Figure 3: Absorption curves for the principal skin chromophores: Oxyhaemoglobin (red line), Melanin (blackline), Water (blue line) and Porphyrin – PpIX (yellow line). Most intense pulsed light (IPL) energy is deliveredbetween 500 - 850 nm.

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 11 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
In order for light to produce any biological effect in skin it must first be absorbed, by a targetchromophore, where transformation through photoexcitation of radiant optical energy intoa different form of energy (usually heat) occurs by specific interaction with tissue.Chromophores are light-absorbing substances with the most common being haemoglobin,water, and melanin within tissue. Resonance between the energy of the photons scatteringin tissue and molecules in their path, may lead to the photon causing an excited energy statein the absorbing molecule. The absorbed energy is most frequently converted into heat butcan also be re-emitted from the tissue as fluorescence or be utilised for a photochemicalreaction [Figure 3].
Tissue Targets
Chromophores and Selective Photothermolysis
Anderson and Parrish proposed the concept of photothermolysis and selectivechromophore excitation as the mechanism for vascular and pigmented lesion treatment andreduction. This concept plays a significant role when explaining the difference betweentreatment using intense pulsed light devices and the single wavelength laser. A substancethat absorbs light is called a chromophore - so what are these chromophores and where arethey located?
The major relevant skin chromophores are: Melanin: the pigment generated by epidermal melanocytes (also found in hair). Haemoglobin: the red pigment in blood and other tissue. Keratin: the desiccated protein that comprises the outer skin layers and hair. It also
comprises the warty bulk of keratoses and calluses. Porphyrins: Naturally occurring protoporphyrin IX (PPIX) can act as a photosensitive toxin
under certain conditions. Water: present in large quantities in most of the cells of our body
These absorb different wavelengths to varying degrees [Figure 3 & 4].
Melanin has clear absorption characteristic in the visible spectrum. At the shorterwavelengths, melanin absorption increases. For maximum penetration in tissue withminimal absorption in darker epidermal melanin, near infrared wavelengths above 800 nmare more effective.
Haemoglobin on the other hand has a more distinctive absorption characteristic and hasabsorption peaks at about 534 nm and 578 nm. Using a monochromatic laser has theadvantage of most of the light being able to pass through the melanin but be stronglyabsorbed by the haemoglobin chromophore. Thus, dilated capillaries and telangiectasias canbe selectively coagulated in a single treatment. As most of the energy in the typical filteredIPL spectrum is between 500 and 850 nm, IPL is suitable to treat both vascular andpigmented lesions in addition to hair removal [Figure 4].

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 12 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Laser & Intense Light Source Output Spectrum
Figure 4: Absorption spectrum for oxyhaemoglobin (red), Melanin (black), water (blue), porphyrin (yellow)vs. typical cutaneous laser and IPL wavelengths.
The greatest range of light tissue interaction in cutaneous light therapy takes place between400 nm and 1200 nm as shown by the absorption curves for melanin, blood, water andporphyrin in Figure 4. Most intense pulsed light (IPL) energy is delivered between 500 -850nm.
Heating Effects and the Thermal Relaxation Time (TRT)
Tissue damage from thermal effects is also related to the duration of the optical radiationexposure (pulse width) and the temperature reached in the tissue. If the optical radiationexposure to the tissue is for a short duration (less than 1 second) the tissue will suffer alesser degree of damage, than if longer exposure time is used. Lasers and intense pulsedlight sources typically utilise photothermal or heat damaging skin interactions to obtain theirclinical outcomes [Figure 5].
Figure 5: For increasing photon energy density, the biophysical effects of photon interactions increase fromphotochemical (wavelength dependent) to photothermal to photomechanical (ablation).

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 13 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Energy is conducted to surrounding tissues – but this depends on how conductive the tissuesare. The effect is minimized if laser pulses are shorter than the relaxation time. ThermalRelaxation Time (TRT) is the time it takes for approx. 50% of the heat absorbed by a body tobe lost. So, laser/IPL theories indicate choosing pulse times to match or are less than TRT inorder to optimise damage to target tissue while minimising damage to surrounding tissue.
Spot size on tissueIn the case of lasers and IPL equipment, the size and spatial uniformity of the delivery areaof light at the surface of the skin will also influence the successful penetration of sufficientoptical energy to damage the chosen target (Figure 6). A lens positioned on a handpiece ofan infrared ablative laser, e.g. CO2 and Erbium:YAG laser, focuses a laser beam to a suitablespot size for the intended application. A lens can also be utilized internally within the laserhousing in order to focus the laser energy at the beam aperture to the internal diameter of alaser fibre. A large spot size will also allow more rapid area coverage, a useful feature whentreating large skin areas (e.g. hair removal on backs, chests and legs). Large spot size alsomaintains greater efficacy at a deeper penetration.
Figure 6: Light penetration depth is influenced by the size and uniformity of the delivery area of light at thesurface of the skin.Diagram adapted from: Illumination Geometry: The Importance of Laser Beam Spatial Characteristics, 2001,Kurt G. Klavuhn, PhD 2000; (Private Communication).
Conversely, a laser beam can be focused to a tiny spot size on tissue at very high energy,making it the ideal tool for laser microsurgery (e.g. neurosurgery). Depending on thewavelength selected, the cutting laser may also have the ability to coagulate bleeding tissue(e.g. CO2 laser vs. Er:YAG).
Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 14 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Therapeutic Tissue Effect
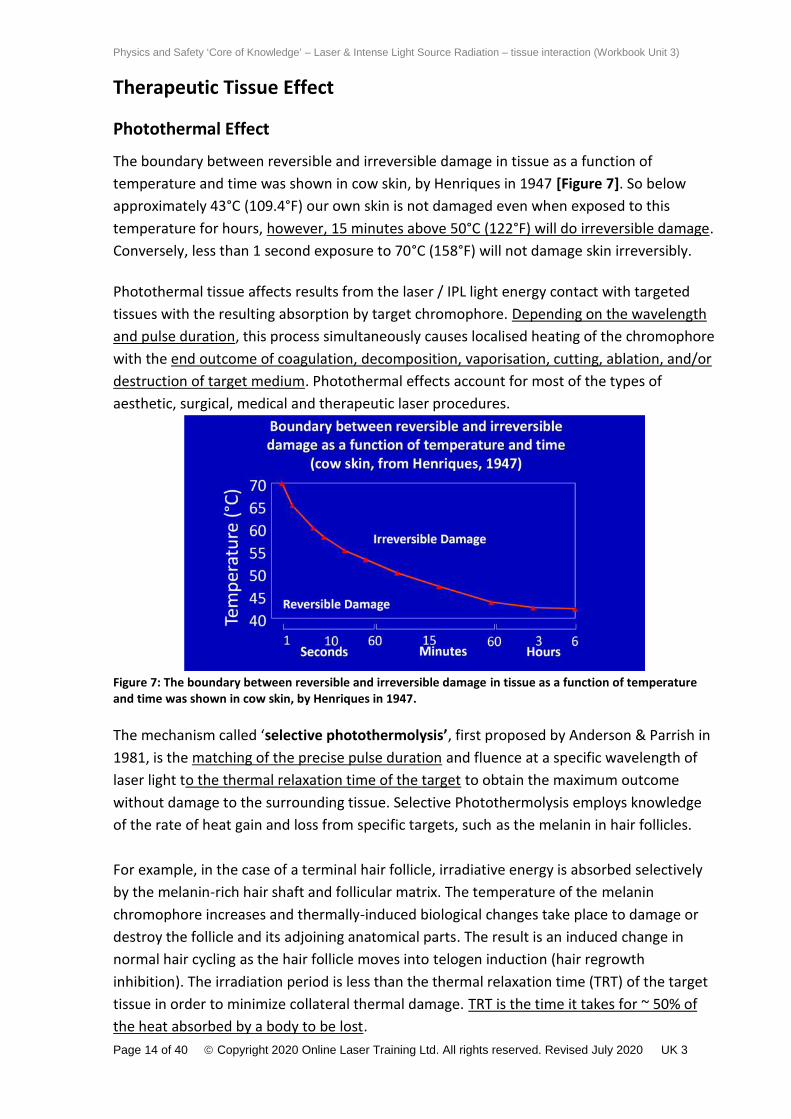
Photothermal EffectThe boundary between reversible and irreversible damage in tissue as a function oftemperature and time was shown in cow skin, by Henriques in 1947 [Figure 7]. So belowapproximately 43°C (109.4°F) our own skin is not damaged even when exposed to thistemperature for hours, however, 15 minutes above 50°C (122°F) will do irreversible damage.Conversely, less than 1 second exposure to 70°C (158°F) will not damage skin irreversibly.
Photothermal tissue affects results from the laser / IPL light energy contact with targetedtissues with the resulting absorption by target chromophore. Depending on the wavelengthand pulse duration, this process simultaneously causes localised heating of the chromophorewith the end outcome of coagulation, decomposition, vaporisation, cutting, ablation, and/ordestruction of target medium. Photothermal effects account for most of the types ofaesthetic, surgical, medical and therapeutic laser procedures.
Figure 7: The boundary between reversible and irreversible damage in tissue as a function of temperatureand time was shown in cow skin, by Henriques in 1947.
The mechanism called ‘selective photothermolysis’, first proposed by Anderson & Parrish in1981, is the matching of the precise pulse duration and fluence at a specific wavelength oflaser light to the thermal relaxation time of the target to obtain the maximum outcomewithout damage to the surrounding tissue. Selective Photothermolysis employs knowledgeof the rate of heat gain and loss from specific targets, such as the melanin in hair follicles.
For example, in the case of a terminal hair follicle, irradiative energy is absorbed selectivelyby the melanin-rich hair shaft and follicular matrix. The temperature of the melaninchromophore increases and thermally-induced biological changes take place to damage ordestroy the follicle and its adjoining anatomical parts. The result is an induced change innormal hair cycling as the hair follicle moves into telogen induction (hair regrowthinhibition). The irradiation period is less than the thermal relaxation time (TRT) of the targettissue in order to minimize collateral thermal damage. TRT is the time it takes for ~ 50% ofthe heat absorbed by a body to be lost.

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 15 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
The forward dominant penetration depth of optical light radiation in human tissue increasesas the wavelength gets longer from ultraviolet to near infrared. Therefore, it is important notonly to match the TRT of the target to the pulse duration of the radiant emission but also toselect a wavelength that will reach the target in the tissue. For example, adult terminal hairfollicles and their vital adnexa may extend deep into the subcutaneous layer. Blue light,which is very well absorbed by the target melanin in the hair shaft and bulb, is unable toreach sufficiently deeply into the skin to achieve adequate absorption to thermally disablethe target hair follicle.
Photoablative EffectPhotoablative is defined as a pure destruction of tissue without any thermal effects ortrauma. The high peak power of very short Ultraviolet (UV) wavelengths (190 nm to 308 nm)causes strong electronic bond breaking within the targeted tissue. When the molecularbonds are broken, the tissue components are superficially vaporised, and heat is carriedaway. The Excimer laser can cleanly ablate to several microns deep without any thermaltissue effects. Excimer lasers are used primarily in Ophthalmology for the LASIK procedureon the eyes for corneal reshaping for corrective vision.
Photoacoustic (Electromechanical) EffectsWhen tissue is exposed to extremely short pulses of optical light radiation i.e. in thenanosecond (ns) domain, tissue targets heat up extremely rapidly. This phenomenon causesdielectric breakdown of tissue leading to rapid thermal expansion from focused areas ofplasma. The propagation of this plasma causes tissue vibrations with resulting thermo-acoustic shock waves and resulting fragmentation. Q-switching, is a technique by which alaser wavelength can be made to produce high frequency pulsed lasers outputs. Thetechnique allows the production of rapid light pulses of standard laser wavelengths at thespeed of a nanosecond (billionth of a second), picosecond (trillionth of a second), andfemtosecond (quadrillionth of a second). These pulses possess extremely high (gigawatt)peak power, much higher than would be produced by the same laser if it were operating in acontinuous wave (constant output) mode.
Such very short pulse photo-disruption is commonly used to shatter tattoo ink particles toallow the macrophages of the body to clear unwanted tattoo ink from skin areas through thelymphatic system. Photo-disruption is also employed to break open clouded secondaryposterior capsules after ophthalmic cataract surgery. Urologic specialties also utilize thiselectromechanical disruption to breakdown stones in the bladder, ureters, kidneys andbiliary stones in a procedure known as laser lithotripsy.

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 16 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Photochemical effects
Photo Dynamic Therapy (PDT)
As far back as the Western Zhou Dynasty in China (771 BC) the combination of sunlight andplant extracts appears in writings for the purpose of causing photochemical reactions totreat conditions such as re-pigmentation of vitiligo-like lesions (white patches of non-pigmented skin).
In recent years, the study of the rates and mechanisms of chemical processes in thepresence of light and the factors on which they depend (photokinetics) has led to a dramaticadvancement in the knowledge and understanding of photodynamic therapy (PDT). PDTinvolves cellular photo-chemical changes caused by light therapy in combination with aphotosensitizing medication (or herbal remedy) which either stimulates or retards a process.
The 3 steps in PDT are: Photosensitizing drug located in the target tissues Activation of the drug, laser, LED, IPL or even normal daylight Biological effects
PDT achieves its effectiveness in skin cancer treatments by exploiting the relatively selectiveuptake by abnormally growing cells. A topically applied photosensitising agent can then beactivated by low power laser or intense visible light source of suitable wavelength. Theresulting photodynamic reaction involves the production of reactive oxygen species, inparticular singlet oxygen, leading to cell death [Figure 12].
Figure 12: Laser radiation being delivered, via a fibre, for photodynamic therapy to treat cancer.Public Domain, https://commons.wikimedia.org/w/index.php?curid=3097611

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 17 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Following PDT treatments, the skin remains hypersensitive to light until the photosensitizingdrug has “washed-out” of the body’s system. Some herbal remedies, such as St. John’s Wort(hypericum) can also make the skin sensitive to some visible and near infrared wavelengths.Most reported drug photosensitivity relates to UV sensitivity, outside the normal range ofsurgical and cosmetic lasers and IPLs.
PDT is a systemic treatment which has multiple indications. In oncology, specialists can treatpremalignant and early-stage cancer and reduce the tumour size in end-stage cancers.Photosensitizing agents, such as Photofrin® (porfimer sodium) medication, is administeredintravenously and subsequently absorbed preferentially by cancer cells. During surgery, alaser beam of suitable wavelength to activate the photosensitizer is positioned at thetumour site via a fibre or with direct fluorescence. Activation of the Photofrin® drugproduces the singlet oxygen which results in cancer cell death.
PDT also has proven ability to kill microbial cells, including bacteria, fungi and viruses. It isused topically in photo-disinfection in endodontics to ‘sterilize’ root canals, disinfect cavitiesin restorative dentistry and disinfect periodontal areas.
PDT can also be used effectively to treat Actinic Keratosis (AKs) in which up to 10% candevelop into squamous cell carcinomas. The photosensitisers that can be used for topicalPDT in skin cancer treatment are either 5-aminolevulinic acid (ALA) or its methyl ester (MAL).They are applied to the skin covering the area to be treated and incubated to allowadequate penetration of the drug. Both ALA and MAL are approved in several countries forthe treatment of AKs, and in some countries for the treatment of Bowen’s disease and BasalCell Carcinoma (BCC).
Figure 13: Left - High intensity blue light (425 nm) used for the professional treatment of acne.
Another example of photochemical effect in dermatology is the absorption of light bynatural or artificial porphyrin produced in association with acne vulgaris. Exposure of acne tointense blue light alone (either professional or home-use) may be used to treat acne throughthe release of singlet oxygen species to kill the acne bacteria [Figure 13].

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 18 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
PDT in acne treatment uses the excitation of ProtoPorphyrin IX (PpIX), which has a largeabsorption peak at around 400 nm, with several smaller peaks at 508 nm, 542 nm, 577 nmand 635 nm. Topical PDT photosensitizer medication targets the infection of the sebaceousunit resulting in enhanced release of singlet oxygen and the destruction of the anaerobic p.acnes bacteria [Figure 14].
Figure 14: Left - Typical UV-Visible absorption spectrum of PpIX. The Soret Band represents the highest peakof absorption by porphyrins (415 nm) and thus photosensitizer activation but has the shallowest penetrationin turbid tissue. The several weaker peaks of porphyrin absorption in the Q-Band (508 nm, 542 nm, 577 nmand 635 nm) however penetrate tissue more deeply. Right - Right – Daylight PDT delivered in NorthernEurope in a heated glass conservatory.
Most recently, powerful diode arrays and ‘daylight PDT’ (where the patient sits ‘outside’ innormal daylight to expose the PDT-treated lesion(s) have opened up the market forcutaneous photodynamic therapy (PDT) in the treatment of basal cell carcinoma, actinickeratosis, Bowen’s disease and acne.
The use of ‘daylight PDT’ requires a minimum of ~2000 lux light exposure for at least 3 hoursand the skin temperature has to be elevated to around 30 degrees Celsius during theirradiation. If lower, the metabolism of the cells will decrease, and not enoughphotosensitizer will be converted into the active protoporphyrin 9. In Northern Europe thisusually requires seating patients comfortably in a heated greenhouse or glass conservatory![Figure 14]
Any device producing wavelengths absorbing at peaks in the Soret Band and Q-Band mayshow potential for treatments ranging from active acne, skin rejuvenation and even Rosacea.
Photobiomodulation (PBM)
Photobiomodulation is an emerging veterinary and medical technique which relies upon the‘a-thermal’ effect (i.e. temperatures less than 37 degrees Celsius) first noticed by surgeonsusing lasers in the 1970s and 1980s, where, in addition to thermal damage to tissue, at theoutermost edges of the laser incisions, tissue healed particularly rapidly. This ‘a-thermal’effect was believed to stimulate the activity of the subcellular components of cells in thisoutermost or ‘ PBM’ zone. Thus, a distinction began to emerge between the ‘photothermal’

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 19 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
effect caused by powerful surgical lasers and intense pulsed light (IPL) systems used tocoagulate or vaporise tissue, and ‘photo-therapeutic’ effect achieved at low photondensities. At first referred to as Low Level Laser (Light) Therapy (LLLT) it is now called‘photobiomodulation’ or ‘PBM’.
The light-emitting diode (LED) was invented in 1962 but they were very unstable, highlydivergent and the output covered a wide band of wavelengths of up to 100 nm on eitherside of the graded wavelength. In the late 1990s high intensity, narrow-band red and blueLEDs including the 670 nm were developed, originally intended for self-use by servingmilitary personnel for temporary minor muscle and joint pain relief, arthritis and musclespasms. PBM has now been used for many years on sports injuries, arthritic joints,neuropathic pain syndromes, back and neck pain. Over 200 randomised clinical trials havebeen published on PBM, half of which are on pain.
In recent years, LEDs have become more stable, powerful and additional wavelengths, mostnotably around 415 nm, 633 nm and 830 nm have emerged onto the market. FDA marketingclearance in the USA and commercialisation of the photosensitizer, 5-ALA (5-Aminolevulinicacid) has opened up the market for LED arrays for cutaneous photodynamic therapy (PDT) inthe treatment of basal cell carcinoma, actinic keratosis, Bowen’s disease and acne as well ascosmetic applications such as skin rejuvenation and stimulation of hair growth in alopecia.
As can be seen in Figure 15, longer wavelength LEDs offer the benefit of deeper penetrationin tissue.
Figure 15: Photospectrogram of a human hand in vivo illustrating optical density and depth of penetration intissue. (Adapted from Smith KC, The Science of Photobiology 1977. Plenum Press, NY, USA).

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 20 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Several definitions of PBM have been attempted, including, ‘‘A form of light therapy thatutilizes non-ionizing forms of light sources, including lasers, LEDs, and broadband light, in thevisible and infrared spectrum. It is a non-thermal process involving endogenouschromophores eliciting photo-physical (i.e., linear and nonlinear) and photochemical eventsat various biological scales. This process results in beneficial therapeutic outcomes includingbut not limited to the alleviation of pain or inflammation, immunomodulation, andpromotion of wound healing and tissue regeneration.’’
Another definition describes the direct transfer of low incident levels of LED photon energyto enhance the level of the cellular energy pool. Damaged or compromised cells will berepaired, functional cells will do their job better and faster; cells will proliferate, or morecells will be recruited in clinical effects in wound healing, pain attenuation, boneregeneration, nerve regrowth, sports medicine, skin rejuvenation and hair regrowth.
Any device producing wavelengths absorbing at these peaks may show potential fortreatments ranging from active acne, skin rejuvenation and even Rosacea.
Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 21 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Popular Cosmetic Laser and Intense Light Source Treatments
Hair Removal with IPL Devices and Lasers
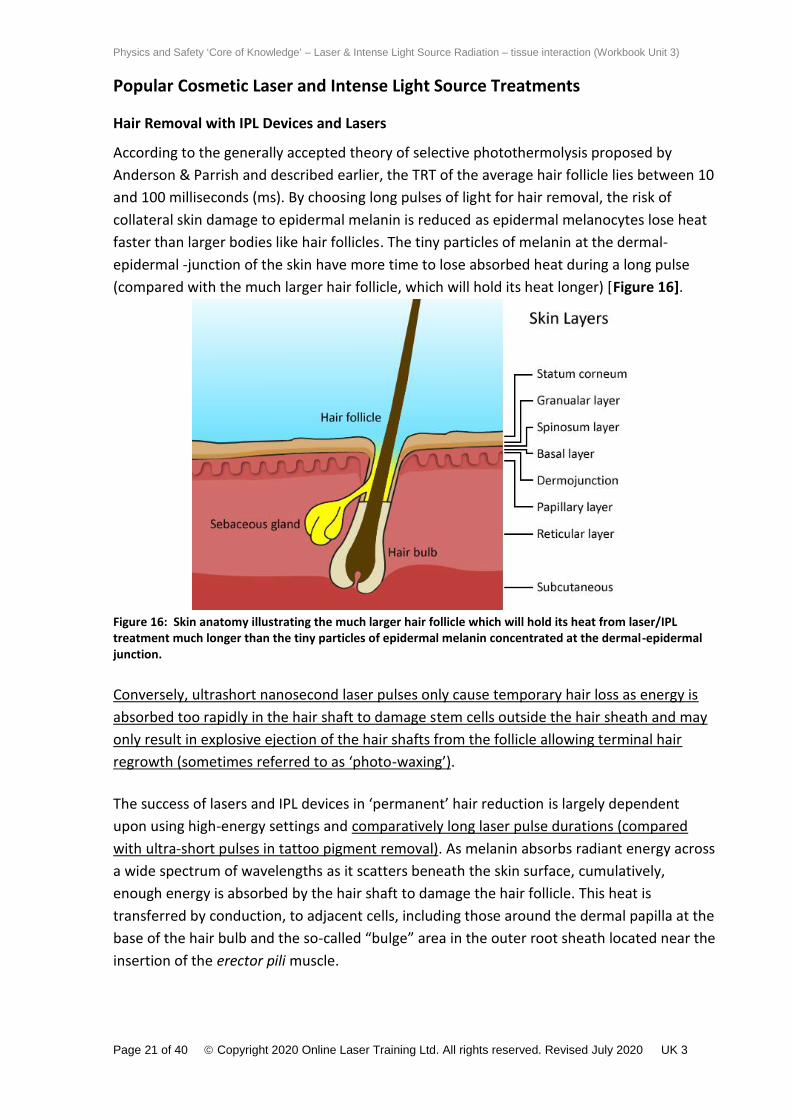
According to the generally accepted theory of selective photothermolysis proposed byAnderson & Parrish and described earlier, the TRT of the average hair follicle lies between 10and 100 milliseconds (ms). By choosing long pulses of light for hair removal, the risk ofcollateral skin damage to epidermal melanin is reduced as epidermal melanocytes lose heatfaster than larger bodies like hair follicles. The tiny particles of melanin at the dermal-epidermal -junction of the skin have more time to lose absorbed heat during a long pulse(compared with the much larger hair follicle, which will hold its heat longer) [Figure 16].
Figure 16: Skin anatomy illustrating the much larger hair follicle which will hold its heat from laser/IPLtreatment much longer than the tiny particles of epidermal melanin concentrated at the dermal-epidermaljunction.
Conversely, ultrashort nanosecond laser pulses only cause temporary hair loss as energy isabsorbed too rapidly in the hair shaft to damage stem cells outside the hair sheath and mayonly result in explosive ejection of the hair shafts from the follicle allowing terminal hairregrowth (sometimes referred to as ‘photo-waxing’).
The success of lasers and IPL devices in ‘permanent’ hair reduction is largely dependentupon using high-energy settings and comparatively long laser pulse durations (comparedwith ultra-short pulses in tattoo pigment removal). As melanin absorbs radiant energy acrossa wide spectrum of wavelengths as it scatters beneath the skin surface, cumulatively,enough energy is absorbed by the hair shaft to damage the hair follicle. This heat istransferred by conduction, to adjacent cells, including those around the dermal papilla at thebase of the hair bulb and the so-called “bulge” area in the outer root sheath located near theinsertion of the erector pili muscle.

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 22 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
This heat absorption causes the induction of catagen phase delaying hair regrowth. It hasbeen shown that, as some surrounding cells damaged by heat coagulation, the follicle ispermanently inhibited from producing further hairs [6].
The ‘best choice’ of light wavelengths by application is illustrated in Figure 17 placingoptimal wavelengths for photo-epilation between approximately 600 nm and 820 nm.Longer wavelengths absorbed by blood and tissue water may also collectively damage hairfollicle support structures, such as the blood supply to the hair bulb, aided by the overalltemperature rise in the adjacent tissue. The use of large spot sizes, together with a widerange of wavelengths, typically from 650-820 nm in Skin Types 1-4 and 1064 nm in SkinTypes 5-6, assists depth of light penetration into the underlying follicular bulb and itsadnexa.
Figure 17: Graph demonstrating the theoretical basis for the best wavelengths for hair removal (650-820 nm)and vascular (540-650 nm) and pigmented lesion (500-600 nm) treatments regarding chromophoreabsorption and light penetration depth.
As there is also melanin in the epidermis (giving the skin its natural colour), care must betaken to select appropriate energy levels according to skin type, to induce the desiredtherapeutic outcome without damaging epidermal melanin. Darker skin, darker, thicker hairand greater hair density require lower energy levels. Lighter skin, lighter thinner hair andlower hair density require higher energy levels. White or vellus hair is virtually unaffected bylight therapy treatment.
Skin Photo-Rejuvenation
Skin photo-rejuvenation is primarily directed at facial treatments and is usually classified aseither "Type 1" (reduction of pigmentation, telangiectasias and erythema) or "Type 2" (non-ablative wrinkle reduction). Laser and IPL devices have only been used to deliver non-invasive treatments since the year 2000. Near infrared lasers (950-2000 nm) demonstratingclinical success with non-ablative wrinkle reduction but with little or no “Type 1”rejuvenation effect. Radiofrequency devices have also been reported to have some clinicaleffects in reducing wrinkles but mostly in combination with infrared laser treatment.

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 23 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Laser and intense light source skin rejuvenation usually relies on absorption by high energymid-infrared wavelengths by water and other chromophores in the tissue including bloodvessels and melanin pigment but not fat or muscle.
Essentially, there are three methods of action used to achieve thermal remodelling: ablativeskin resurfacing, fractional photothermolysis and non-ablative dermal Figure 18.
Figure 18: Graphic representation of the 3 types of thermal remodelling of lines and wrinkles. Adapted from:Manstein D et al. Fractional Photothermolysis: A New Concept for Cutaneous Remodeling Using MicroscopicPatterns of Thermal Injury. Lasers Surg Med 2004; 34:426-438.
Ablative Skin Resurfacing (ASR)
Fully ablative surgical laser resurfacing, usually using CO2 or Er:YAG lasers with scanninghandpieces, permits rapid ablation of the entire epidermis down to the mid-reticular dermisto remove fine lines and wrinkles. The effects on the skin of full laser ablation include anablation crater and a zone of thermally necrosed tissue immediately beneath the ablationcrater, which is removed by the body through the inflammation process. Fully ablativeresurfacing results in punctate bleeding, an inherent level of pain requiring infiltration ortumescent anaesthesia and a need for significant post-operative wound care, involving aminimum of 2 weeks before the patient is able to leave the house [7] Figure 18.
The resultant improvements to photo-damage (including, reducing fine lines and mild tocoarse wrinkles, enlarged pores, skin texture and mottled pigmentation), develop overweeks and months following repeated treatments.
Any long-term tightening of the skin that does occur with ablative resurfacing is due to thehealing process and new collagen formation not to an instant shrinking of the old collagen[8].

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 24 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Figure 18: Erbium YAG laser ablative resurfacing of deep lines and wrinkles, pre- and 3 months posttreatment (Courtesy of Daniel Fleming MD)
Fractional ablative resurfacing, where micro-columns of thermally ablated zones (MTZs) oftissue are created allow the laser operator to reduce the depth of injury to the skin toreduce the side-effect profile. However, although patient down-time is reduced compared tofully ablative resurfacing, multiple fractional treatments may be needed to achieve asatisfactory aesthetic outcome for the patient (Figure 19 – Left).
Figure 19: Left - Fractional ablative resurfacing showing microthermal zones (MTZs) of epidermal damage.Right - Fractional non-ablative resurfacing – epidermis still intact (MENDs visible) [9]
Fractional Photothermolysis (FP)
Fractional photothermolysis employing low fluence laser energy, produces non-ablative,fractionated microscopic zones of dermal damage, without rupturing the epidermis.Overlying each dermal wound is a button-shaped area of necrotic debris, just below thestratum corneum. This debris (MEND – microscopic epidermal necrotic debris) seen inhistology corresponds to small brown spots on the skin surface (Figure 19 – Right).

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 25 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Fractional Photothermolysis (FP)
Fractional photothermolysis employing low fluence laser energy, produces non-ablative,fractionated microscopic zones of dermal damage, without rupturing the epidermis.Overlying each dermal wound is a button-shaped area of necrotic debris, just below thestratum corneum. This debris (MEND – microscopic epidermal necrotic debris) seen inhistology corresponds to small brown spots on the skin surface (Figure 19 – Right).
Non-ablative dermal remodelling (NDR)
Non-ablative dermal remodelling can be achieved with either the full beam width of a laseror IPL using low average irradiance. Comparing ablative and non-ablative skin rejuvenationtreatments, the main weakness of non-ablative techniques is that outcomes are not asdramatic as ablative techniques.
Figure 20: Pre- and post- non-ablative wrinkle reduction. (Courtesy of Christine Dierickx MD)
It is possible that there are numerous light-tissue interaction effects in the stimulation ofnew collagen including:
Low grade inflammatory mediator response following ‘insult’ of superficial micro-vasculature leading to increased type III pro-collagen production
Direct stimulation of the respiratory mitochondrial chain leading to increased type IIIpro-collagen production
Inflammatory mediators released from blood vessels into surrounding tissue(transient cyanosis) following light irradiation leading to increased type III pro-collagen production
Dermal collagen heating (usually under pre- and parallel-cooled epidermis) leading toa heat damage inflammatory response and collagen repair (usually high energylaser/IPL systems)
Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 26 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Collagen production response rates affected by the precise temporal form of the lightpulse (early evidence)
Erythema controlled by fractional distribution of laser energy using micro-lens arrays
As the precise mechanism of collagen stimulation achieved with low laser and IPL energy isunknown, it is difficult to develop a hypothesis for either an ideal pulse structure or energydensity. However, results can be impressive [10] Figure 20.
Light sources, including lasers, IPL and other ILS systems, reportedly have varying degrees ofefficacy in the improvement of photodamage and intrinsic aging (the appearance of skindiscoloration, skin texture, pore size, fine lines and wrinkles). Broadband ‘white’ pulsed light,as delivered by IPL systems, offers several potential advantages over monochromatic laserenergy. Its broadband wavelengths can target multiple chromophores simultaneously,including oxyhaemoglobin, melanin, water and protoporphyrin IX (PpIX).
With intrinsic aging, production of collagen in the skin decreases and existing collagen iseasily damaged by solar UV exposure. Skin loses its smoothness and fine lines and wrinklesbegin to appear as a result of the damage.
Tattoo Removal
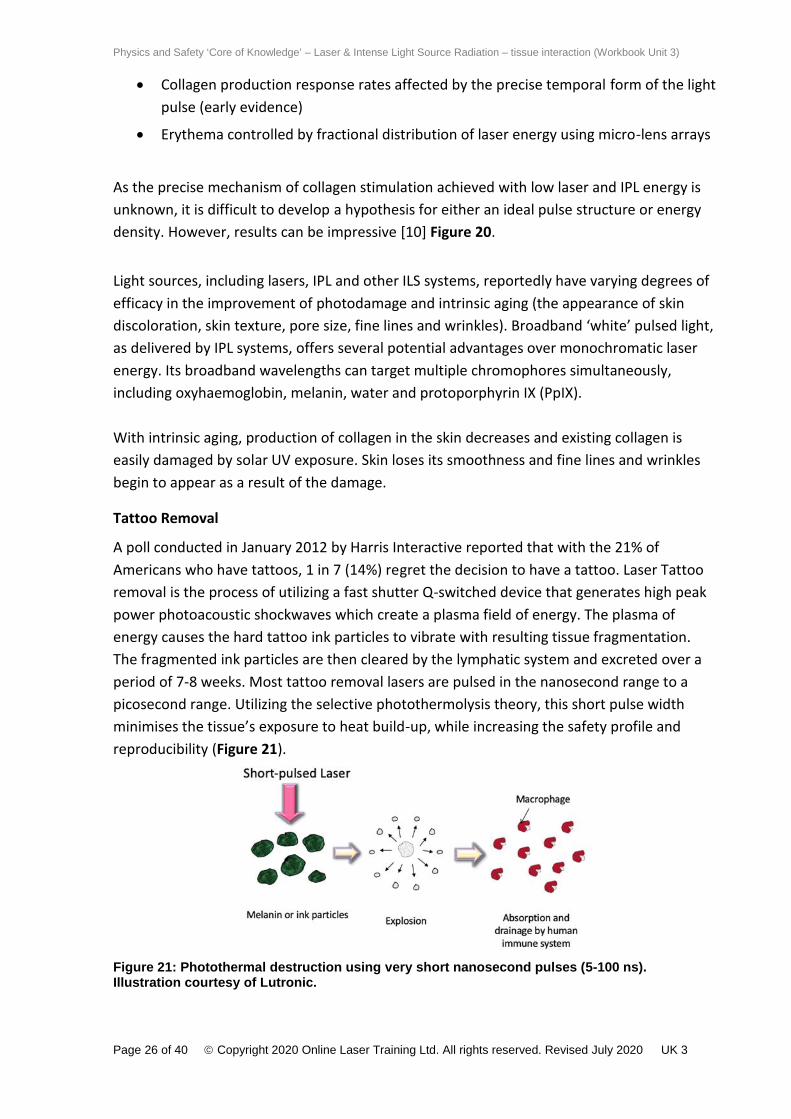
A poll conducted in January 2012 by Harris Interactive reported that with the 21% ofAmericans who have tattoos, 1 in 7 (14%) regret the decision to have a tattoo. Laser Tattooremoval is the process of utilizing a fast shutter Q-switched device that generates high peakpower photoacoustic shockwaves which create a plasma field of energy. The plasma ofenergy causes the hard tattoo ink particles to vibrate with resulting tissue fragmentation.The fragmented ink particles are then cleared by the lymphatic system and excreted over aperiod of 7-8 weeks. Most tattoo removal lasers are pulsed in the nanosecond range to apicosecond range. Utilizing the selective photothermolysis theory, this short pulse widthminimises the tissue’s exposure to heat build-up, while increasing the safety profile andreproducibility (Figure 21).
Figure 21: Photothermal destruction using very short nanosecond pulses (5-100 ns).Illustration courtesy of Lutronic.

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 27 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Factors that determine successful outcomes include: Wavelength of the laser Monochromaticity and pigment components of the ink Skin type Professional versus amateur tattoo
When attempting to remove tattoos, one needs to remember that colour is absorbed by theopposite colour. All tattoo inks have specific light absorption spectra in the electromagneticspectrum of radiation. Green tattoo ink needs to be treated with a Q-switched red 755 nmAlexandrite or Q-switched 864 nm Ruby laser. Red tattoo ink is highly absorbed by greenlaser light at 532 nm. Green 532 nm light is also very effective for lentigines and othermelanin based lesions. Darker skin types can be more difficult to treat, depending on thewavelength of the laser energy. The invisible 1064 nm Nd:YAG laser is poorly absorbed byepidermal melanin, making this the best laser wavelength for darker skin and dark black ink.Recent pastel and white coloured inks contain high concentrations of highly reflectivetitanium dioxide. Consequently, such inks are difficult to remove and may become oxidizedand turn black during the treatments.
Multiple treatment protocols need to be coordinated with the patient along with detailedinstructions on post wound care. Daily dressing changes are required with possible posttreatment sequelae of blistering, hypopigmentation, and even scarring. Nanosecond Q-switched lasers can require 10 – 20 treatment sessions depending on the age and fadedappearance of the tattoo. Amateur tattoos usually clear quickly due to the shallower tissuepenetration and “homemade” dye sources. These treatments are painful, but the discomfortcan be mitigated with the use of a forced air chiller and or the application of a topicalanaesthetic [Figure 22].
Figure 22: James Mutter – CC BY-SA 4.0, Laser tattoo removal using Q-Switch Laserhttps://commons.wikimedia.org/w/index.php?curid=41993579

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 28 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Since the thermal relaxation time of tattoo ink is less than 10 nanoseconds, rapid shutterpicosecond tattoo lasers have emerged as a more effective device. Not only are the numberof treatments reduced, but the decreased fluence offers fewer complications commonlyseen with standard Q-switched laser devices.
Long-pulsed photo-thermal devices, such as long-pulsed lasers and intense pulsed light (IPL)systems, are also wholly unsuitable for safe and effective tattoo removal. Long-pulsed lasersand IPLs have pulse durations (pulse widths) of tens of milliseconds to match the thermalrelaxation time (TRT) of hair follicles and blood vessels with diameters of hundreds ofmicrons compared with tiny particles of tattoo pigment of 0.2-40 microns [11].
Pigmented Lesion Treatments
Figure 23: Solar lentigine on neck a) pre-treatment b) immediately post-treatment exhibiting peri-lesionalerythema and pigment darkening and c) at 4-weeks follow-up with complete resolution (Lumenis, QuantumSR free discharge IPL).
Pigmented lesions are a common condition found in all skin types and may be the result ofintrinsic aging which affects the skin by slow, irreversible tissue degeneration and collagenloss. Likewise, age spots may be caused by extrinsic aging resulting from exposure tooutdoor elements such as sun, wind, and environmental pollution. Asians generally exhibitmore pigmentary dyschromia or Melasma, whereas telangiectasia and diffuse redness arethe primary component of Caucasian photo-aging. Pigmented lesions can vary in colour, sizeand depth.
Figure 24: Solar lentigine dorsum hand a) pre-treatment b) immediately post-treatment and c) at 4-weeksfollow-up (constant spectrum IPL).
Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 29 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Several different types of laser and IPL devices have been used successfully to remove skinpigment with multiple treatment sessions. It is assumed that the mode of action iscoagulation or photo-oxidation of groups of melanosomes in the target lesion by radiantlight energy [12].
The normal sequelae after treatment of superficial epidermal pigmented lesions are a rapiddarkening, crusting and slough-off within a matter of days to a week. It is often believed thathigh energy, short sub-pulse duration, ‘free discharge’ IPL systems are the best to eliminateepidermal pigmentation such as ephilides (freckles) and lentigines (sunspots). Epidermalpigmented lesions, such as age spots, are prime targets for photo rejuvenation and theirremoval contributes to the overall cosmetic outcome for the patient. These pigmentedlesions are typically superficial and respond best to laser and IPL in a wavelength range of500-600 nanometres (nm) where there is high absorption by melanin [Figures 23 & 24].
According to Anderson’s and Parrish’s theory of selective photothermolysis by using veryshort pulsing lasers, such as the frequency doubled Q-switched Nd:YAG, Q-switched rubyand Q-switched alexandrite lasers, the laser light can be targeted to different melaninchromophores at various depths in the skin. The flash lamp pulsed dye laser was the firstlaser developed on the principles of selective photothermolysis. Following this theory,matching the thermal relaxation time (TRT) of melanosomes, in the targeting of pigmentedlesions, suggests that melanosomes can only be destroyed optimally at laser pulse durationsbetween 40 and 750 nanoseconds. Melanin absorbs broadly across a wide range ofwavelengths with superficial epidermal pigmentation treated best with wavelengthsbetween 500 nm and 600 nm.
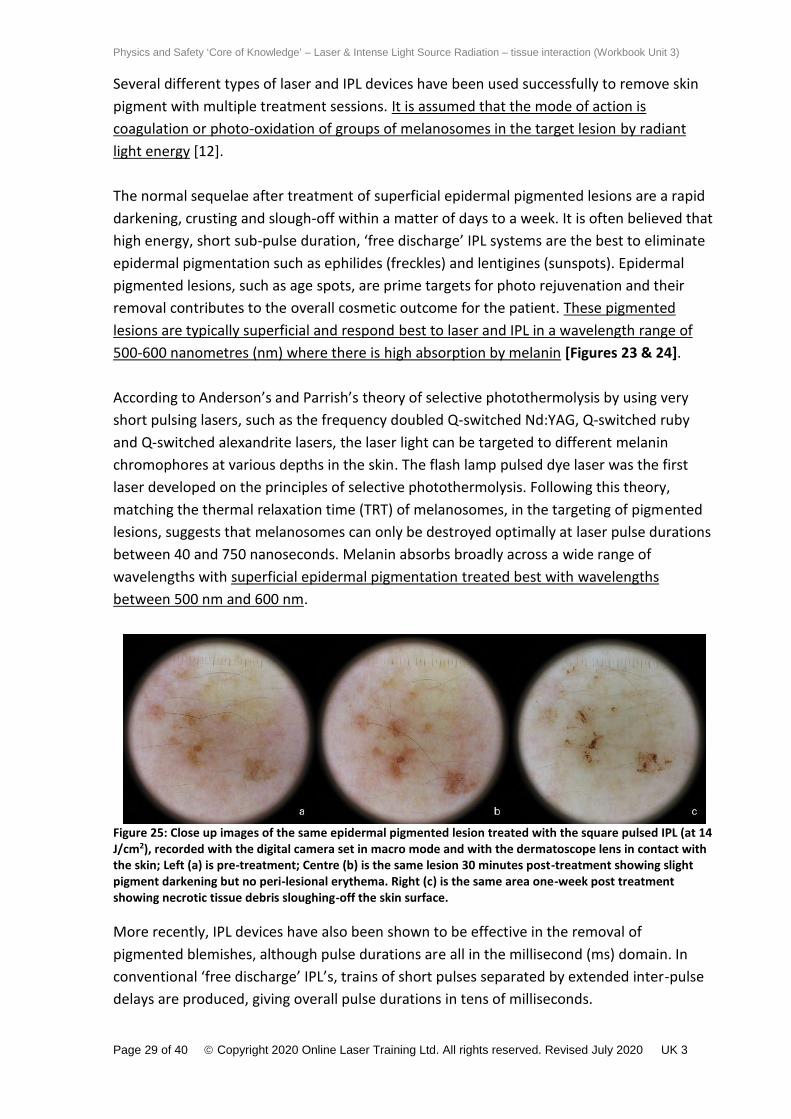
Figure 25: Close up images of the same epidermal pigmented lesion treated with the square pulsed IPL (at 14J/cm2), recorded with the digital camera set in macro mode and with the dermatoscope lens in contact withthe skin; Left (a) is pre-treatment; Centre (b) is the same lesion 30 minutes post-treatment showing slightpigment darkening but no peri-lesional erythema. Right (c) is the same area one-week post treatmentshowing necrotic tissue debris sloughing-off the skin surface.
More recently, IPL devices have also been shown to be effective in the removal ofpigmented blemishes, although pulse durations are all in the millisecond (ms) domain. Inconventional ‘free discharge’ IPL’s, trains of short pulses separated by extended inter-pulsedelays are produced, giving overall pulse durations in tens of milliseconds.

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 30 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
In this case, the principle of selective photothermolysis is assumed to apply to the thermalcoagulation of ‘clumps’ of melanosomes in aggregated groups comprising the pigmentedpatch on the skin. During this process, the normal pigment in the skin is spared with therapid loss of heat from the more widely distributed melanosomes in the epidermal tissue. Itis therefore, more likely that the mechanism of destruction with IPL, leading to photo-oxidation and blackening of lesional melanin is non-specific thermal denaturation or necrosisof the melanosomes, rather than clearly defined photothermolysis [Figure 25].
Haemoglobin, melanin, and water are the primary absorbing chromophores in human skin.Each chromophore has specific peak absorption wavelengths in the electromagneticspectrum. Melanin and haemoglobin absorb well in the wavelength range of 530-950 nm[Figure 4] in target lesions such as solar and senile lentigines, café-au-lait macules, melasmaand post-inflammatory hyperpigmentation, as well as Campbell de Morgan spots andtelangiectasia. The optical energy is absorbed as heat, raising the temperature of the targetand hence, denaturing the key structural proteins. There is greater absorption of epidermalmelanin in darker skin types, whether ethnic or sun-induced and this restricts the available“therapeutic window” and along with it, the IPL’s effectiveness with Fitzpatrick Skin Type’s 4-6.
Typical intense pulsed light (IPL) systems employ high intensity flash lamps that emitpolychromatic light. Contrasting with a laser system, these flash lamps work with incoherentlight in a broad wavelength spectrum of 500 nm to over 1100 nm at energies up to 60 J/cm2.They have options of various wavelengths that can be emitted using a selection ofreflectance or absorption filters. These reflectance or absorption filters generally rangebetween 520 nm and 650 nm, with higher cut off filters used to protect darker skin fromthermal damage caused by shorter wavelengths. The intense light can be delivered as single,double, or multiple sub-pulses within the millisecond domain. The inter-pulse delay andtrains of sub-pulses are intended to protect the superficial epidermis from excess thermalabsorption and consequential damage. These adjustable wavelengths and flexible pulsedurations allow IPL systems to offer wide diversity in the treatment of a variety ofpigmented lesions amongst different skin types. Light is delivered to the patient’s skinthrough a quartz or sapphire glass contact transmission block aperture of varying sizes,which may contain a cooling device to reduce heating of the upper epidermis.
Side effects observed when treating pigmented lesions include pain, transient erythema,swelling, blistering, crusting, ulceration, pigment darkening, desquamation and transienthyperpigmented ‘striping’ of the tissue caused by the glass transmission block beingincorrectly applied during treatment.

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 31 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Vascular Lesion Treatments
Early treatments for vascular lesions were performed with argon lasers, copper vapour /copper bromide lasers and krypton lasers. These lasers emit very long pulses, in the range of100 ms to 300 ms and wavelengths ranging from 400 nm to 578 nm. These laserwavelengths are absorbed by the skin at a very shallow depth from the surface due to arelatively high absorption in melanin. The combination of very long pulse durations (200 msto 300 ms) and the strong tissue absorption generated a high incidence of both immediateand subsequent adverse effects such as superficial burns, skin atrophy, scarring and pigmentdisturbances.
Today, IPLs and lasers are used for the treatment of facial and upper body telangiectasiaincluding 580-590 nm pulsed dye, 810 nm diode, and frequency- doubled 532 nm Nd:YAGlasers. Due mainly to use of short pulse durations (0.45–1.5 ms), these lasers and IPLs affectthe vessels more selectively and hence treatments are safer and more efficacious than theold long-pulse green lasers. An example of visible facial telangiectasia suitable for thermalcoagulation and blanching treatment is shown in [Figure 26] where immediate thermal‘blanching’ through collapse of the vessel wall is the typical result[13].
Figure 26: An example of visible facial telangiectasia suitable for thermal coagulation and blanching, beforeand after four IPL treatments. (Courtesy of Perter Bjerring MD)
The short pulse duration (0.45 ms) of the pulse dye laser reduces the risk of severe long-term adverse effects, but also leads to vessel disruption and visible purpura. This is oftenvery disturbing for the patients.
Light absorption in haemoglobin occurs at wavelengths of 412 nm and up, but due to astrong concurrent melanin absorption in the epidermis, only longer wavelengths reachdeeper vessels in the skin. The most effective wavelength range is in the spectral range from540 nm to 650 nm, incorporating the haemoglobin absorption peaks at 542 nm and 577 nm.For thicker vessels (0.3 mm to 0.5 mm) Kienle et al. predicted – based on the Monte Carlocomputer simulation method – that wavelengths of about 600 nm would be optimal in order

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 32 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
to achieve selective photothermolysis. Broadband intense light sources (intense pulsed light(IPL) systems) are able to emit continuous light spectra which contain significant proportionsof light at wavelengths from 550 nm or 570 nm to 1200 nm, thereby covering all clinicallysignificant absorption peaks.The principal difficulty with treating vascular lesions is that, unlike a static target such aspigmentation or hair follicles, blood is a moving target as it flows through the vessels thatone is seeking to eliminate. It is often difficult to gauge the depth and dimensions of bloodvessels even with the help of diagnostic aids such as magnification and cross-polarized light.It is important for the laser/IPL operator to be aware of underlying medical conditions andmedication (such as anticoagulants like Aspirin, Ibuprofen and Warfarin) that may add to thedifficulty of coagulating target vessels.
Leg vessels are more difficult to treat than facial vessels as they are deeper, darker and havethicker vessel walls. Deeper penetrating wavelength lasers, such as the Alexandrite at 755nm, Diode at 980 nm, and Nd:YAG at 1064 nm, have been used successfully to eliminatesuch vessels with a series of treatments. However, aggressive procedures must be taken toavoid over-treatment at such high energies and consequential side effects.
Acne
The opportunity to use photodynamic therapy (PDT) to treat acne has already beenintroduced earlier in this section. Clinical research has established the photosensitivity ofprotoporphyrin. The absorption characteristics for protoporphyrin IX (PpIX) includesignificant absorption peaks at 508 nm, 542 nm, 577 nm and 635 nm. Several of thesewavelengths are included in the high-energy output of broad-band light using a 500 nm to950 nm filter. These devices will therefore provide a calculated aggregate of energyabsorption in PpIX equal to or greater than that provided by the single wavelength flashlamp pumped pulsed dye laser at 585 nm.
Figure 27: Mechanism of P. acnes destruction by visible light interaction with porphyrins. When exposed toabsorbed light wavelengths, porphyrins act as photosensitizers and generate highly reactive free radicalspecies, one of which is singlet oxygen. These radicals are potent oxidizers and destroy the lipids in the cellwall of the P. acnes. Courtesy of Mariwalla and Rohrer© 2005 Wiley-Liss, Inc.

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 33 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Most high-power IPL systems can produce filtered light in the range 500 nm to 1100 nm athigh fluences. This energy density delivered even at half the maximum output of the IPL atthe peaks of PpIX absorption will exceed 1.5 J/cm2 across all of the most sensitive significantabsorption peaks listed above. The mechanism of P.acnes destruction is simply illustrated byMariwalla and Rohrer and reproduced in Figure 27.
With most IPLs, the use of clear ultrasound coupling gel, both short (and potentially harmful)UV wavelengths and longer infrared (IR) wavelengths (which might cause excessive tissueheating) are largely filtered out. Suitably constructed IPL pulse formation should ensureprecisely dosed energy to target photoacceptors and provide optimum effectiveness instimulating the body’s own immune system response. It has also been suggested that lightabsorption by target cells produces other conditions, which coupled with that of the singletoxygen species induced by PpIX provides a micro-environment unsuitable for P. acnes.
Blue light is 40 times more potent than red light in porphyrin excitation and highlybactericidal in the epidermis. However, blue light is much more rapidly attenuated and thelight intensity decays to almost zero at the depth of a sebaceous gland one millimetre belowthe skin surface. However, the effect of even less than one percent of blue light should notbe ignored as these highly active photons may still have a biological effect in the sebaceousgland.
Apart from photochemical stimulation of endogenous porphyrins and the employment ofexogenous photosensitizers, photothermal interruption of acne’s pathogenesis is a furtheroption. Low intensity visible green light between 500 nm and 570 nm, yellow light 570 nmand 600 nm and red light 600 nm and 780 nm wavelengths all penetrate deeply enough tohave a primary effect on P. acnes in the infundibulum and sebaceous glands. At higherintensities, the longer wavelengths may have a direct coagulative effect on the hyper-vascularity associated with acne, thereby offering a target for selective photothermolysis.The bulk water-heating effect of near and mid-infrared lasers at 1064 nm to 1540 nm mayalso be employed to achieve damage up to several mm into the dermis, thereby alsocapturing sebum in the typically enlarged sebaceous glands of an acne sufferer. Numerouslasers have been marketed for acne treatment in this mid-infrared spectrum with variablesuccess.
The enhanced acne treatment effect with concomitant use of 20% 5-aminolevulinic acid (5-ALA) PS is well documented in the literature. However, it is unlikely that national regulatoryagencies will permit over-the-counter (OTC) use of such potent chemical photosensitizers. Itis plausible that physician-directed use of light therapy in combinations with such productswill emerge in the foreseeable future but this avenue of research is beyond the scope of thiscourse book.
Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 34 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Demodex (a genus of tiny parasitic mites that live in or near hair follicles) may have a role inthe pathogenesis of acne and the mites associated with Rosacea and can be selectivelydamaged by laser and IPL. Research has debated whether their increased numbers are acause of Rosacea, however, some speculate that an overabundance of a demodex maytrigger an immune response or inflammation.
Adverse effects which are to be anticipated with light-based acne treatments generally occurpost-operatively and are similar to those observed during laser/ IPL hair reductiontreatments. The exception being inadvertent phototoxicity with the photosensitizer ALA.
Complete acne remission using light-based technology is only a remote possibility and themost successful way forward will probably involve the combination of light therapy and PDTunder the direction of a physician. However, from the standpoint of better routinemanagement of acne, there is sufficient encouragement from the reported clinical outcomesto anticipate that both blue LEDs and low intensity IPLs offer the opportunity fordevelopment of low energy home devices.
Other Cosmetic Treatments
Although laser / IPL non-invasive hair reduction technology has massively increased theutilisation of energy based devices since the 1980s, the use of surgical CO2 and Erbium:YAGlasers for rhinophyma, cosmetic genital surgery, blepharoplasty and full facial ablativeresurfacing have also expanded the use of lasers significantly in the cosmetic category.
Laser lipolysis: 1064 nm, 1440 nm and 1320 nm laser devices have been designed to destroyfat cells, coagulate bleeding vasculature and heat tissue for tighter skin. Single or multiplewavelength lasers are available for treating localized fat deposits on the face and body.These devices are a surgical procedure requiring tumescent anaesthesia along with theinsertion of a thin cannula and laser fibre into the fatty tissue to “melt” the fat in situ.
Haemostatic incision (e.g. rhinophyma, blepharoplasty, uvulopalatoplasty [LAUP], cervicalconisation, etc.). The surgical laser handpiece focusses the laser beam to a suitable spot sizefor the intended application.Tissue ablation e.g. full ablative skin resurfacing, fractional ablative and non-ablativeresurfacing, endometrial ablation, etc.
Deep Infra-Red skin tightening: Using wavelengths in the range 850 nm to 1800 nm andtissue exposures of 2.5 to 20 seconds to provide deep dermal heating for the treatment ofskin laxity (but not cellulite, fat, muscle or stretch marks).
Laser vaginal skin tightening: Fractional CO2 and Erbium laser ablation and remodelling of thevaginal wall in vaginal relaxation syndrome. Also, incontinence and dyspareunia (painful ordifficult sexual intercourse) has also appeared to be relieved from a series of outpatientprocedures.

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 35 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
EVLT: Endovenous Laser Treatment has proven to be beneficial for the indications of lowerextremity reticular vessels and Greater Saphenous Vein incompetence. Under ultrasound,the fibre laser systems deliver the correct combination of wavelength (810 nm, 980 nm, or1320 nm), pulse duration and pulse interval to effectively damage the wall of the vein beingtreated without causing damage to surrounding structures such as nerves. These systemsprovide long-term treatment for the underlying cause of varicose veins in the lower limbs.
Laser Surgery in Disease, Disorder and InjuryUnlike other surgical instruments, lasers are a unique ocular hazard and the risks when usinglasers have driven the adoption of international standards for laser safety. Traditionally,surgeons have acquired laser surgical skills through observation / preceptorship trainingworking with senior colleagues, attending hands-on laser workshops and conferences.
OBGYN
Lasers used in OBGYN and urology include Carbon Dioxide (10,600 nm), Argon (514 nm), Diodepumped (400-600, 980 & 1470 nm), Tr:YAG (1.5, 1.9 m), Er:YAG (2,940 nm), Nd:YAG (1064 nm)and Ho (2,100 nm). Lasers have been a valuable tool for OBGYN surgeons for over threedecades where they have proved effective in numerous applications including colposcopy(ablation or excision of lesions of the lower genital tract, treatment of dysplasia and warts ofvulva, vagina, perineum and perianal area), vaporisation or excisional cone biopsy in thetreatment of cervical intraepithelial neoplasia (CIN); treatment of vulva intraepithelial neoplasia(VIN) and vaginal intraepithelial neoplasia (VAIN); laparoscopy in intra-abdominal laparoscopicsurgery including endometrial ablation, hysterectomy, adhesiolysis in pelvic adhesion disease,lysis of vascular adhesions; hysteroscopy in the removal of myomas and ovarian fibroids, etc.
ENT
From a number of medically useful lasers, mainly the neodymium YAG and the carbon dioxidelaser are employed in surgical otorhinolaryngology. The most widely used laser in ENT surgery isthe carbon dioxide (CO2) laser. Its main effect of high precision cutting with an extremely finezone of coagulation reduces bleeding considerably after incision.
Main treatments include: Transoral Laryngeal Microsurgery: cordectomies and cordotomies, polyps and laryngeal
papillomas (including diffuse papillomatosis), cordal nodules, benign neoformations,Reinke’s oedema, laryngocele, hyperkeratosis laryngitis, scar tissue, granulomas,congenital web, leukoplakia and erythroplasia, primary laryngeal tumours, surgery afterunsuccessful radiotherapy, paralysis in adduction of the vocal chords, laryngotrachealstenosis, laryngeal amyloidosis.
Middle Ear Surgery: stapedotomies and myringotomies. Oral Surgery: leukoplakias, erythroplasias, papillomas, haemangiomas, tumours (e.g.
glossectomy), Zenker’s diverticulum, choanal atresia, LAUP (Laser Assisted UvuloPalatoplasty), tonsillotomy & tonsillectomy, sialolithiasis (salivary stones).

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 36 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Nasal, Endonasal & Endoscopic Sinus Surgery: turbinate reduction (for hyperplasia ofturbinates), septoplasty, removal of nasal obstructions (e.g. stenosis), recurrentpolyposis nasi & sinuum, synechiae, rhinophyma, cheloids and hypertrophic scars.
Tracheobronchial Tree: stenosis, nodules, polyps, tumours Head & Neck: resection of tumours in sub-facial and neck areas
Orthopaedics
Current orthopaedic lasers function in the ultraviolet (excimer) or in the infrared portion of theelectromagnetic spectrum (carbon dioxide, neodymium: yttrium-aluminium-garnet, holmium).The holmium laser at 2,100 nm wavelength is the most widely used wavelength as anarthroscopic surgical tool. It has a minimal amount of thermal necrosis and is able to cut andablate tissues with great ease. It is clinically useful for meniscal cutting and ablation, lateralretinacular release, release of posttraumatic fibrosis, chondroplasty, synovectomy,debridement, labral tear ablation in a shoulder, subacromial decompression, rotator cuffdebridement, tissue tightening (collagen shrinking), ankle impingement decompression anddebridement, and percutaneous nucleotomy.
Ophthalmic Lasers
Retinal photocoagulation: Photocoagulators cauterize blood vessels with heat generated bythe laser beam. The laser creates tiny, controlled burns that create adhesive forming scartissue. Applications include: Proliferative diabetic retinopathy Retinopathy of prematurity Macular oedema Retinal tears and detachments Branch retinal vein occlusion Choroidal neovascularizationCommonly used lasers include: in the past - Ruby (694 nm), Argon (488, 514 nm), Krypton(647 nm) and currently - frequency-doubled Nd:YAG (532 nm), and yellow semiconductorlaser (577nm).Capsulotomy: Plasma-mediated laser-tissue interactions are applied to fragmentation of theopacified posterior lens capsule (secondary cataract) with a slit-lamp coupled nanosecondNd:YAG laser. Anterior capsulotomy, lens segmentation and corneal incisions can beperformed with a femtosecond laserLaser Iridotomy (LI): A combination of millisecond and nanosecond, argon laser (514 nm) orNd:YAG (532 nm) and QS FD Nd:YAG is used to treat angle closure glaucoma, “pupillaryblock”Selective Laser Trabeculoplasty (SLT): A Q-switched, frequency-doubled, 532 nm Nd:YAGlaser is used to reduce intraocular pressure in patients with open-angle glaucoma whose IOPcan’t be controlled by maximum-tolerated medical therapy or argon laser trabeculoplasty(ALT).Corneal Refractive Surgery: Laser-Assisted In Situ Keratomileusis (LASIK) includes 2 steps: (a)cutting of a flap in the cornea (by mechanical microkeratome or a femtosecond laser) to pull

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 37 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
it back and expose the corneal stroma for laser ablation; (b) precise ablation of the cornealstroma using nanosecond pulses of ArF 193 nm excimer laserto correct refractive errors and improve visual acuity.
Treatment-Related Side Effects
Side Effects and Complications in Cosmetic Treatments
Temporary side effects such as soreness, oedema, redness or irritation, can be dealt with byskin cooling (refrigerated cooling gel packs, forced-air cooling, etc.), calming andmoisturising lotions (e.g. aloe vera), appropriate patient advice and medication if indicated.Hyperpigmentation is usually transient but further treatment should be deferred until thecondition has resolved. The most common side effects of laser/IPL treatment are erythema and oedema
(redness and swelling), which generally occur immediately after treatment andtypically resolve within 24 to 48 hours. If a burn-associated reaction is expected, asingle application of an over-the-counter anti-inflammatory cream or ointment (suchas Eumovate) may be used if available but should not be used beyond 48 hrs.
Mild to moderate pruritus – this will normally settle over 1-3 days but may requiremedication (OTC hydrocortisone) to relieve the itching.
Crusting, blister or burn - suitable burn sprays and healing ointments should berecommended if this occurs. If the reaction persists the client should be referred on toconsult with their doctor. The LPA/LSO should be advised. Follow establishmentadverse incident procedures.
Activation of infection: Herpes simplex, folliculitis, etc. – refer-on for prescribing ofsuitable prophylactic anti-viral or topical or oral anti-biotic medication.
Excessive swelling (oedema), fragile skin, bruising (purpura): Cool area for immediatepain relief; Advise LPA and refer patient on to consult with GP; follow establishmentadverse incident procedures.
Skin pigment changes – both hyperpigmentation and hypopigmentation are possible,however this should be temporary but may take weeks or months to resolvecompletely.
Leukotrichia or “vellus change”– temporary or long-term bleaching of melanin fromhair follicles has been reported in the literature, where previously brown or blackterminal hair changes colour to yellow or white. The effect is usually temporary,normal hair colour returning in one to four months.
Synchronous (or ‘in-phase’) hair growth (most likely after the 3rd or fourth treatment) –as this indicates new anagen hair, treat again as soon as possible for maximum hairreduction effect.
Discolouration or “smudging” of tattoos and/or semi-permanent makeup throughthermal absorption in coloured pigment by visible or IR laser wavelengths or parts ofthe broadband IPL spectrum - mask tattoos with opaque adhesive dressings to shield

Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 38 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
the tattoo pigment from laser/light energy, identify semi-permanent make-up pigmentbefore treating with laser. From a light-skin tissue interaction standpoint, powerfullaser and IPL outputs should be kept at least 3-5 mm away from the edge of visibletattoo ink.
Scarring – apply silicone gel sheet, refer-on to healthcare professional. Steroid orinterferon injections, resurfacing, fillers, further laser treatment (to reduce redness),etc.
Photosensitivity reaction - check for PDT therapy, refer-on to healthcare professionalfor suitable medication.
Paradoxical Hair Growth
In some patients, laser/IPL hair removal treatment has a paradoxical effect of stimulatinghair growth: new terminal hair growth has been observed in areas untreated but in closeproximity to the treated ones. The incidence of paradoxical hair growth, usually associatedwith polycystic ovarian syndrome (PCOS) and ovarian hyperandrogenism, in professionaltreatments has been reported to range from 0.6% to 10% (Figure 28).
The most susceptible patients are female individuals with darker skin types (III-VI) andreceiving facial treatments. In most cases, this paradoxical hair growth occurs at a site thathas a high vellus (fine hair count) and is relatively free of terminal hairs, such as adjacent tountreated facial areas or neck. All laser and light sources have the potential to cause hairinduction as there has been no clear relationship established between the type of hairremoval device and fluence used with the incidence of paradoxical hair growth. Possiblecauses include the effect of inflammatory mediators and using sub-therapeutic low fluenceparameters causing induction of the hair cycle [14].
Based on clinical experience, it is recommended in this subset of users not to start lasertreatment in order to prevent paradoxical hair growth or in cases where it occurs, to stopfurther laser treatment and revert to traditional hair removal methods such as waxing.
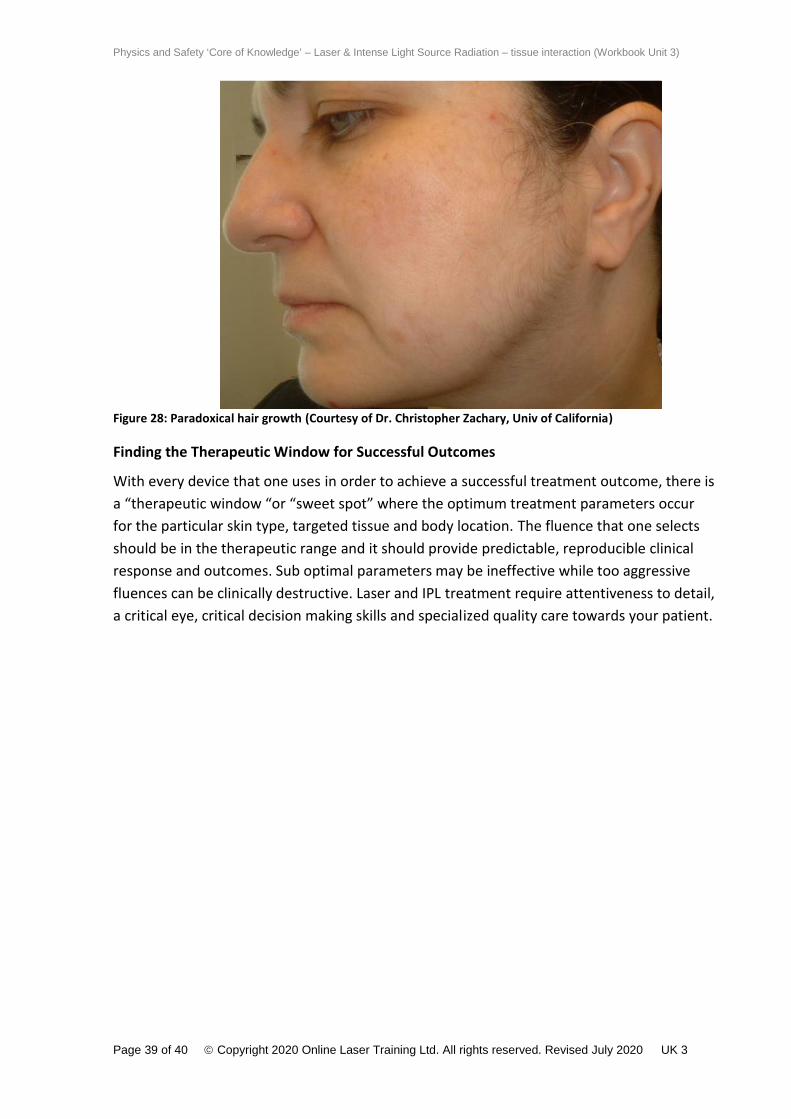
Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 39 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
Figure 28: Paradoxical hair growth (Courtesy of Dr. Christopher Zachary, Univ of California)
Finding the Therapeutic Window for Successful Outcomes
With every device that one uses in order to achieve a successful treatment outcome, there isa “therapeutic window “or “sweet spot” where the optimum treatment parameters occurfor the particular skin type, targeted tissue and body location. The fluence that one selectsshould be in the therapeutic range and it should provide predictable, reproducible clinicalresponse and outcomes. Sub optimal parameters may be ineffective while too aggressivefluences can be clinically destructive. Laser and IPL treatment require attentiveness to detail,a critical eye, critical decision making skills and specialized quality care towards your patient.
Physics and Safety ‘Core of Knowledge’ – Laser & Intense Light Source Radiation – tissue interaction (Workbook Unit 3)
Page 40 of 40 Copyright 2020 Online Laser Training Ltd. All rights reserved. Revised July 2020 UK 3
References
[1] CLC/TR 50448:2005 Guide to levels of competence required in laser safety. Available at:https://shop.bsigroup.com/ProductDetail?pid=000000000030138690[2] IEC TR 60825-8:2006 Safety of laser products – Part 8: Guidelines for the safe use of laserbeams on humans. Available at: https://webstore.iec.ch/preview/info_iec60825-8%7Bed2.0%7Den.pdf[3] MHRA: Lasers, intense light source systems and LEDs - Guidance for Safe Use in medical,surgical, dental and aesthetic practices. September 2015 Available at:https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/474136/Laser_guidance_Oct_2015.pdf[4] Essential Standards Regarding Class 3B and Class 4 Lasers and Intense Light Sources inNon-surgical Applications. October 2016 – published by the British Medical LaserAssociation. Available at: https://www.bmla.co.uk/bmla-essential-standards/[5] Z136.3 2011 American National Standard for Safe Use of Lasers in Health Care. Availableat: https://webstore.ansi.org/standards/lia/ansiz1362011#:~:text=in%20Health%20Care-,ANSI%20Z136.,altered%20or%20symptoms%20are%20relieved.[6] Town G, Botchkareva N, Uzunbajakava N, Nuijs A, van Vlimmeren M, Ash C, Dierickx C.Light-based home-use devices for hair removal: Why do they work and how effective theyare? Lasers Surg Med. 2019; 51:481-490.[7] Fleming D. Controversies in skin resurfacing: the role of erbium. J Cutan Laser Ther. 1999;1:15-21.[8] Shim E, Tse Y, Velazquez E, et al. Short pulse carbon dioxide laser resurfacing in thetreatment of rhytides and scars. Dermatol Surg. 1998; 24: 113±17.[9] Manstein D, et al. Fractional Photothermolysis: A New Concept for CutaneousRemodeling Using Microscopic Patterns of Thermal Injury. Lasers Surg Med. 2004; 34:426-438.[10] Dierickx CC, Anderson RR. Visible light treatment of photoaging. Dermatol Ther. 2005;18:192-208.[11] Barcaui CB. Localized hypertrichosis after IPL tattoo removal. Dermatol Surg. 2007;33:621-622. DOI: 10.1111/j.1524-4725.2007.33126.x[12] Emerson R, Town G. Hair removal with a novel, low fluence, home-use intense pulsedlight device: Preliminary Results. J Cosmet Laser Ther. 2009; Vol. 11:2:98-105.[13] Bjerring P, Christiansen C, Troillius A. Intense pulsed light source for treatment of facialtelangiectasiss. J Cosmet Laser Ther. 2001; 3:169-173.[14] Town G, Bjerring P. Is paradoxical hair growth caused by low-level radiant exposure byhome-use laser and intense pulsed light devices? J Cosmet Laser Ther. 2016; 18:6:355-362.
This is the end of Unit 3
Laser & intense light source radiation - tissue interaction





























